M
ARTAM
ADEJ1, M
AGDALENAS
OKALSKA−J
URKIEWICZ1, B
EATAN
OWAK1, A
NNAC
ZARNY2,
E
WAZ
ACZYŃSKA2, P
IOTRW
ILAND1The Activity of STAT−3 in Patients
With Rheumatoid Arthritis
Ocena aktywności czynnika STAT−3 u pacjentów
chorych na reumatoidalne zapalenie stawów
1 Department of Rheumatology and Internal Diseases Silesian Piasts University of Medicine in Wrocław, Poland 2 Department of Infectious Diseases, Institute of Immunology and Experimental Therapy, Polish Academy
of Sciences, Wrocław, Poland
Adv Clin Exp Med 2008, 17, 4, 405–409 ISSN 1230−025X
ORIGINAL PAPERS
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Background.This study of Jak/STAT activation in RA describes constitutive STAT−3 DNA binding activity in freshly isolated RA mononuclear cells. Data suggest that rheumatoid arthritis synovial fibroblast survival and their abnormal phenotype are dependent on STAT−3. The objective was to evaluate the activity of STAT−3 in peripheral blood leucocytes in patients with RA and compare it with parameters of disease activity used in clinical practice. Material and Methods. Thirty−five patients (28 females, 80%) who met the revised American College of Rheumatology criteria for rheumatoid arthritis and 30 healthy controls (20 females, 67%) were enrolled in the study. Venous blood samples were taken from all participants. STAT−3 activity was measured by an immunocyto− chemical method in peripheral blood leukocytes as the percentage of stained cells per hundred cells. Blood sam− ples were also taken from all patients to measure ESR, CRP, WBC, RBC, PLT, and hemoglobin level. X−rays of the hands were also taken. DAS28 and HAQ were also determined.
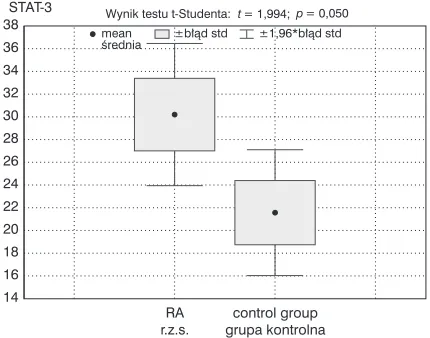
Results.Mean DAS28 was 5.04 (range: 2.4–8.2). Of the 35 RA patients, 25 (71%) had positive rheumatoid factor and erosive changes of the hand was found in 20 (57%). In the RA (women compared with the healthy controls, the activity of STAT−3 was higher (28.3 ± 18.4% vs. 18.2 ± 13.5%, p< 0.05). Comparing STAT−3 in the whole pop− ulation of RA patients and in the controls, the correlation was on the borderline of significance (30.2 ± 18.9% vs. 21.6 ± 15.5%, p= 0.05). Correlations between STAT−3, WBC (Rp= –0.39, p< 0.05), and RBC (Rp= 0.36, p< 0.05) in RA patients were observed. There was also correlation between STAT−3 activity and disease duration (Rp= 0.445827,
p< 0.05). No correlation was seen between STAT−3 activity evaluated in white blood cells and values of HAQ, DAS28, ESR, CRP, platelets, hemoglobin, hematocrit, and number of swollen and painful joints.
Conclusions.The activity of STAT−3 was higher in RA patients (significantly higher in RA women) than in a group of healthy controls. No significant correlation was found in this group between STAT−3 and the parameters of RA activity, except for WBC and RBC. This is a preliminary study and a larger group of RA patients is needed for sta− tistically significant conclusions (Adv Clin Exp Med 2008, 17, 4, 405–409).
Key words:rheumatoid arthritis, STAT−3.
Streszczenie
Wprowadzenie. Współczesne badania nad patogenezą r.z.s. zwracają uwagę na nieprawidłowy fenotyp synowio− cytów przejawiający się opornością na apoptozę oraz nadmierną ich proliferacją zależną od czynnika STAT−3. Cel pracy. Ocena aktywności STAT−3 w leukocytach krwi obwodowej u chorych na r.z.s. oraz porównanie z kla− sycznymi wykładnikami aktywności choroby.
