O R I G I N A L R E S E A R C H
Evaluation of Exertional Ventilatory Parameters
Using Oscillometry in COPD
This article was published in the following Dove Press journal: International Journal of Chronic Obstructive Pulmonary Disease
Yuji Yamamoto Keisuke Miki Takanori Matsuki Kiyoharu Fukushima Yohei Oshitani Hiroyuki Kagawa Kazuyuki Tsujino Kenji Yoshimura Mari Miki Hiroshi Kida
Department of Respiratory Medicine, National Hospital Organization Osaka Toneyama Medical Center, Osaka, Japan
Background:Oscillometry is a tool to measure respiratory impedance that requires minimal
patients’effort. In patients with chronic obstructive pulmonary disease (COPD), the
correla-tion of respiratory impedance at rest with exercorrela-tional ventilatory parameters, including exercise tolerance, has scarcely been reported. In addition, the utility of oscillometric
parameters might differ between the inspiratory and expiratory phases due to airflow
obstruction during expiration, but the hypothesis had not been validated. The aim of the present study was to investigate whether oscillometric parameters are associated with exer-tional ventilatory parameters in patients with COPD.
Methods: Fifty-five subjects with COPD who attended clinics at the National Hospital Organization Osaka Toneyama Medical Center performed spirometry, oscillometry, and cardiopulmonary exercise testing (CPET) within 2 weeks. The correlations between
para-meters of spirometry, oscillometry, and CPET were analyzed using Spearman’s rank
correla-tion coefficient, univariate, and multivariate analyses.
Results: Respiratory reactance had better correlations with the CPET parameters than respiratory resistance. Moreover, inspiratory reactance at rest correlated with the CPET parameters stronger than expiratory reactance. In particular, inspiratory resonant frequency
(Fres-ins) correlated with peak oxygen uptake (rS=−0.549, p<0.01) and dead space to tidal
volume ratio at peak exercise (rS=0.677, p<0.01) and the best predicted expiratory tidal
volume (VTex) at peak exercise of all the oscillometric parameters (rS=−0.679, p<0.01).
However, the correlation between Fres-ins and VT ex at peak exercise became weak in
subjects with severe and very severe COPD during exercise.
Conclusion:Measurement of respiratory reactance is useful for the effortless evaluation of not only exertional ventilatory parameters but exercise tolerance in patients with COPD. The correlation of respiratory impedance with exertional ventilatory parameters can become weak in patients with advanced COPD; thus, the measurement of oscillometry might not be appropriate for evaluating exertional ventilatory parameters of patients with advanced COPD.
Keywords:dyspnea, dynamic hyperinflation, airflow obstruction, resonant frequency, tidal volume
Introduction
Globally, chronic obstructive pulmonary disease (COPD) is currently the third
leading cause of death and a major cause of morbidity.1 Improving exercise
tolerance or better physical activity would result in the better prognosis in COPD
patients.2Exercise tests, including 6-minute walk testing (6MWT) and
cardiopul-monary exercise testing (CPET), are the gold standard for evaluation of exercise
tolerance.3–5 6MWT is common and easier to perform than CPET, but CPET can
Correspondence: Keisuke Miki Department of Respiratory Medicine, National Hospital Organization Osaka Toneyama Medical Center, 5-1-1 Toneyama, Toyonaka, Osaka 560-8552, Japan
Tel +81-6-6853-2001 Fax +81-6-6853-3127
Email [email protected]
International Journal of Chronic Obstructive Pulmonary Disease
Dovepress
open access to scientific and medical research
Open Access Full Text Article
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
evaluate exertional ventilatory parameters more
precisely.4,5Often, however, the tests cannot be performed
in patients with dysmobility, making the evaluation of
exertional ventilatory parameters difficult. Therefore,
effortless evaluations of exertional ventilatory parameters are needed in the patients. As methods easy to evaluate exertional ventilatory parameters, pulmonary function tests, including spirometry and oscillometry, might be important.6,7
Oscillometry, which involves measurements of
within-breath changes in respiratory impedance, measures
respiratory resistance (Rrs) and respiratory reactance (Xrs). Rrs represents the sum of airway resistance and
viscous resistance of the lung and thoracic tissue,8 while
Xrs is considered to reflect the elastance and inertia of the
respiratory system.9 Measurement of respiratory
impe-dance using oscillometry is less time-consuming and
requires minimal patients’ cooperation.10 In fact,
oscillo-metry can be used to evaluate patients with severely advanced COPD who are unable to perform even
spirometry.10
In patients with COPD, Rrs and resonant frequency (Fres) correlate negatively and Xrs at a lower frequency of oscillation correlates positively with forced expiration
volume in 1 second (FEV1)/forced vital capacity (FVC)
ratio.11Since peripheral airway obstruction becomes more
severe during expiration,12these oscillometric parameters
change dynamically during respiratory cycle. In particular, Rrs becomes higher and Xrs shifts to a more negative
direction in the expiratory phase.13,14 Moreover, when
airflow obstruction develops, expiratory flow at a given
lung volume reaches its maximal value despite increasing
expiratory driving pressure; this is called expiratoryflow
limitation (EFL).15–17 EFL during exercise promotes
dynamic hyperinflation and contributes to a rapid and
shallow breathing pattern.15,18Xrs is normally thought to
reflect the elastic and inertial properties of the respiratory
system in patients without EFL.19 In patients with EFL,
however, oscillatory signals cannot pass through the points of airway obstruction and reach the alveoli; thus, Xrs
reflects the mechanical properties of airways proximal to
the choke points which are much stiffer than the periphery
and becomes more negative.19
As other pathophysiology in COPD patients,
ventila-tory inefficiency during exercise are reported.16,20 In
patients with ventilatory inefficiency, dead space to tidal
volume ratio (VD/VT) becomes higher during exercise.20–22
Ventilatory inefficiency is one of the components that
affect exercise tolerance in COPD,23 but the correlation
between ventilatory inefficiency and oscillometric
para-meters had not been investigated.
The above observations suggest that the utility of oscil-lometric parameters might differ between the inspiratory and expiratory phases. However, the association between each inspiratory and expiratory oscillometric parameter and ventilatory CPET parameters has never been thor-oughly investigated, although the association of
oscillome-try with 6MWT and CPET has been previously
reported.24,25 In addition, the utility of each oscillometric
parameter for evaluating and predicting exertional
ventila-tory parameters, including ventilaventila-tory inefficiency and
exercise tolerance, has not been investigated in patients with COPD. The information obtained from oscillometry might be clinically useful for assessing the mechanisms of exercise impairment and the effects of interventions.
The aims of the present study were as follows: (1) to investigate inspiratory and expiratory oscillometric meters that are associated with exertional ventilatory
para-meters in COPD patients; and (2) to confirm the utility of
oscillometry in COPD patients with various airflow
obstructions.
Methods
Subjects
A total of 105 patients with COPD who attended clinics at National Hospital Organization Osaka Toneyama Medical Center or participated in several ethically approved research studies on COPD, between August 2015 and July 2019 were screened in the study. The patients were
confirmed to have a FEV1/FVC ratio of <0.70 after using
a bronchodilator and were diagnosed with COPD based on their spirometry, smoking history, and symptoms including chronic cough, sputum, and dyspnea. The patients
there-fore satisfied the definition of the Global Initiative for
Chronic Obstructive Lung Disease (GOLD).26 Only
COPD patients who underwent spirometry, oscillometry, and CPET were included. Their drug regimens were not changed within 4 weeks before the measurements in this study. Patients were excluded if they were not clinically
stable or had exacerbations, defined as increased dyspnea
associated with a change in the quality and quantity of sputum, for at least three months before the present study. Patients were excluded if they had malignant tumors, severe heart disease, or bronchial asthma (ie a history of bronchial asthma, or respiratory symptoms that i) occur
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
variably over time and vary in intensity, ii) occur at night or on waking, or iii) are triggered by exercise, including
CPET). The qualified 55 symptomatic subjects who met
the study criteria [modified Medical Research Council
(MRC) dyspnea scale≥1] were evaluated using the
exam-inations described in the following sections.
