a
1-Proteinase Inhibitor Therapy for the Prevention of Chronic Lung
Disease of Prematurity: A Randomized, Controlled Trial
Joseph A. Stiskal, MDi; Michael S. Dunn, MD*; Andrew T. Shennan, MB*; Karel K. E. O’Brien, MB‡; Edmond N. Kelly, MB‡; Robert I. Koppel, MDi; Diane W. Cox, PhD§; Shinya Ito, MD§;
S. Lesley Chappel, RN§; and Marlene Rabinovitch, MD§
ABSTRACT. Background. An imbalance between in-creased neutrophil elastase and a dein-creased antiprotease shield has been suggested as a factor contributing to the development of chronic lung disease (CLD). We hypoth-esized that administration of a1-proteinase inhibitor
(A1PI), also known asa1-antitrypsin, to premature
neo-nates would prevent CLD.
Design. A randomized, placebo-controlled, prospec-tive study of A1PI supplementation was performed. Ne-onates<24 hours of age with birth weights 600 –1000 g on respiratory support, and 1001–1250 g with respiratory distress syndrome (RDS) were eligible. Intravenous A1PI (60 mg/kg) or placebo was infused on days 0, 4, 7, and 14. Primary outcome was CLD in survivors, defined as the need for supplemental oxygen on day 28.
Results. A total of 106 patients were recruited. There were no significant differences between groups in birth weight or incidence of RDS. The incidence of CLD in survivors was lower in the treated group, but the differ-ence did not reach statistical significance (relative risk [RR], 0.79; confidence interval [CI], 0.60 –1.02). This ben-eficial trend persisted at 36 weeks corrected gestational age (RR, 0.48; CI, 0.23–1.00). The incidence of pulmonary hemorrhage was lower in the treated group (RR, 0.22; CI, 0.05– 0.98). Other complications were not significantly different between groups.
Conclusions. In this, the first trial of a protease inhib-itor for the prevention of CLD in premature infants, the infusions were well-tolerated. A1PI therapy may impede the development of CLD and appears to reduce the inci-dence of pulmonary hemorrhage in some neonates born prematurely.Pediatrics1998;101:89 –94;a1-proteinase in-hibitor, bronchopulmonary dysplasia, infant, randomized, controlled trials; serine proteinase inhibitors.
ABBREVIATIONS. CLD, chronic lung disease; RDS, respiratory distress syndrome; A1PI,a1-proteinase inhibitor.
C
hronic lung disease (CLD) or bronchopulmo-nary dysplasia is the end result of unresolved neonatal acute lung injury.1 Affected infants develop an overly aggressive inflammatory response that can progress to pulmonary fibrosis and result in a prolonged need for respiratory support andhospi-talization. Compared with infants with respiratory disease who are born at term, preterm infants may be unable to down-regulate the inflammatory response to tissue injury.2Current therapies directed toward reducing pulmonary inflammation, such as dexa-methasone, can have significant side effects.3
Initial descriptive data identified low functional levels of protease inhibitor activity in infants with respiratory distress syndrome (RDS) compared with controls.4 Infants dying from RDS had the lowest levels. Rosenfeld and colleagues5 noted that a low functional level of a1-proteinase inhibitor (A1PI) at birth was a better predictor of CLD than traditional risk factors such as birth weight, gestational age, or severity of RDS. Merritt suggested that proteolytic enzymes released by inflammatory cells in the lung play a pivotal role in the development of epithelial injury and aberrant connective tissue remodeling that characterize CLD.6 These data supported the hypothesis that therapy with exogenous protease in-hibitors might restore protease/antiprotease balance and prevent the development of CLD. Availability of a commercial preparation of A1PI with a good safety profile has made it possible to test this hypothesis.
The potential for this approach was reinforced by a laboratory study performed by Koppel and co-work-ers.7They evaluated whether administration of exoge-nous A1PI delivered by intraperitoneal injection could protect rat pups from the effects of hyperoxia. De-creased arterial number, inDe-creased arterial muscularity, right ventricular hypertrophy, and decreased lung compliance developed in the control animals, but those pretreated with A1PI were protected.
