Occupational Therapy Workforce Analysis
I. Introduction
The purpose of this project was to determine the current and projected occupational therapy workforce for the Winnipeg Regional Health Authority (WRHA) facilities in Winnipeg and in doing so to predict the likelihood of a balance between supply and demand in the future. In particular, it was deemed important to identify potential workforce deficiencies with the idea to mitigate such shortages.
Originally the intention was to review the available data and develop a document similar to the WRHA RN Required Supply Model document.1 Due to the numerous challenges unique to the Allied Health
Professions, it was determined that as well as determining future workforce, it was important to develop an understanding of the factors affecting supply and demand. These factors have been identified, to assist in formulating potential strategies to alter the future situation favorably.
The data required to make projections was not readily available and so a primary focus of the project became the development,
implementation, and maintenance of the appropriate tools for projecting and monitoring the workforce so that the process was repeatable, if desired, and could remain ongoing.
The overall aim of the project was to contribute to achieving and maintaining an optimal and stable Allied Health Workforce.
II. Methodology
The first task was to define the type of data required and to determine how best to utilize the data to provide a projection of workforce.
Secondly it was determined that, as the prediction of workforce
balance will be based on a relatively small sample size it was important to further clarify the issues affecting workforce supply and demand.
The findings and observations noted in this discussion paper are based on a review of the current literature and related reports as well as interviews with a variety of sources. The literature that had been used in formulating the RN Required Supply Model was reviewed.1-7 Medline was searched using workforce and the discipline, in this case occupational therapy, health human resources, health manpower, and human resource planning.Information was obtained from the licensing organization, The Association of Occupational Therapists of Manitoba (AOTM), the professional organization, The Canadian Association of Occupational Therapists (CAOT), and the educational institution, University of Manitoba, School of Medical Rehabilitation (U of M, SMR). The information reported by the licensing organization is self reported data. Reports formulated by other interest groups were reviewed and key points identified.
The position vacancy data was obtained through the WRHA's collection system and clarified by the occupational therapy
management representatives. The most recent sample was used in the analysis as the data has only been collected on a quarterly basis for approximately a year and a half and inaccuracies existed in the
previously collected data. Information regarding retirement, ages, and years of service was obtained through the payroll systems (Ceridian, Health Sciences Centre, and St. Boniface General Hospital), as the
HEPP database was not usable due to varied union affiliations and a lack of common labour codes among the occupational therapy
employees.
Information regarding the number of occupational therapy graduates was obtained from the University of Manitoba (U of M), School of Medical Rehabilitation.
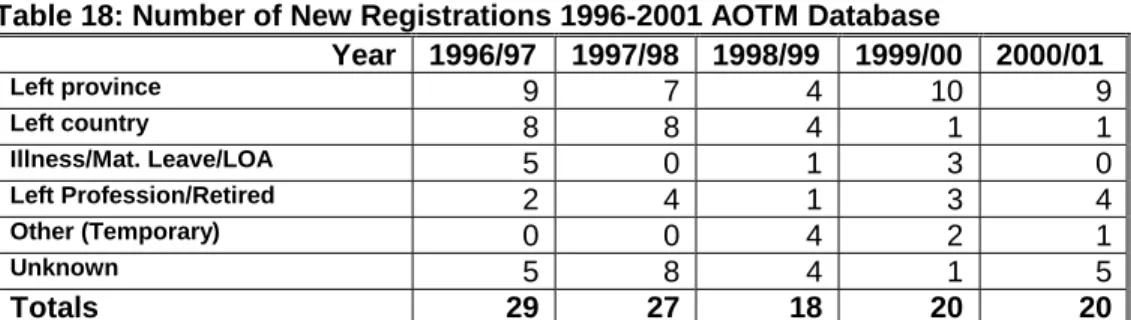
Demographic information and data regarding the employment patterns of therapists for the past five years was obtained from the Association of Occupational Therapists of Manitoba (AOTM).
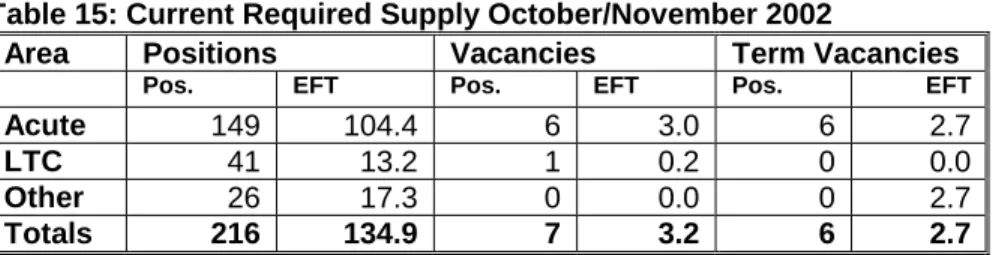
The data collected was reviewed to determine whether there would be an appropriate supply of occupational therapists in the future. The information reviewed included the number of graduates. Supply included numbers of graduates retained and new registrants, the current workforce required was obtained through the position/vacancy data collection and the payroll system, and attrition numbers were based on data from the licensing body and retirement information, using the Magic 80 and age ranges. The number of occupational therapists working within the WRHA amounts to approximately 216 positions. Considering these low numbers, caution must be used when interpreting the data.
For the purposes of this project the need or requirement side of the equation was based on the current requirement of the Winnipeg region, that is, the number of occupational therapists currently
employed by the WRHA at this time. The requirements are based on the current level of service delivery and future needs or variations to these needs have not been considered.
The identification of trends and issues affecting the occupational therapy workforce as well as factors affecting work life, recruitment, and retention have been outlined.
Recommendations, gleaned from the review of numerous sources, have been included for consideration.
III. Profession Description
In the Winnipeg Regional Health Authority Profile document, occupational therapy is described as a "health profession whose members collaborate with clients in enabling occupation." 8
As described by the United States Department of Labor, "occupational therapists (OTs) help people improve their ability to perform tasks in their daily living and working environments. They work with individuals who have conditions that are mentally, physically, developmentally, or emotionally disabling." 9
Occupational therapists work in a variety of settings including
hospitals, rehabilitation centres, private practices, psychiatric settings, extended care facilities, schools, community health organizations, work sites, industry, government, and client's homes. Therapists work in both acute and chronic care settings. A primary role for occupational therapy is that of an educator in all areas of practice. Occupational therapists working in acute care generally provide service between 7:30 and 16:30 seven days a week with discharge planning services being provided on weekends. 10 Although the level of self-employment has increased significantly over the last ten years it still remains
relatively low at 12% compared to an average of 17% for all occupations. 11
Human Resources Development Canada describes occupational therapists as requiring an undergraduate or graduate degree from an accredited program, which must include a period of practical
supervised training. 11 Occupational therapists require registration in all jurisdictions in Canada.
A fairly high proportion of occupational therapists work at more than one location as depicted in Table 1 and 2.
