Atherosclerosis Surrogate Marker in Diabetic Patients
Full text
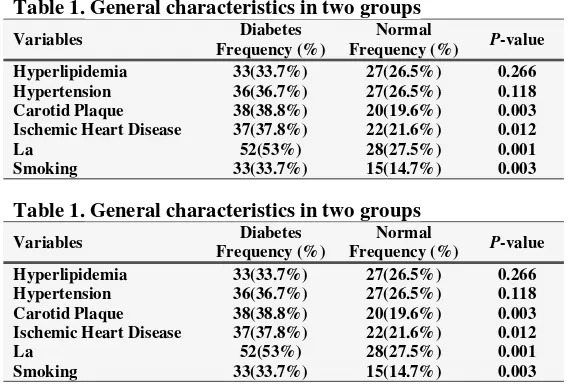
Figure
Related documents
The arrival of the Internet, and the World Wide Web suddenly made it possible for all three of these aspects - content delivery, communications, and learner management - to
Na psoríase foi detetado um aumento de IL-17 na pele dos doentes, assim como de IL-22, citocina também pro- duzida pelas células Th17 que, aparentemente, contribui para
The findings of this study could be summarized as follows: (i) the pattern of past dividends does significantly influence dividend decisions in Nigeria; (ii) the level
This study examines the relationship between CEO duality and the performance of Pakistani public listed companies by using a sample of five years, from 2007 to 2011.. This study
The present investigation examined the structural relations among: perceived organizational support; perceptions of organizational processes; workload; perceived
smoking of cigarettes (P 0.01). This implies a weakness in at least some of the adaptive strategies of cognitive regulation. In the same vein, according to the results of
Hyland's (2005) model of metadiscourse was adopted to analyse 30 transcriptions of Islamic Friday sermons delivered in the English language. The findings revealed that
CRF: Corticotrophin-releasing factor; CUMS: Chronic unpredictable mild stress; DALYs: Disability-adjusted life-years; GTT: Glucose tolerance test; HOMA-IR: Homeostasis model
![(E) N′ [2 (4 Chloro 3 nitrophenylsulfonyloxy) 3 methoxybenzylidene]isonicotinohydrazide acetic acid tetrasolvate](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)