The present study was designed to test the hypoth-esis that four intravenous infusions of A1PI given to very preterm infants over the first 2 weeks of life would result in augmentation of antiprotease activ-ity, inhibition of neutrophil elastase activactiv-ity, and protection from the development of CLD.
METHODS
A multicenter, prospective, randomized, double-blind, pla-cebo-controlled trial was performed. Institutional review board approval was obtained from the three hospitals in the University of Toronto Perinatal Complex: Women’s College Hospital, Mount Sinai Hospital, and the Hospital for Sick Children. The protocol was approved by the Bureau of Biologics, Health and Welfare, Canada.
Eligibility
Infants with birth weights of 600 to 1000 g requiring endotra-cheal intubation and neonates with birth weights of 1001 to 1250 g From *Women’s College Hospital, ‡Mount Sinai Hospital, the §Hospital for
Sick Children and theiUniversity of Toronto, Toronto, Ontario, Canada. Presented in part at the annual meeting of the Pediatric Academic Societies’, Washington, DC, May 6 –10, 1996.
Received for publication May 19, 1997; accepted Sep 16, 1997.
Reprint requests to (J.A.S.) Service of Neonatology, Bryn Mawr Hospital, 130 S Bryn Mawr Ave, Bryn Mawr, PA 19010.
with RDS were eligible for inclusion in the study. Infants were deemed to have RDS if they required assisted ventilation and supplemental oxygen, exhibited characteristic features (decreased lung volume, reticulogranular appearance of the lung fields, and/or air bronchograms) on chest roentgenogram, and were treated with surfactant. Newborns were excluded if they were.24 hours of age, were considered moribund, or had congenital anom-alies. Informed parental consent was required in all cases.
Randomization
Randomization was carried out centrally by the pharmacist using computer-generated random number tables. Allocation was concealed in sequentially numbered, opaque, sealed envelopes arranged in blocks of 4 and organized into 10 different strata. Stratification was based on birth weight (600 – 800, 801–1000, 1001– 1250 g) and whether the infant was inborn or outborn. Infants who were products of multiple gestations were randomized individu-ally. Investigators, parents, and caretakers were blinded to group allocation. No crossover was allowed, and the medication was not available outside of the study.
Study Maneuver
The A1PI or placebo infusion was prepared and coded by the pharmacist. The placebo was Albumin (Human) 5% (USP), which has a similar appearance to the study medication. A1PI (Prolastin/ Bayer), also known asa1-antitrypsin, was supplied as a single-dose vial of sterile lyophilized powder containing purified human A1PI with a functional activity of 500 mg. The medication was reconstituted with 20 mL of sterile water.
A dose of 60 mg/kg (2.4 ml/kg) of A1PI or an equivalent volume of placebo was infused over 5 minutes by the study nurse, investigator, or house officer as soon as possible after randomiza-tion and no later than 24 hours of age. Repeat doses were infused on days 4, 7, and 14 at a standard time of 10:00am. Heart rate and blood pressure were measured before and at 15, 30, 60, and 120 minutes after the infusion.
Functional and antigenic plasma levels of A1PI were performed on days 0, 1, 2, 3, 4, 7, 10, 14, and 28 on the first 23 patients.8 Trough and day 28 levels were performed on the remainder. Functional levels were calculated from the inhibitory capacity of the plasma on pancreatic porcine elastase. Antigenic levels were measured by electroimmunoassay with monospecific antihuman A1PI antibody.
Other aspects of clinical management were determined by the clinical care team working under the guidance of the neonatolo-gist in charge. Bovine lipid extract surfactant (BLES Biochemicals Incorporated, London, Ontario, Canada) was given using a stan-dard rescue approach.9Conventional mechanical ventilators were used in conjunction with nasotracheal tubes. After a brief period of stabilization, infants were cared for in humidified isolettes. Total parenteral nutrition including intravenous lipid emulsion was generally started on the third day of life. Nasopharyngeal continuous positive airway pressure was commonly applied to facilatate extubation. It was not the routine of the units to pre-scribe antimicrobial therapy for tracheal colonization with Urea-plasma urealyticum.
