Hannah Lea Pieper
An undergraduate proposal of a thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in
the Department of Exercise and Sport Science in the College of Arts & Sciences.
The University of North Carolina at Chapel Hill 2020
Approved by:
J.D. DeFreese, PhD
ACKNOWLEDGEMENTS
First and foremost, I wish to express my deepest gratitude to my incredible thesis advisor, Dr. J.D. DeFreese, for the endless time and aid you devoted to helping me with this research project. I never would have imagined completing a project of such breadth was within my capabilities, but thanks to your guidance and knowledge, it happened. Thank you for allowing me to realize that research doesn’t have to be boring and for teaching me about all about burnout and the many aspects of the research process that led to my interest in pursuing this project. Thank you for your remarkable patience and endless solutions to my many, many questions. It is whole-heartedly appreciated that your great advice for my study proved monumental towards the success of this study. I would also like to recognize the invaluable assistance that my thesis committee members, Dr. Johna Register-Mihalik and Dr. Zachary Kerr, provided during my study. Your generous devotion of time amongst such busy schedules has meant so much to me.
I wish to acknowledge the support and great love of my family. Dad, your constant and unwavering display of care to your patients has shown me what selflessness truly is. I can only hope to be as great of a physician as you are one day. Mom, your interest in my research and regular update requests are just a glimpse of your enormous heart and thoughtfulness. Thank you for listening to me and always keeping me motivated! Noah, thanks for setting the bar high. Your intelligence motivates me daily to push my limits and set the greatest goals. You’re an amazing person and an even more amazing brother. Stone, thank you for being my shoulder to lean on and listening ear. You give the best advice when the road gets tough and keep me going; this work would not have been possible without all of your input.
TABLE OF CONTENTS
ABSTRACT………...6
CHAPTER 1………7
Introduction….………7
Statement of the Problem………8
Purpose of the Study…..………12
Significance of Study…..……….. 12
Research Questions/Hypotheses………13
CHAPTER 2……..………18
Introduction/Theoretical Framework of Burnout………..18
Theoretical Framework of Burnout Prevention….………21
Prevalence of Burnout in Medical Residents…….………22
Psychosocial Factors………..24
Perceived Stress…..……….. 24
Perceived Social Support……….. 25
Demographics…..………..26
Gender…..………..26
Age/Number of Years in Training…..……….. 27
Average Number of Hours Worked per Week………. 28
Specialty Type………...30
Summary…….……….. 31
CHAPTER 3…….……… 33
Procedure…..………34
Measures….………..35
Burnout….………36
Perceived Stress….……….……..37
Perceived Social Support…..………38
Demographics……….………..39
Data Screening…..………....………30
CHAPTER 4………….………...….41
Preliminary Data Screening….………...……..41
Descriptive Variables and Demographic Statistics……..………...……..41
Results in Accordance with Hypotheses………...………42
Tables………46
CHAPTER 5…………..………...50
Discussion……….50
Limitations………56
Conclusion……..………..57
ABSTRACT
Burnout is an increasing medical phenomenon in the healthcare world and is particularly detrimental to lives and work of medical residents. Despite this, little research is focused on medical residents, who are at the forefront of their careers and prone to high levels of burnout. Therefore, the current study examined associations among burnout, burnout’s relation to
CHAPTER 1
Introduction
In recent years there has been a quiet exodus in addition to increasing medical errors from medical residents and by many who enter other healthcare professions (Hagemaster, 1983). These residents are unable to adjust to academic idealism and the realities of medical physician practice. Low pay, heavy and rigorous work hours, patient demands, and rotating shifts are invariable factors that can contribute to the burnout syndrome (Hagemaster, 1983). Extant research literature suggests there is still ongoing confusion as to what point the cross over from job stress to burnout occurs. Many do concede, however, that burnout develops when stress reaches an intolerable level and that medical residents are ideal hosts because of the demanding nature of their work (Baruch-Feldman et al., 2002; Halbesleben & Buckley, 2004; Shanafelt et al., 2002). The World Health Organization recently recognized burnout as an “occupational phenomenon” in its most recent Revision of the International Classification of Diseases (ICD-11), however, it has not yet been classified as a medical condition. According to Maslach, the syndrome is defined as being made up of emotional exhaustion (EE), depersonalization (DP), and reduced personal accomplishment (PA) (Maslach et al., 1996). Emotional exhaustion refers feelings of being exhausted and overextended due to the depletion of emotional resources. Depersonalization is characterized by the negative, cynical, and detached response to other people including colleagues and patients. Reduced personal accomplishment is the tendency to evaluate oneself negatively and feelings of unhappiness and dissatisfaction with one’s
Although there exists extensive amounts of research on burnout in medical professionals, research on burnout in medical residents, or physicians who have finished medical school and are receiving training in a specialized area (Shiel, 2018), is limited. This is unusual as both the nature of their work and their susceptibility to stress places them at a high risk for burnout. Medical residents, in particular, have an exceptionally stressful work environment. In a review of literature, Butterfield (1988) reported that inadequate sleep, fatigue, excessive time demands and lacking social support all represent the major stressors of a medical resident. The research that suggests burnout causes a diminished quality of patient care raises concern regarding the well-being of the resident. This concern stems from the known tendency for residents to make more frequent errors when giving care compared to medical professionals (Engel, Rosenthal, & Sutcliffe, 2006). They also lack the same number of training years and experience as professionals. Burnout, on top of inexperience, is a case where intervention and prevention should be sought tirelessly for. Throughout the transition from medical student to practicing physician, many residents face uncertainty regarding inexperience, treatment issues, and the making of life and death decisions (Engel, Rosenthal, & Sutcliffe, 2006). This is why it is crucial to examine how burnout differs in residents from that of the practicing physician. Additionally, a broader understanding of burnout in medical residents will aid in recognizing and preventing the medical phenomenon. Because the exact causal factors of burnout have yet to be understood, this study will examine several factors that have been hypothesized, but not yet empirically
Job stressors vary greatly and are often predisposing factors to illness. According to Gerson, stress symptoms can include distractibility, impaired concentration, confusion, drowsiness, depression, and anxiety responses such as chest pain and shortness of breath (Gerson, 1979). When considering these symptoms along with the high stress hospital environments, where residents complete their final years of training before practicing
With the increasing influx of women in the medical profession it is extremely relevant to examine the possible gender differences in the prevalence of burnout in medical residents (van der Velden et al, 2008). However, the previous research that exists presents conflicting results, with no real evidence that proves one theory over the other. For instance, Prins et al. (2010) indicated in a Dutch study that female medical residents are more emotionally exhausted but less depersonalized than their male colleagues. However, Fahrenkopf et al. found that there was no association between gender and burnout (2008), and another study found that women, in general, were at a higher risk for burnout. This discrepancy might have been caused by differences in subjects, instruments, specialties, research methods, and countries. The lack of clarity on gender differences in organizationally relevant phenomena, such as work burnout, frequently generates ungrounded speculations that may (mis)inform organizational decisions (Purvanova, Radostina, & Muros, 2010). These inconsistent findings create a strong need to better understand the association between gender and burnout in medical residents.
Though previous studies have focused on both age and number of years in training, often times mixed results were obtained by different studies. Burnout is a phenomenon that may present during medical school, and may develop or continue to exist in residents and practicing physicians. The literature to date seems to support the notion that there are a variety of factors during medical school that contribute to burnout in physicians, and that burnout is a phenomenon that develops cumulatively over an extended period of time (Dyrbye et al, 2006, Zoccolillo et al, 1986, Firth, 1986, Delva et al, 2002, McManus et al, 2004, Willcocl et al, 2004, Dahlin
studies have found an inverse relationship between the prevalence of burnout and age among physicians in practice, suggesting that early in their careers (Shanafelt et al, 2009, Shanafelt et al, 2012), physicians may experience little relief from the high levels of work-related stress
documented during training. However, because research on number of years in training and burnout in residents, specifically, rather than physicians, as a whole, is limited, this aspect of resident burnout needs to be further explored.
In addition to the previously mentioned variables of interest, there is one particularly pertinent factor that will be addressed in this exploration of burnout and it relationship to medical residents. Given the trend among medical students away from primary care medicine and
towards specific specialties that allow for more controllable lifestyles (Enoch et al, 2013), the identification of factors associated with specialty choice is important; burnout is one such factor. Unlike the other demographic variables of interest in this study, specialty type has little to no previous literature. The studies that do exist and are conducted in the United States
predominantly focus on only one residential specialty (Elmore et al., 2016, Lebares et al., 2018, West et al., 2011, Golub et al., 2007, Levin et al., 2017, Attenelo et al. 2018)- making it
can be used to cultivate subsequent plans of burnout prevention prior to the resident’s matriculation into solo practice.
Regarding the known prevalence of burnout, the few studies that do exist vary greatly in burnout percentages, going from 18% in American Obstetrics and Gynecology residents in Garza et al. (2004) all the way to 82% in a study among medical residents in Kenya in Raviola et al. (2002). Such extreme discrepancies are likely the result of methodological differences. Burnout studies conducted in the United States predominantly focus on medical professionals, rather than medical residents in particular. This makes it challenging to suggest that any previous research on medical professionals, as a whole, is applicable to residents, as both their high levels of responsibility and low levels of autonomy makes these relatively young residents highly susceptible to experiencing the negative effects of burnout. With this being said, the need for understanding the prevalence of burnout in American medical residents is great in order to further our knowledge of its development and causes.
of burnout in medical residents and the different types of medical specialties in which they pursue.
Research Questions
Based on theory, past empirical findings, and extant gaps in knowledge, multiple research questions arose. Primary research questions and hypotheses include:
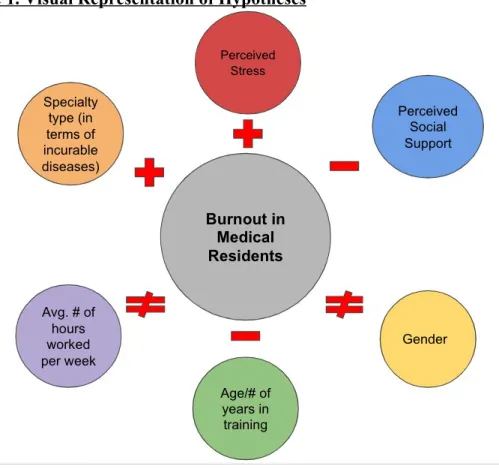
Figure 1. Visual Representation of Hypotheses
1. What is the overall prevalence of burnout in a sample of U.S. medical residents?
Hypothesis 1. Burnout will appear to be significantly prevalent in the majority (>0.5) of the sample of medical residents used for this study.
“nearly half of medical residents report[ing] at least one symptom of burnout” (Berg, 2018). Burnout in any proportion of the population of residents is unwanted, therefore, noting what proportion of residents in the sample have burnout in comparison to the AMA’s statement may help stress burnout’s severity and need for intervention. One study even suggests that as many as 82% of study respondents exhibited symptoms of burnout in a study among medical residents in Kenya in Raviola et al. (2002).
2. What is the association of perceived levels of stress and burnout levels in a sample
U.S. medical residents?
Hypothesis 2. High levels of perceived stress levels will appear to be positively associated with high levels of burnout in residents.
Justification. This hypothesis is predicated on findings from one particular study which suggested that burnout symptomology is initiated by the experience of job stress, and that high burnout levels were also associated with greater mood disturbance and poorer general health (Hillhouse, Adler, & Walters, 2000). The present study hopes to provide further validation of this stressor-response relationship.
3. What is association of perceived levels of social support and burnout levels in a
sample U.S. medical residents?
Hypothesis 3. High levels of social support will be negatively associated with high levels of burnout in residents.
fellow colleagues, which found that the best predictor if burnout appeared to be dissatisfaction with emotional support received from supervisors (Prins et al, 2004). However, the present study plans to examine perceived social support from individuals both at work and outside of work.
4. What is the association of gender and burnout levels in a sample of U.S. medical
residents?
Hypothesis 4. Burnout levels will not differ between men and women in a sample of U.S. medical residents.
Justification. Findings reported on the effect of gender on burnout in the past have been inconsistent (Maslach et al., 2001). Some studies found more women
showed symptoms of burnout; some reported that more men showed symptoms of burnout, while others found no difference between men and women. Thus, we hypothesize no association in the current study.
5. What is the association of age and burnout levels in a sample of U.S. medical
residents?
Hypothesis 5. Younger residents will report higher levels of burnout than older residents.
Justification. This is based on the findings of previous studies where age was consistently found to be related to burnout, as younger employees reported burnout more often than those over 40 years of age (Maslach et al., 2001).
6. What is the association of number of years in training and burnout levels in a sample
Hypothesis 6. Residents with less training years will report higher levels of burnout than more experienced residents.
Justification. This is based on the implication that burnout appears early in a persons’ career (Maslach et al., 1996).
7. What is the association of average number of hours worked per week and levels of burnout in a sample of U.S. medical residents?
Hypothesis 7. There will be no significant association between average number of hours worked per week and burnout.
Justification. Findings in the past have been contradicting and inconclusive. This association test hopes to serve as an additional resource added to the knowledge base regarding burnout and its relation to work hours.
8. What is the association of medical specialty type and levels of burnout in a sample of
U.S. medical residents?
Hypothesis 8. Residents in the specialties of emergency medicine and
psychiatrics, who tend to treat chronically ill or dying patients, will experience more burnout than residents in specialties like family and pediatric medicine, who more often treat young children and patients with curable diseases.
CHAPTER 2
Introduction- Theoretical Framework of Burnout
Maslach, whose definition of burnout was previously mentioned, has become a pioneer in this field of study as he both described burnout as a specific syndrome and developed a tool to assess it. The first of Maslach’s three primary symptoms of burnout syndrome is emotional exhaustion (Maslach et al., 1996). When a resident’s resources are depleted, they can no longer give of themselves psychologically. In the second symptom, depersonalization, negative feelings are directed toward the patient. The physician may start to feel that the patient actually deserves his problems. The third symptom involves personal feelings. The residents rate their own patient interactions poorly and are unhappy with themselves and the work environment in this final symptom of a reduced sense of accomplishment. Burnout is, undeniably, so multidimensional it is difficult to assess. Whether it occurs in the physician who is completely devoted to his
patients, or in the physician with no real commitment, each of the three symptoms of burnout become personally and professionally devastating. Emotional exhaustion, depersonalization, and reduced sense of accomplishment serve as key symptoms to help recognize the presence of the over-arching burnout phenomenon in individuals.
Burnout is particularly problematic for physicians who are at the forefront of their
conceptualized as a type of prolonged response to chronic emotional and interpersonal stressors that occurs in three stages. This framework is useful as it addresses both the emotional and physical aspects associated with resident burnout. Additionally, the framework provided is made specifically to examine burnout in medical professionals and practicing physicians.
Figure 2. Visual Representation of Burnout Framework
I. Stage of Exposure: The physician is exposed to a wide range of various stressors at work which have a depletory effect on the physician’s health and work. Initially resilient, stagnation occurs where the physicians are still doing their job but are gradually becoming detached from them, as opposed to total depletion. While exposure to stressors continues, there is a depletion of reserves which is
characterized by physicians questioning their own effectiveness and the value of their job (Dunn, Iglewicz, & Moutier, 2008).
which constitute the internal structure of the reservoir. While some physicians may resort to apathy to defend against a depleting reservoir, others may appraise specific stressors as depleting their reservoir and then focus on purposeful efforts aimed at replenishing it. However, these coping attempts may prove to be
adaptive or maladaptive depending on the stress levels, the ore-existing state of the individual components of the reservoir, and the extent of reliance on a particular coping strategy.
III. Stage of Burnout: This stage is dependent upon whether coping strategies have been successful in replenishing the depleting reservoir. When the rate of depletion from stressors exceeds the rate of replenishment with coping strategies over a period of time, physician reserves drop below critical levels resulting in what we know as burnout. When physicians are not successful at replenishing and shoring up the reservoir, the resulting burnout can lead to diminished mental health and compromised patient care (Agius, Blenkin, Deary et al., 1996).
From this point, occupational or job burnout can be divided into three degrees based on its severity (Endler & Parker, 1999). The first degree of burnout is characterized by a failure to keep up, complacency regarding the existing state of affairs and a gradual loss of reality. Second degree burnout is accompanied by increasing physical and emotional deterioration, where physicians seemingly have little energy to face their daily work. Third degree burnout involves major physical and/or psychological breakdown accompanied most commonly by depression as well as other forms of mental illness. Based on this burnout development theory in the
workplace, it is reasonable to assume that burnout may develop when residents perceive
variables such as residents who are younger in age, have had less years in residential training, and those who work in specialties with chronically or terminally ill patients.
Theoretical Framework of Burnout Prevention
This burnout prevention framework describes burnout as a relationship between the sources (stressors) and the proposed solutions (coping strategies- social support). The model could serve as an aid in the understanding of resident burnout to ultimately design more effective interventions for the disease. The model conceptualizes burnout as a chronic sequential process progressing through three stages of exposure-reaction-burnout. Designing burnout prevention strategies explicitly in terms of these three strategies will ensure that the proposed intervention is indeed addressing the phenomenon of burnout. Prevention strategies are conceptualized into three levels where primary prevention is targeted at the first stage of exposure, secondary prevention at the second stage of reaction, and tertiary prevention at the third stage of burnout. These burnout prevention studies have been developed from anecdotal reports with meticulously devised interventions to prevent burnout in healthcare professionals (Cosway et al 2000,
Edelwich & Brodsky, 1980). The present study, however, does not intend to propose in depth ideas on strategies to prevent burnout, rather, it hopes to understand differences in the variables of interest and how they vary across specialties. At a very minimum, this study may help interventionists understand the potential impact of future interventions across different specialties. One size intervention strategies may need to be reconsidered.
I. Primary Prevention: The action taken prior to the onset of depletion in the reservoir which removes the possibility that burnout will even occur. This prevention is
II. Secondary Prevention: The action which halts the progress of a depleting reservoir at its incipient stage and prevents further depletion which leads to burnout. Adaptive coping strategies replenishing the reservoir that has been depleted by stressors are designed as secondary prevention, because their intent is to prevent burnout from progressing.
III. Tertiary Prevention: All the measures which are available to limit the residual deficits following the burnout experience. Interventions that treat physicians who are already suffering from burnout are designated as tertiary prevention.
While these prevention strategies sound impressive, there is another level of prevention that needs special attention: primordial prevention. Primordial prevention, or, primary prevention, refers to the prevention of the emergence of stressors as predictors of burnout in physicians whom burnout has not yet occurred. Primordial prevention focuses on strengthening the reservoir through a variety of approaches intending to make future physicians more resilient to the effects of all kinds of every day stressors. The purpose of this study is aimed to discover new
Prevalence of Burnout in Medical Residents
Previous studies on burnout suggest that burnout levels are high among medical residents and may be associated with depression and problematic patient care (Thomas, 2004). However, currently available data are insufficient to identify causal relationships. Moreover, given the heterogeneous nature and limitations of the available studies, as well as the importance of having rigorous data to understand and prevent resident burnout, large, prospective studies are needed. Most of the research studies to date of burnout in residency were found to be small,
cross-sectional surveys, designed to show numerous bivariate associations between burnout dimension scores and personal factors, work characteristics, mental health disorders, and job performance measures
Regarding the known prevalence of burnout in residents, the few studies that do exist vary greatly in burnout percentages, going from 18% in American Obstetrics and Gynecology residents in Garza et al. (2004) all the way to 82% in a study among medical residents in Kenya in Raviola et al. (2002). Such extreme discrepancies are likely the result of methodological differences. Comparing research examining only one particular specialty to research examining all residential specialties make analyses problematic when it comes to generalizing results. Additionally, comparing residency burnout across different countries is also difficult as both the cultural and educational environments vary greatly from place to place. Burnout studies
among program intensity present themselves as confounding variables. With this being said, the need for understanding the prevalence of burnout in American medical residents is great in order to further our knowledge of its development and causes.
Psychosocial Factors
Perceived Stress
Burnout, in relation to perceived psychological stress, has been conceptualized as a person-environment transaction involving an appraisal of whether contextual demands exceed individual resources (Lazarus, 1996;1990). We can compare this to the first stage of exposure in Edelwich & Brodsky’s model of burnout, where exposure to stressors, or contextual demands, becomes present. In the second stage of reaction where depletion of reserves begins, or exceeds individual resources. and coping strategies, are attempted to reverse effects of stressors. Finally, in the final stage of burnout, where the rate of depletion from stressors and replenishment from coping strategies is compared in order to determine the level at which burnout occurs.
nonparticipating control group, suggesting that modifying the depersonalization dimension of burnout may be particularly challenging.
A study by Ospina-Kammerer and Figley also recruited 24 family practice residents who were available to participate in four weekly seminars to learn stress reduction techniques (2003). Following the intervention, mean MBI scores decreased in the intervention group. Both studies were small, though, possibly with limited generalizability. More concerning, however, is that intervention participants may have overrepresented older and more efficient residents, as only residents with enough free time to volunteer received the intervention and residents without free time were assigned to the control group. The small sample sizes also did not allow for efficacy to be analyzed by burnout severity. It may be that more randomized efficacy studies of stress management training workshops are needed.
While past research has proven that stress plays a huge rule in the work of medical residents, the intervention strategies attempted lack adequate solutions. We must first better understand stress and its relationship to burnout in order to implement effective plans for intervention. The present study plans to investigate and better understand how the onset of burnout is related to stress in medical residents, in order to aid in future intervention plans.
Perceived Social Support
stress, it makes sense that medical students satisfied with their own lives have been found to have low perceived stress and high resilience, and to seek social support. In addition, social support and good relationships with family members and friends increase quality of life. Low social support, on the other hand, is related to poor academic self-perception, as well as mental health problems among medical students.
One 2015 study by Park et al found that empathy and social support were positively
correlated while empathy and stress were negatively correlated. Where low levels of empathy lead to patient dissatisfaction, problems in medical communication, and even medical errors, so does burnout. In another study by Shanafelt et al, about three fourths of the residents in the study rated that talking with family, a significant other, or other residents were “significant” or
“essential” strategies, while residents with burnout were more likely to give such ratings to physical exercise and “a survival attitude” (2005). Additionally, residents with burnout reported feeling irrelevant and uncertain. Despite this, however, they were less likely to rate as important presentations in stress and depression, constructive feedback, and career counseling (Shanafelt et al, 2005).
Demographics
Gender
Some demographic and personality characteristics are presumed to be stable over time and are thought to precede the onset of burnout in residency. In past literature, however, few demographic factors seem to be consistently associated with burnout in residents. Informed by Edelwich & Brodsky’s burnout model, the demographic variables of interest in this study (i.e., gender, age/number of years in training, average number of hours worked per week, and specialty type) fit within the framework and will aid in our determination of potential causal factors of burnout in residents.
Because women have a higher lifetime risk of developing depression (Bertakis et al, 2001), it is reasonable to ask whether this increased risk extends to burnout as well. However, findings reported on the association of gender, an individual's subjective perception of their sex and their sexual orientation (National Institute of Health), with burnout in the past have been inconsistent (Maslach et al., 2001). Some studies found more women showed symptoms of burnout; some reported that more men showed symptoms of burnout, while others found no difference between men and women. Yet, not all studies reported burnout specifically by gender, and, therefore, these data are limited. Our study seeks to add to the current literature base
regarding burnout and its relation to gender.
Age/Number of Years in Training
Dahlin &Runeson, 2007, Rosal et al, 1997). While age does not directly fit into Edelwich & Brodsky’s model as a stressor or response to that stressor, it may be that age is a factor which causes some individuals to be more prone to these stressors than others.
While it is often assumed that one’s number of years in training, or how long one has participated in their residency education, is dependent upon age, this is not necessarily true. Some residents may have begun their medical school education immediately upon graduating from an undergraduate institution, while others may have changed careers after a few decades of working in another profession. Therefore, we must examine both age and number of years in residency training separately.
Although burnout is known to develop over time, one study found that age and burnout appeared to be inversely related in physicians, where younger physicians had higher levels of burnout than older physicians (Shanafelt et al, 2009, Shanafelt et al, 2012). This study is limited, though, as practicing physicians are much older and more experienced than medical residents. Where younger physicians present to be more burnt out than older physicians, it may be that younger residents are less burnt out than older residents, as they are newer relative to the system of medical education. Consequently, it is necessary to assess the relationship between burnout and the age of medical residents as their demographics, regarding age, differ greatly from that of the practicing physician.
Number of Hours Worked per Week
failed to decrease burnout levels (Panagopoulou, Montgomery, & Benos, 2006). It may be of use to place the average number of hours worked per week in comparison to the stressors in
Edelwich & Brodsky’s burnout model. We may see that work hours relates to higher perceived stress or lower perceived social support, and thus, interventions could be produced to
simultaneously target the variable which predisposes one to the stressor and the stressor itself. Findings suggested by both Geurts et al (1999) and Sargent et al (2004) suggested that increasing work hours are associated with higher burnout. From this, one might expect the mandatory work hour restrictions implemented by the ACGME to result in reduced
depersonalization scores, however, this was not found to be the case in the longitudinal study conducted by Gelfand et al (2004), which compared surgery residents’ self-reported work hours and burnout scores one week before and six months after the 80-hour workweek restriction. Instead, although work hours decreased significantly because of a reduction in educational activity and home call hours, mean burnout scores did not; in fact, depersonalization scores actually increased from 56% to 80% (Gelfand et al, 2004). However, in this analysis, burnout scores and work hours weren’t analyzed by residency year, so a significant but small effect within a single residency year may not be discerned. The work hours restriction failing to decrease any levels of burnout was further solidified by a recent study from Ripp et al. (2015) which found that the implementation of these duty hour restrictions did not change the burnout rates in American internal medicine residents. Pisljar et al. (2011) concluded that interventions to prevent work stress must look more closely at interventions that will help all hospital employees cope with their growing workload, longer hours and unsocial schedules.
might persist despite work-hour changes, whereas lower burnout rates might be observed in residents never exposed to the work-hour schedule prior to the restriction (2001). In addition, post restriction burnout levels were measured during the winter months, where burnout may already be higher. Another 2019 study by Sun et al. which examined burnout levels in
anesthesiology residents suggested that a greater number of hours worked per week and higher amount of student debt were associated with a higher risk of distress and depression, but not burnout (Sun et al. 2019). The study concluded that burnout, distress, and depression are all notable among anesthesiology residents and that perceived institutional support, work-life balance, strength of social support, workload, and student debt impact physician well-being (Sun et al. 2019). The results from this particular study are not generalizable beyond this population of anesthesiology specialists to all other residents specialties, though. The present study will
address the gap of comparison among all resident specialty types, and whether some are more susceptible to burnout over others.
Specialty Type
relates to each one of these specialties in order to directly develop plans for intervention and treatment.
What we do know is that one study examined the associations between resident burnout and specialty choice with respect to perceived lifestyle controllability and income and found that emotional exhaustion burnout was significantly associated with choices of specialties with more controllable lifestyles (Enoch et al, 2013). On the contrary, however, reports from two Finnish studies (Korkeila et al. 2003; Olkinuora et al., 1990) revealed that burnout was found more in physicians who work in specialties that treat incurable, chronically ill, or dying patients in specialties such as Oncology, Pulmonary Diseases, and Psychiatry compared to burnout found in doctors with specialties who treat patients with favorable prognoses and curable diseases in specialties such as Obstetrics & Gynecology; Ear, Nose and Throat; and Ophthalmology. Another 2010 study in France compared burnout levels amongst two specialties: medical and radiation oncologists, and hematologists (Blanchard et al. 2010). The study found that burnout levels were highest amongst oncology residents. It suggested that interventions such as support groups, more intense coaching by senior physicians, training programs on “breaking bad news” and teaching of stress management skills (Blanchard et al. 2010). Though this study found possible causal factors of burnout, it lacked the comparison to all other medical specialties. In addition, being that both studies were conducted in European countries, where the social aspects of medical training is entirely different than it is in the United States, it is difficult to fully know whether these results can be generalized across U.S. residency training programs. Our study will further add information regarding the position that social support groups and teaching of stress management skills would be beneficial as an intervention to burnout.
Due to the literature on resident burnout still being in the preliminary stages of probing for associations in small samples, it is premature to conclude that different findings reflect true differences between specialties. Still, these studies, each with their methodological limitations, seem to suggest that resident burnout exists in various specialties and internationally. The studies also suggest that burnout is associated with stress and problematic clinical performance as burnout and stress often co-occur. However, we want to explore the relationship between the onset of burnout and various demographic variables, perceived stress, and perceived social support. Additionally, we believe that understanding resident burnout could be enhanced by deciphering the work characteristics that residents face, as they are complex and vary by specialty, program, and postgraduate year. Our study plans to characterize burnout, with a sufficiently large sample, and identify risk factors associated with burnout. From this, we hope to gain a better understanding of how preventative structural reform may be more beneficial than time-intensive stress management training, such as the interventions listed in the above studies.
CHAPTER 3
Research Design/Population Sample
This study used a cross-sectional study design through the use of a self-report questionnaire. The questionnaire was distributed online via Qualtrics to all of the medical residents in training at 32 randomly selected United States Allopathic Medical Doctor (MD) training centers, out of a total of 143 that exist within the United States. Notably, all Doctor of Osteopathic Medicine (DO) programs (36 schools) were excluded from the selection process due to the different nature of their training program. A list of all the U.S. MD medical schools was obtained from the Association of American Medical Colleges (AAMC). All Canadian and Pharmacy schools were excluded prior to being entered into a random choice generator system. The first 32 medical schools randomly chosen by the generator were used for this study.
expected about 412 responses from the first four schools, however, after contacting 32 schools, we received only 94 responses. This resulted in a response rate of approximately 1%, assuming that all program directors who did not directly indicate that they would not be allowing their residents to participate forwarded the survey email to their program’s residents. This response rate is merely an estimate, though, as we do not know for certain the total number of residents that this study reached.
Procedure
Following the ethics approvals from the University of North Carolina’s institutional review board, information about the study and requests for participation were electronically emailed out to the residential program advisors of four randomly selected schools at a time, for a total of eight times. Program advisors who agreed to allow their residents to participate in the research were administered the survey in one of two ways. Either the advisor directly provided the investigator with an email list of the residents in their program and the investigator emailed them, or a link to the confidential survey was provided to the program advisor who then
residents/program advisors were sent one last final reminder. Because the response rate from the first set of four randomly selected schools was not sufficient, a second wave of four randomly selected schools was sent the survey 24 hours after wave one was sent the initial reminder. This process was repeated until a sufficient number of responses were recorded, for a total of 8 waves, or 32 medical schools. The one and two-week reminder emails served the purpose of attempting to increase response rates. All questionnaire responses were anonymous and submitted via the use of Qualtrics. This was to eliminate any form of evaluating bias when analyzing the final data.
Before beginning the survey, participants were given information detailing the voluntary nature of the study as well as their right to withdrawal. Participants were given an estimate that the survey should take no longer than fifteen minutes. Consent was obtained as part of the online survey protocol. After consent was obtained, participants were given general instructions on how to complete the survey. For the first half of the survey, participants were asked to complete the questions assessing burnout, or their feelings toward their work as medical residents. For the second half of the survey, participants were asked to answer a series of questions regarding their perceived stress, perceived social support, gender, age, number of hours worked per week, and specialty type.
Measures
Demographics
Participants were asked to self-report their age, gender, medical school, number of years in their residency training, and what medical specialty they are currently practicing. Specialty type was divided into twenty broad categories for residents to select from. These choices included: Allergy and Immunology, Anesthesiology, Dermatology, Diagnostic Radiology, Emergency Medicine, Family Medicine, Internal Medicine, Medical Genetics, Neurology, Nuclear Medicine, Obstetrics and Gynecology, Ophthamalogy, Pathology, Pediatrics, Physical Medicine and Rehabilitation, Preventative Medicine, Psychiatry, Radiation Oncology, Surgery, and Urology. These twenty specialties were placed under three sub-categories for the purpose of analyses:
-The sub category primarily works with terminally ill or dying patients included: Pathology, Radiation Oncology, Neurology, Nuclear Medicine, Surgery, Anesthesiology, Emergency Medicine and Obstetrics and Gynecology.
-The sub categoryprimarily works with temporarily ill or problematic issues
included: Diagnostic Radiology, Dermatology, Medical Genetics, Physical Medicine and Rehabilitation, Urology and Psychiatry.
-The sub category primarily works with patients over long periods of time/follow-ups included: Allergy and Immunology, Internal Medicine, Pediatrics, Family Medicine, Ophthamalogy and Preventative Medicine.
Burnout
Burnout was measured using the Maslach Burnout Inventory- