Ji-Feng Feng, Xing-Ming Zhou, Wei-Min Mao
Prognostic Analysis of Colorectal Cancer
Patients with Diabetes Mellitus in China
– the Experience of a Single Institution
Prognostyczna analiza chorych na raka jelita grubego i cukrzycę
w Chinach – doświadczenia jednej instytucji
Department of Oncological Surgery, Zhejiang Cancer Hospital, Hangzhou, China
Abstract
Background. Diabetes mellitus (DM) plays an important role in cancer prevalence and outcomes. Many studies have shown that DM increases the risk of colorectal cancer (CRC), but this association is controversial.
Objectives. The aim of this study was to investigate the outcomes and prognostic factors related to DM among CRC patients.
Material and Methods. A retrospective analysis was conducted of 773 patients with CRC treated at Zhejiang Cancer Hospital from January 2000 to December 2005. Based on medical records, the authors investigated the dif-ferences between patients with and without DM and analyzed the impact of DM among CRC patients. The overall cumulative probability of survival was calculated by the Kaplan-Meier method, and the difference between the two groups of patients was assessed by the log-rank test. Univariate and multivariate analyses using the Cox regres-sion proportional hazard model were performed to evaluate the prognostic parameters for survival. A conditional logistic regression analysis was also performed to evaluate the prognostic parameters for recurrence.
Results. Among the 773 patients, 75 patients had DM (9.70%). The mean age of the DM group was significantly higher than the non-DM group. The prevalence of CRC patients with DM was closely related to increasing age. The body mass index (BMI) was significantly higher in the DM group than in the non-DM group. The existence of lymph metastases was also significantly higher in the DM group than in the non-DM group. According to the Kaplan-Meier method, the five-year survival rate was 58.7% in the DM group and 65.3% in the non-DM group; no significant differences were found between the two groups in overall survival rates. A multivariate Cox regres-sion analysis of survival showed that TNM stage, lymph metastases, gross type and surgery type were significantly related to survival rates. A logistic regression analysis of recurrence showed that TNM stage (p = 0.005), lymph metastases (p = 0.002) and surgery type (palliative resection vs. radical resection, p = 0.036) were associated with a 3.648-fold, 11.938-fold and 11.004-fold increased risk of recurrence, respectively.
Conclusions. DM did not affect overall survival, but was associated with an increased risk of recurrence in patients with CRC (Adv Clin Exp Med 2011, 20, 4, 473–480).
Key words: colorectal cancer (CRC), diabetes mellitus (DM), prognostic analysis, recurrence, survival.
Streszczenie
Wprowadzenie. Cukrzyca (DM) odgrywa ważną rolę w występowaniu raka i wynikach leczenia. Wiele badań wykazało, że DM zwiększa ryzyko raka jelita grubego (CRC), ale ten związek jest kontrowersyjny.
Cel pracy. Zbadanie rezultatów leczenia i czynników prognostycznych związanych z cukrzycą wśród pacjentów z CRC.
Materiał i metody. Przeprowadzono retrospektywną analizę 773 pacjentów z CRC leczonych w Zhejiang Cancer Hospital od stycznia 2000 do grudnia 2005 r. Na podstawie dokumentacji medycznej autorzy badali różnice między pacjentami z DM i bez i ocenili wpływ DM wśród pacjentów z CRC. Łączne prawdopodobieństwo przeżycia obliczono metodą Kaplana-Meiera, a różnicę między dwiema grupami chorych oceniano za pomocą testu log- -rank. Przeprowadzono jednowymiarową i wielowymiarową analizę za pomocą modelu regresji proporcjonalnego hazardu Coxa w celu oceny czynników rokowniczych przeżycia. Przeprowadzono również warunkową regresję logistyczną do oceny czynników rokowniczych nawrotu choroby.
Adv Clin Exp Med 2011, 20, 4, 473–480 ISSN 1230-025X
ORIgINAl PAPERS
China is a country with a large population, and it is experiencing an increasing number of diabetes mellitus (DM) cases, with an estimated 42.3 million patients predicted by 2030 [1]. Many studies have revealed that a history of DM significantly increases the incidence of cancer [2–5]. The association be-tween DM and colorectal cancer (CRC) has been studied most actively. Many reports have demon-strated that the risk of CRC is increased in DM patients [6, 7]. In addition, a meta-analysis of epi-demiologic studies reported that DM is associated with a moderate increased risk of CRC overall [8].