Primary and Secondary Outcomes
The primary outcome was the incidence of CLD in survivors. Infants were deemed to have CLD if they required supplemental oxygen at 28 days of age to maintain a hemoglobin oxygen satu-ration above 90%.
Secondary outcomes included incidence of oxygen dependence at 36 weeks’ corrected gestational age10and whether an infant met predetermined criteria for treatment with corticosteroids. Steroid criteria were defined as a requirement for mechanical ventilation and fraction of inspired oxygen of.0.30 for at least 48 hours after day 16 of life. The criteria were developed by consensus as rep-resenting reasonable indications for the prescription of dexameth-asone for CLD. Achievement of these criteria did not mandate treatment with steroids. Therapy with corticosteroids was delayed until after the full course of study medication had been given to more accurately assess the effect of A1PI. However, if the clinician managing an infant decided that treatment was indicated earlier, steroid criteria were considered to have been met. No consistent
dosing strategy was followed once therapy with corticosteroids was instituted.
Other efficacy parameters tracked included age at final extuba-tion, age off supplemental oxygen, and age off all respiratory support (mechanical ventilation, nasal continuous positive airway pressure, and/or supplemental oxygen). In a blinded manner, day 28 chest roentgenograms were graded by three neonatologists using a standard scoring system11and day 28 electrocardiograms were assessed for right ventricular hypertrophy or strain inter-preted by a pediatric cardiologist. The use of medications to treat CLD was recorded.
Complications of Prematurity
Common complications experienced by premature infants were defined prospectively in the protocol. Pulmonary hemorrhage was said to occur when blood-stained secretions were recovered from the endotracheal tube. Intraventricular hemorrhage was diag-nosed by serial echoencephalography and graded according to the criteria of Volpe.12Periventricular leukomalacia,13necrotizing en-terocolitis,14and retinopathy of prematurity15were also identified and graded by commonly accepted criteria. The diagnosis of patent ductus arteriosus was made on clinical grounds with con-firmatory echocardiography available. Use of indomethacin and surgical ligation were monitored. Sepsis was defined by recovery of bacteria or fungi from blood or cerebrospinal fluid. Any other adverse events occurring during the study period were also re-corded.
Other safety parameters monitored included a complete blood count and liver and renal function tests performed on study day 28. A 2-year developmental follow-up assessment will also be performed.
Confounders
To allow the full effect of the study medication to be appreci-ated, several confounders that might influence the primary and secondary outcomes were identified. The use of intravenous lipid emulsions, blood products, and breast milk was carefully tracked as was fluid intake over the first 2 weeks of life. Tracheal coloni-zation byUreaplasma urealyticumwas assessed by culturing tra-cheal aspirates obtained on days 0, 4, and 14.
Statistical Analysis
Sample Size
A review of the Women’s College Hospital database of infants who met eligibility criteria revealed that 60% of infants surviving to 28 days required supplemental oxygen. To judge the interven-tion effective, a 50% reducinterven-tion in the incidence of this outcome was sought. Based on a two-tailedaof 0.05 and abof 0.2, the estimated sample size required to show such a reduction was 48 subjects per treatment group. With a predicted mortality rate of 10% before 28 days of age, a total sample size of 106 patients was chosen.
Analysis
Data were analyzed using the Statistical Analysis System (SAS, Cary, NC, version 6.10) computer program. Descriptive statistics (means and standard deviations) were used to describe the char-acteristics of the study population. Incidence comparisons were made using Fisher’s exact test while continuous numerical data were analyzed using two-tailedttests. Relative risks were calcu-lated with a normal approximation to the binomial distribution being assumed to obtain confidence intervals. All analyses were based on group assignment (intention to treat). Only thePvalue for the primary outcome was considered for experiment-wise error. All otherPvalues were accepted as indicating trends to-ward statistical significance as no correction was made for multi-ple comparisons. Comparisons of all safety-related outcomes were made with the patients grouped as actually treated. These com-parisons of incidence were expressed as relative risks with 95% confidence intervals. No interim analyses were performed.
or modify the protocol if complications occurred at a frequency greater than would be expected in this population.
