Volume 5, Issue 4, May 2017
‘MediBase’ Aadhar based medical record system
S.R.Rajeswari, SushmitaSuman, VaishaliPorwal, Jenifer Sneha
Abstract—The paper discussesdevelopment of an efficient electronic medical record with a unique patient identifier. This is to enable hospitals, physicians and individuals in India to efficiently share their records. As we see electronic medical record keeping system coming into the market, two problems still remain outstanding, one of them being a need to connect all this data to a unique patient identifier and second problem is a need for a unified data. With MediBase patient data is available readily and there is no need to depend on patients to bring their previous records. All the relevant medical history is recorded and sorted by the software and is available at a single screen all linked to the patient’s unique identifier.
Keywords
—
electronic medical record, unified patient identifier, unified data.I.
I
NTRODUCTIONAs we are in the modern era, the field of medicine is additionally making an attempt to use the data technology to enhance patients' care. One among the foremost important IT applications in health care is the electronic medical record (EMR). The main motivation of this paper is to explore EMR in terms of data retrieval. The broad areas discussed during this paper are the model of medical data and therefore the challenges in indexing, sharing and linking of medical records.
Proper delivery of patient care is important and depends on the flexibility to retrieve relevant data regarding the patient as quickly as possible. The accessibility of complete healthcare data must be accessible to everybody concerned within the delivery of patient healthcare from researchers making an attempt to search out causes, treatments, and cures for diseases to the patient themselves. The ability to universally access all patient healthcare data in an exceedingly timely fashion is of utmost importance.
II.
S
HIFTING TO ELECTRONIC MEDICAL RECORD SYSTEM AND ITS ADVANTAGESResearchers all over the world have many different definition of Electronic Medical Records (EMR) in their studies. According to Haslina and Sharifah Mastura [1] and Boonstra and Broekhuis [2], EMR plays an important role in providing patients’ medical histories, which include one or more computerised clinical information system that collects,
stores, and displays patients’ informationFurthermore, EMR consists of clinical information repository, order entry, processed provider order entry, pharmacy, and clinical documentation applications.
The adoption of EMR system brings each positive and negative problem that requires to be mentioned. It is necessary to analyse the problems to confirm that the adoption of the EMR system process is successful and economical. Few of the advantages of this system are, it is simple and provides remote access to patients’ information. Also it improves administrative tasks and is time and space saving. Lastly it brings legibility, is up-to-date and conjointly decreases medical errors.
According to Md. Zan [3], the general public hospitals are typically related to slow and inefficient services. Thus, many of us don't seem to be comfortable using the services in public hospitals because the time to get the treatment is long. The projected system looks forward to eradicate issues like these.
III. LITERATURE SURVEY
A. Model of medical information
Volume 5, Issue 4, May 2017 history isn't always the reality regarding an individual
instead is a set of thoughts and observations of an individual at a given time and place.
B. FIRD Framework
The work done by D. C. Leonard et al. (2009), [5] proposes the fingerprint, iris, retina scan, and DNA (FIRD) framework that utilize a patient’s biometric characteristics to unambiguously associate them to their medical information. The framework establishes an infrastructure that may distinctively determine a patient to his or her complete electronic healthcare record (EHCR) with actual exactness and accuracy. The framework’s inner workings can collect records that aren't properly allotted to the universal patient identifier (UPI), remove records that don't belong to the patient, and correct errors and omissions among the patient’s EHCR. The creation of a uniform nationwide electronic healthcare record system within the united states would need some way to match a composite of an individual’s recorded healthcare data to a known individual patient out of roughly 300 million individuals to a 1:1 match, leading to a final information compilation that has a whole healthcare history to the healthcare supplier, whereas reducing medical errors and lowering healthcare price. D. C. Leonard [5] proposed this system for implementation in USA in combination with the SSN.