As the prevalence of DM increases, the preva-lence of CRC with DM will increase. There are, however, still controversies about how DM affects outcomes in patients with CRC. The aim of this study was to investigate the outcomes and prognos-tic factors related to DM among CRC patients.
Material and Methods
A retrospective analysis was conducted of 773 patients with CRC treated at Zhejiang Cancer Hos-pital from January 2000 to December 2005. Among the 773 patients, 75 cases (9.7%) had DM; among these, two patients had diabetes type 1 and 73 pa-tients had diabetes type 2. Standardized criteria were used to identify DM: two consecutive fasting glucose levels ≥ 7.0 mmol/l (126 mg/dl) or both 1- and 2-hour blood levels ≥ 11.1 mmol/l (200 mg/ dl) obtained during a standard oral glucose toler-ance test. All the patients underwent colorectal surgery (radical resection or palliative resection), and a final CRC diagnosis of adenocarcinoma was confirmed by histopathology. The mean follow-up duration was 4.5 years.
On the basis of the patients’ medical records, the authors investigated the differences between the CRC patients with and without DM. The relationship between DM and such factors as
age, gender, body mass index (BMI), tumor size and location, the existence of lymph metastases, TNM stage, histological differentiation, gross type, surgery type, recurrence and survival was analyzed.
Statistical Analysis
The statistical analysis was conducted with SPSS 17.0 software (SPSS Inc., Chicago, Il, USA). The distribution of baseline characteristics be-tween patients with and without DM patients was evaluated using either Fisher’s exact or χ2 tests in the case of categorical variables or the Student’s t-test in the case of continuous variables. The over-all cumulative probability of survival was calculat-ed by the Kaplan-Meier method, and the difference between the two groups of patients was assessed by the log-rank test. Univariate and multivariate analyses using the Cox regression proportional hazard model were performed to evaluate the prognostic parameters for survival. A conditional logistic regression analysis was also performed to evaluate the prognostic parameters for recurrence. A p-value less than 0.05 was considered to be sta-tistically significant.
Results
The baseline characteristics for the DM and non-DM patients are presented in Table 1. The mean age of the DM group was 62.5 ± 10.8 years (range: 37 to 84 years), which was significantly higher than the non-DM group’s mean age of 56.8 ± 7.5 (p = 0.012). The prevalence of CRC patients with DM was closely related to age (r = 0.824,
p = 0.023): 3.30% for patients < 40 years in age (3/91), 5.53% for the 40–49-year-olds (14/253), 8.85% for the 50–59-year-olds (17/192), 20.31%
Wyniki. Wśród 773 pacjentów 75 chorowało na cukrzycę (9,70%). Średni wiek pacjentów chorych na cukrzycę był znacznie większy niż w grupie bez cukrzycy. Częstość występowania CRC u chorych na cukrzycę była ściśle związana z wiekiem. Wskaźnik masy ciała (BMI) był znacząco większy w grupie z cukrzycą niż w grupie bez cukrzy-cy. Istnienie przerzutów do węzłów chłonnych było istotnie większe w grupie z cukrzycą niż w grupie bez cukrzycukrzy-cy. Według metody Kaplana-Meiera, 5-letnie przeżycie miało 58,7% pacjentów w grupie z cukrzycą i 65,3% w grupie bez cukrzycy, nie stwierdzono istotnych różnic między grupami w ogólnej przeżywalności. Wieloczynnikowa anal-iza regresji Coxa dotycząca przeżycia wykazała, że stadium TNM, przerzuty do węzłów chłonnych, typ makrosko-powy i rodzaj zabiegu były istotnie związane z czasem przeżycia. Analiza regresji logistycznej nawrotu wykazała, że stopień TNM (p = 0,005), przerzuty do węzłów chłonnych (p = 0,002) i rodzaj operacji (resekcja paliatywna vs
radykalna resekcja, p = 0,036) wpływają na odpowiednio 3.648-krotnie, 11,938-krotnie i 11,004-krotnie większe ryzyko nawrotu.