RESULTS
Enrollment began in June 1994 and was completed in November 1995. At the inborn units, 367 patients met eligibility criteria, the parents of 167 were con-tacted, and the parents of 106 gave informed consent. The first 2 patients enrolled at the outborn center died and recruitment was halted. The safety commit-tee reviewed the cases and recommended that the study may proceed. However, no further enrollment took place at the Hospital for Sick Children. Consent was withdrawn by one family of an infant in the placebo group after a single infusion had been given. There were four protocol violations in the treatment group (single doses missed) and two in the placebo group (1 infant missed a single dose and 1 infant was given five times the correct volume). No patients were excluded from the analysis. A total of 53 pa-tients were randomly allocated to each group.
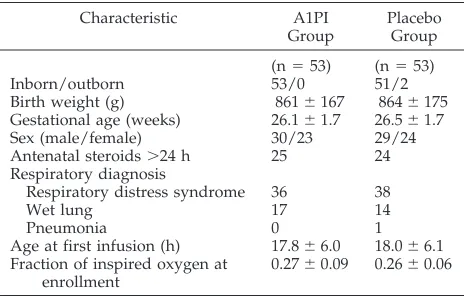
There were no significant differences between groups in the incidence of prolonged rupture of the membranes, abdominal delivery, multiple gestation, intrauterine growth restriction, or the other preran-domization characteristics listed in Table 1. Infusions were well-tolerated with no significant differences between heart rates or blood pressure between groups. There were no significant differences be-tween groups in plasma antigenic or functional A1PI levels at any of the time points studied. Renal, he-patic, and hematologic measurements were not per-turbed.
There were nine deaths before the 28-day evalua-tion point, five in the treatment group and four in the placebo group. With respect to the primary outcome, the incidence of oxygen dependence at day 28 in survivors, the null hypothesis was not rejected. Other outcomes are shown in Table 2. Oxygen de-pendence at 36 weeks’ corrected gestational age was lower in the treated group but the difference did not reach statistical significance. The group of infants receiving A1PI were extubated 1 day earlier, weaned to room air 11 days earlier, and free from the need for respiratory support 10 days earlier than infants in the placebo group. Although 31 infants in each group met the predetermined steroid criteria, only 20 of
the A1PI-treated infants compared with 28 of the placebo-treated infants were treated with dexameth-asone. Fewer infants in the treated group were pre-scribed inhaled steroids (budesonide) and bron-chodilators (salbutamol). Almost all of the infants in both groups received caffeine and very few infants received chronic diuretic therapy. Electrocardio-grams on infants who received active and placebo treatment noted right ventricular hypertrophy in 12 versus 6 and ischemia in 13 versus 17. The age at which infants in each group tolerated weaning to room air is shown in the Figure by using Kaplan-Meier curves.
Safety parameters are shown in Table 3. The inci-dence of pulmonary hemorrhage was lower in the A1PI group. There were no differences between groups in the incidence of patent ductus arteriosus, intracranial complications, or retinopathy of prema-turity. There were six cases of necrotizing enteroco-litis in the treatment group (two stage I, and four stage III). Three infants in the A1PI group died after day 28 but before hospital discharge. Of the deaths that occurred in the active treatment group five were due to sepsis or necrotizing enterocolitis, two were due to intracranial hemorrhage, and one was due to pulmonary hemorrhage. All four infants in the pla-cebo group died from hemorrhages: two intracranial and two pulmonary.
The relationship between confounding variables and group assignment was assessed. The groups were comparable with respect to the volume of fluid, intravenous lipid, breast milk, and blood products received. Intravenous lipid was commenced in both groups at a mean age of 2 days. Tracheal colonization with Ureaplasma urealyticum was present in 38% of the A1PI-treated infants and 30% of those who re-ceived placebo.