C. UPI (Unique Patient Identifier)
Carpenter [6] mentioned that the department of Health and Human Services in 1973 reported that they are object to shift forward toward “Standard Universal Identification”. The proposed Universal Patient identifier (UPI) ought to have the subsequent features: singularity, verifiability, dependability, and trailing. The proposed UPI consists of seven digit date code, six digit geographical code relate to the place of birth, five digit sequence code to spot born on a similar date within the same geographical area, and one single check digit, that make the total size is nineteen digits. For examples, 9930301^044273^00047^2 represent an individual born in March 1, 1993 in Minneapolis, MN- USA. The proposed UPI is used as Universal provider Identification (UPI) by adding one digit refers to P (provider), or MD, or RN etc. The author also said that the proposed UPI is reasonable and versatile and might be easily adapted using the accessible infrastructure. The proposed UPI codes using base 34 digits bit base and check digit algorithm used to defend against miskey and digit inversion.
D. EMR framework for Malaysia’s Public Hospitals
Nurul Izzatty Binti Ismail and Nor Hazana Binti Abdullah [7] in their work projected the EMR Adoption Framework to notice problems like cost related problems, technology-related problems, human-technology-related problems, and legal problems that will influence or have an effect on the EMR adoption. Over that, the distinctive problems like budgets, number of beds and new or recent hospitals found by the researchers in the study are appeared on the framework. This study was carried out in relation to the healthcare system under the Malaysian government.
E. Unique ID number for patient’s
The wall street journal in the year 2012 published an article under the HealthCare column questioning the need for patients’ of having a Unique ID Number for All Medical Records. Reasons leading to this discussion being Lack of an easy, uniform way to identify patients and link them to their health data, doctors, hospitals, pharmacies, insurance plans and others throughout health care have created a sea of unrelated patient-identity numbers that are bogging down our medical-records system. This brought the question of importance of security in relation to health database.
F. RFID
Samaneh Madanian [8], in his work proposed the use of RFID as the unique patient identifier. In his study RFID has shown its potential to help healthcare systems enhance patient safety; as [9] reported, around 70% of the respondents to a Bearing Point Study believed that the most important implementation of RFID benefits patients by improving their safety. In another study [10], a combination of bar coding and RFID was examined to verify the patients’ medical and identification data
All these study point towards a need for a unique patient identifier for a 1:1 match when an individual’s details are searched in the big data pool and shows great concern for the security of the data.
Volume 5, Issue 4, May 2017 this case is however would such system uniquely determine
every patient and link him/her to composite medical records in one-to-one match [14].
Since this paper is focused totally on a nationwide unified healthcare database system for the purpose of sharing personal health data through a national health network that can improve the quality of health care. Thus first there is a need to analyse the options for identifying the patients uniquely. There are two approaches to accomplish this task (1) Statistical Matching and (2) Unique Patient identifier (UPI) [15].
1. Statistical Matching: Statistical matching tries to integrate enough data regarding an individual to form a unique key used to locate his/her electronic health record. It strings attributes such as: name, date of birth (DOB), contact number, address, and gender.The drawback in such key is that some attributes, like name, DOB, and postal code, don't seem to be unique to the individual; others, like address, could change overtime. As the database of records gets larger, additional personal attributes should be superimposed to keep the key distinctive.Searching algorithms utilized in this approach vary from requiring a precise match on a selected set of attributes or to more advance probabilistic pattern matching. The development of statistical matching depends on human to clarify queries and reduce ambiguity this is known as disambiguation.
2.Unique Patient Identifier: Unique patient identification is a technique for linking patients to their electronic medical records that exist globally in a domain (state, country, region, or world). The American Society for Testing and Materials (ASTM, 2000) Standard Guide lists desirable attributes of a UPI, including that it be:
Unique- Each UPI should be linked to only one individual i.e. different individualcannothave the same UPI.
Non disclosing- The UPI should not incorporate any personal information for instance name or DOB to prevent revealing the confidential info of the patient.
Invariable- The UPI should not change in the lifetime of an individual. Except in some exclusive cases like identity theft.
Canonical- Each person should be linked with only one UPI in order to prevent fragmentation of patient’s healthcare data.
Ubiquitous- Every individual should definitely have one UPI irrespective of age, gender, community or qualification.This is tough to attain, notably if participation is voluntary, however the alternative is a hybrid system, within which some patient information cannot be found employing a UPI.