Materiał i metody. Do badania zakwalifikowano 35 chorych spełniających kryteria rozpoznania r.z.s. (wg ACR) oraz 30 osób zdrowych stanowiących grupę kontrolną. Analizy aktywności czynnika STAT−3 dokonywano w leu− kocytach krwi obwodowej metodą immunocytochemiczną, sumując liczbę zabarwionych komórek na sto ocenia− nych w preparacie. U każdego chorego określano ponadto DAS28, HAQ, a także oceniano następujące parametry morfotyczne krwi WBC, RBC, PLT, Hb, MCV oraz OB i CRP.
Rheumatoid arthritis (RA) is the most com− mon form of inflammatory joint disease. The destruction of cartilage by inflammatory tissue, known as pannus, consisting of proinflammatory cells (macrophages and synovial fibroblasts) that produce cytokines, chemokines, and angiogenic factors, is very characteristic in the course of dis− ease [1]. Changes in the synovium are crucial to the inflammatory process that occurs in RA. In the typical case, RA is bilateral symmetric polyarthri− tis involving small and large joints in the upper and lower extremities. In most patients, small proximal joints of the fingers and toes as well as the ankles or wrists are the first to become affect− ed. Along with articular signs, systemic symptoms such as fatigue, malaise, weight loss, anemia, and thrombocytosis may be present. In the case of sys− temic RA, other extra−articular manifestations may occur. These comprise systemic vasculitis, pulmonary nodules, interstitial fibrosis, secondary amyloidosis, pericarditis, and keratoconjunctivitis sicca.
RA affects about 0.5–1 per cent of the popula− tion and women suffer more than men at a ratio of 3 to 1. The etiology and pathogenesis of the dis− ease are not clear. The cytokines produced by the cells involved in the inflammatory process seem to play a key role in the pathogenesis of RA. Some cytokines act through the members of the Jak/STAT family (Janus kinase/Signal Transducer and Activator of Transcription), a group of factors involved in cellular activation, proliferation, and differentiation through the regulation of gene expression. The Jak/STAT pathway seems to be an important element in the pathogenesis of RA. Cytokines, after binding to their receptors, activate Jak kinases, which are responsible for tyrosine phosphorylation and the activation of latent cyto− plasmic transcription factors, STATs. After phos− phorylation, STATs dimerize and then translocate to the nucleus where, after binding to DNA, they activate transcription [2]. There are seven known
members of the mammalian STAT family, STAT1− STAT6 (including STAT5A and STAT5B). Although each STAT protein can be activated by multiple ligands, some cytokines preferentially activate particular STATs; for example, interleukin 6 (IL−6) and IL−10 preferentially activate STAT−3.
Material and Methods
Thirty−five patients who met the revised American College of Rheumatology criteria for definite rheumatoid arthritis and thirty healthy subjects participating as a control group were enrolled in the study. All the patients with RA were treated with disease−modifying anti−rheumat− ic drugs (DMARDs), excluding TNF blockers. Venous blood samples were taken from each of the participants. The activity of STAT−3 was measured by an immunocytochemical method in peripheral blood leucocytes which were separated using den− sity gradient. The detection of STAT−3 was done using anti−STAT−3 antibodies (commercial tests: Chemicon Intern. Inc., USA) and agents for color reaction (Novocastain Super ABC Kit, Novocastra DAB Substrate Kit for Peroxidase, Newcastle, UK). The result was expressed as the percentage of stained cells in each group of one hundred cells. The final value was the mean of three independent samples. Blood samples were also taken from each of the patients to measure the erythrocyte sedi− mentation rate (ESR) and the levels of C−reactive protein (CRP), white blood cells (WBC), red blood cells (RBC), platelets (PLT), and hemoglo− bin. X−rays of the hands were also taken. The dis− ease activity score (DAS28) and Health Assessment Questionnaire (HAQ) were deter− mined.