DISCUSSION
The etiology of CLD is thought to be multifactorial. The most important risk factors for the development of CLD include degree of prematurity, severity of RDS, duration and intensity of oxygen therapy, and mechanical ventilation.16Inflammation is also known to play a role in the pathogenesis of CLD and influx of neutrophils into the air spaces of human neonates with RDS has been demonstrated. A 20-fold increase in cell number in tracheal aspirates from infants who went on to develop CLD was documented compared with those with an uneventful recovery.17The influx, which is noted between 48 and 96 hours, disappears by the end of 1 week except in infants who go on to manifest signs of CLD.18Neutrophils synthesize elas-tase, a potent serine protease. Release of neutrophil elastase results in the hydrolysis of extracellular ma-trix components, as well as immunoglobulins, sur-factant proteins, fibrinogen, and complement.19,20 Merritt et al17have shown that neutrophil elastase is elevated in the tracheal lavage fluid of infants with RDS who go on to develop CLD. Injury to the devel-oping lung connective tissue, especially elastin and collagen, occurs when an imbalance exists between the production of proteases and the capability of inhibitor proteins to neutralize them. Evans et al3 TABLE 1. Baseline Characteristics of the 106 Patients
Characteristic A1PI Group
Placebo Group
(n553) (n553)
Inborn/outborn 53/0 51/2
Birth weight (g) 8616167 8646175 Gestational age (weeks) 26.161.7 26.561.7 Sex (male/female) 30/23 29/24 Antenatal steroids.24 h 25 24 Respiratory diagnosis
Respiratory distress syndrome 36 38
Wet lung 17 14
Pneumonia 0 1
Age at first infusion (h) 17.866.0 18.066.1 Fraction of inspired oxygen at
enrollment
0.2760.09 0.2660.06
found a decrease in trypsin inhibitory activity in the cord blood of preterm infants with RDS and infants with the most severe RDS had the lowest levels. This suggests that preterm infants may be at risk of pro-tease-antiprotease imbalance and are therefore sus-ceptible to the development of unresolved neonatal acute lung injury.
A1PI is a naturally-occurring glycoprotein synthe-sized by the liver and found in blood, tracheal
secre-tions, and colostrum. It shields the lung from prote-olysis by forming a complex with neutrophil elastase. Both the formation of this complex and oxidation of a methionine residue lead to its inacti-vation. Immature synthesis or increased inactivation is known to occur in at-risk neonates.21
In a review of protease-antiprotease interactions in the immature lung, Merritt and Hallman6stated that therapies designed to prevent or ameliorate CLD TABLE 2. Respiratory Outcomes in the 97 Survivors
Variable A1PI (n548) Placebo (n549) RR 95% CI
Status on day 28*
Beathing room air 18 10
Oxygen dependence 30 39 0.79 0.60–1.02
Chest x-ray score 1.661.1 2.061.4 n.s.
Oxygen dependence at 36 weeks CGA† 8 18 0.48 0.23–1.00
Death or oxygen dependence at 36 weeks CGA 15 22 n.s. Age at extubation (d) 28.2621.6 29.1619.2 n.s.
Age off oxygen 45.6639.3 56.8636.7 n.s.
Age off respiratory support 52.9636.6 63.2631.9 n.s.
Steroid criteria 31 31 0.96 0.57–1.64
Dexamethasone 20 28 0.73 0.48–1.10
Budesonide 12 23 0.53 0.30–0.94
Salbutamol 19 32 0.61 0.40–0.91
The denominator for each variable is the number of surviving babies at each time period, i.e., the primary outcome is based on the cohort alive at 28 days of age, while use of medications is based on the cohort who survived to hospital discharge.
*P5.08. †P5.06.
CGA, corrected gestational age is the gestational age plus the chronologic age after birth.
Figure. Kaplan-Meier curve of time to wean to room air by group alloca-tion. The age at which each survivor finally was weaned to room air is de-scribed by a Kaplan-Meier curve. A1PI-treated infants are indicated by a solid line; placebo-treated infants are indicated by a dashed line. The median time in oxygen was reduced by A1PI therapy from 57 to 41 days.