Various government issued picture IDs available in India today are Voter ID card, Ration card, Driver’s Licence, Passport and UID (Aadhar card). Following is the result when these identifiers are analysed for the above mentioned UPI standards:
Voter ID Card: Voter IDs are not issued to an individual under the age of 18 years, this if used as an UPI limits inclusion of healthcare database for the minors.
Ration Card: Ration cards are generally issued for a family as a whole, and thus it violates the uniqueness of the UPI.
Driver’s Licence: Similar to the voter ID card, a driver’s licence is issued on the basis of age and driving skills, hence not making it available for every single individual.
Passport: Passport complies with all the above mentioned UPI except being ubiquitous, which suggest an alternate hybrid system, within which some patient information cannot be found using a UPI.
UID (Aadhar card): Though passport is in line with all the suggested UPI standards, the UID gives additional benefits of biometric details and QR scanning options for faster and more accurate results.
V.
EMR ADOPTION BY HOSPITALS IN INDIA We do have EMR record concepts in India, but the concept is not widely adopted. More and more hospitals are adopting it. Most of the Tier 1 cities based tertiary care and specialty hospitals have Patient and Healthcare Management's systems - but not a comprehensive EMR. The complete adoption process of the EMR system relies on these few factors: [15]1. Digitalisation of all the medical records maintained by the healthcare centres at all level.
Volume 5, Issue 4, May 2017 professionals and healthcareinstitutions are
required in order to deliver high-quality healthcare to the patient it serves.
3. Development of a unique patient identifier, to enable physicians, hospitals, patients and other authorized users to share clinical and administrative records more efficiently.
4. The highest level of security needed in context to the sensitivity of the data in concern.
The proposed system architecture deals with these factors to help in the adoption of the EMR framework in the Indian Healthcare system. The system is kept simple without any unwanted functionalities keeping its use easy to ensure more and more people using it. The system proposes to use one single patient database for all healthcare centres, making the data unified nationwide. It is suggested that Aadhar number should be the UPI in this case considering the large database already in use under it and the possibility of biometric verification of the user.
VI.
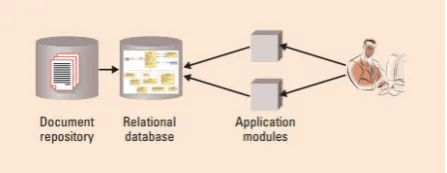
EMR ARCHITECTUREFor the EMR to be successful within the clinical community, it should have an appealing and responsive interface that has an upscale overview of data and effective search mechanisms for one patient at a time. Hence it is convenient to store data as a relational data model, even if it’s more common to search out document based primary information stores.
FIGURE 1.HIGH LEVEL ARCHITECTURE FOR AN EMR
For this reason, our most preferredEMR solution uses a relational database between the EMR interface and also the document store that is automatically updated once an information supplier uploads new documents (Figure 1). This relative database acts as associate degree application cache, during which the contents may be deleted and regenerated pro re nata as a result of the master data stored within the document repository.
Jens Edlef Møller and Henrik Vosegaard [11] in their work for Denmark’s Healthcare database mentioned that the
primary aspects of a basic EMR to be data collection and application which are often considered separately and might even be developed by different groups (integration architects and application developers, for example). But the overall solution should be designed with an end-to-end perspective in mindbecause application functionality depends on data structure and quality.
The proposed system divides the user base into categories according to the allowed visibility of data. Four different categories where identified for the system:
1. Pharmacy – This category has the minimum visibility of a patient’s medical record. As the only data required by them are the prescribed medicines to an individual.
2. Patient – A patient has been given the visibility of only his/her own data base. Though there is an option of sharing the database with other individual but only with consent from both the sharer’s and receiver’s end.
3. Doctor –They can view the record of any individual provided they have the UPI of the concerned patient.
4. Admin – They have access to the complete database of the system, including the doctor’s and pharmacy’s details.
VII.
