A RETROSPECTIVE STUDY OF OUTCOME OF
SEVERE TRAUMATIC BRAIN INJURY
AMONG ADULT PATIENTS IN
EMERGENCY DEPARTMENT OF
HOSPITAL UNIVERSITI SAINS MALAYSIA
By
DR. MARDHIAH BINTI JUSOH
Dissertation Submitted in Partial Fulfillment of The
Requirements For The Degree of Master of Medicine
(EMERGENCY MEDICINE)
SCHOOL OF MEDICAL SCIENCES
UNIVERSITI SAINS MALAYSIA
2
ACKNOWLEDEGEMENT
Alhamdulillah, thanks to merciful Allah for all the countless gifts offered to me. I would like to express my deepest gratitude to those who gave me the possibility to complete this dissertation. Special thanks to my supervisor, Associate Professor Dr. Kamarul Aryffin bin Baharuddin, Lecturer, Consultant Emergency Physician and Head Department of Emergency and Trauma of Universiti Sains Malaysia for his full support, expert guidance and encouragement throughout my study and research.
I would also like to thank Dr Najib Wajdi, biostatistician from Community Health Department of Universiti Sains Malaysia for his encouragement, creative and comprehensive advice until this work came to existence. And furthermore, I would like to thank the Director of Hospital Universiti Sains Malaysia who gave me permission to proceed with my dissertation.
And my special and sincere thanks to my family, especially to my husband, Dr. Hazrul Abdul Hamid, for his understandings and supports on me in completing this dissertation, my parents, Jusoh Ali and Mariati Awang Chik, who gave their full support and encouragement on me, my beloved children, Muhammad Yusuf, Maryam Safiyah and Muhammad Luth for all sacrifices that they had made for me during this study period and also my beloved brother and sisters. Also special thanks to Dr. Hamzah Abdul Hamid, who guided me regarding the statistical analysis.
Not forgotten, to all my friends and colleagues who had helped me to complete my thesis, thanks for all your kind endless help and support during this study.
3
TABLE OF CONTENTS
PAGE
ACKNOWLEDGEMENT ii
TABLE OF CONTENTS iii
LIST OF TABLES viii
LIST OF FIGURES x LIST OF ABBREVIATIONS ABSTRAK xi xiii ABSTRACT xv CHAPTER 1 - INTRODUCTION 1
CHAPTER 2 - LITERATURE REVIEW 6
2.1 Glasgow Coma Scale (GCS) 9
2.2 Age 9
2.3 Types of Intracranial Lesions and Midline Shifts 10
2.4 Pupillary Response 12 2.5 2.6 Hypoxemia Hypotension 12 13 2.7 Temperature 14 2.8 Coagulopathy 14 2.9 2.10 Hyperventilation Lactate Level 15 15 2.11 Blood Glucose 16 2.12 Decompressive Surgery 16
4
2.13 Glasgow Outcome Scale (GOS) 17
CHAPTER 3 - OBJECTIVES 19
3.1 General Objectives 20
3.2 Specific Objectives 20
3.3 Research Null Hypothesis 21
3.4 Definitions 21 CHAPTER 4 - METHODOLOGY 22 4.1 Study Design 23 4.2 Study Population 23 4.2.1 Source Population 23 4.3 Inclusion Criteria 23 4.4 Exclusion Criteria 23 4.5 Sampling Method 24 4.6 Sample Size 24 4.7
4.6.1 Sample Size for Mortality Outcome
4.6.2 Sample Size for Mortality According to Primary CT Scan 4.6.3 Sample Size for Pupillary Response
4.6.4 Sample Size for Glasgow Coma Scale (GCS) Research Tools 24 25 26 27 28 4.8 Data Collection 28
4.9 Data Entry and Analysis 29
4.10 Conflict of Interest 31
4.11 Approvals (Appendix A-1(a), A-1(b), A-2, A-3) 32
5
4.13 Schedule (Gantt Chart) (Appendix B) 34