TABLE 3. Complications of Prematurity
Variable A1PI (n553) Placebo (n553) RR 95% CI
Respiratory complications
Pulmonary hemorrhage 2 9* 0.22 0.05–0.98
Pulmonary interstitial emphysema 1 2 0.50 0.05–5.35
Pneumothorax 1 3 0.33 0.04–3.10
PDA - Total/indo/ligated 27/24/3 25/20/1 1.08 0.73–1.59
IVH - Total 30 22 1.36 0.92–2.03
- Grade III–IV 5 9 0.41 0.16–1.05
PVL 5 4 1.25 0.36–4.40
NEC 6 0
ROP - Total/Cryo 23/2 26/0 0.88 0.59–1.34
Sepsis 16 18 0.89 0.51–1.55
Death before discharge 7 4 1.75 0.54–5.63
may require institution before or soon after the elab-oration of free elastase or other proteases into the air spaces before structural alteration of lung connective tissue and basement membrane structure ensues.6 The protease-antiprotease imbalance can be cor-rected by two strategies: reduction of elastase or augmentation of its inhibitors. Dexamethasone ther-apy of bronchopulmonary dysplasia has been shown to decrease bronchoalveolar lavage elastase ac-tivity.22Yoder23confirmed that dexamethasone treat-ment resulted in a significant decrease in the require-ment for respiratory support, improved pulmonary function, as well as pulmonary inflammatory indices expressed as neutrophil counts, elastase/2 3 A1PI, albumin, and fibronectin. It also provides a possible explanation for a mechanism of action of dexameth-asone in CLD. At this time there are conflicting re-ports regarding the efficacy of steroids in early RDS for the prevention of CLD. Because dexamethasone is associated with a significant complication rate, the alternative strategy of augmenting antiprotease pro-tection to prevent CLD was studied.
It was found in this randomized trial that supple-mentation of A1PI improved several clinical outcome parameters. The study had the power to show a 50% reduction in the primary outcome: oxygen require-ment at 28 days of age. Although improverequire-ment was noted, this level of protection was not achieved al-though a more modest reduction might still be clin-ically significant. This outcome was chosen in this initial trial to estimate a treatment effect for out-comes10in future trials. Encouraging trends toward improved outcome were noted, most notably through the reduction of pulmonary hemorrhage, mean days of oxygen therapy, the use of inhaled steroids and bronchodilators. A reduction in pulmo-nary hemorrhage would be consistent with animal models of elastolytic damage and protection by pro-tease inhibitors.24,25 Similarly, A1PI may have some protective effect against the development of reactive airway disease.26 Further work is needed to deter-mine if these findings were due to the effect of the medication or chance events.
Other than the incidence of pulmonary hemor-rhage, the observed frequency of complications of prematurity did not differ between groups. There was a trend toward more total but less severe intra-cranial hemorrhage in the treated cohort. Hemor-rhagic complications have not been described with adult usage. Although the incidence of infection was similar in both groups, more infants treated with A1PI died of infection or necrotizing enterocolitis. Administration of exogenous A1PI could theoreti-cally alter an infant’s immune response. This, how-ever, would be counter to the experience in its use in cystic fibrosis, where A1PI improves the bactericidal properties of epithelial lining fluid.27
Alternative explanations for the clinical findings can be offered. Confounders for the primary out-come were identified before study enrollment but not all potential confounders could be assessed. Ini-tial patient characteristics were well-matched. The incidence ofUreaplasma urealyticumcolonization also did not differ. A standard approach to therapy was
used, and no new management strategies were in-troduced during the study period.
CONCLUSION
This was the first randomized clinical trial de-signed to examine whether direct inhibition of neu-trophil elastase would lead to a reduction in the incidence or severity of CLD in very preterm infants. Four intravenous doses of A1PI were well-tolerated in very preterm neonates. A1PI appears to reduce the incidence of pulmonary hemorrhage and may im-pede the development of CLD in some neonates born prematurely. Further work is needed to determine if these findings were due to the effect of the medica-tion or chance events. Addimedica-tional study may also reveal that improved efficacy can be achieved through the use of an alternative dosing strategy. Further study is in progress with the aim of deter-mining the safety, efficacy, and pharmacokinetics of varying doses of A1PI versus placebo for the preven-tion of CLD.
ACKNOWLEDGMENTS
This work was supported by a grant from Bayer/Canadian Red Cross-Research and Development Fund.
We thank the nurses, physicians, pharmacists, and respiratory therapists for their assistance in the completion of this project. Teresa Barry Longley, RN, was instrumental in coordinating the study. We would also like to thank Kim Hanna, Trudy Lingham, and Geraldine Wyile from Bayer, Inc, for their support.
REFERENCES
1. O’Brodovich HM, Mellins R. Bronchopulmonary dysplasia: unresolved neonatal acute lung injury.Am Rev Respir Dis. 1985;132:694 –709 2. Jones CA, Cayabyab RG, Kwong KYC, et al. Undetectable interleukin
(IL)-10 and persistent IL-8 expression early in hyaline membrane disease: a possible developmental basis for the predisposition to chronic lung inflammation in preterm newborns.Pediatr Res. 1996;39:966 –975 3. Dexamethasone for neonatal chronic lung disease. Lancet. 1991;338:
982–983. Editorial
4. Evans HE, Keller S, Mandl I. Serum trypsin inhibitory capacity and the idiopathic respiratory distress syndrome.J Pediatr. 1972;81:588 –592 5. Rosenfeld W, Concepcion L, Evans H, Jhaveri R, Sahdeu S, Zabaleta I.
Serial trypsin inhibitory capacity and ceruloplasmin levels in prema-tures at risk for bronchopulmonary dysplasia.Am Rev Respir Dis. 1986; 134:1229 –1232
6. Merritt TA, Hallman M. Interactions in the immature lung: protease-antiprotease mechanism of lung injury. In: Merritt TA, Northway WH Jr, eds.Bronchopulmonary Dysplasia. Palo Alto, CA: Blackwell Scientific Publications; 1988:117–130
7. Koppel R, Han RNH, Cox D, Tanswell AK, Rabinovitch M. a1
-antitrypsin protects neonatal rats from pulmonary vascular and paren-chymal effects of oxygen toxicity.Pediatr Res.1994;36:763–770 8. Cox DW, Billingsley GD, Siewertsen MA.a1-antitrypsin. In: Hommes
FA, ed.Techniques in Diagnostic Human Biochemical Genetics: A Laboratory Manual.New York, NY: Wiley-Liss, Inc; 1991:473– 489
9. Dunn M, Shennan AT, Zayack D, Possmayer F. Bovine surfactant re-placement therapy in neonates of less than 30 weeks’ gestation: a randomized controlled trial of prophylaxis versus treatment.Pediatrics. 1991;87:377–386
10. Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period.Pediatrics. 1988;82:527–532 11. Toce SS, Farrell PM, Leavitt LA, Samuels DP, Edwards DK. Clinical and
roentgenographic scoring systems for assessing bronchopulmonary dysplasia.Am J Dis Child. 1984;138:581–585
12. Volpe JJ. Intraventricular hemorrhage in the premature infant— current concepts. Part II.Ann Neurol. 1989;25:109 –116
13. Calvert SA, Hoskins EM, Fong KW, Forsyth SC. Periventricular leukomalacia: ultrasonic diagnosis and neurologic outcome.Acta Pae-diatr Scand.1986;75:489 – 496
staging criteria.Pediatr Clin North Am. 1986;33:179 –200
15. International Committee for the Classification of the Late Stages of Retinopathy of Prematurity. An international classification of retinop-athy of prematurity.Pediatrics. 1988;82:37– 43
16. Ehrenkranz RA, Mercurio MR. Bronchopulmonary dysplasia. In: Sinclair JC, Bracken MB, eds.Effective Care of the Newborn Infant. Oxford, England: Oxford University Press; 1992:399 – 424
17. Merritt TA, Cochrane CG, Holcomb K, et al. Elastase anda1-proteinase
inhibitor activity in tracheal aspirates: role of inflammation in the pathogenesis of bronchopulmonary dysplasia. J Clin Invest. 1983;72: 656 – 666
