Vol. 7, No. 3 (2017): 1760-1764 Research Article
Open Access
I
ISSSSNN::22332200--66881100
Evaluation of Various Thyroid Hormones on the
patients with Thyroid cancer
Madlen Qassm abbas*
College of Dentistry, Tikreet University, Iraq.
* Corresponding author: Madlen Qassm abbas, e-mail: madlenqasim@yahoo.com
ABSTRACT
In severe illness of cancer cause, depression of the thyroid hormone system may occur in otherwise euthyroid patients, Sixty five specimens of blood were collected from 65 patients with thyroid cancer and 50 healthy between 30 and 48 years old attending the thyroid centre in Al yarmook teaching hospital from the period November 2014 to June 2015. All samples were inoculated to study different characteristics of hormones. The blood was collected for hormonal assay the results revealed a gradual decrease in serum TT3 levels with a concomitant increase in Serum Thyroid stimulating hormone TSH level when compared with control healthy and also a reduction in TT4 in thyroid cancer patients compared with control healthy.
Keywords:
Thyroid cancer; hormonal identification.1. INTRODUCTION
Cancer in thyroid gland consider as rapid growth of the cancerous cell with no control around the gland and another part of the human patients body, this type of cancer disease which affect the people in different ages at the same time most of them have recovery after treatment (1). Studies appeared different type of carcinoma divided based on the site of cell to: Papillary, follicular; medullary; hurtle cell; anaplastic ,nodules. Most of these type of carcinoma benign appeared as over growth but in the advance patient appeared as malignant may lead to death (3). In some patients nearly 24% the carcinoma developed from the thyroid itself due to disorder in its activity but most of the cases carcinoma developed in the part of the patient's body and the disease referred as lymphoma (4,5). There are different factors leading to thyroid cancer and the most causative agent is exposure to radiation and it has been reported that there is a linear relationship between thyroid cancer and exposure to radiation in different forms and waves (6). Currently, thyrotropin (TSH), free thyroxine (tT4), or FT4 combined with total triiodothyronine (TT3) is recommended for use as indicators in laboratory testing to assess thyroid function clinically (e.g., in the guidelines of the American Thyroid Association (ATA)) (7, 8). However, this recommendation is not based on
credible clinical evidence or on the grounds of a large enough demographic data set. According to the existing references, the clinical value of the three parameters (TT3, TT4, and TSH) has not been elaborated clearly (9). The current study designed to investigate hormonal identification of thyroid cancer patients based on hormonal abnormality.
2. MATERIALS AND METHODS
Sixty five specimens of blood were collected from 65 patients with thyroid cancer and 50 healthy between 30 and 48 years old attending the thyroid centre in Al yarmook teaching hospital from the period from November 2014 to June 2015. All samples were inoculated to study different characteristics of hormones. All the experiment blood samples were drawn and serum was collected by centrifugation. Thyroid stimulating hormone (TSH) concentrations were measured and free thyroxine (TT4), and total triiodothyronine (TT3) in serum by ELISA kits (Beckman-France), as presented in standard assay (10) procedures represented in figure 1. The results were analyzed using one-way analysis of variance (ANOVA), the level of statistic was set at P<0.05(11).
Procedure for T3
Preparation: 50 ml of the serum samples from the patients and compared it with standard from healthy and added it to the wells of plates
Add 100µl of working reagent A, T3 enzyme reagent to all wells Shaking the micro titter plate slowly
Incubation 60 minutes at room temperatures Discard the contents of the micro plate
(3times) Add 350µl of wash buffer
Add a100µl of working substrate solution into well Incubation 15 minutes at room temperature
Add 50µl stop solution to each Swirl the micro plate 20-30 second Read the absorbance in each wells at 450 nm
Procedure for T4
Format the micro plate wells for each serum reference, control and patient specimen Add 25µl of the appropriate serum reference or specimen into each well
Add 100µl of working reagent A, T4 enzyme reagent to all wells Swirl the micro plate 20-30 second
Incubation 60 minutes at room temperature Discard the contents of the micro plate
(3times) Add 350µl of wash buffer Add100µl of working substrate solution into well
Incubation 15 minutes at room temperature Add50µl stop solution to each Swirl the micro plate 20-30 second Read the absorbance in each wells at 450 nm
Procedure for TSH
Format the micro plate wells for each serum reference, control and patient specimen Add 50μl of the appropriate serum reference or specimen into each well
Add 100µl of TSH -enzyme reagent to all wells Swirl the micro plate 20-30 second Incubation 60 minutes at room temperature
Discard the contents of the micro plate (3times) Add 350µl of wash buffer Add100µl of working substrate solution into well
Incubation 15 minutes at room temperature Add50µl stop solution to each Swirl the micro plate 20-30 second Read the absorbance in each wells at 450 nm
Figure 1: Procedure of hormone analysis subjected during the present study.