Statistical analysis was done using the Statistica program. The parametric distribution of the variables was verified with the Shapiro−Wilk and Liliefors test. When continuous variables met
U 71% badanych stwierdzono seropozytywną postać choroby, a u 57% obecność zmian radiologicznych odpowia− dających III–IV okresowi zaawansowania wg Steinbrockera. Różnica aktywności czynnika STAT−3 w grupie ba− danej w porównaniu do grupy kontrolnej znajdowała się na granicy istotności statystycznej (30,2% SD 18,9% vs
21,6% SD 15,5%, p = 0,05), była natomiast istotnie statystycznie większa wśród chorych na r.z.s. kobiet w porów− naniu ze zdrowymi (28,3% SD 18,4% vs18,2% SD 13,5%, p < 0,05). Stwierdzono istotną statystycznie zależność między STAT−3 a stężeniem leukocytów i czerwonych krwinek w badanej grupie. Nie obserwowano korelacji mię− dzy STAT−3 a klasycznymi wskaźnikami aktywności choroby (DAS28, OB, CRP, stężenie hemoglobiny, płytek krwi czy liczba bolesnych i obrzękniętych stawów).
Wnioski. W przedstawionym badaniu zaobserwowano większą aktywność STAT−3 wśród kobiet chorych na r.z.s. w stosunku do grupy kontrolnej. Różnica ta była mniej istotna w odniesieniu do całości badanej grupy. Nie obser− wowano różnic w aktywności STAT−3 w zależności od aktywności choroby ani jej zaawansowania radiologiczne− go (Adv Clin Exp Med 2008, 17, 4, 405–409).
the assumptions for a parametric distribution, the Student t−test was used for comparison between groups. Variables not meeting the distribution assumptions were analyzed using the Mann− Whitney Utest, Wilcoxon test, Kruskal−Wallis test, and Friedman test. The correlations were estab− lished by Spearman’s correlation test and, when a linear correlation was detected, the Pearson coef− ficient was determined. Two−sided P values less than 0.05 were considered as significant.
The study was approved by the Silesian Piasts University of Medicine’s Local Bioethics Committee and all the subjects gave their written informed consents before they entered the study. Funds was received from a Silesian Piasts Medical University of Medicine grant.
Results
The study included thirty−five (28 females, 80%) RA patients and thirty controls (20 females, 67%). The RA patients were divided into three
groups according to DAS28 value: group A with low disease activity (DAS28 ≤3.2) and including 3 patients (9%), group B with moderate disease activity (3.2 < DAS28 ≤ 5.1) and 15 patients (43%), and group C with high disease activity (DAS28 > 5.1) and 17 patients (48%). The mean value of DAS28 in each group of disease activity was 2.66 in group A, 4.23 in group B, and 6.18 in group C. The mean age of the RA patients was 55.6 (range: 27–74) years. Of the 35 RA patients, 25 (71%) had positive rheumatoid factor and ero− sive changes of the hand were found in 20 (57%). Mean disease duration was 12.97 (range 1–39) years. The mean duration of morning stiffness was 91 (range: 0–300) minutes.
In the women with RA the activity of STAT−3 was higher than in the healthy control population (mean ± SD: 28.3 ± 18.4% vs. 18.2 ± 13.5%, p < 0.05) (Table 1). Comparing STAT−3 in the whole population of RA patients and in the control group, the correlation was on the borderline of significance (30.2 ± 18.9% vs. 21.6 ± 15.5%, p= 0.05) (Fig. 1). Correlations between STAT−3 and WBC
Table 1. Comparison of STAT−3 activity between RA patients and healthy subjects
Tabela 1.Porównanie aktywności STAT−3 w grupie chorych na r.z.s. oraz w grupie kontrolnej
STAT−3 RA patients Control group
(Chorzy na r.z.s.) (Grupa kontrolna)
STAT−3 n= 35 n= 30 p= 0.050
mean value (wartość średnia) 30.2 21.6
standard deviation SD
(odchylenie standardowe) 18.9 15.5
median xmed
(mediana xmed) 27 18
minimum value xmin
(wartość minimalnaxmin) 0 2
maximum value xmax
(wartość maksymalnaxmax) 95 69
STAT−3, women (kobiety) n= 28 n= 20 p= 0.042
mean value (wartość średnia) 28.3 18.2
standard deviation SD
(odchylenie standardowe) 18.4 13.5
median xmed
(mediana xmed) 27 17
minimum value xmin
(wartość minimalnaxmin) 0 2
maximum value xmax
(wartość maksymalnaxmax) 95 49
STAT−3, men (mężczyźni) n= 7 n= 10 p= 0.326
mean value (wartość średnia) 37.7 28.3
standard deviation SD
(odchylenie standardowe) 20.5 17.6
median xmed
(mediana xmed) 31 30
minimum value xmin
(wartość minimalnaxmin) 17 6
maximum value xmax
(Rp = –0.39, p< 0.05) and RBC (Rp= 0.36, p< 0.05) in RA patients were found (Figures 2–3). No correlation was seen between STAT−3 activity in white blood cells and the values of HAQ, DAS28, ESR, CRP, platelets, hemoglobin, hematocrit, and the number of swollen and painful joints.
Discussion
The first published studies regarding Jak/STAT activation in RA described constitutive STAT−3 DNA binding activity in mononuclear cells fresh− ly isolated from the synovial fluid (SF) of RA patients. These data suggested that soluble factors contained in the SF of patients with RA activated STAT−3 in control human monocytes [3, 4]. It is not completely clear which cytokines are involved in STAT−3 activation in RA synovitis. It is postulated that members of the IL−6 family (especially IL−6, a proinflammatory cytokine, but also IL−11, onco− statin M, and leukemia inhibitory factor (LIF)), IL− 10, IL−15, platelet−derived growth factor (PDGF), epidermal growth factor (EGF), and IFNα/β are involved in the process.
The present study showed that the activity of STAT−3 was higher in RA patients (significantly higher in women with RA) compared with a group of healthy individuals. It is interesting that STAT−3 activity was higher only in the subgroup of women, but not in men. This may be connected with the small number of men involved in the study (n = 7). On the other hand this may be relat− ed to an unknown pathological process that is associated with gender. The fact that RA occurs more often in women than in men is well known. An explanation for this fact was not found in any other study estimating STAT−3 activity. A more numerous group of patients is needed for reliable conclusions. No significant correlation was found in this group between STAT−3 and parameters of RA activity, except for WBC and RBC counts. This study is one of the few reports estimating the activity of STAT−3 in the peripheral blood leuko− cytes of patients with RA.
An experiment with a dominant−negative STAT−3 mutants provided evidence supporting the role of STAT−3 in the pathogenesis of arthritis [5]. It is postulated that the mechanism by which STAT−3 contributes to the pathogenesis is suppression of synovial fibroblast apoptosis [6]. Previous data confirmed the important role of STAT−3 in the sur− vival and expansion of synovial fibroblasts, which are needed to sustain the inflammatory process in RA. The data presented by Krause et al. indicated that ablation of STAT−3 function resulted in convert− ing EGF (epidermal growth factor) from a growth
Fig. 1.Comparison of STAT−3 activity between ana− lyzed groups
Ryc. 1. Porównanie aktywności STAT−3 między anali− zowanymi grupami
RA r.z.s. 14
16 18 20 22 24 26 28 30 32 34 36
38 Wynik testu t-Studenta:t= 1,994;p= 0,050 mean
œrednia
±1,96*b³¹d std ±b³¹d std
control kontrolna
group grupa STAT-3
Fig. 2. Correlation between STAT−3 activity and WBC
Ryc. 2.Zależność aktywności STAT−3 od liczby krwinek białych
WBC = 11,6 - 0,07 * STAT-3 Korelacja:r= -0,392
0 20 40 60 80
2 4 6 8 10 12 14 16 18 20 22
100 95% p. ufnoœci
STAT-3 WBC
Fig. 3. Correlation between STAT−3 activity and RBC
Ryc. 3.Zależność aktywności STAT−3 od liczby krwinek czerwonych
RBC = 3,92 + 0,0074 * STAT-3 Korelacja:r= +0,359
0 20 40 60 80 100
95% p.ufnoœci
3,0 3,2 3,4 3,6 3,8 4,0 4,2 4,4 4,6 4,8 5,0 RBC
factor for synoviocytes to a death factor [6]. This confirms the abnormal growth properties of syn− ovial fibroblasts in RA. The abnormal phenotype of synovial fibroblasts is characterized by increas− ed proliferative ability, resistance to apoptosis, and invasiveness of adjacent tissues. It is also noted that these cells exhibit cell−autonomous defects that contribute to the pathogenesis of RA [7]. There is some evidence that may confirm the participation of synovial fibroblasts in RA synovitis. RA fibrob− lasts are thus resistant to the induction of apoptosis and have a high proliferative potential. They pro− duce EGF and PDGF which, acting as autocrine factors, overexpress ErbB2/HER2, and accumulate mutations in the oncogenes p53 and ras. The hypothesis that dysregulated synoviocyte growth and survival in RA are dependent on STAT−3 is still being examined. Krause et al. suggested that STAT− 3 works by maintaining myc and pim−1 expression, increasing the expression of antiapoptotic Bcl fam− ily proteins, and by opposing proapoptotic signal delivered by, for example, EGF [6]. It also acts by suppressing Fas expression. STAT−3 also con− tributes to the pathogenesis of rheumatoid arthritis by promoting T−cell survival and antibody produc− tion [8].