Study Design
The subjects were evaluated using all three evaluation methods, oscillometry, spirometry, and CPET, within, at
most, a 2-week time period when the subjects’ clinical
symptoms were stable. If oscillometry and spirometry were performed on the same day, spirometry was
per-formed after oscillometry. Short-acting β2-agonists were
not used for more than 12 hours before these tests in all subjects. Long-acting antimuscarinic agents (LAMA) and
long-acting β2-agonists (LABA) were not withdrawn
before the measurements of oscillometry, spirometry, and CPET. The Institutional Review Board of National Hospital Organization Osaka Toneyama Medical Center approved the study protocols and chose an opt-out system
to obtain subjects’ informed consent (approval number,
TNH-2,019,037).
Measurement of Respiratory
Impedance Using Oscillometry
Respiratory impedance was measured at rest with broad-band oscillometry using a commercially available device (Mostgraph-01, Chest MI Co, Ltd, Tokyo, Japan). The methods were performed according to the standard
recommendations.8Partitioned (inspiratory and expiratory)
and average oscillometric parameters and were measured.
Differences between inspiratory and expiratory phases (Δ)
were calculated regarding all oscillometric parameters. As indicators of the frequency dependence of Rrs, Rrs at 5 and 20 Hz (R5 and R20, respectively) and the difference between R5 and R20 (R5-R20) were used. In addition, Xrs at 5 Hz (X5), Fres, and a low-frequency reactance area (ALX) were used as indicators of respiratory reactance. Fres indicates the point where Xrs becomes more domi-nated by inertial rather than elastic forces, and ALX is
defined as the integral of X5 to the Fres.
CPET
Symptom-limited exercise tests were performed using an electrically-braked cycle ergometer (CV-1000SS, Lode, Groningen, The Netherlands) using a CPET system
(Marquette CASE series T 2001, GE Healthcare, Tokyo, Japan; Aeromonitor AE 310S, Minato Medical Science
Co, Ltd, Osaka, Japan).5 First, pre-exercise resting
mea-surements were taken after reaching a steady-state period during at least 3 min of breathing through a mask. Next, incremental testing was performed by increasing 10W per 2 minutes. Before commencing the CPET, subjects were asked to put in maximum effort in the exercises performed during CPET. CPET was then performed until exhaustion without further encouragement, especially during exercise. The subjects were asked to maintain a cycle ergometer speed of about 60 rpm. The following CPET parameters
were measured: expiratory tidal volume (VTex), VD/VT,
mean expiratoryflow [VTex/expiratory time (Te)],
breath-ing frequency (fR), minute ventilation (V’E), V’E/V’CO2,
inspiratory duty cycle (Ti/Ttot), and oxygen uptake (V’O2).
These data were measured breath-by-breath and collected as 30 s averages at rest, during exercise at 2 min intervals, and at the end of exercise. In addition, dyspnea intensity
(10-point modified Borg category-ratio scale) was
evalu-ated at rest, at the last 15 s of each exercise stage, and at the end of exercise.
Spirometry
The subjects underwent spirometry using the CHESTAC 8800 spirometer (Chest MI, Inc, Tokyo, Japan) before
CPET according to the recommendations of the
American Thoracic Society.27 Predicted vital capacity
and predicted FEV1were calculated according to the
for-mula developed by the Japanese Respiratory Society.28
Statistical Analysis
The subjects were grouped into the GOLD stage I and II subgroup (Subgroup A) and the GOLD stage III and IV
subgroup (Subgroup B). The Mann–Whitney U-test was
used for comparison of various parameters among the
subgroups. Spearman’s rank correlation coefficient (rS)
and univariate analyses were used for bivariate correlation analysis of the parameters of respiratory impedance and CPET. Multiple stepwise linear regression analysis was performed to detect the variables of oscillometry that
were significant determinants of VT ex, VT ex/Te, fR,
V’E, and V’O2. After detecting the most significant oscillo-metric determinants, univariate and multivariate analyses were performed for interaction analyses. These statistical analyses were performed using EZR Version 1.38 (based
on R Version 3.5.2 and R commander Version 2.5–1,
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
Saitama, Japan).29 In all analyses, p<0.05 was taken to indicate statistical significance.
Results
Baseline Characteristics
Among 55 subjects included in the present study, 16 sub-jects were GOLD stage I or II and 39 subsub-jects were GOLD stage III or IV (Table 1). There were no differences between the subgroups in age, body mass index, and smoking history. As for oscillometry, expiratory impe-dance showed wider variation than inspiratory impeimpe-dance (Table 2). Resistance parameters, Fres, and ALX were higher and X5 was more negative in Subgroup B (Table
3 and Figure 1). Thus, respiratory impedance variously
correlated with the severity of airflow obstruction.
Regarding CPET (Table 4), V’O2at rest was higher in
Subgroup A (Table 5). At peak exercise, VTex, VTex/Te,
V’E, V’O2, and Ti/Ttot (p<0.01) were higher in Subgroup
A (Table 5). These data showed that Subgroup A had better exercise tolerance than Subgroup B. Moreover,
given that VD/VTat rest and peak exercise was higher in
Subgroup B (Table 5), the results showed ventilatory
inef-ficiency and low oxygen uptake during exercise in subjects
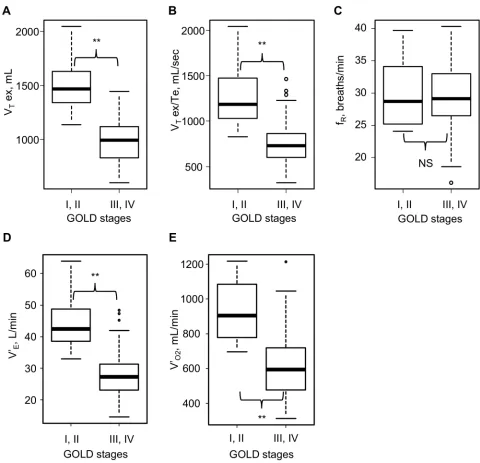
with severe airflow obstruction. However, no significant
difference was observed in fRbetween the two subgroups,
perhaps because of its wide variation (Figure 2). Whilst, fR
correlated positively with VTex/Te and V’Eat peak
exer-cise, but not with VT ex among all subjects
(Supplementary Figure 1).