4.14 Data Collection Form (Appendix C) 34
CHAPTER 5 - RESULTS 35
5.1 Demographic Data 36
5.2 Types of Referral 36
5.3 Mechanism of Injury 37
5.4 Age 37
5.5 Glasgow Coma Scale (GCS) 40
5.6 Pupillary Response 40
5.7 Vital Signs 41
5.7.1 Heart Rate (HR) 5.7.2 Respiratory Rate (RR) 5.7.3 Temperature
5.7.4 Systolic Blood Pressure (SBP) 5.7.5 Diastolic Blood Pressure (DBP)
41 41 41 42 42
5.8 Midline Shifts on CT Scan 44
5.9 Primary CT Brain Findings 44
5.10 Types of Herniation 45
5.11 Blood Investigations 47
5.11.1 Full Blood Count (FBC) 5.11.2 Blood Glucose
5.11.3 Arterial Blood Gas (ABG) 5.11.4 Coagulation Profile
47 48 49 50
6
5.13 Length of ICU and Hospital Stay 54
5.14 Outcome According to Glasgow Outcome Scale (GOS) 55 5.15 Prognostic Factors for Predicting Outcome (Mortality) 57
5.15.1 Univariate Analysis 57
5.15.1(a) Age 5.15.1(b) Gender
5.15.1(c) Glasgow Coma Scale (GCS) 5.15.1(d) Pupillary Response
5.15.1(e) Vital Signs
5.15.1(f) Primary CT Brain Findings 5.15.1(g) Blood Investigations 57 58 58 58 58 59 60 5.15.2 Multivariate Analysis 69 CHAPTER 6 - DISCUSSION 72 6.1 General 73 6.2 Demographic Data 73 6.2.1 Nationality 6.2.2 Gender 6.2.3 Race 74 74 75 6.3 Age 75 6.4 Types of Referral 77 6.5 Mechanism of Injury 78
6.6 Glasgow Coma Scale (GCS) 79
6.7 Pupillary Response 80
6.8 Types of Brain Lesions on Primary CT Scan 81
7
6.10 Vital Signs 82
6.10.1 Heart Rate
6.10.2 Systolic Blood Pressure (SBP) 6.10.3 Diastolic Blood Pressure (DBP)
6.10.4 Respiratory Rate (RR) and Temperature
82 83 84 84
6.11 Blood Investigations 85
6.11.1 Full Blood Count (FBC) 6.11.2 Arterial Blood Gas (ABG) 6.11.3 Coagulation Profile 6.11.4 Blood Glucose 85 86 89 90 6.12 6.13 6.14 Surgical Intervention
Length of Hospital and ICU Stay Univariate and Multivariate Analysis
91 91 92 CHAPTER 7 - CONCLUSION 93 CHAPTER 8 - LIMITATIONS 96 REFERENCES 99 APPENDICES 108
8
LIST OF TABLES
PAGE
Table 5.1 Frequency and Percentage of Mortality According to Demographic Data, Types of Referral, Mechanism of Injury, Types of Vehicle and Motorcycle
39
Table 5.2 Frequency and Percentage of Mortality According to Clinical Findings
43
Table 5.3 Frequency and Percentage of Mortality According to Primary CT Brain Findings
46
Table 5.4 Frequency and Percentage of Mortality According to Initial Blood Investigation: FBC, Coagulation Profile and Blood Glucose
52
Table 5.5 Frequency and Percentage of Mortality According to Initial Arterial Blood Gases and Lactate Level
53
Table 5.6
Table 5.7
Frequency and ercentage of Mortality According to Surgical Intervention and Outcome
Crude Odd Ratio (OR), 95% CI and p-value for Univariate Unadjusted Binary Logistic Regression on Demographic Data
56
64
Table 5.8 Crude Odd Ratio (OR), 95% CI and p-value for Univariate Unadjusted Binary Logistic Regression on Clinical Findings
65
Table 5.9 Crude Odd Ratio (OR), 95% CI and p-value for Univariate Unadjusted Binary Logistic Regression on Primary CT Brain Findings
9 Table 5.10
Table 5.11
Crude Odd Ratio (OR), 95% CI and p-value for Univariate Unadjusted Binary Logistic Regression on Initial Blood Investigations
Crude Odd Ratio (OR), 95% CI and p-value for Univariate Unadjusted Binary Logistic Regression on Initial Arterial Blood Gases and Lactate