Wnioski. Cukrzyca nie wpływa na całkowity czas przeżycia, ale wiąże się ze zwiększonym ryzykiem nawrotu u cho-rych z CRC (Adv Clin Exp Med 2011, 20, 4, 473–480).
tween the two groups in tumor size and location, gross type, TNM stage, histological differentiation and surgery type. Tumor recurrence was signifi-cantly higher in the DM group than in the non-DM group (29.3% vs.16.6%; p = 0.010).
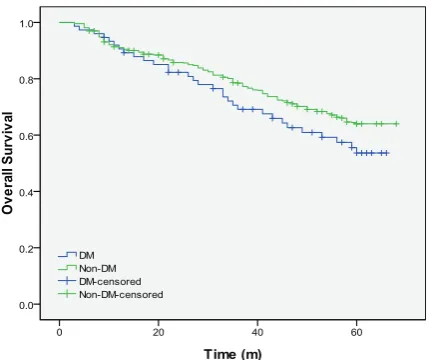
According to the Kaplan-Meier method, the five-year survival rate was 58.7% in the DM group and 65.3% in the non-DM group; no significant differences were found between the two groups in overall survival rates (Fig. 2; p = 0.099). In a uni-variate Cox regression analysis of survival (Table 2), there were significant differences in TNM stage (Fig. 3A; p = 0.004), lymph metastases (Fig. 3B; for the 60–69-year-olds (26/128), 14.10% for the
70–79-year-olds (11/78) and 12.90% for the pa-tients > 80 years (4/31) (Fig.1). Among the sub-jects, 454 (58.7%) were male and 319 were female (41.3%), and there was no significant difference in gender distribution between the DM and non-DM groups (p = 0.388). The body mass index (BMI) was significantly higher in the DM group than in the non-DM group (25.3 ± 2.4 kg/m2 vs. 23.8 ± 3.7 kg/m2; p = 0.003). The existence of lymph metasta-ses was also significantly higher in the DM group than in the non-DM group (37.3% vs. 25.2%; p = 0.027). There were no significant differences
be-Table 1. Baseline characteristics of colorectal cancer (CRC) patients with and without diabetes mellitus (DM)
Tabela 1. Wyjściowa charakterystyka chorych na raka jelita grubego (CRC) z i bez cukrzycy (DM) DM (n = 75 cases)
(Chorzy na cukrzycę) Non-DM (n = 698 cases)(Chorzy bez cukrzycy) P-value
Age – years (Wiek – lata) 62.5 ± 10.8 56.8 ± 7.5 0.012
gender – n, % (Płeć) male
female 48 (64.0)27 (36.0) 406 (58.2)292 (41.8)
0.388
BMI (kg/m2) 25.3 ± 2.4 23.8 ± 3.7 0.003
Tumor size – cm (Rozmiar guza – cm) 5.1 ± 2.6 4.8 ± 1.8 0.126
Tumor location – n, % (Umiejscowienie guza) colon
rectum 22 (29.3)53 (70.7) 157 (22.5)541 (77.5)
0.195
TNM stage – n, % (Klasyfikacja TNM) I
II III IV
14 (18.7) 35 (46.7) 19 (25.3) 7 (9.3)
79 (11.3) 378 (54.2) 163 (23.4) 28 (4.1)
0.063
lymph metastases – n, % (Przerzuty do węzłów chłonnych) no
yes 47 (62.7)28 (37.3) 523 (74.8)176 (25.2)
0.027
gross type – n, % (Typ makroskopowy) mass
infiltrative ulcerative
42 (56.0) 27 (36.0) 6 (8.0)
347 (49.7) 234 (33.8) 117 (16.8)
0.141
Differentiation – n, % (Zróżnicowanie) good
moderate poor
17 (22.7) 51 (68.0) 7 (9.3)
153 (22.0) 436 (62.5) 109 (15.5)
0.345
Surgery type – n, % (Rodzaj operacji) radical resection
palliative resection 67 (89.3)8 (10.7) 657 (94.1)42 (5.9)
0.134
Recurrence – n, % (Nawroty) no
yes 53 (70.7)22 (29.3) 582 (83.4)116 (16.6)
0.010
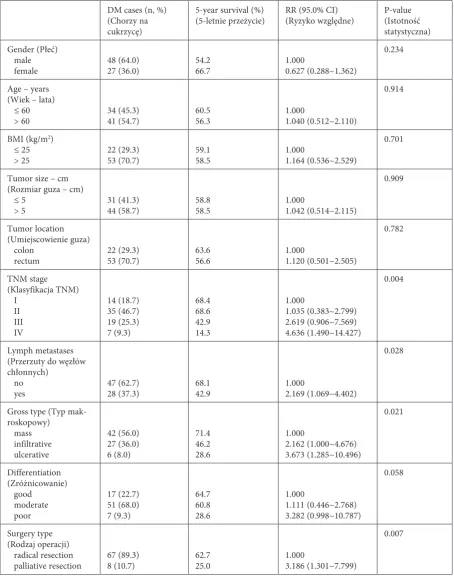
p = 0.028), gross type (Fig. 3C; p = 0.021), and sur-gery type (Fig. 3D; p = 0.007). Differentiation was not an influential parameter for the survival rate (p = 0.058), but the five-year survival was higher in
the cases of well-differentiated and moderately-dif-ferentiated tumors than poorly-difmoderately-dif-ferentiated ones (64.7, 60.8 and 28.6% respectively). A conditional multivariate Cox regression analysis of survival
Table 2. Univariate Cox regression analysis of overall survival for CRC patients with DM
Tabela 2. Jednoczynnikowa analiza regresji Coxa całkowitego przeżycia dla pacjentów z CRC i cukrzycą
DM cases (n, %) (Chorzy na cukrzycę)
5-year survival (%)
(5-letnie przeżycie) RR (95.0% CI)(Ryzyko względne) P-value(Istotność statystyczna) gender (Płeć)
male
female 48 (64.0)27 (36.0) 54.266.7 1.0000.627 (0.288~1.362)
0.234
Age – years (Wiek – lata) ≤ 60
> 60 34 (45.3)41 (54.7) 60.556.3 1.0001.040 (0.512~2.110)
0.914
BMI (kg/m2)
≤ 25
> 25 22 (29.3)53 (70.7) 59.158.5 1.0001.164 (0.536~2.529)
0.701
Tumor size – cm (Rozmiar guza – cm) ≤ 5
> 5 31 (41.3)44 (58.7) 58.858.5 1.0001.042 (0.514~2.115)
0.909
Tumor location (Umiejscowienie guza) colon
rectum 22 (29.3)53 (70.7) 63.656.6 1.0001.120 (0.501~2.505)
0.782
TNM stage (Klasyfikacja TNM) I
II III IV
14 (18.7) 35 (46.7) 19 (25.3) 7 (9.3)
68.4 68.6 42.9 14.3
1.000
1.035 (0.383~2.799) 2.619 (0.906~7.569) 4.636 (1.490~14.427)
0.004
lymph metastases (Przerzuty do węzłów chłonnych)
no
yes 47 (62.7)28 (37.3) 68.142.9 1.0002.169 (1.069~4.402)
0.028
gross type (Typ mak-roskopowy)
mass infiltrative ulcerative
42 (56.0) 27 (36.0) 6 (8.0)
71.4 46.2 28.6
1.000
2.162 (1.000~4.676) 3.673 (1.285~10.496)
0.021
Differentiation (Zróżnicowanie) good
moderate poor
17 (22.7) 51 (68.0) 7 (9.3)
64.7 60.8 28.6
1.000
1.111 (0.446~2.768) 3.282 (0.998~10.787)
0.058
Surgery type (Rodzaj operacji) radical resection
palliative resection 67 (89.3)8 (10.7) 62.725.0 1.0003.186 (1.301~7.799)
0.007
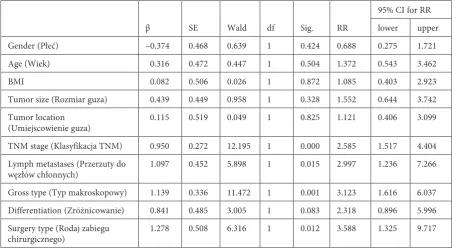
Table 3. Multivariate Cox regression analysis of overall survival for CRC patients with DM
Tabela 3. Wieloczynnikowa analiza regresji Coxa całkowitego przeżycia pacjentów z CRC i DM
β SE Wald df Sig. RR
95% CI for RR lower upper
gender (Płeć) –0.374 0.468 0.639 1 0.424 0.688 0.275 1.721
Age (Wiek) 0.316 0.472 0.447 1 0.504 1.372 0.543 3.462
BMI 0.082 0.506 0.026 1 0.872 1.085 0.403 2.923
Tumor size (Rozmiar guza) 0.439 0.449 0.958 1 0.328 1.552 0.644 3.742
Tumor location
(Umiejscowienie guza) 0.115 0.519 0.049 1 0.825 1.121 0.406 3.099
TNM stage (Klasyfikacja TNM) 0.950 0.272 12.195 1 0.000 2.585 1.517 4.404 lymph metastases (Przerzuty do