Table 1: Location of Principal Employment on April 112 AOTM
1999 2000 2001 1st 2nd 1st 2nd 1st 2nd
Hospital 93 7 103 8 105 10 Psych Facility 27 3 28 1 28 2 Rehab Hospital 37 2 36 1 40 3 Long Term Hospital 19 0 17 5 17 4 Private Practice Clinic 17 11 20 11 25 8 School System 20 5 23 12 23 7 Industry 3 1 4 0 4 0 Government 4 1 4 1 4 0 Ext. Care 12 10 10 8 19 12 Community 58 19 65 16 65 18 University 8 7 9 6 9 12 Other 7 1 7 1 10 5 No Response 9 0 9 2 14 3 Total 314 67 335 72 363 84 Note: 2nd position contains working statistics for secondary plus tertiary positions.
Table 2:Percentage of Occupational Therapists Working in 2 or More Locations – April 1st12
1999 2000 2001
21.3% 21.5% 23.1%
The CIHI data indicated a marked increase in the number of
occupational therapists practicing in Canada for1988 to 1997. 13 The overall growth rate was 127.5% over that period. In part, this increase was as a result of changes to the regulatory requirements in a number of provinces. The population per active occupational therapist has decreased over the timeframe of 1988-1997. In Manitoba in 1988 there were 4,667 people per occupational therapist compared to 4,015 in 1997. Manitoba demonstrated the least change in population per therapist for this time frame. For Canada as a whole the population per active occupational therapist decreased from 8,140 in 1988 to 3,900 in 1997.
Human Resources Development Canada (HRDC) noted that from 1988 to 1993 the profession grew 53.1% and from 1993-1998 it grew
an additional 46.7%.11 The number of workers reporting part-time employment is 28% compared to an average of 19% for other occupations. 11 In the USA 30% of occupational therapists report working part-time. 9 Based on the payroll information, within the WRHA, the percentage of therapists working part-time is 42.6%.
Table 3: Work Status WRHA
CGH GGH HSC SBGH SOGH VGH DLC MHC RVHC Totals %
FT 5 5 36 19 6 2 6 0 4 83 40.7
PT 6 6 40 14 6 4 1 5 5 87 42.6
Casual 2 5 12 4 3 6 0 2 0 34 16.7
Total 13 16 88 37 15 12 7 7 9 204 100
The profession remains predominately female (see Table 4). 12 At a national level, 92% of occupational therapists are female compared to only 45% for other occupations. 11 Increased maternity benefits and family responsibilities may have workforce implications for this group. The high percentage of part-time workers is likely as a result of the male /female distribution.
Table 4: Male/Female Distribution of Working Occupational Therapists Apr. 112 1999 2000 2001
# % # % # % Female 289 92.0 307 91.6 329 90.6
Male 25 8.0 28 8.4 34 9.4
Total 314 335 363
Occupational therapists have one of the lowest unemployment rates for professional occupations and for occupations in the healthcare sector with the national rate averaging 1.4% from 1996 to 1998, compared to the national average of 6.0% for all occupations. 11 The U.S. Department of Labor predicts that employment of occupational therapists will increase faster than average through 2010.9
HRDC states that the average earnings for occupational therapy are among the lowest for professional occupations but are comparable to other occupations in the healthcare sector. 11
IV.
Literature Review
A number of reports describing the occupational therapy workforce experience have been generated in recent years and key points from these reports and articles are provided.
i. Profile of the Allied Health Workforce
(Winnipeg Hospital Authority - September 1999,Update June 2001)
The Winnipeg Hospital Authority prepared this report in September of 1999 8 and an update to this report was completed in June 2001.10 It was designed to provide a comprehensive overview of each allied health profession employed in the Winnipeg hospital system. The report identified a number of important issues common to the allied health professions such as wage rates, recruitment and retention issues, scope of practice concerns, student education and enrollment, program management, seven-day week coverage, relief budgets, and workload measurement standards.
The information describing the professional role of the occupational therapist has been utilized in the previous section on professional description.
The document noted that therapists are required to be licensed to practice in the province.
An important role identified for occupational therapists is the development and dissemination of patient education information. Therapists actively participate in the supervision and education of occupational therapy students by providing direct clinical teaching as well as supervision of students in the clinical setting.
The importance of participating in research is noted as a means of improving practice standards although at present there are no
occupational therapists with research grants and so time is "borrowed" from clinical practice. 10
Relief budgets are limited or non-existent for this group. Since the inception of WRHA any new programs are provided with a relief budget but existing programs do not have this benefit. Although efforts to create a pool of casual workers has been attempted it has met with limited success as the numbers available are unable to keep up with the demand for service and so unscheduled absences are not able to be covered. Also, there is not dedicated personnel or systems to support the management of a relief pool of workers.
Issues identified as affecting the ability of the WRHA to recruit and retain staff include:
• Salaries - the report identified that therapists in Manitoba are the 7th lowest paid in the country and staff in professional leader positions are not adequately compensated.
• Benefit packages do not necessarily meet the needs of the workers.
• Opportunities for career laddering, although they exist, are difficult to attain as therapists have little opportunities to develop the skills required for the job.
• Work environments need to be structured to provide therapists with flexible schedules, varied work opportunities, collegial support, and continuing education opportunities.
• Environmental issues such as providing access to appropriate technology such as cell phones and computers to enable therapists to provide better service.
Concern was expressed regarding the ability of the hospital staff to provide clinical placements for students. The ability to provide these placements is based on vacancies, staff turnover, and term versus permanent positions. Already difficulty is encountered when trying to provide student placements and it is anticipated that with the increased enrollment the situation will become even more difficult.
Recommendations provided in the report to improve the situation for occupational therapists within the WRHA included:
• Increase funding for clinical equipment, office and assistive technology, and staffing in an effort to improve the working environment.
• Provide equipment such as computers to enable therapists to better function in the community.
• Complete a review of the current organizational structure keeping in mind that occupational therapists prefer to be
supervised by their own discipline and that practice is improved by a more functional department organizational structure.
• Allocate appropriate resources to enable occupational therapists to participate at an appropriate level in non-patient care
activities related to program management. At this time additional resources have not be provided to meet this demand.
• Review salaries and increase them appropriately to improve staff retention.
• Provide additional support for continuing education activities.
ii. Canadian Association of Occupational Therapists (CAOT) Confirms Occupational Therapy Shortage in Canada
(CAOT August 2002)
The CAOT conducted a survey of all occupational therapy university programs and regulatory bodies in an effort to collect data regarding education, supply, and distribution of occupational therapists.14
This data was combined with that from the Canadian Institute for Health Information, Statistics Canada, and the CAOT membership database and key points were identified.
Key Points
• The supply of occupational therapists (OTs) must significantly increase across Canada to meet existing demands. From 1991-2000 the number of active OTs increased 62% across Canada and in Manitoba the increase was 88%. The ratio of OTs per 100,000-population increased from 25.5 in 1996 to 30.9 in 2000. Manitoba had the highest ratio at 36.8/100,000. The report noted that the province of Manitoba continues to report shortages of OTs despite this high ratio. As a result of these reported shortages a 66% increase in seats at the University of Manitoba has been approved by the government.
• Shifts to new areas of practice for OTs has increased the demand for services, as has the high rate of attrition for OTs after the first year of practice and after 45 years of age. Self-employment for this group rose from 11% in 1995 to 23.1% in 2000.
• Despite an increase in OT graduates over the past ten years the demand for OTs remains great. Between 1995 and 1999 master's level members increased from 7.7% to 10.9% and doctorate level members from 0.03% to 1.7%.
• Applicants to OT education programs have decreased in the last six years possibly as a result of changing demographics of university age groups, the move to a masters level entry at some programs, and the decrease in attractiveness of health professions based on working conditions and low salaries.
CAOT proposes to assist its members by assisting with further analysis of problem, working in collaboration with regions to identify supply requirements, working with education programs to increase enrollment, assisting employers with the development of recruitment and retention strategies, and preparing a position statement
iii. Access to Occupational Therapy - Position Statement
(Canadian Association of Occupational Therapists 2001)
The Canadian Association of Occupational Therapists (CAOT)
released a position statement in May of 2002 expressing concern "that the health and well-being of Canadians is adversely affected due to the lack of equal access to quality occupational therapy services."15
It is recommended in the document that:
• Occupational therapy be recognized as an essential and necessary health service.
• Adequate funding, resources, and support be provided to ensure that professional standards and a high quality of occupational therapy are maintained.
• Enrollment in occupational therapy programs and the use of foreign trained graduates be increased to alleviate the shortages of occupational therapists.
• Strategies be implemented to recruit occupational therapists to under-serviced areas.
CAOT will assist in ensuring access to quality occupational therapy services by advocating for participation of occupational therapists in a variety of sectors, marketing occupational therapy to appropriate groups, working with provincial occupational therapy groups to determine the supply equipments, working with the educational institutions, developing and promoting standards of education and practice, and providing professional education and practice resources.
Therapists cite high caseloads and workloads as the most important factors affecting job satisfaction. The report makes note that to match the current level of service 1,800 new and active occupational
therapists are required. Increased enrollment is needed to meet service demands.
iv. 1999-2001 Job Choice Survey Summary Report
(University of Manitoba School of Medical Rehabilitation 2001)
This survey was compiled in August 2001.16 University of Manitoba physiotherapy and occupational therapy graduates were surveyed in the spring of their graduation year to identify factors that might
influence job choice and work life. The overall response rate was 61% with a 72.2% response from occupational therapy students and 48.9% for physiotherapy.
Key Points
• 68% of occupational therapy graduates planned to practice in Manitoba after graduation.
• Common factors identified in determining place of employment after graduation from occupational therapy were; family, working conditions, friends, opportunity for full-time employment, and job or commitments of spouse/partner.
• Preferred age group of patients was adolescents, seniors, and children.
• Preferences for practice areas were rehabilitation centre, community agency or general hospital, consulting, and public school system.
• Only 39% indicated that they intended to practice full-time for their entire career. The intentions expressed were 32.5% would move to part-time after one-five years and 25.0% intended to work for 6 -10 years before moving to part-time.
• 95.2% stated that a competitive salary or a higher salary would keep them working in the province.
• 100% of those surveyed wanted salaries competitive with other provinces.
v. Winnipeg Regional Health Authority - Occupational Therapy Leadership Group Issues Management
(October 2001)
This paper was prepared by the WRHA Occupational Therapy Leadership Management Group as part of an Issues Management Exercise.17 Information from this document has been summarized and key points identified.
1. Caseload Guidelines
Need to develop caseload guidelines by accessing current research information, identifying current practices in the province, defining patient population groupings, designing and conducting a pilot study, comparing to other sites, analyzing data and making recommendations, and disseminating the information. 2. Clinical Practice Guidelines
Need to ensure that occupational therapy is represented on care map author teams and that representation is current, evidence based, and consensual from all facilities.
3. WMS and Data Management
Review systems used, determine inconsistencies, determine current usage, and clarify relationship between WMS data, standards of performance, and caseload guidelines. 4. Documentation Guidelines
Need to develop standards across WRHA facilities. 5. Human Resources/Workforce Planning
Identify current workforce demographics including attrition rates and define workforce issues.
6. Continuing Professional Education
Ensure common understanding of continuing professional education.
Develop systems to improve awareness and access to continuing education.
7. Clinical Education of Students
Increased enrollment at U of M will result in increased placements. Difficult to accommodate student placements due to increased workloads and increased number of part-time and casual staff. Need to provide support and recognition to clinicians supervising students.
8. Research
The level of interest, skills, knowledge, and opportunity in regards to research is inconsistent across the region.
vi. Review of Relevant Literature
A review of the current literature identified a number of articles dealing with recruitment and retention issues for occupational therapists. The following summarizes the most applicable articles.
Jones, Johnson, Beasley, and Johnson (1996) identified that there are significant and increasing shortages of allied health professionals that are likely to increase as the population ages.18 Previously in 1991 Elwood identified a shortage of occupational therapists in 44% of the United States. 19 In the Jones, Johnson, Beasley, and Johnson study, conducted in South Carolina, strategies used in the past to at least temporarily relieve staff shortages included "the provision of good salaries, flexible work schedules, child care, and other incentives." The strategy of using less skilled staff had been explored but this approach was controversial. The difficulty with many of these strategies, when used in isolation, was that facilities worked against facilities in an attempt to reduce staff shortages. The information obtained through the use of focus groups determined that inadequate educational resources, low salaries, insufficient continuing education and tuition assistance, and a lack of clinical placements all contributed to the shortages. The number of graduates was identified as being
inadequate to meet the needs. A coordinated approach was advocated with educational groups and healthcare facilities working together to alleviate the shortages.
A survey was conducted in British Columbia to determine the current and future manpower requirements for the province. 20,21 Resignations for the year 1981 were high at 31.6% suggesting that younger
occupational therapists were changing jobs as more interesting or higher paid positions became available. Regardless of the reason for the turnover the impact created difficulties with staff stability, long term
planning, high recruitment costs, and difficulty with supervising
students. The assessment of needs demonstrated that there would be a need to increase OTs by 187% to 245% over the period from 1976 to 1986 depending on the group surveyed. The primary solution proposed to deal with the manpower shortage was to increase enrollment at the University of British Columbia. The difficulty with this solution was that there were not enough qualified educators to accommodate a
substantial increase. The possibility of introducing refresher courses to facilitate the re-entry to practice was also proposed. The importance of gathering and analyzing this type of data was stressed to enable long term planning.
Salvatori, Williams, Polatajko, and MacKinnon (1992) reviewed the occupational therapy manpower shortage in Ontario and identified factors affecting retention and attrition as well as determining
strategies to improve the situation. 22 The shortage was predicted to continue despite an increase to enrollment and the implementation of strategies to improve retention and decrease attrition was
recommended. The strategies included among others;the sponsorship of re-entry candidates and new graduates for return of service, the provision of promotional opportunities and career path alternatives, increasing job autonomy, increasing participation in management and decision-making, providing flexible work hours, improving salaries and benefits, the development of excellence in leadership and
management, providing rewards, recognizing work contributions, offering a variety of work challenges, increasing the appropriate use of support personnel, and the provision of opportunities and funding for continuing education.
In a later study, Solomon, Salvatori, and Berry surveyed therapists working in Northwestern Ontario in an attempt to determine factors
associated with recruitment and retention. 23 Although this study only dealt with rural therapists, factors affecting job satisfaction were
reported as well. It was determined that personal factors that were not related to the job were the most influential in deciding location of employment. Job factors that had a positive effect on remaining in the job included the ability to be independent, hours of work, and type of caseload. The provision of opportunities for continuing education was important in decreasing feelings of professional isolation.
Wilkins and Rosenthal (2001) surveyed forty occupational therapists in an attempt to determine the factors influencing the therapist's decision to work with the elderly and children. 24 Although this study limited its focus to therapists working in geriatrics and pediatrics the findings may apply to other areas of practice. Factors positively influencing the decision to work in a particular field included availability of work, positive exposure to the area as a student, opportunities to work part-time, and opportunities for promotion and continuing education. Additional job characteristics associated with work selection were the level of autonomy, proximity to home, flexibility, and the recognition by other team members. Most therapists surveyed identified the lack of promotional opportunities and financial rewards as obstacles in
regards to work. The point was made that the provision of opportunities for flexible working conditions may encourage women with children to continue work while managing their personal lives.
Smith, Schiller, Grant, and Sachs designed and delivered a survey aimed at identifying recruitment and retention strategies as well as measuring the effectiveness of the strategies. 25 It was identified that the top three recruitment strategies were referrals from existing staff members, professional development opportunities, and advertisements in newspapers. The top retention strategies included "interpersonal
staff member relationships, employee appraisals, and continuing education." Recruitment and retention of staff was identified as critical to the delivery of high quality service. Commonly used recruitment strategies, in addition to those noted above, included program development, competitive salaries, opportunities for supervising
students, flexible scheduling, and the contacting of previous applicants. Long-term care facilities did not utilize the strategies to the same
extent as acute and rehabilitation facilities. The provision of flexible scheduling and job fairs was most effective in long-term care and least effective in the rehabilitation and acute care facilities. The most
commonly used retention strategies included the development of positive interpersonal staff relationships, employee appraisals, continuing education, the provision of supervision and feedback, a supportive environment, and employee recognition. The directors surveyed identified that the provision of on site daycare may be an effective recruitment strategy but noted that it had not been commonly used. The work itself and the salary were identified by directors is the most effective recruitment tools. Effective retention strategies were noted to be often the same as job satisfaction strategies and included recognition, opportunities for professional growth, positive working relationships, flexible work schedules, and competitive salaries. Directors were advised to incorporate the most effective recruitment strategies into their job advertisements and to utilize effective retention strategies to improve job satisfaction and retain employees.
Okerlund, Jackson, Parsons, and Comsa (1994) conducted a study to examine the factors affecting the shortage of occupational therapists in Utah. 26 Although based in the Unites States the factors identified may have relevance in Canada. Relevant points from this study included the fact that 23% of respondents indicated that they were hired for their first job by the institution at which they had completed their internship
or training. Factors identified as being advisable to include in a
recruitment program included salary and benefits, access to continuing education, flexible working schedules, positive treatment by coworkers, opportunity to participate in decisions, and job freedom. These are listed in order of importance. Similar factors were identified for job satisfaction and job retention. Recruitment and retention strategies identified included; having a school in the state, directing efforts to encouraging students to pursue the career, providing student placements, assisting with education costs, and ensuring job satisfaction.
Rozier, Gilkeson,and Hamiltion (1992) surveyed occupational therapy students to determine their career expectations. 27 The reasons why students entered into the profession are likely tied in closely with factors that influence recruitment and retention. Previous studies had indicated that salaries were not of great importance but in this survey students indicated that good salaries were desirable. Other factors identified by students as favourably influencing their decision to pursue an occupational therapy career included; the ability to help others, job availability, job prestige, and previous experience working in an
occupational therapy setting.
An earlier study conducted by Freda (1991) also identified factors considered by therapists when deciding to leave or remain in a job. 28 The importance of retaining therapists was stressed as the effect of turnover can be very high in terms of financial costs, which are estimated to be anywhere from $2500 to $25,000, and the negative effect that high turnover has on other staff. The study identified that the factors affecting retention varied somewhat depending on years of experience. This point is important, as managers may need to focus retention efforts in different areas depending on the experience of the
therapist. Extensive paperwork was identified as a major stressor for occupational therapists and patient care was generally identified as the most rewarding aspect of the job particularly for less experienced therapists. With experience, therapists began to identify program development as important. Management responsibilities were not seen as a rewarding aspect of the job until the 7-10 year range of
experience. This has ramifications for professional development as needs differ with years of experience. Therapists across all ranges of experience viewed increased salaries and promotional experience as being rewarding. The need to adapt retention strategies as therapists progress through their careers is an important aspect of staff retention.
Bailey (1990) conducted a study examining the reasons why occupational therapists left the profession. 29,30 The reason for
conducting the study was to assist in determining ways to prevent this attrition and this topic is discussed in a subsequent article. Bailey identified that attrition was a major issue in regards to workforce and noted that retention is critical. The primary reasons for leaving the profession included those related to child rearing and maternity, relocation, inadequate salary, lack of opportunities for promotion, workloads, stress, dissatisfaction with the work itself, dissatisfaction with the bureaucracy, and the inability to work part-time. It was found that almost four times as many single, compared to married therapists, changed professions because their salaries were too low. As the largest number of therapists left to be at home with their children, Bailey proposed that working conditions must be made more amenable to working mothers. Possible strategies included job share positions, flexible hours, and flexible benefit packages. Staff that work in job share positions had a high probability of returning to work full-time at a later date which provided the added benefit of not having to recruit or train new employees down the road. The provision of on-site daycare
may also assist in the retention of working mothers. The need to ease re-entry into the profession is important as many therapists do take time off for child rearing and then do not feel able to return to the profession. The provision of re-entry to practice programs was deemed important to alleviate this situation. Lack of opportunities for
advancement was noted to be an important factor in the attrition of therapists. To achieve advancement therapists frequently had to leave behind the title of occupational therapist for more generic titles and the number of positions available was sparse. A high number of therapists surveyed (30%) left to pursue training in fields other than occupational therapy. The lack of graduate programs in occupational therapy
frequently led therapists to pursue further education in another field such as special education. High caseloads leading to stress and burnout were also a reason for leaving the profession. Other reasons for leaving included disillusionment with the profession, frustration with bureaucracy, types of caseload, not being able to work to their full ability, conflict with supervisors, illness including occupational back strain, desire for greater autonomy, and lack of continuing education opportunities. By addressing these issues, attrition of occupational therapists may be decreased.
Occupational therapists were surveyed in regards to job satisfaction by Madill, Macnab, Brintnell, Stewin, and Fitzimmons in 1987. 31
Therapists in the low extrinsic group were identified as seeking advancement, autonomy, prestige, and appropriate economic return. This group generally consisted of front line clinicians. Highly satisfied workers on both intrinsic and extrinsic measures tended to be
therapists in administrative or management positions where they could likely have greater control, authority and status within their work
environment. It was identified that management personnel may not be providing the most effective style of management and may actually be
contributing to problems associated with underutilization of skills and staff turnover. Clinicians do not need a high level of supervision but rather a demonstrated excellence in negotiation at the administrative level. Staff therapists are capable of providing solutions to unit
management issues and their expertise in these areas should be acknowledged. It is suggested that the Canadian Association of Occupational Therapists develop and deliver an education program designed to improve management skills of occupational therapists, include program evaluation and management courses in graduate occupational therapy programs, and offer a workshop dealing with department management at the annual CAOT conference.
Occupational therapists have been moving into private practice at a greater rate. The reasons for this exodus from the public sector are described in an article by McClain, McKinney, and Ralston (1992). 32 The authors surveyed a group of occupational therapists working in private practice and asked them about their motivation to change jobs as well as factors relating to preparation and perceived risks and benefits. The primary reasons for making a move onto private enterprise included the ability to establish their own pay schedules, flexible working hours, the ability to use their own creativity and
imagination and to make independent clinical decisions, the desire for autonomy, opportunity to specialize, more control over the quality of their work, and the potential for higher salaries. An understanding of these factors is useful in developing strategies for retention.
There are not a large number of therapists in private practice in Manitoba at the present time but this form of practice is gradually increasing, particularly in the areas of pediatrics and occupational medicine. Bridle and Hawkes (1990) provided an overview of private practice and occupational therapy in response to a group of therapists
who were interested in private practice and wanted a better
understanding of the nature of the business. 33 A survey was sent to therapists in private practice. The average length of employment prior to embarking in a private endeavor was slightly more than six years. The most common reasons identified for moving to private practice were the desire for autonomy (54%), limitations of institution based practice (49%), potential for higher income (22%), lack of job
opportunities (11%), and the "other" category which included flexible scheduling, specialized practice, etc. About one third of respondents worked full-time with the remainder working part-time. The study revealed great diversity among those surveyed but the information regarding the reasons for moving to private practice has relevance to staff retention.
As identified in the Profile document there is a need to provide occupational therapists with the skills to successfully achieve higher-level positions.8, 10 Chilton (1990) further described this issue. 34 A survey was completed by 116 supervisors and it was determined that 40% did not have a quality assurance plan and 53% had not
completed management courses prior to assuming their current management position. It was identified that the profession must be proactive in the development of management personnel. Aspiring managers were encouraged to make the shift from having the client as their first priority to developing a better understanding of management issues. Therapists, who provide student supervision, need to develop management level skills to enable them to provide this service and continuing education programs should address this need. Therapists in management positions are advised to develop a network of support within their profession. The development of excellence in management is also cited as an important factor in regards to retention as a skillful manager will be better able to meet the needs of staff. Overall the
author appealed to the profession to enhance career development opportunities to maintain therapists with the potential to spearhead the profession. Occupational therapy managers must demonstrate the required blend of excellence in clinical practice and strong
management skills to assist in shaping practice. Recommendations included the inclusion of continuing education opportunities at a national level to develop management skills, the provision of appropriate courses at the graduate level, and the inclusion of a workshop/institute at the annual conferences.
In an attempt to retain skilled therapy staff a hospital in Ontario, a "clinical ladder" was instituted to decrease turnover and attrition. 35 The problems associated with attrition of occupational therapists were reviewed. It was noted that the estimated national annual turnover rate was 32.6%. The cost of recruiting and retraining a new staff member is estimated to be as high as 50% of the new employee's annual salary. Staff shortages have a negative effect on the employer, other staff, patients, and the profession in general. Shortages of occupational therapists have resulted in other professions encroaching on their scope of practice. Lack of opportunity for advancement, the need for greater autonomy, and the lack of recognition of clinical skills have all been identified as contributing to job dissatisfaction. Opportunities for occupational therapists who enjoy patient contact fall into three
categories; remain a staff therapist and expect no further advancement in salary or recognition after five or six years, relocate to a new facility in an attempt to add variety to the job, or move into an administrative area leaving patient care behind. The creation of a clinical ladder was an attempt to provide an alternative career opportunity. Attainment of advancement was well defined and only those deserving of recognition were promoted. The promotion was difficult enough that staff perceived a change in status with the promotion. Only those making a significant
contribution to the organization were promoted. The number of positions available was not limited to ensure that all staff were motivated to achieve clinically. Although the implementation of this plan has not been conclusively proven to be an effective retention tool, the results have been positive.
Selby Smith and Crowley36 reviewed issues surrounding labour force planning for Allied Health in Australia. The need to refine the tools of analysis and to continue to identify factors affecting supply and demand was identified. The high proportion of women in allied health professions was noted, which was associated with greater demands in regards to child rearing and responsibilities in the home.
Abelson identified the need to determine why staff leave and whether or not the departure was avoidable or unavoidable, desirable or
undesirable.37 Factors that positively affect turnover such as ambiguity, conflict, and job tension were described. Individual factors that reduce turnover were age and tenure as well as employees having greater family responsibility. Factors that were inversely related to turnover included organizational and professional commitment and positive leader behavior. Identifying units with high turnover and planning for future needs may assist in decreasing turnover. Other managerial strategies included decreasing job pressures, implementing career development programs, providing more job autonomy and
responsibility as desired by staff, and having appropriate levels of flexibility and rigidity. In regards to salary, Abelson determined that the amount has the most influence at the entry level and decreased after that. Employees who were satisfied with most other important factors were not inclined to leave an organization, even if the pay was a little less than that at other locations.
A review paper completed by Mobley (1979) summarized a number of studies examining employee turnover.38 The negative relationship between turnover and tenure, job satisfaction, and satisfaction with supervision was described. Higher salaries were noted to generally result in higher tenure and in situations where salaries were high, if there was a perceived difference between the expected and the actual salary, tenure was shorter. The perception of status within the
organization, generally demonstrated by knowledge of the
organizational procedures and a perception of control, were associated with longer tenure. It was also noted that the availability of alternative jobs was positively associated with turnover.
The National Health Service (NHS) had been experiencing difficulties with staff recruitment and retention and health service employers identified the need to improve performance in this area. With this in mind, Gray and Phillips looked to businesses in other sectors of the economy to determine if recruitment and retention techniques used there could be applied to healthcare. 39 The companies reviewed were chosen based on their importance in the economy, their varied staffing requirements, and their high percentage of female employees. The companies included Midland Bank, a supermarket chain, and British Rail.
Salaries are frequently cited as a major consideration in regards to recruitment and retention and yet there is evidence that indicates that other factors may play a major role as well. One survey of nurses who had left the NHS indicated that staffing levels were more influential than pay in their decision to leave. In regards to recruitment, nurses not currently employed claimed that the availability of part-time
positions and assistance with childcare arrangements was more important than salary in determining their return to work.
Changing pay levels was identified as one method of altering recruitment and retention and was being used by other companies. The NHS has a central system whereby a review group sets salary rates. Salaries may vary based on location and difficult to fill positions have been supplemented, but otherwise managers have had little ability to alter salaries. The NHS has now given local managers more discretion in setting salaries.
As well as allowing salary adjustments, the three companies surveyed instituted policies to improve recruitment, which included; targeting recruitment, reducing organization restriction on recruitment, improving community links, increasing part-time positions, introducing new
technologies and work-practices to decrease the need to recruit, implementing training for new staff, and improving information systems. Companies improved community links by liaison with the education sectors, providing job experiences, and supporting school projects.
The three companies surveyed identified the part-time work force as the major target of their efforts. Midland Bank began heavily promoting part-time employment and ensured that part-time contracts were brought in line with full-time contracts in terms of benefits and the provision of regular work hours. Job sharing opportunities were supported whenever possible. The ability to provide time off over the summer months was supported by replacing workers with student workers over the summer when possible.
The implementation of recruitment strategies necessitated improved information systems to enable the tracking of the effect of the
strategies, staff recruitment efforts, employees' career development, and the number of staff leaving as well as the reasons why they leave. British Rail implemented the use of a system that was able to monitor who applied for positions, the background of the applicant, the number interviewed, the number offered positions, and the number of jobs accepted.
The supermarket chain had implemented a "Career Bridge Scheme" which allowed staff to take temporary breaks in employment to pursue other activities. The break could be up to three years with an option of part-time employment for the subsequent two years. Midland Bank offered a similar plan for employees who had been with the company for at least two years. These employees were able to take a hiatus from work for up to five years without experiencing a loss of benefits. During the break time the employees were required to work at least two weeks each year and attend refresher meetings. The strategy of allowing career breaks may result in increased turnover but in the long run may result in an improved supply of workers over the long term.
As many workers within the businesses surveyed were women, the provision of childcare was considered an important tool in keeping women at work. Midland Bank estimated that the cost of replacing an employee was equal to one year of salary and was about twice the cost of subsidizing childcare for four years. The Bank implemented a cost-sharing scheme with workers in the late 1980's. Employees' returning to work had risen from 30% in 1989 to 50% by late 1991.
Other strategies aimed at improving retention of staff included providing career counselling, providing additional education for
managers, providing staff support during the initial months of
employment, and the hiring of occupational health nurses to address health-related concerns of employees.
Improved information systems were felt to be essential. Both the Bank and British Rail routinely conduct exit interviews in order to better understand the reasons for staff leaving employment.
The evaluation of recruitment and retention strategies was encouraged to ensure cost effectiveness.
V.
Other Factors Affecting Recruitment and Retention
Discussion took place with the Occupational Therapy Leadership Group, the Winnipeg Regional Health Authority (WRHA) Occupational Therapy Professional Leader, the Association of Occupational
Therapists of Manitoba, and other WRHA occupational therapy managers.
Professional Issues
Vacant positions have been filled by other disciplines in some cases so although the vacancy is no longer a problem there still exists an issue in regards to professional suitability and the fact that the position is still vacant to occupational therapy. This occurred recently with a position at Seven Oaks General Hospital.
Continuing Education
Concerns expressed included that funding and opportunities for educational purposes were not consistent throughout the region. Coverage for staff attending courses is not generally available as part of a relief budget. As availability of continuing education has been identified as a critical factor affecting recruitment and retention it was suggested that provisions be made for leave to attend courses, financial support for attending courses, relief budgets to provide replacement staff, and funding to support a continuing education
coordinator. The need for a regional continuing education program and a regional library service has been identified.
Program Management
There was concern expressed regarding the inconsistent manner in which the program management model has been implemented across the region. At certain facilities the professional leaders may be required
to carry a full caseload while at other facilities the position may more closely resemble a management position. The perceived lack of career advancement opportunities as a result of the disabling of occupational therapy departments was of concern. There was concern that the ability to participate on professional committees was compromised and peer contact was less under the program management scenario. This was perceived as undesirable, as mentorship and collegial support were diminished. The additional remuneration paid for professional leader positions was felt to be inadequate considering the
responsibilities of the positions.
Relief Budgets
Vacancy data was not felt to accurately reflect the true staffing situation as many facilities have little or no relief budget to cover
absences. Long-term employees have accrued extended vacation time and sick benefits. Coverage for these absences is generally not
available and this results in decreased coverage and increased workloads for other staff. Overtime is generally recorded and taken back as time, not in salary, again resulting in a decrease in coverage. Any new programs that are implemented do have relief budgets associated with them, but a gap exists at present. The need to have adequate and equitable relief budgets as well as a WRHA float pool of therapists available for relief work was identified.
Table 5: Occupational Therapy Relief Budgets (as reported by facilities)
CGH GGH HSC SBGH SOGH VGH DLC MHC RVC RCC
EFT 0.875 0.0 .46 0.8 .4 0.0 .05 0.0 Note : At SOGH relief is provided for vacation but only for the hours 9-2:30. No coverage is available for sick time coverage. Riverview has vacation relief available.
Without adequate relief budgets coverage of workload becomes
increasingly difficult (see Table 5). This imposes additional stress on all employees.
Table 6 describes the approximate number of weeks of vacation accrued by occupational therapy staff within the WRHA. The total number of weeks of vacation required to be covered within the region totals 653 weeks. The line described as "per week" indicates the number of staff/EFT who would be absent if the weeks of vacation were taken evenly throughout the year.
Table 6: Years of Service and Weeks Vacation
CGH GGH HSC SBGH SO VGH DLC MHC RVHC Totals 0-3 9 6 28 17 7 3 4 3 5 86 4-9 2 1 20 6 4 1 2 2 0 39 10-19 0 4 24 9 1 2 1 0 4 45 20+ 0 0 4 1 0 0 0 0 0 5 #Staff 11 11 76 33 12 6 7 5 9 170 Weeks 35 42 308 126 42 23 25 17 35 653 Per Week 0.7 0.8 5.9 2.4 0.8 0.4 0.5 0.3 0.7
Note: Data from Community Therapy Services/ Rehabilitation Centre for Children/ Personal Care Homes was not available. Casual staff was not included in this table.
Research
As health care funding is being more critically associated with evidence based practice the availability of a research budget is desirable in ensuring that treatment is effective and based on best practice.
Salaries
Specific salaries will not be discussed in this document. Salary ranges have been included in the Winnipeg Regional Health Authority - Profile of the Allied Health Workforce- Occupational Therapy, June 2001 document.
The School of Medical Rehabilitation recruits top students and the salary is relatively poor at graduation when compared to other professions with similar responsibilities and education.
Work Patterns
It is assumed that many therapists work part-time by choice although newer graduates may prefer full-time employment. The WRHA payroll information indicates that 51.2% of occupational therapists, not
including casual workers, report being employed in a part-time position.
At the present time, over 20% of therapists report working at more than one location.12 (See Table 2) Whether this reflects a lack of full time positions, varied interests, the need for greater remuneration, etc. is unknown.
Occupational therapy is primarily a female profession with over 90% of practicing therapists being female (See Table 4) and the increase in maternity benefits from six months to one year could have workforce implications.
The area of difficult to fill positions has not been explored and there exists the possibility that certain areas of practice are less desirable and may become difficult areas to service in the future. Weekend coverage has increased for certain programs ensuring that patients receive a continuum of care and that discharge is not delayed based on lack of availability of occupational therapy care. Overall this is a positive move but may result in difficulty covering the Monday to Friday positions left vacant due to weekend time off. Relief budgets are
provided for this coverage but staff may not be available.
National Exam
In order to be a member of the Canadian Association of Occupational Therapists, applicants must have graduated from an accredited
occupational therapy program or a program recognized by the World Federation of Occupational Therapists, have Canadian citizenship or authorization to practice OT in Canada, have completed 1000 hours of supervised fieldwork as part of their education, and must successfully complete the CAOT Certification Examination. "The purpose of the CAOT Certification Examination is to ensure that all applicants for CAOT membership demonstrate they have met a minimum standard in the written application of professional and applied knowledge prior to admission in the Association."40 The cost of writing the examination is $350.00.
Private Practice
The growth rate in private practice has been gradual but steady. The most common areas of practice are pediatrics and occupational medicine.
Use of Support Personnel
In a study completed by Russell and Kanny in 1998 the use of aides in occupational therapy practice was examined and it was suggested that occupational therapists would benefit from taking a proactive role in determining how best to utilize aides to improve service delivery. 41 In an effort to optimize efficiency the ratio of OTs to aides must be determined. The CAOT endorses the use of support personnel as a method of expanding and increasing access to OT services. 42 CAOT provides recommendations in regards to support personnel training and encourages their membership in CAOT.
VI. Education
Information
A fact sheet paper on Changes to Educational Requirements and a Position Statement on Entry Level Education of Occupational
Therapists in Canada were compiled by the Canadian Association of Occupational Therapists and provided information about the new educational requirement for academic accreditation effective 2008.43,44
It was announced in November 2001 that a professional Master's degree would be the minimum entry requirement to the profession in Canada as of 2010. As of 2008, CAOT will only grant academic accreditation to programs leading to a Master's degree as the entry credential. The decision to proceed to Master's level entry was based on the evolution of occupational therapy practice to more independent settings requiring a higher level of autonomy and a need for more mature students capable of advanced critical thinking and evidence based practice. Increased management and administrative abilities are required in these more independent settings.
Potential benefits include enhancement of professional status,
enhancement of research capability, improved preparation for labour force, increased remuneration, and improved autonomy. A Master's level would more accurately reflect the length, scope, and rigor of the program.
The School of Medical Rehabilitation is introducing a new program for occupational therapy in the year 2003. The new program will provide a Master's designation following a first degree. Students will be required to complete a general degree in Arts or Science or another approved degree prior to entry into the program. The undergraduate degree has a number of pre-requisite courses. As a result of this change in
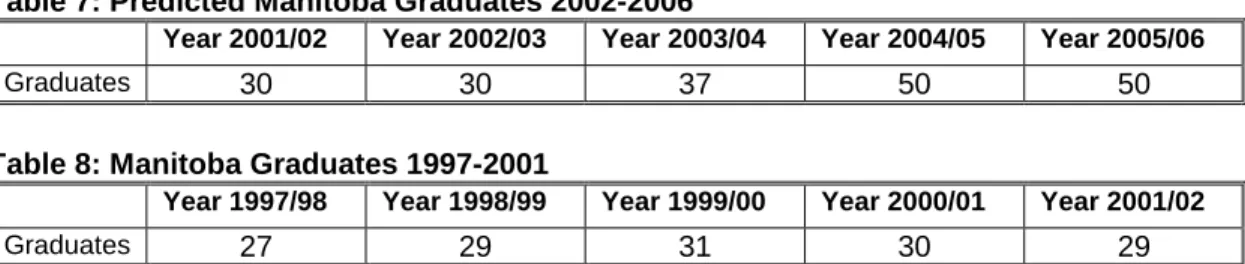
past enrollment at the University of Manitoba, School of Medical Rehabilitation, Occupational Therapy Division has been 30 students per year. The graduating class will increase to 40 students for 2003 and then 50 students for 2005. (See Table 7) The students convocate in October of the second academic year indicated in the table.
Table 7: Predicted Manitoba Graduates 2002-2006
Year 2001/02 Year 2002/03 Year 2003/04 Year 2004/05 Year 2005/06
Graduates 30 30 37 50 50
Table 8: Manitoba Graduates 1997-2001
Year 1997/98 Year 1998/99 Year 1999/00 Year 2000/01 Year 2001/02
Graduates 27 29 31 30 29
The School of Medical Rehabilitation has been discussing the need for a greater diversity in the make-up of the students selected for the program and the need to recruit students from rural and northern Manitoba and those with Aboriginal ancestry has been identified. 45
Entrance requirements for the school are competitive with the average GPA for the years 1997-2001 being 3.7 out of a maximum of 4.5.
The annual tuition fees and costs for books/supplies are substantial. The required clinical placements and internships not only incur costs for the students but also decrease their earning power over the
summer break. The annual fees including supplies, books, and clinical placements costs are as follows; Year 2 - $5718.05 and Year 3 - $5827.65.46 These amounts do not include the cost of the first year of university, which is required prior to entry into the program nor the costs associated with the Summer Fieldwork courses which are required at the end of both second and third year. Costs for the first year of the new program are not available as the costs for the new program have not been determined as yet. Many students entering the
program in the past had already completed degrees or more than one year of university education.
Fieldwork is an integral part of the education of occupational therapy students. Over the course of their program the students have
placements in a variety of settings including community, acute care, rehabilitation, and rural setting.
Students participate in six placements including 2-four week and 4 six-week placements for a total of 1200 hours of practical experience. CAOT requires that therapists complete a minimum of 1000 hours of fieldwork over the course of their studies in a variety of practice areas.47 All sites for fieldwork must be approved by the University Academic Fieldwork Coordinator or by CAOT. A minimum of one placement outside of Winnipeg is required. Students are provided with financial assistance to cover accommodation and transportation costs for placements outside of Winnipeg except for the two summer
fieldwork placements. The University of Manitoba is the only university in Canada to provide this kind of support. Students pay a registration fee for their clinical placement. Two summer fieldwork placements are required and may take place at sites across Canada
Each year approximately 180 occupational therapy fieldwork placements are provided in Manitoba and Saskatchewan with the majority of placements occurring in WRHA facilities. 47 (See Appendix Education Information)
Within the WRHA occupational therapists with one year of experience are expected to supervise a minimum of one student per year.
Therapists within the region frequently assist with student education as sessional lecturers.10
It is evident from Table 9 that the majority of occupational therapists practicing in Manitoba are graduates of the University of Manitoba (81.6%). 12 The location of graduation indicated reflects the location at which the therapist received their first degree in occupational therapy allowing them to practice. The graduates may have gone on to receive degrees at higher levels at the University of Manitoba or other
universities. The University of Manitoba has continued to offer the degree completion program and many of the foreign and Canadian trained graduates may have initially registered in Manitoba at the time they came to complete their degrees.
Table 9: Educational Background of Working Occupational Therapists in Manitoba (First OT Degree) – April 1st. 12
Location of Graduation Number Registered Percentage
Manitoba 296 81.6 Canada 41 11.3 Foreign 23 6.3 No Response 3 0.8 Total 363 100 Student Supervision
The ability to provide supervised clinical practice for students is an important factor in the recruitment of new graduates. The ability to provide student placements affords the facility an opportunity to
preview performance of potential staff members. When students have positive experiences they are more likely to apply for employment at that facility. It is extremely important to create a vision of a good working environment for students as an aid to recruitment.
The supervision of students requires a commitment of time as well as a manageable caseload. In situations where staff shortages may exist or caseloads are high, staff may view the supervision of students as a hardship. It may be particular important to compete for internships
during which time students can assist somewhat with caseloads and may be more actively assessing and seeking out work experiences.
VII. Licensure
Information
The Association of Occupational Therapists of Manitoba (AOTM) is the provincial regulatory organization for the profession. The association is responsible for the protection of the public and in this capacity the association registers qualified individuals to practice and addresses any complaints against its members. The Occupational Therapists Act was proclaimed in 1985 (see Appendix). A new Occupational
Therapists Act received Royal Assent in July 2002 but will not come into effect until the date is set by proclamation.
Prior to licensure applicants must have completed a minimum of 480 hours of work within the three years preceding the date of application or have completed a reentry program in the past 18 months or have graduated in the previous 18 months. Applicants must have graduated from the University of Manitoba occupational therapy program or educational equivalency. Applicants must not have a regulatory history that would prevent registration. The annual registration fee is $185.00 for practicing and conditional members and $74.00 for non-practicing and reentry candidates. Applicants applying from outside the country pay a credentialing fee as well. Mutual Recognition Agreement has been signed with other Canadian provinces.
At present the AOTM does not have a continuing education
requirement nor does it require its members to maintain malpractice insurance. These requirements are likely to change under the new act.
Re-entry candidates are required to complete a re-entry program consisting of an examination as well as a period of supervised practice. This examination may become a requirement for all applicants under the new act.
VIII. Age Distributions and Retirement Information
Canadian healthcare providers are, on average, getting older. The Canadian Institute for Health Information (CIHI) reports that from 1994-2000 the average age has risen almost 2 years from 39.1 to 40.8 years.13
There has not been a demonstrable age increase in occupational therapists in Manitoba from 1999-2001. (See Table 10) There are only 10% of occupational therapists in Manitoba working past the age of 50 years.
Table 10: Age Distribution of Working Occupational Therapists 1999-2001 – April 1st AOTM 12
Year Total 20-29 30-39 40-49 50-59 60-69 No Response # % # % # % # % # % # % 1999 314 80 25.5 106 33.8 90 28.7 30 9.5 2 0.6 6 1.9 2000 335 81 24.2 116 34.6 98 29.2 32 9.6 3 0.9 5 1.5 2001 363 95 26.2 125 34.5 105 28.9 31 8.5 3 0.8 4 1.1 Avg% 25.3 34.3 28.9 9.2 0.8 1.5
Table 11: Age Distribution WRHA Occupational Therapists 2001
Within the WRHA the age ranges are similar to the provincial ranges with the majority of therapists being in the 30 to 39 age range (45.6%) representing 93 employees. The age distributions indicate that only
Age Distribution of WRHA Occupational Therapists
0 20 40 60 80 100 29 39 49 59 69 More Age Range Fr equency
three occupational therapists are working past the age of 60 and the age 50-59 group represents 4.4% of the total working group.
Table 12: Age Distribution of WRHA Occupational Therapists
Age Ranges in Years WRHA # WRHA %
20-29 56 27.5 30-39 93 45.6 40-49 43 21.1 50-59 9 4.4 60-69 3 1.5 70+ 0 0 Total 204 100%
Early retirement is becoming more common and this is particularly true for the public sector with 55 being the most popular retirement age for that group. As well, women tend to retire earlier that men, likely as a result of the age difference between spouses.48
Table 13 indicates the year at which WRHA occupational therapists will reach age 55, 60, and age 65. Over the next five years 11 occupational therapists will reach the age of 55. This represents 5.4% of the
workforce.
Table 13: Number of WRHA Occupational Therapists Age 55, 60, and 65 Year Age 55 Age 60 Age 65
2002 5 2 0 2003 1 1 0 2004 2 1 0 2005 1 0 0 2006 2 0 2 Totals 11 4 2
Data from Community Therapy Services/ Rehabilitation Centre for Children/ Personal Care Homes was not available.
Employees are entitled to an unreduced pension benefit once their age plus years of service total 80. Table 14 indicates the number of
employees at each site that will reach Magic 80 over the next five years.
Table 14: Number of WRHA Occupational Therapists Attaining Magic 80 Year CGH GGH HSC SBGH SO VGH DLC MHC RVHC Totals 2002 0 0 1 0 0 0 0 0 0 1 2003 0 1 0 0 0 0 0 0 0 1 2004 0 0 0 0 0 0 0 0 1 1 2005 0 1 1 0 0 0 0 0 0 2 2006 1 0 2 0 0 0 0 0 0 3 Totals 1 2 4 0 0 0 0 0 1 8
Data from Community Therapy Services/ Rehabilitation Centre for Children/ Personal Care Homes was not available. Information from the Healthcare Employees Pension Plan indicates
that 20% of members with Magic 80 at age 50 retire and 25% of members with Magic 80 at 55 years of age retire.