EMR RELATIONAL DATABASEEMR relational database is a set of tables consisting information fitting into predefined classes concerning the patients. Every table (sometimes known as relation) contains one or more data classes in columns. Every row contains distinctive instance of information for the classes outlined by the columns. As an example, typical patient information would come with a table that describes a patient with columns for name, address, phone range etc. Another table would describe a malady: disease, patient, date. A practitioner who uses the information could obtain a view of the information that matches his needs. Fig 2 shows
Volume 5, Issue 4, May 2017 A relation is defined as a set of tuples that have the same the
attributes. A tuple represents an object and information about the object. Objects are typically physical objects or concepts. A relation is usually described as a table, which is organized into rows and columns. All the data referenced by an attribute are in the same domain and comply to the same constraints [13].
In some circumstances, there is a case to be made for extracting key clinical information (extraction), clean-up the information (transformation), and writing (loading) the data into a database specifically designed to ease data analysis; this operation is termed data cleansing. This method could be recurrent across multiple databases, providing uniform, concept-compatible data in “normalized” form. By performing this method and paring down the quantity of information, the dependability of research is enhanced and summarized information becomes accessible to be extracted and manipulated easily. Fig. 3 shows the above processes.
FIGURE 3.DATA CLEANSING PROCESS
VIII.
PROPOSED METHODOLOGYThis analysis aims to highlight one of the most necessary challenges that doctors face to have valuable data regarding their patients, that consequently aid them to give higher service. Patients might have more than one medical history in differentinstitutes that use different medical care systems. the need to connect the practitioner to just one shared system that holds all the patient’s medical records has been inflated as a must step to improve medical care services. This paper aims to shed light on the importance of medical records and therefore the need to improve the medical services provided to the patient in the country.
The proposed system first looks for the best available unique identification system that already exists with complete structured personnel details of the user. For this purpose UID (Aadhar card) issued by the government is the currently best available option. Alsothe UID database enables us to integrate the clinical database with the biometric verification. Here the databases in use are 1.The
UID database as maintained by the government 2.The nationwide unified clinical database and 3.Individual Doctor, Admin and Pharmacy database for each hospital using our service. Using the above mentioned databases the overlaying relational database is formed for the system (Fig 2).
As seen in Fig 3. Once the databases are ready the next step is the extraction of info. According to the search query the system will extract the required content from the relational database formed. This information is then transformed and brushed up according to the privileges under the logged in account. The final cleaned-up data is then sent to the UI for display.
The importance of biometric verification system can be seen in various cases of emergency, especially when the patient under observation is not in the condition to give out his information in order to get his medical history on time. In such cases the doctor will have an option of accessing the patients’ vital information using his finger print or his cornea image. This will speed up the diagnosis and treatment hence enabling the practitioners to give a better service.
IX.
DISCUSSIONStudies have shown a lot of advancement in digitalisation of the healthcare database, many countries have even a taken a step towards its implementation.The various levels of these studies show a growth chart starting from the need of a digitalised system for medical database to the use of radio frequency [8] to track the real time vitals of a patient. As for when we look into the Indian healthcare system only a bunch of high end hospitals and hospital chains have taken the initiative to keep a digitalised database.
Volume 5, Issue 4, May 2017
X.
FUTURE WORKFuture aspects of the proposed system include using the database for other greater purposes. One of this can be population based disease analysis; the database can be used to study the effects of various treatment methods, drugs and vaccines on very large data set, hence, providing precise and efficient study results. Other view in which the record can be used is Health Insurance monitoring and authentication: A module of the Software bundle can offer tools to use the medical history of the patients to monitor their previous record and authenticate insurance claims. But most of all it can be used to aid Crime Investigation. This database can be structured and utilised to meet the need of certain investigations where the medical history of suspects or victims might be required.
In views of an individual the further enhancement of the proposed system can be integrated with an RFID (Radio Frequency Identification).By using RFID, healthcare will be able to attain value saving and reduce patient death rate as a result of the human errors not only by real-time and precise data but conjointly through perceptive right service at right time for the correct person and with best quality.
XI.
CONCLUSIONA wide vary of things will have an effect on the adoption of EMR systems at large hospitals in developing countries. a large range of potential edges may be attributed to those systems, and a few of those edges, like reducing waiting times for patients, might indeed be bigger for hospitals in the developing world than within the developed world. The same as the developed world the environment at large hospitals in developing countries may be quite complicated.