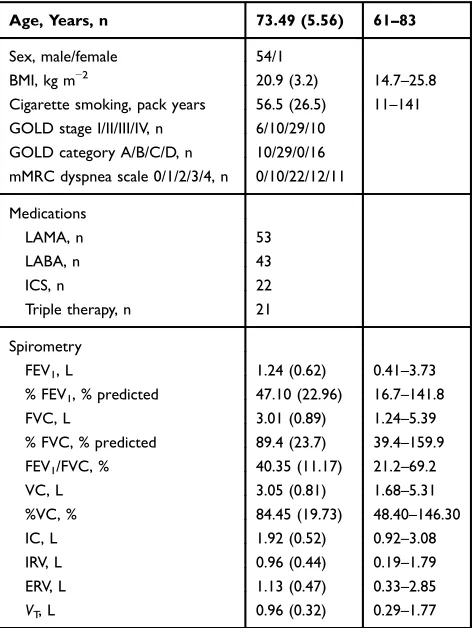
Table 1Subjects’Baseline Characteristics (n=55)
Age, Years, n 73.49 (5.56) 61–83
Sex, male/female 54/1
BMI, kg m−2 20.9 (3.2) 14.7–25.8
Cigarette smoking, pack years 56.5 (26.5) 11–141 GOLD stage I/II/III/IV, n 6/10/29/10
GOLD category A/B/C/D, n 10/29/0/16 mMRC dyspnea scale 0/1/2/3/4, n 0/10/22/12/11
Medications
LAMA, n 53
LABA, n 43
ICS, n 22
Triple therapy, n 21
Spirometry
FEV1, L 1.24 (0.62) 0.41–3.73
% FEV1, % predicted 47.10 (22.96) 16.7–141.8
FVC, L 3.01 (0.89) 1.24–5.39
% FVC, % predicted 89.4 (23.7) 39.4–159.9 FEV1/FVC, % 40.35 (11.17) 21.2–69.2
VC, L 3.05 (0.81) 1.68–5.31
%VC, % 84.45 (19.73) 48.40–146.30
IC, L 1.92 (0.52) 0.92–3.08
IRV, L 0.96 (0.44) 0.19–1.79
ERV, L 1.13 (0.47) 0.33–2.85
VT, L 0.96 (0.32) 0.29–1.77
Note:Data are presented as the mean (SD) and the minimum and maximum values, unless otherwise stated.
Abbreviations:BMI, body mass index; ERV, expiratory reserve volume; FEV1,
forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; IC, inspiratory capacity; ICS, inhaled corticosteroids; IRV, inspiratory reserve volume; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; mMRC dyspnea scale, modified Medical Research Council dyspnea scale; SD, standard deviation; VC, vital capacity; VT, tidal volume.
Table 2 Results of Baseline Respiratory Impedance at Rest (n=55)
R5, cmH2O/L/s
Inspiratory 3.62 (1.30) 1.20–6.96 Expiratory 4.88 (2.19) 1.53–13.83
Average 4.25 (1.64) 1.54–10.04
ΔR5 −1.26 (1.50) −7.59–1.19
R20, cmH2O/L/s
Inspiratory 2.74 (0.80) 1.13–4.75 Expiratory 3.32 (1.28) 1.44–7.94
Average 3.03 (0.96) 1.49–6.08
ΔR20 −0.58 (0.91) −3.76–0.77
R5-R20, cmH2O/L/s
Inspiratory 0.89 (0.60) −0.07–2.80 Expiratory 1.56 (0.99) 0.01–5.89
Average 1.23 (0.74) 0.01–3.96
ΔR5-R20 −0.68 (0.71) −3.86–0.52
X5, cmH2O/L/s
Inspiratory −1.29 (0.85) −3.55 -−0.16 Expiratory −3.64 (3.12) −12.56 -−0.08 Average −2.47 (1.89) −7.54 -−0.13
ΔX5 2.36 (2.58) −0.16–10.05
Fres, Hz
Inspiratory 14.53 (5.81) 5.91–30.60 Expiratory 20.08 (7.81) 5.56–34.28
Average 17.31 (6.47) 5.74–32.18
ΔFres −5.55 (4.65) −18.51–1.04
ALX, cmH2O/L/s × Hz
Inspiratory 9.32 (9.12) 0.54–42.08 Expiratory 33.74 (33.57) 0.29–145.30
Average 21.53 (20.14) 0.46–83.41
ΔALX −24.41 (28.24) −123.78–0.92
Note:Data are presented as the mean (SD) and the minimum and maximum values, unless otherwise stated.
Abbreviations:ALX, low-frequency reactance area;Δ, difference between inspira-tory and expirainspira-tory phases; Fres, resonant frequency; R5 and R20, respirainspira-tory system resistance at 5 and 20 Hz, respectively; SD, standard deviation; X5, respira-tory system reactance at 5 Hz.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
Identi
fi
cation of Oscillometric
Parameters That Best Predicted
CPET Parameters
Univariate analyses showed that respiratory resistance at rest hardly correlated with CPET parameters at rest, and
inspiratory reactance at rest correlated with VTex, VTex/Te,
V’E, and V’O2 at rest (Table 6). However, oscillometric
parameters at rest variously correlated with CPET
para-meters at peak exercise except for fR (Table 7 and
Supplementary Table 1). Moreover, VTex, VTex/Te, V’E,
and V’O2showed a stronger correlation with parameters of
reactance than resistance, and all the inspiratory oscillo-metric parameters showed stronger correlation with these CPET parameters than expiratory oscillometric parameters. In addition, multiple stepwise linear regression analysis determined Fres-ins as the parameter with the strongest
correlation with VT ex, VT ex/Te, V’E, and V’O2
(Supplementary Table 2). Therefore, Fres-ins was detected
as the most significant determinant of exertional ventilatory
parameters, including exercise tolerance. However, the cor-relation of exertional ventilatory parameters with Fres-ins
was weaker than that with FEV1, which included the
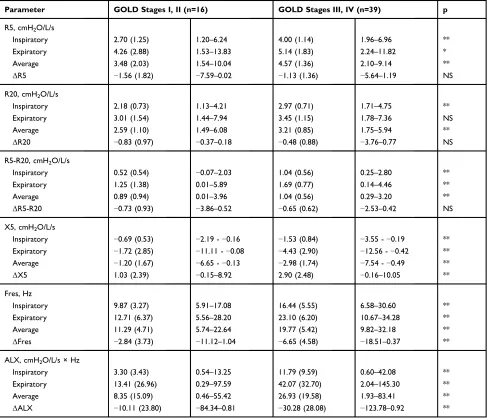
Table 3Results of Baseline Respiratory Impedance at Rest in the Various GOLD Stages (Stages I–IV) (n=55)
Parameter GOLD Stages I, II (n=16) GOLD Stages III, IV (n=39) p
R5, cmH2O/L/s
Inspiratory 2.70 (1.25) 1.20–6.24 4.00 (1.14) 1.96–6.96 **
Expiratory 4.26 (2.88) 1.53–13.83 5.14 (1.83) 2.24–11.82 *
Average 3.48 (2.03) 1.54–10.04 4.57 (1.36) 2.10–9.14 **
ΔR5 −1.56 (1.82) −7.59–0.02 −1.13 (1.36) −5.64–1.19 NS
R20, cmH2O/L/s
Inspiratory 2.18 (0.73) 1.13–4.21 2.97 (0.71) 1.71–4.75 **
Expiratory 3.01 (1.54) 1.44–7.94 3.45 (1.15) 1.78–7.36 NS
Average 2.59 (1.10) 1.49–6.08 3.21 (0.85) 1.75–5.94 **
ΔR20 −0.83 (0.97) −0.37–0.18 −0.48 (0.88) −3.76–0.77 NS
R5-R20, cmH2O/L/s
Inspiratory 0.52 (0.54) −0.07–2.03 1.04 (0.56) 0.25–2.80 **
Expiratory 1.25 (1.38) 0.01–5.89 1.69 (0.77) 0.14–4.46 **
Average 0.89 (0.94) 0.01–3.96 1.04 (0.56) 0.29–3.20 **
ΔR5-R20 −0.73 (0.93) −3.86–0.52 −0.65 (0.62) −2.53–0.42 NS
X5, cmH2O/L/s
Inspiratory −0.69 (0.53) −2.19 -−0.16 −1.53 (0.84) −3.55 -−0.19 **
Expiratory −1.72 (2.85) −11.11 -−0.08 −4.43 (2.90) −12.56 -−0.42 **
Average −1.20 (1.67) −6.65 -−0.13 −2.98 (1.74) −7.54 -−0.49 **
ΔX5 1.03 (2.39) −0.15–8.92 2.90 (2.48) −0.16–10.05 **
Fres, Hz
Inspiratory 9.87 (3.27) 5.91–17.08 16.44 (5.55) 6.58–30.60 **
Expiratory 12.71 (6.37) 5.56–28.20 23.10 (6.20) 10.67–34.28 **
Average 11.29 (4.71) 5.74–22.64 19.77 (5.42) 9.82–32.18 **
ΔFres −2.84 (3.73) −11.12–1.04 −6.65 (4.58) −18.51–0.37 **
ALX, cmH2O/L/s × Hz
Inspiratory 3.30 (3.43) 0.54–13.25 11.79 (9.59) 0.60–42.08 **
Expiratory 13.41 (26.96) 0.29–97.59 42.07 (32.70) 2.04–145.30 **
Average 8.35 (15.09) 0.46–55.42 26.93 (19.58) 1.93–83.41 **
ΔALX −10.11 (23.80) −84.34–0.81 −30.28 (28.08) −123.78–0.92 **
Notes:Data are presented as the mean (SD) and the minimum and maximum values, unless otherwise stated. *and **p<0.05 and p<0.01 by the Mann–WhitneyU-test, respectively.