węzłów chłonnych) 1.097 0.452 5.898 1 0.015 2.997 1.236 7.266
gross type (Typ makroskopowy) 1.139 0.336 11.472 1 0.001 3.123 1.616 6.037 Differentiation (Zróżnicowanie) 0.841 0.485 3.005 1 0.083 2.318 0.896 5.996 Surgery type (Rodaj zabiegu
chirurgicznego) 1.278 0.508 6.316 1 0.012 3.588 1.325 9.717
BMI – body mass index, RR – risk ratio, CI – confidence interval. BMI – wskaźnik masy ciała, RR – ryzyko względne, CI – przedział ufności.
Table 4. logistic regression analysis of recurrence for CRC patients with DM
Tabela 4. Analiza regresji logistycznej nawrotu dla pacjentów z CRC i DM
β S.E. Wald df Sig. OR
95% CI for OR lower upper
gender (Płeć) –0.270 0.785 0.119 1 0.731 0.763 0.164 3.554
Age (Wiek) –0.549 0.746 0.543 1 0.461 0.577 0.134 2.491
BMI 0.352 0.799 0.194 1 0.660 1.421 0.297 6.809
Tumor size (Rozmiar guza) 0.217 0.687 0.100 1 0.752 1.242 0.323 4.779
Tumor location
(Umiejscowienie guza) 0.223 0.782 0.081 1 0.776 1.250 0.270 5.789
TNM stage (Klasyfikacja TNM) 1.294 0.460 7.897 1 0.005 3.648 1.479 8.994
lymph metastases (Przerzuty do
węzłów chłonnych) 2.480 0.816 9.243 1 0.002 11.938 2.414 59.043
gross type (Typ makroskopowy) 0.476 0.501 0.899 1 0.343 1.609 0.602 4.299 Differentiation (Zróżnicowanie) 0.564 0.638 0.780 1 0.377 1.757 0.503 6.136 Surgery type (Rodaj zabiegu
chirurgicznego) 2.398 1.146 4.381 1 0.036 11.004 1.165 103.959
showed that TNM stage (risk ratio [RR] = 2.585, 95% confidence interval [CI] 1.517 to 4.404; p = 0.000), lymph metastases (RR = 2.997, 95% CI 1.236 to 7.266;
p = 0.015), gross type (RR = 3.123, 95% CI 1.616 to 6.037; p = 0.001), and surgery type(RR = 3.588, 95% CI 1.325 to 9.717; p = 0.012) were significantly related to survival rates (Table 3). A logistic regres-sion analysis of recurrence showed that TNM stage (p = 0.005), lymph metastases (p = 0.002) and sur-gery type(palliative resection vs. radical resection,
p = 0.036) were associated with a 3.648, 11.938 and 11.004-fold increase in the risk of recurrence, re-spectively (Table 4).
Discussion
In the baseline parameters, the present study found no significant differences between patients
with and without DM regarding gender, tumor size and location, TNM stage, histological differentia-tion, gross type and surgery type. However, as shown in Table 1, DM patients were significantly older and had lymph metastases and tumor recurrences more frequently than non-DM patients. These results are in agreement with several other previous reports [9–11]. In the present study, the prevalence of DM among CRC patients was closely related to age (r = 0.824, p = 0.023): A larger proportion of patients with DM were 60–69 years old, while in the study of Shonka et al. [12] a larger proportion of patients with DM were ≥ 70 years at the time of diagnosis.