67
68
Table 5.12 Adjusted Odd Ratio (OR), 95% CI and p-value for Multivariate Adjusted Binary Logistic Regression on Demographic Data and Clinical Findings
70
Table 5.13
Table 5.14
Adjusted Odd Ratio (OR), 95% CI and p-value for Multivariate Adjusted Binary Logistic Regression on Primary CT Brain Findings
Adjusted Odd Ratio (OR), 95% CI and p-value for Multivariate Adjusted Binary Logistic Regression on Initial Blood Investigations
71
10
LIST OF FIGURES
PAGE
Figure 2.1 Glasgow Coma Scale (GCS) 8
11
LIST OF ABBREVIATIONS
ABG Arterial blood gas
aPTT activated partial thromboplastin time
bpm beats per minute
CBF Cerebral blood flow
CO2 Carbon dioxide
CPG Clinical Practice Guidelines CPP Cerebral perfusion pressure
CT Computed Tomography
DBP Diastolic blood pressure
DAI Diffuse axonal injury
ED Emergency department
EDH Extradural hemorrhage
FBC Full blood count
GCS Glasgow Coma Scale
GOS Glasgow Outcome Scale
Hb Hemoglobin
HCO3 Bicarbonate
HCT Hematocrit
HR Heart rate
HRPZ 2 Hospital Raja Perempuan Zainab 2 HSNZ Hospital Sultanah Nur Zahirah HUSM Hospital Universiti Sains Malaysia
ICP Intracranial pressure
12
INR International normalized ratio
IVH Intraventricular hemorrhage
MLS Midline shifts
MOH Ministry of Health
MVA Motor vehicle accident
pCO2 Partial pressure carbon dioxide
pO2 Partial pressure oxygen
PT Prothrombin time
RR Respiratory rate
SAH Subarachnoid hemorrhage
SBP Systolic blood pressure
SD Standard deviation
SDH Subdural hemorrhage
TBI Traumatic Brain Injury
TWC Total white count
13
KAJIAN RETROSPEKTIF KESAN KECEDERAAN KEPALA
YANG TERUK DI KALANGAN PESAKIT DEWASA
DI JABATAN KECEMASAN
HOSPITAL UNIVERSITI SAINS MALAYSIA
ABSTRAK
Kecederaan kepala adalah salah satu penyebab terbesar kepada kematian dalam abad ini. Dalam beberapa kajian yang telah dijalankan sebelum ini, beberapa faktor yang berkaitan dan faktor prognosis telah dikenalpasti mempunyai kaitan dengan kematian pada pesakit kecederaan kepala yang teruk. Namun, masih ada yang masih hangat diperbincangkan. Di Malaysia, peratus kematian pesakit yang menghidapi kecederaan kepala yang teruk masih lagi tinggi sementara kebanyakan pesakit yang terselamat mempunyai kesan yang tidak diingini seperti kurang upaya yang teruk kesan daripada kecederaan kepala primer dan sekunder.
Kajian ini dijalankan di Jabatan Kecemasan Hospital Universiti Sains Malaysia (HUSM) memandangkan HUSM merupakan pusat rujukan bagi kes-kes pembedahan kepala di Kelantan dan hospital-hospital besar dan daerah di sekitarnya. Dalam kajian ini, kesan kecederaan kepala yang teruk yang dialami oleh pesakit-pesakit dewasa dilihat berdasarkan markah Glascow Outcome Scale (GOS). Skala ini digunakan untuk menilai fungsi pesakit kecederaan kepala yang teruk antaranya; kurang upaya ringan, sederhana atau teruk, vegetatif atau kematian. Selain itu, tujuan kajian ini juga adalah untuk mengenalpasti faktor-faktor yang mempunyai kaitan dengan kematian pada pesakit kecederaan kepala yang teruk dan boleh menjangkakan hasil kesan kecederaan.
14
Ini termasuk faktor umur, jantina, respon anak mata, markah Glasgow Coma Scale (GCS), tanda-tanda vital, keputusan darah dan CT kepala.