Abbreviations:ALX, low-frequency reactance area;Δ, difference between inspiratory and expiratory phases; Fres, resonant frequency; GOLD, Global Initiative For Chronic Obstructive Lung Disease; NS, not significant; R5 and R20, respiratory system resistance at 5 and 20 Hz, respectively; SD, standard deviation; X5, respiratory system reactance at 5 Hz.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
correlation of FEV1with V’O2(rS=0.823, p<0.01) and that with V’E(rS=0.903, p<0.01) (Table 7).
Analysis Between Fres-Ins at Rest
and CPET Parameters
Comparing CPET parameters at rest with those at peak
exercise, VTex, VTex/Te, V’E, and V’O2showed stronger
correlations with Fres-ins at peak exercise than at rest (Figure 3). Regarding analyses of fRand Fres-ins, statistical signifi -cance was not observed at either rest or at peak exercise.
Moreover, the differences of CPET parameters between at peak exercise and at rest correlated with Fres-ins, including VTex (rS=−0.571, p<0.01), VTex/Te (rS=−0.598, p<0.01), V’E (rS=−0.555, p<0.01), and V’O2 (rS=−0.558, p<0.01).
This indicated the statistically more significant difference in
correlation coefficients at peak exercise compared with at
rest during CPET. Therefore, during exercise, the correlation between Fres-ins at rest and CPET parameters became stronger.
In addition, Fres-ins correlated with an index of the ventilatory inefficiency: VD/VTat peak exercise (rS=0.677,
Figure 1Inspiratory impedance at rest in the various GOLD stages (stages I–IV) (n=55). (A) Respiratory resistance and GOLD stages at baseline. (B) Respiratory reactance and GOLD stages at baseline. Sixteen subjects were GOLD stage I or II and 39 subjects were GOLD stage III or IV. **p<0.01 by the Mann–WhitneyU-test.
Abbreviations:ALX, low-frequency reactance area; Fres, resonant frequency; GOLD, Global Initiative for Chronic Obstructive Lung Disease; R5 and R20, respiratory system resistance at 5 and 20 Hz, respectively; X5, respiratory system reactance at 5 Hz.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
p<0.01). However, FEV1 correlated with VD/VT at peak
exercise stronger than Fres-ins (rS=−0.715, p<0.01)
(Table 7).
Correlation Between Fres-Ins at
Rest and CPET Parameters at Peak
Exercise
As indicated by the scatter plots of Fres-ins and VTex, VT
ex/Te, V’E, and V’O2(Figure 3), the correlations between
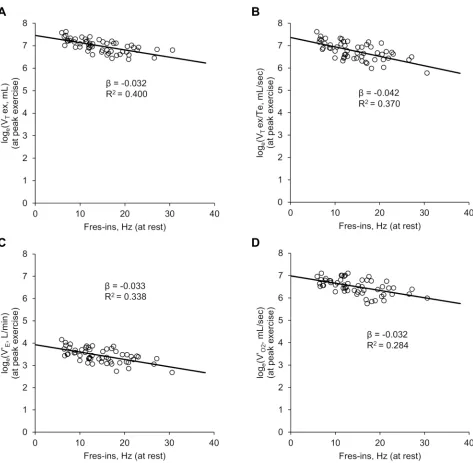
the various parameters can be considered nonlinear and exponential. Therefore, analyses between Fres-ins and the natural logarithms of these CPET parameters were per-formed. Fres-ins correlated negatively and linearly with the natural logarithms of the CPET parameters (Figure 4).
Combined with the results of Figure 1, which indicated
that Fres-ins correlated positively with the GOLD stages, these analyses using logarithmic conversion implied that the correlation between Fres-ins and the CPET parameters becomes weak in advanced stages of COPD.
Discussion
The present study highlights four majorfindings regarding
the correlation between respiratory impedance and exer-tional ventilatory parameters: 1) inspiratory rather than expiratory oscillometric parameters correlated with exer-tional ventilatory parameters stronger; 2) Fres-ins at rest correlated with exertional ventilatory parameters and
reflected exercise tolerance in COPD subjects; 3)
Fres-ins correlated with ventilatory inefficiency during exercise;
and 4) the correlation between respiratory impedance and
Table 4Results of Cardiopulmonary Exercise Testing at Peak Exercise and at Rest (n=55)
At Peak Exercise At Rest
Incremental load testing
VTex, mL 1132 (332) 597–2047 696 (169) 354–1192
VTex/Te, mL/sec 924 (363) 322–2043 370 (90) 175–660
fR, breaths/min 29 (5) 16–40 21 (6) 8–32
V’E, L/min 33.0 (10.6) 14.6–63.9 13.7 (2.5) 6.8–19.1
Ti/Ttot 0.38 (0.08) 0.24–0.68 0.37 (0.07) 0.22–0.62
V’O2, mL/min 711 (236) 313–1218 249 (45) 171–361
VD/VT 0.40 (0.05) 0.31–0.50 0.44 (0.04) 0.38–0.54
V’E/V’CO2 46.6 (7.6) 33.3–72.3 61.6 (8.6) 46.5–81.9
Note:Data are presented as the mean (SD) and the minimum and maximum values, unless otherwise stated.
Abbreviations:fR, breathing frequency; SD, standard deviation; Te, expiration time; Ti/Ttot, inspiratory duty cycle; VD, physiological dead space; VD/VT, dead space to tidal
volume ratio; V’E, minute ventilation; V’E/V’CO2, ventilatory equivalent for carbon dioxide; V’O2, oxygen uptake; VT, tidal volume; VTex, expiratory tidal volume; VTex/Te,
mean expiratoryflow.