There have been several reports showing that the prognosis for colorectal cancer is poor in DM patients. In a study conducted with 3759 surgi-cally-treated CRC patients, the five-year survival rate was significantly lower in DM patients (57%) compared with non-DM patients (66%); the same study also showed that DM patients had a 42% in-creased risk of death from any cause and a 21% increased risk for recurrence after adjustment for other predictors of colon cancer [13]. Siddiqui et al. [14] suggested a correlation between poor glycemic control and a clinically aggressive course for CRC in DM patients, and a meta-analysis by Stein et al. [15] indicated that among CRC patients with DM the all-cause mortality rate is 32% higher than in patients without DM[16].However, since Meyerhardt et al. [13] found that the cancer recur-rence rate was higher in DM patients, it may be that the increased recurrence associated with DM is what led to the increased mortality rate.
There are, however, still controversies about how DM affects outcomes in CRC patients. An epidemiological study by Kune et al. [17] reported that the prevalence of DM in CRC patients was the same as in the control group. Will et al. [18] re-ported that the risk of colorectal cancer was high-er in DM patients, but found no diffhigh-erence in the mortality rate among DM patients. In addition, Shonka et al. [12] showed that DM did not affect either the stage at diagnosis or outcomes from co-lon cancer, and Jullumstrø et al. [19] indicated that DM is not a factor affecting TNM stage, tumor dif-ferentiation at presentation, the type of treatment or the short-term outcome from CRC.
The present study found that the five-year survival rate in the DM group (58.7%) was sig-nificantly lower than the non-DM group (65.3%) (p = 0.099), suggesting that DM may negatively influence outcomes of CRC patients. Considering the fact that the recurrence rate in DM patients was significantly higher than in the non-DM patients (p = 0.010), this result coincides with the conclu-sion of Meyerhardt et al. [13] and Stein et al. [15], but differs from the findings of Noh et al. [11]. 0
50 100 150 200 250 300
< 40 40–49 50–59 60–69 70–79 > 80 age (years)
number (n)
0.00% 5.00% 10.00% 15.00% 20.00% 25.00%
percentage (%)
total cases DM cases percentage
Fig. 1. The prevalence of CRC patients with DM was closely related to increasing age
Ryc. 1. Częstość występowania CRC u chorych na cukrzycę była ściśle związana z wiekiem
Fig. 2. Kaplan-Meier survival curves of overall survival for CRC patients with and without DM (p = 0.099)
In the present study, TNM stage, lymph me-tastases, gross type and surgery type had signifi-cant impact on survival, and TNM stage, lymph metastases and surgery type were also significantly related to recurrence rates in CRC patients with DM. In conclusion, this study found that the prev-alence of DM among CRC patients was closely re-lated to age. DM did not affect overall survival, but was associated with an increased risk of recurrence in patients with CRC.
There potential limitations of the present study include the relatively small number of patients, as well as the fact that the prognostic analysis was ret-rospective, the mean follow-up duration was short and the study was conducted by a single institution. Moreover, it did not provide enough information on the details of the treatment of DM patients.
Fig. 3. Kaplan-Meier survival curves according to the TNM stage (3A; p = 0.004); according to lymph metastases (3B;
p = 0.028); according to gross type (3C; p = 0.021); and according to type of surgery (3D; p = 0.007)
Ryc. 3. Krzywe przeżycia Kaplana-Meiera w zależności od klasyfikacji TNM (3A, p = 0,004), od przerzutów do węzłów chłonnych (3B, p = 0,028); od typu makroskopowego (3C, p = 0,021) oraz w zależności od rodzaju operacji chirurgicznej (3D, p = 0,007)
A B
C D
References
[1] Wild S, Roqlic G, Green A, Sicree R, King H: global prevalence of diabetes: estimates for the year 2000 and pro-jections for 2030. Diabetes Care 2004, 27, 1047–1053.
[3] Veldt BJ, Chen W, Heathcote EJ, Wedemeyer H, Reichen J, Hofmann WP, de Knegt RJ, Zeuzem S, Manns MP, Hansen BE, Schalm SW, Janssen HL: Increased risk of hepatocellular carcinoma among patients with hepatitis C cirrhosis and diabetes mellitus. Hepatology 2008, 47, 1856–1862.
[4] Larsson SC, Orsini N, Brismar K,Wolk A: Diabetes mellitus and risk of bladder cancer: A meta-analysis. Diabetologia 2006, 49, 2819–2823.
[5] Larsson SC, Mantzoros CS, Wolk A: Diabetes mellitus and risk of breast cancer: A meta-analysis. Int J Cancer 2007, 121, 856–862.
[6] Limburg PJ, Vierkant RA, Fredericksen ZS, Leibson CL, Rizza RA, Gupta AK, Ahlquist DA, Melton LJ 3rd, Sellers TA, Cerhan JR: Clinically confirmed type 2 diabetes mellitus and colorectal cancer risk: A population-based, retrospective cohort study. Am J gastroenterol 2006, 101, 1872–1879.
[7] Yang YX, Hennessy S, Lewis JD: Type 2 diabetes mellitus and the risk of colorectal cancer. Clin gastroenterol Hepatol 2005, 3, 587–594.
[8] Larsson SC, Orsini N, Wolk A: Diabetes mellitus and risk of colorectal cancer: A meta-analysis. J Natl Cancer Inst 2005, 97, 1679–1687.
[9] Payne JE, Meyer HJ: The influence of other diseases upon the outcome of colorectal cancer patients. Aust N Z J Surg 1995, 65, 398–402.
[10] Polednak AP: Comorbid diabetes mellitus and risk of death after diagnosis of colorectal cancer: A population- -based study. Cancer Detect Prev 2006, 30, 466–472.
[11] Noh GY, Hwang DY, Choi YH, Lee YY: Effect of diabetes mellitus on outcomes of colorectal cancer. J Korean Soc Coloproctol 2010, 26, 424–428.
[12] Shonka NA, Anderson JR, Panwalkar AW, Reed EC, Steen PD, Ganti AK: Effect of diabetes mellitus on the epidemiology and outcomes of colon cancer. Med Oncol 2006, 23, 515–519.
[13] Meyerhardt JA, Catalano PJ, Haller DG, Mayer RJ, Macdonald JS, Benson AB 3rd, Fuchs CS: Impact of diabe-tes mellitus on outcomes in patients with colon cancer. J Clin Oncol 2003, 21, 433–440.
[14] Siddiqui AA, Spechler SJ, Huerta S, Dredar S, Little BB, Cryer B: Elevated HbA1c is an independent predic-tor of aggressive clinical behavior in patients with colorectal cancer: a case-control study. Dig Dis Sci 2008, 53, 2486–2494.
[15] Stein KB, Snyder CF, Barone BB, Yeh HC, Peairs KS, Derr RL, Wolff AC, Brancati FL: Colorectal cancer outcomes, recurrence and complications in persons with and without diabetes mellitus: a systematic review and meta-analysis. Dig Dis Sci 2010, 55, 1839–1851.
[16] Chen CQ, Fang LK, Cai SR, Ma JP, Yang GX, Yang W, Zhan WH, He YL: Effects of diabetes mellitus on prog-nosis of the patients with colorectal cancer undergoing resection: a cohort study with 945 patients. Chin Med J (Engl) 2010, 123, 3084–3088.
[17] Kune GA, Kune S, Watson LF: Colorectal cancer risk, chronic illnesses,operations and medications: case control results from the Melbourne Colorectal Cancer Study 1988. Int J Epidemiol 2007, 36, 951–957.
[18] Will JC, Galuska DA, Vinicor F, Calle EE: Colorectal cancer: another complication of diabetes mellitus? Am J Epidemiol 1998, 147, 816–825.
[19] Jullumstrø E, Kollind M, Lydersen S, Edna TH: Diabetes mellitus and outcomes of colorectal cancer. Acta Oncol 2009, 48, 361–367.
Address for correspondence:
Ji-Feng Feng
Department of Oncological Surgery Zhejiang Cancer Hospital
No. 38 guangji Road Hangzhou
China
Tel.: +86-0571-88122038 E-mail: [email protected]
Conflict of interest: None declared