Kajian retrospektif yang dijalankan ini melibatkan 96 pesakit dengan kecederaan kepala yang teruk. Pesakit-pesakit ini disusuli sehingga dibenarjan keluar dari wad untuk mengenalpasti kesan yang dialami. Daripada 96 pesakit ini, satu pertiga dari mereka meninggal ketika dirawat di hospital yang merangkumi 34.4% (33) manakala selebihnya 65.6% (63) adalah terselamat. Bagi pesakit yang terselamat; 31.3% (30) daripada pesakit ini mengalami keadaan kurang upaya ringan, manakala bagi kurang upaya sederhana dan teruk masing-masing adalah 15.6% (15). Selebihnya, 3.1% (3) daripada mereka mengalami vegetatif.
Dengan menggunakan model binary logistic regression, beberapa faktor prognosis yang boleh menjejaskan kesan bagi pesakit dengan kecederaan kepala yang teruk telah dikenalpasti. Ini termasuk faktor umur, markah GCS, respon anak mata, kehadiran pendarahan subdural dan peralihan garis tengah otak, tahap gula, darah putih, pH, pCO2, HCO3, lactate, PT, INR dan tempoh masa kemasukan ke ICU dan hospital.
Manakala, faktor umur, markah GCS, respon anak mata, tempoh masa kemasukan ke hospital dan peralihan garis tengah otak melebihi 5 mm merupakan faktor-faktor yang signifikan dengan sendirinya.
15
A RETROSPECTIVE STUDY OF OUTCOME OF
SEVERE TRAUMATIC BRAIN INJURY AMONG
ADULT PATIENTS IN EMERGENCY DEPARTMENT
HOSPITAL UNIVERSITI SAINS MALAYSIA
ABSTRACT
Traumatic brain injury (TBI) has become one of the major causes of death in this decade. Some of the associated and prognostic factors have been proven to have correlation with mortality in severe TBI in studies which were done earlier. However, some of them are yet still debatable. In Malaysia, the percentage of mortality of the patients presented with severe TBI is still high while a lot of survived patients had unfavorable outcome; persistently vegetative and severely disabled, as results of complications of primary and secondary brain injury.
This study was done at Emergency Department (ED) of Hospital Universiti Sains Malaysia (HUSM) as HUSM is the center of referral for neurosurgical cases in Kelantan and nearby tertiary and district hospitals. In this study, the outcome of the adult patients with severe TBI were observed according to Glasgow Outcome Scale (GOS) upon discharge. This scale was used to assess the functional ability of the patients either low, moderate or severely disabled, persistently vegetative or death. Besides that, the aim of this study was also to determine the associated and prognostic factors that can predict the outcome of severe TBI patients. This include gender, age, clinical findings such as Glasgow Coma Scale (GCS) score, pupillary response, vital signs, blood investigations and primary CT brain findings.
16
A retrospective study was done with 96 patients with severe TBI were enrolled. These patients were followed-up until discharge to identify their outcome. From 96 patients, one third of them which accounted 34.4% (33) died and 65.6% (63) survived. The survived patients; 31.3% (30) of them were discharged with good outcome (low disability), while both moderate and severely disabled, accounted about 15.6% (15) each. 3.1% (3) of them were discharged with vegetative state.
Using the binary logistic regression model, a few prognostic factors were found to be significantly affecting the outcome of the severe TBI. These include, age, GCS score, abnormal pupillary response, presence of subdural hemorrhage (SDH) and midline shifts, total white count (TWC), pH, pCO2, HCO3, lactate and glucose level,
prothrombin time (PT), INR and length of ICU and hospital stay. Whereby age, GCS score, abnormal pupillary response, duration of hospital stay and presence of midline shifts more than 5 mm on CT brain were factors that independently significant.
17
CHAPTER 1
Introduction
18
INTRODUCTION
Trauma remains one of the major presentations to the emergency departments (ED) in most of the hospitals worldwide. It was reported that trauma accounted 27.3 deaths per 100 000 population per year (Steven R.S. et al, 1993). In Malaysia, the road traffic fatality rate in Malaysia was higher than global rate (25 vs 18 per 100,000 population) (World Health Organization, 2013). Almost half of the ED visits are due to traumatic cases (National Trauma Database, 2007). In 2007 for example, Malaysia National Trauma Database reported that almost 120 thousands of trauma patients visited to the ED in five participating centers which were Hospital Selayang, Hospital Kuala Lumpur, Hospital Sultanah Bahiyah, Hospital Pulau Pinang and Hospital Sultanah Aminah, with overall mortality in these centers was about one third for major trauma. Although the report was only based on these five centers, it gives a rough estimation that trauma is one of the common causes of morbidity and mortality in Malaysia.