3. RESULTS AND DISCUSSION
To study the disorder of hormones, the analysis of blood sample subjected and appeared that there is a significant difference between the healthy group and thyroid cancer patients during the period of study as appeared in table (1)
Hormonal changes play important roles in the patients with thyroid cancer. Table (1) represented and summarized the hormonal profile of patients compared
Table 1: Average of Thyroid stimulating hormone (T.S.H), (TT3) and (TT4) in patients with Thyroid cancer compare with healthy.
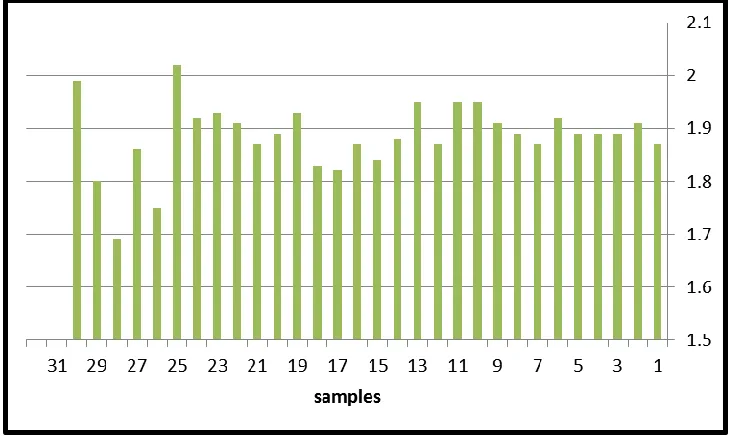
Figures 2,3 and 4, summarize the concentrations profile of the three studied hormones TSH, TT3 and TT4 in patients with Thyroid cancer.
Figure 2: Thyroid stimulating hormone (T.S.H) in patients with Thyroid cancer compared with healthy.
Figure 3: Thyroid TT3 mIU/ml in patients with Thyroid cancer compared with healthy.
NO. TSH, mIU/ml TT3 mIU/ml TT4 mIU/ml
Average 16.0±0.07 5.61±0.05 22.9±0.05
Control
Figure 4: Thyroid TT4 mIU/ml in patients with Thyroid cancer compared with healthy.
The profile of TSH in current study may be caused by regulation of SF-1gene activity is generally regulated by Adrenocorticotropin (ACTH) and gonadotropin (TH and TSH) and intracellular cAMP/PKA signal pathway which is a major signaling pathway that transmits the signal from extracellular stimuli to the nucleus (12). Also our present result in hormonal changes may be related to the individuals might have external genitalia which cannot evaluate the difference in an individual’s genitalia or abnormality in secondary reproductive organs and adrenal glands. Adrenal gland abnormality may rise due to deficiency of hormones which further might result in various health problems. (13). Thyroid disease can always be ruled out when the serum TSH level is normal without drug administration or in the absence of obvious hypothalamic-pituitary disease (14).However, even in a thyroid disease-free population, Gammage found that high-normal thyroid function could have an impact on the human health, such as atrial fibrillation (15). Heeringa et al. conducted a prospective cohort study with 1,426 subjects, which showed that peoplewith normal thyroid function could also show the correlation between TSH, TT4and the risk of atrial fibrillation [16]. Therefore, the thyroid function testing of healthy people is equally important. Studies in healthy people < 50 years old showed that there are a variety of progressive changes in hypothalamic-pituitary thyroid axis function. These changes will affect the accurate assessment of thyroid function. These changes on circulating T4 and TSH are minimal, while the effect on T3 is relatively larger [17, 18]. Therefore, TSH and T4 are more stable and accurate for the evaluation of thyroid function in healthy people. At any age, TSH secretion is modulated by T4 levels, and the responsiveness of the thyroid-pituitary axis is most likely different at different ages
factor (TNF) and interleukin (IL), and these cytokines can reduce the secretion of TSH, TT4 and inhibit gene expression of TBG in liver. The secretion and release of thyroid hormones from the thyroid gland generally occurs at the normal levels in healthy people. In the absence of factors affecting the TBG, serum thyroid hormone levels can be maintained within a certain range. Therefore, TT4 and FT4 both may reflect thyroid function. De Alfieri et al. have shown that, in populations with normal thyroid function at baseline, increasing TT4 levels tended to predict long-term mortality [19].
4. CONCLUSION
Our study showed that there was significant difference between Thyroid cancer patients and healthy humans studied group which may be due to molecular changes that is more precise and less consuming time in studying thyroid cancer and this result may help in controlling and develop treatment for such cases.
5. REFERENCES
1. S.Danzi and I. Klein, “Thyroid hormone and the cardiovascular system,”Medical Clinics of NorthAmerica, vol. 96,no. 2, pp. 257–268, 2012.
2. C. F. Yazbeck and S. D. Sullivan, “Thyroid disorders during pregnancy,” Medical Clinics of North America, vol. 96, no. 2, pp. 235–256, 2012.
3. R. Mansoor, S. R. Rizvi, and S. T. Huda, “Spectrum of thyroid diseases: an experience in the tertiary care and teaching hospital,” Annals of Pakistan Institute of Medical Sciences, vol. 6, pp. 101–106, 2010.
4. A. Khan, M. M. A. Khan, and S. Akhtar, “Thyroid disorders, etiology and prevalence,” Journal of Medical Sciences, vol. 2, pp. 89–94, 2002.
7. E. N. Pearce, J. V. Hennessey, and M. T. McDermott, “New American thyroid association and American association of clinical endocrinologists guidelines for thyrotoxicosis and other forms of hyperthyroidism: significant progress for the clinician and a guide to future research,” Thyroid, vol. 21, no. 6, pp. 573– 576, 2011.
8. J. R. Garber, R. H. Cobin, H. Gharib et al., “Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the AmericanThyroid Association,” Endocrine Practice, vol. 18, no. 6, pp. 988–1028, 2012.
9. H. Al-Adsani, L. J. Hoffer, and J. E. Silva, “Resting energy expenditure is sensitive to small dose changes in patients on chronic thyroid hormone replacement,” Journal of Clinical Endocrinology andMetabolism, vol. 82,no. 4, pp. 1118–1125, 1997.
10.Katz P, Bellet N, less M.CEDIATM total an automated homogenous enzyme-immunoassay for serum total fsh,testosteron. Clin Chem.1991;37:9936.
11.Steel, RG. and Torries JH. (1980). Principal and Procedures of Statistics. Abiometrical approach 2nd Ed. McGraw - Hill Book Company. New York USA.
12.S. Ghosh, M. Howlett, D. Boag, I. Malik, and A. Collier, “Interference in free thyroxine immunoassay,” European Journal of Internal Medicine, vol. 19, no. 3, pp. 221–222, 2008.
13.K. Ohba, J. Y. Noh, T. Unno et al., “Falsely elevated thyroid hormone levels caused by antirutheniuminterference in the Elecsys assay resembling the syndrome of inappropriate secretion of thyrotropin,” Endocrine Journal, vol. 59,no. 8, pp.663–667, 2012.
14.E. Mingote, T. Mero˜no, R. Rujelman et al., “High TSH and low T4 as prognostic markers in older patients,” Hormones, vol.
15.P. T. Trzepacz, I. Klein, M. Roberts, J. Greenhouse, and G. S. Levey, “Graves’ disease: an analysis of thyroid hormone levels and hyperthyroid signs and symptoms,” The American Journal of Medicine, vol. 87, no. 5, pp. 558–561, 1989. 16.H.Yang,W. Zhang, Q. Kong et al., “Effects of pubertal exposure
to thiazole-Zn on thyroid function and development in female rats,” Food and Chemical Toxicology, vol. 53, pp. 100–104, 2013.
17.J. D. Broussard, M. E. Peterson, and P. R. Fox, “Changes in clinical and laboratory findings in cats with hyperthyroidism from 1983 to 1993,” Journal of the American Veterinary Medical Association, vol. 206, no. 3, pp. 302–305, 1995. 18.M. E. Peterson, C. Meli´an, and R. Nichols, “Measurement of
serum concentrations of free thyroxine, total thyroxine, and total triiodothyronine in cats with hyperthyroidism and cats with nonthyroidal disease,” Journal of the American Veterinary Medical Association, vol. 218, no. 4, pp. 529–536, 2001.
19.M. E. Peterson, “Diagnostic tests for hyperthyroidism in cats,” Clinical Techniques in Small Animal Practice, vol. 21, no. 1, pp. 2–9, 2006.
20.E. M. Kaptein, “Clinical application of free thyroxine determinations,” Clinics in Laboratory Medicine, vol. 13, no. 3, pp. 653– 672, 1993.
*****
© 2017; AIZEON Publishers; All Rights Reserved