Previous reports estimating the activity of STAT−3 in RA concentrated on synovial fluid cells and synovial tissue. Those data indicated exclu−
sive activation of STAT−3 (estimated by tyrosine phosphorylation) in RA patients, but not in osteoarthritis patients [5]. These results are similar to those of the present study, which compared RA patients to a healthy population. However, a dif− ferent method was used to estimate the activity of STAT−3 in peripheral blood leucocytes. Supporting data are provided by the fact that inhibiting STAT− 3 activity by its natural suppressor SOCS3 protein results in reducing the severity of antigen−induced arthritis in animal models [5].
Therefore, STAT−3 becomes an interesting therapeutic target for the future treatment of RA. Firstly, loss of STAT−3 function leads to an effec− tive induction of apoptosis of RA synoviocytes. Secondly, targeting STAT−3 converts endogenous− ly produced growth factors (EGF) into a proapop− totic signal eliminating pathogenic cells. There is little information about whether this is only a local process or is reflected in other cells. The present study confirms the hypothesis that RA is a sys− temic disease and that the local pathological process is reflected in the overall changes. However, no relationship with markers of disease activity was found except for correlation of red and white blood cell counts. This is a preliminary study and a more numerous group of RA patients is needed for statistically significant conclusions.
References
[1] Weynad C, Goronzy J, Takemura S, Kurtin P:Cell−Cell interaction in synovitis. Interactions between T cells and B cells in rheumatoid arthritis. Arthritis Res 2000, 2, 457–463.
[2] Ivashkiv L, Hu X: The JAK/STAT Pathway in Rheumatoid Arthritis: Pathogenic or Protective? Arthritis Rheum 2003, 48(8), 2092–2096.
[3] Sengupta T, Chen A, Zhong Z, Darnell J, Ivashkiv L:Activation of monocyte effector genes and STAT fami− ly transcription factors by inflammatory synovial fluid is independent of interferon gamma. J Exp Med 1995, 181, 1015–1025.
[4] Wang F, Segupta T, Zhong Z, Ivashkiv L: Regulation of the balance of cytokine production and the signal trans− ducer and activator of transcription (STAT) transcription factor activity by cytokines and inflammatory synovial fluid cells. J Rheumatol 2001, 28, 1952–1959.
[5] Shouda T, Yoshida T, Hanada T, Wakioka T, Oishi M, Miyoshi K: Induction of the cytokine signal regulator SOCS3/CIS3 as a therapeutic strategy for treating inflammatory arthritis. J Clin Invest 2001, 108, 1781–1788. [6] Krause A, Scaletta N, Ji J, Ivashkiv L: Rheumatoid arthritis synoviocyte survival is dependent on STAT−3.
J Immunol 2002, 169, 6610–6616.
[7] Firestein G, Zvaifler: How important are T cells in chronic rheumatoid synovitis. Arthritis Rheum 1990, 33, 1437. [8] Akira S:Roles of STAT−3 defined by tissue−specific gene targeting. Oncogene 2000, 19, 2607–2611.
Address for correspondence:
Marta Madej
Department of Rheumatology and Internal Diseases Silesian Piasts University ul. Borowska 213
50−556 Wrocław Poland
Tel. 0691510642
E−mail: [email protected]