Table 5Results of Cardiopulmonary Exercise Testing (CPET) at Rest and at Peak Exercise in Various GOLD Stages (Stages I–IV) (n=55)
GOLD Stages I, II (n=16) GOLD Stages III, IV (n=39)
At peak exercise At rest At peak exercise At rest
Incremental load testing
VTex, mL 1515 (246)* 1137–2047 739 (145) 488–935 975 (214) 597–1445 679 (177) 354–1192 VTex/Te, mL/sec 1297 (296)* 927–2043 383 (56) 292–467 771 (265) 322–1464 366 (102) 175–660
fR, breath/min 29 (5) 24–40 20 (4) 14–27 29 (5) 16–40 21 (6) 8–32
V’E, L/min 44.1 (8.3)* 33.0–63.9 14.1 (2.0) 10.4–17.6 28.5 (7.9) 14.6–48.3 13.6 (2.8) 6.8–19.1 Ti/Ttot 0.43 (0.06)* 0.35–0.60 0.38 (0.07) 0.30–0.62 0.36 (0.09) 0.24–0.68 0.36 (0.08) 0.22–0.62 V’O2, mL/min 928 (168)* 696–1218 270 (45)* 171–361 622 (201) 313–1214 240 (42) 173–327 VD/VT 0.35 (0.03)* 0.31–0.40 0.42 (0.04)* 0.38–0.49 0.42 (0.04) 0.34–0.50 0.45 (0.04) 0.38–0.54 V’E/V’CO2 44.9 (6.1) 36.0–54.4 59.5 (8.5) 46.5–78.3 47.2 (8.1) 37.0–72.3 62.5 (8.6) 46.6–81.9
Notes:Data are presented as the mean (SD) and the minimum and maximum values, unless otherwise stated. *p<0.05 by the Mann–WhitneyU-test comparing with each CPET parameter of subjects with GOLD stages III and IV.
Abbreviations:CPET, cardiopulmonary exercise testing; fR, breathing frequency; GOLD, Global Initiative for Chronic Obstructive Lung Disease; SD, standard deviation; Te,
expiratory time; Ti/Ttot, inspiratory duty cycle; VD, physiological dead space; VD/VT, dead space to tidal volume ratio; V’E, minute ventilation; V’E/V’CO2, ventilatory
equivalent for carbon dioxide; V’O2, oxygen uptake; VT, tidal volume; VTex, expiratory tidal volume; VTex/Te; mean expiratoryflow.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
exertional ventilatory parameters became weak in subjects
with severe airflow obstruction. To the best of our
knowl-edge, this is thefirst study to evaluate exertional
ventila-tory parameters using respiraventila-tory impedance at rest. In COPD patients, inspiratory reactance at rest, parti-cularly Fres-ins, better correlated with ventilatory para-meters at peak exercise than those at rest. During exercise, due to the combination of decreased elastic recoil pressure and increased airway resistance, patients with
COPD require a longer expiratory time to enable complete
expiration of tidal volume.30 However, the simultaneous
increase in fR results in a short expiratory time, which is
insufficient for COPD patients to exhale their entire tidal
volume due to airflow obstruction, leading to dynamic
hyperinflation.18 Accordingly, oscillometric parameters
correlate variously with spirometric parameters including
FEV1,31which reflects the severity of airflow obstruction.
However, oscillometry has not been considered a surrogate
Figure 2Results of cardiopulmonary exercise testing at peak exercise in the various GOLD stages (stages I–IV) (n=55). (A) Expiratory tidal volume at peak exercise in the various GOLD stages. (B) Mean expiratoryflow (VTex/Te) at peak exercise in the various GOLD stages. (C) Breathing frequency (fR) at peak exercise in the various GOLD
stages. (D) Minute ventilation (V’E) at peak exercise in the various GOLD stages. (E) Oxygen uptake (V’O2) at peak exercise in the various GOLD stages. **p<0.01 by the Mann–WhitneyU-test.
Abbreviations:fR, breathing frequency; GOLD, Global Initiative for Chronic Obstructive Lung Disease; NS, not significant by the Mann–WhitneyU-test; V’E, minute
ventilation; V’O2, oxygen uptake;VTex, expiratory tidal volume;VTex/Te, mean expiratoryflow.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
test for spirometry, because these tests do not necessarily evaluate the same breathing conditions and each oscillo-metric parameter reportedly only fairly or moderately
cor-relates with spirometric parameters.31,32 Therefore, the
correlations between oscillometry and exertional ventila-tory parameters also seemed to be moderate. Nevertheless, we assessed the utility of oscillometry because it is parti-cularly useful for assessing the respiratory pathophysiol-ogy of COPD and for evaluating the exertional ventilatory parameters of patients who are unable to perform even spirometry.
This study suggested that inspiratory impedance at rest correlates with exertional ventilatory parameters of CPET better than does expiratory impedance. Inspiratory rather than expiratory oscillometric parameters were reportedly
less variable.7Airways tend to open during inspiration and
the pressure pulses can be transmitted to the periphery, but
airflow obstruction during expiration was suggested to
occur with inhomogeneity in the lung.7,33 Hence, the
more variability of expiratory oscillometric parameters
was probably due to the inhomogeneity of airflow
obstruction.7In addition, in patients with COPD, loss of
lung elastic recoil causes EFL, and more negative ΔX5
and higher inspiratory X5 were considered to predict the
presence of EFL.19,34,35 Therefore, subjects in Subgroup
B were estimated to have developed EFL compared with Subgroup A subjects (Table 3). Given that the correlation of Fres-ins with CPET parameters became weak in advanced COPD subjects (Figure 4), EFL and/or dynamic
hyperinflation might potentially have associated with the
inhomogeneity of airflow obstruction. Therefore,
inspira-tory impedance might be a more useful parameter for evaluating exertional ventilatory parameters in patients with COPD. In addition, oscillometry might be useful for
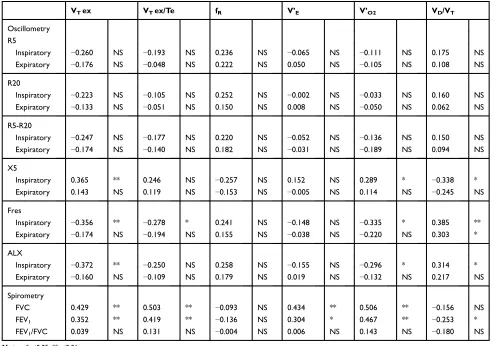
Table 6 Spearman’s Rank Correlation Coefficient Between Parameters of Respiratory Impedance at Rest, Spirometry, and Cardiopulmonary Exercise Testing at Rest (n=55)
VTex VTex/Te fR V’E V’O2 VD/VT
Oscillometry R5
Inspiratory −0.260 NS −0.193 NS 0.236 NS −0.065 NS −0.111 NS 0.175 NS
Expiratory −0.176 NS −0.048 NS 0.222 NS 0.050 NS −0.105 NS 0.108 NS
R20
Inspiratory −0.223 NS −0.105 NS 0.252 NS −0.002 NS −0.033 NS 0.160 NS
Expiratory −0.133 NS −0.051 NS 0.150 NS 0.008 NS −0.050 NS 0.062 NS
R5-R20
Inspiratory −0.247 NS −0.177 NS 0.220 NS −0.052 NS −0.136 NS 0.150 NS
Expiratory −0.174 NS −0.140 NS 0.182 NS −0.031 NS −0.189 NS 0.094 NS
X5
Inspiratory 0.365 ** 0.246 NS −0.257 NS 0.152 NS 0.289 * −0.338 *
Expiratory 0.143 NS 0.119 NS −0.153 NS −0.005 NS 0.114 NS −0.245 NS
Fres
Inspiratory −0.356 ** −0.278 * 0.241 NS −0.148 NS −0.335 * 0.385 **
Expiratory −0.174 NS −0.194 NS 0.155 NS −0.038 NS −0.220 NS 0.303 *
ALX
Inspiratory −0.372 ** −0.250 NS 0.258 NS −0.155 NS −0.296 * 0.314 *
Expiratory −0.160 NS −0.109 NS 0.179 NS 0.019 NS −0.132 NS 0.217 NS
Spirometry
FVC 0.429 ** 0.503 ** −0.093 NS 0.434 ** 0.506 ** −0.156 NS
FEV1 0.352 ** 0.419 ** −0.136 NS 0.304 * 0.467 ** −0.253 *
FEV1/FVC 0.039 NS 0.131 NS −0.004 NS 0.006 NS 0.143 NS −0.180 NS
Notes:*p<0.05; **p<0.01.
Abbreviations:ALX, low-frequency reactance area; FEV1, forced expiratory volume in 1 second; fR, breathing frequency; Fres, resonant frequency; FVC, forced vital
capacity; NS, not significant; R5 and R20, respiratory system resistance at 5 and 20 Hz, respectively; Te, expiratory time; V’E, minute ventilation; V’O2, oxygen uptake; VTex,
expiratory tidal volume; VTex/Te, mean expiratoryflow; X5, respiratory system reactance at 5 Hz.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
detecting the inhomogeneity of airflow obstruction in COPD. Further investigations are necessary to validate the hypothesis.
The present study indicated that Fres-ins was the best
oscillometric parameter for predicting V’O2 and V’E at
peak exercise. Given the stronger correlation between
Fres-ins at rest and VT ex at peak exercise than that
between Fres-ins at rest and VT ex at rest (Figure 3),
respiratory reactance at rest might correlate with the
degree of VT expansion. Consequently, Fres-ins might
have correlated with V’O2at peak exercise, which is
cal-culated using V’E: the product of VTex and fR. Given that
changes in X5 and Fres related to small airway
broncho-dilation in COPD,36 Fres-ins might have reflected airway
obstruction and correlated with VTex. Further studies to
assess the correlation of Fres-ins with VT ex might be
necessary. The present study suggested that respiratory
impedance measured by oscillometry, particularly respira-tory reactance at rest, is useful for evaluating exertional
ventilatory parameters quantitatively and can be
a complementary tool for predicting exercise tolerance, although the utility of oscillometry was not better than that of spirometry.
In addition, the present study suggested that respiratory
reactance correlated with ventilatory inefficiency. In
Subgroup B, increased VD/VT at peak exercise showed
ventilatory inefficiency during exercise (Table 5). This
was also supported by the prolonged expiratory time and the shallow breathing pattern (Table 5). Moreover, the
correlation between Fres-ins and VD/VT indicated that
Fres-ins might be used as a surrogate marker for
ventila-tory inefficiency during exercise because VD/VT is
a common marker of ventilatory inefficiency.16,20
Fres-ins might potentially be useful as an index easy to measure
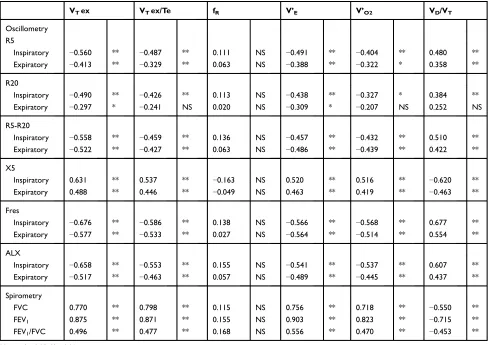
Table 7 Spearman’s Rank Correlation Coefficient Between Parameters of Respiratory Impedance at Rest, Spirometry, and Cardiopulmonary Exercise Testing at Peak Exercise (n=55)
VTex VTex/Te fR V’E V’O2 VD/VT
Oscillometry R5
Inspiratory −0.560 ** −0.487 ** 0.111 NS −0.491 ** −0.404 ** 0.480 **
Expiratory −0.413 ** −0.329 ** 0.063 NS −0.388 ** −0.322 * 0.358 **
R20
Inspiratory −0.490 ** −0.426 ** 0.113 NS −0.438 ** −0.327 * 0.384 **
Expiratory −0.297 * −0.241 NS 0.020 NS −0.309 * −0.207 NS 0.252 NS
R5-R20
Inspiratory −0.558 ** −0.459 ** 0.136 NS −0.457 ** −0.432 ** 0.510 **
Expiratory −0.522 ** −0.427 ** 0.063 NS −0.486 ** −0.439 ** 0.422 **
X5
Inspiratory 0.631 ** 0.537 ** −0.163 NS 0.520 ** 0.516 ** −0.620 **
Expiratory 0.488 ** 0.446 ** −0.049 NS 0.463 ** 0.419 ** −0.463 **
Fres
Inspiratory −0.676 ** −0.586 ** 0.138 NS −0.566 ** −0.568 ** 0.677 **
Expiratory −0.577 ** −0.533 ** 0.027 NS −0.564 ** −0.514 ** 0.554 **
ALX
Inspiratory −0.658 ** −0.553 ** 0.155 NS −0.541 ** −0.537 ** 0.607 **
Expiratory −0.517 ** −0.463 ** 0.057 NS −0.489 ** −0.445 ** 0.437 **
Spirometry
FVC 0.770 ** 0.798 ** 0.115 NS 0.756 ** 0.718 ** −0.550 **
FEV1 0.875 ** 0.871 ** 0.155 NS 0.903 ** 0.823 ** −0.715 **
FEV1/FVC 0.496 ** 0.477 ** 0.168 NS 0.556 ** 0.470 ** −0.453 **
Notes:*p<0.05; **p<0.01.
Abbreviations:ALX, low-frequency reactance area; fR, breathing frequency; FEV1, forced expiratory volume in 1 second; Fres, resonant frequency; FVC, forced vital
capacity; NS, not significant; R5 and R20, respiratory system resistance at 5 and 20 Hz, respectively; Te, expiratory time; V’E, minute ventilation; V’O2, oxygen uptake; VTex,
expiratory tidal volume; VTex/Te, mean expiratoryflow; X5, respiratory system reactance at 5 Hz.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
for adding or choosing interventions to improve
ventila-tory inefficiency in patients with COPD, although further
studies are needed.37 The present studyfirst showed that
oscillometric parameters correlated with ventilatory ineffi
-ciency during exercise and indicated the potential role of respiratory impedance for effortlessly assessing exertional ventilatory parameters qualitatively in COPD patients.
The correlation between respiratory impedance and exertional ventilatory parameters can become weak in
patients with advanced COPD. In the present study, the
more reducedVTex/Te in Subgroup B implied that airflow
obstruction during exercise became more severe (Table 5). Moreover, as described above, subjects in Subgroup B were estimated to have developed more severe EFL than those in Subgroup A. In addition, the exponential correlations between Fres-ins at rest and CPET parameters at peak exercise showed that the correlations between oscillometry and CPET became weak in COPD subjects
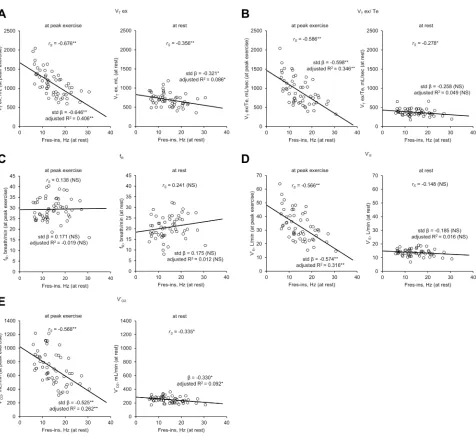
Figure 3Results of univariate analyses and Spearman’s rank correlation coefficient analyses between inspiratory resonant frequency (Fres-ins) at rest and ventilatory parameters of cardiopulmonary exercise testing (CPET) (n=55). In eachfigure, the graphs on the left show the results of Fres-ins at rest and CPET ventilatory parameters at peak exercise, while those on the right show the results of Fres-ins at rest and ventilatory parameters at rest, respectively. (A) Fres-ins and expiratory tidal volume (VTex).
(B) Fres-ins and mean expiratoryflow (VTex/Te). (C) Fres-ins and breathing frequency (fR). (D) Fres-ins and minute ventilation (V’E). (E) Fres-ins and oxygen uptake (V’O2).
*p<0.05; **p<0.01.
Abbreviations:CPET, cardiopulmonary exercise testing; fR, breathing frequency; Fres-ins, inspiratory resonant frequency; NS, not significant; R 2
, R-squared; rS, Spearman’s
rank correlation coefficient; stdβ, standardized regression coefficient estimate; V’E, minute ventilation; V’O2, oxygen uptake; VTex, expiratory tidal volume; VTex/Te, mean
expiratoryflow.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
with severe airflow obstruction (Figure 4). Given these results, oscillometry might not be appropriate for evaluat-ing exertional ventilatory parameters in advanced COPD patients with EFL because wide variations in respiratory reactance level at rest decrease the accuracy of evaluation. The present study included a small number of subjects and was a single-center study; thus, further investigations are
needed to validate the hypothesis and to verify the clinical utility of oscillometry in patients with advanced COPD.
The present study had some limitations. First, it was a single-center investigation and some selection bias might
have affected the findings. Second, this study included
a small number of subjects. In particular, only one female subject was included in the study. In addition, the number
Figure 4Results of Spearman’s rank correlation coefficient and univariate analyses of the correlation between inspiratory resonant frequency (Fres-ins) at rest and ventilatory parameters of cardiopulmonary exercise testing (CPET) at peak exercise (n=55).Interaction analyses were performed for Fres-ins and natural logarithms of exertional ventilatory parameters of CPET. All the analyses were statistically significant (p<0.01). (A) Fres-ins and expiratory tidal volume (VTex). (B) Fres-ins and mean
expiratoryflow (VTex/Te). (C) Fres-ins and minute ventilation (V’E). (D) Fres-ins and oxygen uptake (V’O2).
Abbreviations:β, unstandardized regression coefficient estimate; CPET, cardiopulmonary exercise testing; Fres-ins, inspiratory resonant frequency; R2, R-squared; V’E, minute ventilation; V’O2, oxygen uptake; VTex, expiratory tidal volume; VTex/Te, mean expiratoryflow.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
of COPD subjects with each GOLD stage was small. Hence, a larger study population is required to validate the results. Third, this study did not include a healthy control group because only symptomatic subjects who underwent oscillometry, spirometry, and CPET were eval-uated retrospectively.
In conclusion, respiratory reactance at rest, particularly Fres-ins, was able to estimate exertional ventilatory para-meters of CPET. Inspiratory reactance is useful for effort-lessly predicting exertional ventilatory parameters both quantitatively and qualitatively in patients with COPD, but oscillometry might not be appropriate to evaluate exertional ventilatory parameters in patients with advanced COPD with EFL. Further investigations of oscillometry to accurately evaluate exertional ventilatory parameters and to improve the clinical utility are necessary.
Abbreviations
ALX, low-frequency reactance area; β, unstandardized
regression coefficient estimate; BMI, body mass index;
COPD, chronic obstructive pulmonary disease; CPET,
car-diopulmonary exercise testing; Δ, difference between
inspiratory and expiratory phases; ERV, expiratory reserve
volume; FEV1, forced expiratory volume in 1 second; fR,
breathing frequency; Fres, resonant frequency; Fres-ins inspiratory resonant frequency; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; IC, inspiratory capacity; ICS, inhaled corticoster-oids; IRV, inspiratory reserve volume; LABA, long-acting
β2-agonists; LAMA, long-acting muscarinic antagonists;
R2, R-squared; R20, respiratory resistance (Rrs) at 20
Hz; R5, Rrs at 5 Hz; R5-R20, difference between R5 and
R20; Rrs, respiratory resistance; rS, Spearman’s rank
cor-relation coefficient; SD, standard deviation; stdβ,
standar-dized regression coefficient estimate; Te, expiratory time;
Ti/Ttot, inspiratory duty cycle; VC, vital capacity; VD,
physiological dead space; VD/VT, dead space to tidal
volume ratio; V’E, minute ventilation; V’E/V’CO2,
ventila-tory equivalent for carbon dioxide; V’O2, oxygen uptake;
VT, tidal volume; VTex, expiratory tidal volume; VTex/
Te, mean expiratory flow; X5, respiratory reactance (Xrs)
at 5 Hz; X5-ins, inspiratory X5; Xrs, respiratory reactance.
Data Sharing Statement
All data generated or analyzed during this study are
included in this published article and its supplementary
material file.
Ethics Approval and Consent to
Participate
The present study was conducted according to the princi-ples of the Declaration of Helsinki and was approved by the ethics committee of NHO Osaka Toneyama Medical
Center (approval number, TNH-2,019,037). The
Institutional Review Board of NHO Osaka Toneyama
Medical Center chose an opt-out system to obtain subjects’
informed consent.
Acknowledgments
The authors would like to thank Ms S Ito, Ms S Sakaguchi and Mr T Uenishi for their help with the CPET measurements.
Author Contributions
YY contributed to conceptualizing and designing the study, data collection and analysis, and wrote the manu-script. KM cared for all the subjects, contributed to con-ceptualizing and designing the study, data analyses, and revision of the manuscript. TM, KF, YO, HK, KT, and KY contributed to collecting subject data and revising the manuscript. MM and HK contributed to data interpretation and design of the study. All the authors reviewed and
approved the submission of thefinal manuscript.
Funding
The authors received no specific funding for the present
study.
Disclosure
The authors declare no conflicts of interest in association
with the present study.
References
1. GBD 2017. Causes of death collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392 (10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7.
2. Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study.Chest.2011;140(2):331–342. doi:doi:10.1378/chest.10-2521 3. ATS Committee on Proficiency Standards for Clinical Pulmonary
Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102.
4. American Thoracic Society, American College of Chest Physicians. ATS/ACCP statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;167(2):211–277. doi:10.116 4/rccm.167.2.211.
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
5. Puente-Maestu L, Palange P, Casaburi R, et al. Use of exercise testing in the evaluation of interventional efficacy: an official ERS statement.
Eur Respir J.2016;47(2):429–460. doi:doi:10.1183/13993003.00745-2015
6. Diaz O, Villafranca C, Ghezzo H, et al. Role of inspiratory capacity on exercise tolerance in COPD patients with and without tidal expiratory flow limitation at rest. Eur Respir J. 2000;16 (2):269–275. doi:10.1034/j.1399-3003.2000.16b14.x
7. Kubota M, Shirai G, Nakamori T, Kokubo K, Masuda N, Kobayashi H. Low frequency oscillometry parameters in COPD patients are less variable during inspiration than during expiration.