The ultimate system that's implemented might have to incorporate options that pay special attention to accommodating sceptical users and people lacking IT skills. Take into account pursuing user interfaces that are very similar to paper records so as to assist users feel more comfortable with adopting the system. Social components of the system that include social and financial incentives to use the system, in addition as programs that facilitate promote computing outside the work context, may also prove valuable.
REFERENCES
[1]Haslina and Sharifah Mastura. Acceptance model of Electronic Medical
Record. Retrieved January, 3, 2011, at
http://www.docstoc.com/docs/39354269/JAIMS
[2] Boonstra, A. and Broekhuis, M. (2010, 6 August). Barriers to the acceptance of electronic medical records by physicians from systematic review to taxonomy and interventions. BMC Health Services Research 2010. Published online 2010 August 6. Retrieved January, 3, 2011 at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2924334/.
[3] Md. Zan Saari. (2007, 5 December). Kos Rawatan Mahal: Pilihan
di Tangan Pengguna. Retrieved April, 21, 2011, at
http://www.yadim.com.my/Kesihatan/KesihatanFull.asp?Id=175
[4] Rector, A.L., No lan, W.A., Kay ,S. "Foundations for an Electronic Medical Record." Methods of Information in Medicine .No 30,pp. 179- 186,1991.
[5] D. C. Leonard et al. Realization of a Universal Patient Identifier for Electronic Medical Records Through Biometric Technology Ieee Transactions On Information Technology In Biomedicine, Vol. 13, No. 4, July 2009
[6]Paul Carpenter and Christopher Chute, “The Universal Patient Identifier- A Discussion and Proposal”, Proc Annu Symp Comput Appl Med Care. 1993: 49–53.
[7] Nurul Izzatty Binti Ismail and Nor Hazana Binti Abdullah
“Developing Electronic Medical Records (EMR) Framework for Malaysia’s Public Hospitals”, 2011 IEEE Colloquium on Humanities,
Science and Engineering Research (CHUSER 2011), Dec 5-6 2011, Penang
[8] Samaneh Madanian “The Use of E-Health Technology in Healthcare
Environment: The Role of RFID Technology”, 10th International conference on e-commerce with focus on e-tourism 2016.
[9] H. J. Yazici, “An exploratory analysis of hospital perspectives on real time information requirements andperceived benefits of RFID technology
for future adoption,” International Journal of Information Management, vol.
34, no. 5, pp. 603-621, 2014.
[10] J. L. Wilkerson, and C. L. McDonald Jr, “RFID in healthcare,” The Journal of Organizational Leadership & Business Texas a& M University Tex Ark Ana, pp. 1-8, 2007.
[11]Jens Edlef Møller and Henrik Vosegaard “ Experiences with Electronic
Health Records” Healthcare IT PRO March/April 2008.
[12] Jeremiah Scholl et. al. “A case study of an EMR system at a large
hospital in India: Challenges and strategies for successful adoption”,
Journal of Biomedical Informatics Volume 44, Issue 6, December 2011, Pages
[13] J. Fong, S.M. Huang, a Frame Model Approach for Expert and Database System Integration, 1999.
Volume 5, Issue 4, May 2017
[15] RAND Corporation, Identity Crisis: An Examination of the Costs and Benefits of a Unique Patient Identifier for the U.S. Health care System, 2008. RAND Health, www .rand.org.
SushmitaSuman (1031320061)
Department of Computer Science and Engineering, SRM University, Ramapuram
CampusBharthiSalai, Ramapuram, Chennai-089, Tamil Nadu
Email ID: [email protected] Contact number: 9710326048 MsS.R.Rajeswari(M.E.) Assistant professor
Department of Computer Science and Engineering SRM University
Chennai, India
Email ID: [email protected] VaishaliPorwal (1031320070)
Department of Computer Science and Engineering, SRM University, Ramapuram Campus
BharthiSalai, Ramapuram, Chennai-089, Tamil Nadu
Email ID: [email protected] Jennifer Sneha (1031320093)
Department of Computer Science and Engineering, SRM University, Ramapuram Campus
BharthiSalai, Ramapuram, Chennai-089, Tamil Nadu