18. Ogden BE, Murphy SA, Saunders GC, Pathak D, Johnson JD. Neonatal lung neutrophils and elastase/proteinase inhibitor imbalance.Am Rev Respir Dis. 1984;130:817– 821
19. McDonald JA, Kelly DG. Degradation of fibronectin by human leuko-cyte elastase: release of biologically active fragments.J Biol Chem. 1980; 255:8848 – 8858
20. Liau DF, Yin NX, Huang J, Ryan SF. Effects of human polymorphonu-clear leukocyte elastase upon surfactant proteins in vitro.Biochim Bio-phys Acta. 1996;1302:117–128
21. Bruce MC, Wedig KE, Jentoft N, et al. Altered urinary excretion of elastin cross-links in premature infants who develop
bronchopulmo-nary dysplasia.Am Rev Respir Dis. 1985;131:568 –572
22. Gerdes JS, Harris MC, Polin RA. Effects of dexamethasone and indo-methacin on elastase,a1-proteinase inhibitor, and fibronectin in
bron-choalveolar lavage fluid from neonates.J Pediatr. 1988;113:727–731 23. Yoder MC, Chua R, Tepper R. Effect of dexamethasone on pulmonary
inflammation and pulmonary function of ventilator-dependent infants with bronchopulmonary dysplasia. Am Rev Respir Dis. 1991;143: 1044 –1048
24. Fletcher DS, Osinga DG, Hand KM, et al. A comparision of a1
-proteinase inhibitor, methoxysuccinyl-ala-ala-pro-val-chloromethylke-tone and specific b-lactam inhibitors in an acute model of human polymorphonuclear leukocyte elastase-induced lung hemorrhage in the hamster.Am Rev Respir Dis. 1990;141:672– 677
25. Kawabata K, Suzuki M, Sugitani M, Imaki K, Toda M, Miyamoto T. ONO-5046, a novel inhibitor of human neutrophil elastase.Biochem Biophys Res Commun. 1991;177:814 – 820
26. Forteza R, Botvinnikova Y, Ahmed A, et al. The interaction of a1-proteinase inhibitor and tissue kallikrein in controlling allergic ovine
airway hyperresponsiveness.Am J Respir Crit Care Med. 1996;154:36 – 42 27. McElvaney NG, Hubbard RC, Birrer P, et al. Aerosola1-antitrypsin
treatment for cystic fibrosis.Lancet. 1991;337:392–394
DEMAND-BASED MEDICINE
“We’re flying by the seat of our pants. But with severely ill kids, families want us to try something.”
Doctor quoted on giving Prozac to children. In: Strauch B. Use of anti-depression medicine for young patients has soared.New York Times. August 10, 1997.
DOI: 10.1542/peds.101.1.89
1998;101;89
Pediatrics
Marlene Rabinovitch
and
Edmond N. Kelly, Robert I. Koppel, Diane W. Cox, Shinya Ito, S. Lesley Chappel
Joseph A. Stiskal, Michael S. Dunn, Andrew T. Shennan, Karel K. E. O'Brien,
Prematurity: A Randomized, Controlled Trial
-Proteinase Inhibitor Therapy for the Prevention of Chronic Lung Disease of
1
α
Services
Updated Information &
http://pediatrics.aappublications.org/content/101/1/89
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/101/1/89#BIBL
This article cites 23 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/pulmonology_sub Pulmonology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.101.1.89
1998;101;89
Pediatrics
Marlene Rabinovitch
and
Edmond N. Kelly, Robert I. Koppel, Diane W. Cox, Shinya Ito, S. Lesley Chappel
Joseph A. Stiskal, Michael S. Dunn, Andrew T. Shennan, Karel K. E. O'Brien,
Prematurity: A Randomized, Controlled Trial
-Proteinase Inhibitor Therapy for the Prevention of Chronic Lung Disease of
1
α
http://pediatrics.aappublications.org/content/101/1/89
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.