Respir Physiol Neurobiol. 2009;166(2):73–79. doi:10.1016/j. resp.2009.01.007
8. Oostveen E, MacLeod D, Lorino H, et al. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur Respir J. 2003;22(6):1026–1041. doi:10.1183/09031936.03.00089403
9. Bickel S, Popler J, Lesnick B, Eid N. Impulse oscillometry: inter-pretation and practical applications. Chest. 2014;146(3):841–847. doi:10.1378/chest.13-1875
10. Tse HN, Tseng CZS, Wong KY, Yee KS, Ng LY. Accuracy of forced oscillation technique to assess lung function in geriatric COPD population.Int J Chron Obstruct Pulmon Dis.2016;11:1105–1118. doi:10.2147/COPD.S102222
11. Cavalcanti JV, Lopes AJ, Jansen JM, Melo PL. Detection of changes in respiratory mechanics due to increasing degrees of airway obstruc-tion in asthma by the forced oscillaobstruc-tion technique. Respir Med. 2006;100(12):2207–2219. doi:10.1016/j.rmed.2006.03.009
12. McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction and emphysema in chronic obstructive pulmonary disease.N Engl J Med.2011;365(17):1567–1575. doi:10.1056/NEJMoa1106955 13. Paredi P, Goldman M, Alamen A, et al. Comparison of inspiratory
and expiratory resistance and reactance in patients with asthma and chronic obstructive pulmonary disease.Thorax.2010;65(3):263–267. doi:10.1136/thx.2009.120790
14. Yamauchi Y, Kohyama T, Jo T, Nagase T. Dynamic change in respiratory resistance during inspiratory and expiratory phases of tidal breathing in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2012;7:259–269. doi:10.2147/COPD.S30399
15. Calverley PMA. Flow limitation and dynamic hyperinflation: key concepts in modern respiratory physiology. Eur Respir J. 2005;25 (1):186–199. doi:10.1183/09031936.04.00113204
16. O’Donnell DE, Elbehairy AF, Faisal A, Webb KA, Neder JA, Mahler DA. Exertional dyspnoea in COPD: the clinical utility of cardiopulmonary exercise testing. Eur Respir Rev. 2016;25 (141):333–347. doi:10.1183/16000617.0054-2016
17. Koulouris NG, Dimopoulou I, Valta P, Finkelstein R, Cosio MG, Milic-Emili J. Detection of expiratoryflow limitation during exercise in COPD patients.J Appl Physiol.1997;82(3):723–731. doi:10.1152/ jappl.1997.82.3.723
18. O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease.Proc Am Thorac Soc.2006;3 (2):180–184. doi:10.1513/pats.200508-093DO
19. Dellacà RL, Santus P, Aliverti A, et al. Detection of expiratoryflow limitation in COPD using the forced oscillation technique.Eur Respir J.2004;23(2):232–240. doi:10.1183/09031936.04.00046804 20. Elbehairy AF, Ciavaglia CE, Webb KA, et al. Pulmonary gas
exchange abnormalities in mild chronic obstructive pulmonary dis-ease. Implications for dyspnea and exercise intolerance.Am J Respir Crit Care Med.2015;191(12):1384–1394. doi:10.1164/rccm.201501-0157OC
21. Neder JA, Berton DC, Arbex FF, et al. Physiological and clinical relevance of exercise ventilatory efficiency in COPD.Eur Respir J. 2017;49(3):1602036. doi:10.1183/13993003.02036-2016
22. Neder JA, Berton DC, Müller PDT, et al. Ventilatory inefficiency and exertional dyspnea in early chronic obstructive pulmonary disease.
Ann Am Thorac Soc.2017;14(Supplement_1):S22–S29. doi:10.1513/ AnnalsATS.201612-1033FR
23. Caviedes IR, Delgado I, Soto R. Ventilatory inefficiency as a limiting factor for exercise in patients with COPD. Respir Care. 2012;57 (4):583–589. doi:10.4187/respcare.01342
24. Di Marco F, Terraneo S, Job S, et al. Cardiopulmonary exercise testing and second-line pulmonary function tests to detect obstructive pattern in symptomatic smokers with borderline spirometry.Respir Med.2017;127:7–13. doi:10.1016/j.rmed.2017.04.006
25. Zimmermann SC, Thamrin C, Chan AS, Bertolin A, Chapman DG, King GG. Relationships between forced oscillatory impedance and 6-minute walk distance after pulmonary rehabilitation in COPD.
Int J Chron Obstruct Pulmon Dis. 2020;15:157–166. doi:10.2147/ COPD.S225543
26. Global Initiative for Chronic Obstructive Lung Disease. Global strat-egy for prevention, diagnosis and management of COPD. Available from:https://goldcopd.org/. Accessed April 27, 2020.
27. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/ 09031936.05.00034805
28. Kubota M, Kobayashi H, Quanjer PH, et al. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig.2014;52(4):242–250. doi:10.1016/j.resinv.2014.03.003 29. Kanda Y. Investigation of the freely available easy-to-use software
“EZR” for medical statistics. Bone Marrow Transplant. 2013;48 (3):452–458. doi:10.1038/bmt.2012.244
30. Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinfl a-tion in chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis.2014;9:187–201. doi:10.2147/COPD.S38934
31. Yamamoto S, Miyoshi S, Katayama H, et al. Use of the forced-oscillation technique to estimate spirometry values.
Int J Chron Obstruct Pulmon Dis. 2017;12:2859–2868. doi:10.21 47/COPD.S143721
32. Shirai T, Kurosawa H. Clinical application of the forced oscilla-tion technique. Intern Med. 2016;55(6):559–566. doi:10.2169/ internalmedicine.55.5876
33. Goldman MD, Carter R, Klein R, Fritz G, Carter B, Pachucki P. Within- and between-day variability of respiratory impedance, using impulse oscillometry in adolescent asthmatics. Pediatr Pulmonol. 2002;34(4):312–319. doi:10.1002/ppul.10168
34. Akita T, Shirai T, Mori K, et al. Association of the forced oscillation technique with negative expiratory pressure in COPD.Respir Physiol Neurobiol.2016;220:62–68. doi:10.1016/j.resp.2015.09.002 35. Dellacà RL, Duffy N, Pompilio PP, et al. Expiratoryflow limitation
detected by forced oscillation and negative expiratory pressure.Eur Respir J.2007;29(2):363–374. doi:10.1183/09031936.00038006 36. Borrill ZL, Houghton CM, Tal-Singer R, et al. The use of
plethysmo-graphy and oscillometry to compare long-acting bronchodilators in patients with COPD. Br J Clin Pharmacol. 2008;65(2):244–252. doi:10.1111/j.1365-2125.2007.03013.x
37. Weatherald J, Sattler C, Garcia G, Laveneziana P. Ventilatory response to exercise in cardiopulmonary disease: the role of chemo-sensitivity and dead space. Eur Respir J. 2018;51:2. doi:10.1183/ 13993003.00860-2017
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020
International Journal of Chronic Obstructive Pulmonary Disease
Dovepress
Publish your work in this journal
The International Journal of COPD is an international, peer-reviewed journal of therapeutics and pharmacology focusing on concise rapid reporting of clinical studies and reviews in COPD. Special focus is given to the pathophysiological processes underlying the disease, inter-vention programs, patient focused education, and self management
protocols. This journal is indexed on PubMed Central, MedLine and CAS. The manuscript management system is completely online and includes a very quick and fair peer-review system, which is all easy to use. Visit http://www.dovepress.com/testimonials.php to read real quotes from published authors.
Submit your manuscript here:https://www.dovepress.com/international-journal-of-chronic-obstructive-pulmonary-disease-journal
International Journal of Chronic Obstructive Pulmonary Disease downloaded from https://www.dovepress.com/ by 118.70.13.36 on 27-Aug-2020