Traumatic brain injury (TBI) is a leading cause of death and disability worldwide, with 1.5 million affected people die and several million received emergency treatment (Reminger et al, 2005). This huge number of statistic caused burden especially in low and middle income countries (Perel et al, 2007). TBI is considered as part of the major traumatic injuries. It can be isolated, but 35% of the cases are also associated with extra-cranial injuries such as limb fractures, thoracic or abdominal injuries (Andrew et al, 2008). The mechanism can be resulted either from a motor vehicle accident (MVA), fall, assault or external blows to the head (Jean et al, 2006). Violence also was reported as one of the cause of closed head injury with approximately 7-10% of cases and the number keep on increasing (Jiang J.Y. et al, 2007). MVAs are the major cause
19
of death and disabilities in both more and less developed countries, particularly in young people (Murray et al, 1997). Whereby, in people older than 65 years old, falls are the leading cause of death and disability from TBI (US National Centre for Injury Prevention and Control, 1999). However with the modern health facilities nowadays, the age span is increasing with a lot of elderly population still able to drive and be on road. This contributed to the increasing number of patients within this age group presented with trauma to ED.
In the United States, it is estimated that about 1.4 million people presented for medical care for TBI each year from 1995 through 2001. The analysis also found that,
approximately 50 thousands (3.6%) of them died from their injuries, 235 thousands (17%) were hospitalized, and 1.1 million (80%) were treated as outpatients(National Centre for Injury Prevention and Control Traumatic Brain Injury, 2006).
TBI is more common in young adults, particularly male. Overall, males are about twice as likely as females to experience TBI. Young children aged 0-4 years and older adolescents aged 15-19 years are more likely to sustained TBI. The elderly, aged more than 75 years with TBI have the highest incidence of hospitalization (Langlois et al, 2004).
Whereby in Malaysia, more than 90% of the major trauma cases involved the head and neck region and mostly involved the young age group, within the age group of 15-34 years old. More than half of major trauma had Glasgow Coma Scale (GCS) of 8 and less (National Trauma Database, 2007). A systemic review of brain injury epidemiology done in Europe, searched for related articles from 1980 to 2003, showed
20
that 90% of the TBI was classified as mild, 6% as moderate and 4% as severe, according to the GCS score (Springer Link, 2005). The mortality rate of the severe TBI patients were about 30% (Jiang J.Y. et al, 2002).
TBI can be defined as a non-degenerative, non-congenital insult to the brain from an external mechanical force which possibility leading to long-term or lifelong, permanent or temporary cognitive impairment, behavioural and emotional consequences (US National Institute of Health, 1998). Each year, about 52 thousands death and 80 thousands permanent severe neurological disabilities, result from the severe TBI (Sosin et al, 1996). As TBI may cause serious complications, patients with TBI-related disability face lots of challenges in effort to ensure that they are able to return to good functional ability of life (Jean et al, 2006). Not only the TBI patients, this disability also gives huge impact to the family and may cause burdened for them. Even mild TBI, including concussion, can cause long term cognitive problems that affect a person’s functional ability to perform daily activities and return to work (McAllister et al, 2001). As compared to spinal cord injury-related disability, patients with TBI-related disability has 14 times higher percentage of injury-related productivity loss (Finkelstein et al, 2006).
Prevalence of long-term disability from TBI in the United States population, estimated that at the beginning of 2005, 3.17 million people in the United States (1.1% of the total population) were living with long-term disability that resulted from TBI (Zaloshnja et al 2008). The outcome of the TBI mostly measured using the Glasgow Outcome Scale (GOS). A study observing the outcome of severe TBI showed that, 36% made of the patients made a good recovery, 24% were moderately disabled but
21
able to care for themselves, 8% were left severely disabled, and 2% were vegetative requiring institutional care; 30% of the patients died (Donald et al, 1977).
Although the prognosis and outcome depends on the severity of the injury as well as the time of presentation to the ED, there are other factors that may contribute to the prognosis and predict the outcome of the TBI patients. Despite good resuscitation and management during arrival to the ED, it is important to know the prognostic prediction of those with brain injury to prevent secondary insult and cause further damage to the brain. These include age, GSC score, pupillary reactivity, blood pressure, intracranial pressure, blood glucose, platelet count, body temperature, cerebral lactate, and types of intracranial lesions (Engelien et al, 2016). It is very important to know the significantly proved prognostic factors and to determine the impact of these factors to the outcome of TBI to prevent the secondary brain injury and improve the treatment and management to increase the survival probability and ensure good prognosis.
As these predictive factors can predict the outcome of the TBI patients, it is best to manage and treat these TBI patients in neurosurgical centres. Early referral is indicated in view of odds of death increase 2.15 times if treated in a non-neurosurgical centre (Patel et al, 2006).
The rationale of this study is to determine the outcome of severe TBI as TBI is one of the common presentations in ED and commonly occurred in adults. In Malaysia, there is still lack of published data regarding the epidemiology of severe TBI, the outcome and its prognostic factors. Recent data on the epidemiology is not much available as currently the age population is different compared to old previous years.
22
CHAPTER 2
Literature Review
23
LITERATURE REVIEW
TBI is the most common cause of death and disability worldwide. Over the years, the mortality of the patients with severe TBI has decreased and the outcome has improved. An organised trauma system that allows rapid resuscitation and direct transport to the experienced trauma centre has significantly lowers the mortality and morbidity (Jamshir G., 2000).
TBI is graded as mild, moderate or severe based on the level of consciousness or a score according to GCS after initial primary survey performed. A trauma patient with mild TBI has a GCS score of 14 to 15. They usually have concussion with full neurological recovery, although some of them might have short term memory and concentration difficulties (Rimel et al, 1981). In moderate TBI, the patients usually restless with the GCS score of 9 to 13, whereby in severe TBI the GCS score was 8 and below and the patients usually comatose (Mass A.I.R. et al, 2008).
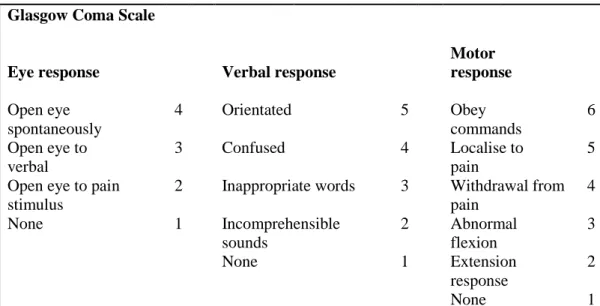
GCS score consists of three parameters. It assesses the eye response, verbal response and motor response. The GCS is scored between 3 and 15, with 3 being the worst, and 15 the best, as shown in the below table. A score of 13 or higher correlates with a mild TBI, 9 to 12 is a moderate TBI and 8 or less is a severe TBI (Mass A.I.R. et al, 2008).
24
Glasgow Coma Scale
Eye response Verbal response
Motor response Open eye spontaneously 4 Orientated 5 Obey commands 6 Open eye to verbal 3 Confused 4 Localise to pain 5 Open eye to pain
stimulus
2 Inappropriate words 3 Withdrawal from pain 4 None 1 Incomprehensible sounds 2 Abnormal flexion 3 None 1 Extension response 2 None 1
Figure 2.1: Glasgow Coma Scale (GCS)
Head injury does not always implicate TBI. To diagnose TBI, besides the clinical signs and symptoms, CT brain still remains the preferred method of assessment to detect the intracranial bleeding and determine the structural damage. It is present in almost all patients with severe and moderate TBI, but is also reported in 14% of the patients with GCS of 14, which is in mild TBI. As general, CT brain is indicated in all TBI patients with GCS of 14 and below and in full GCS patients in the presence of risk factors (Andrew et al, 2008).
Severe TBI may precipitates the release of inflammatory response. This event may cause the surge of stress hormones such as catecholamine. A lot of studies had done to determine the correlation and prognostic factors that may worsened the mortality and morbidity, therefore the outcome of patients with severe TBI can be predicted. A study, done by Gordon et al, published in year 2007 in Journal of Neurotrauma, entitled Multivariable Prognostic Analysis in Traumatic Brain Injury: Results from the IMPACT Study, showed that the most important prognostic factors of severe TBI that were identified include age, GCS motor score, pupils response, CT characteristics,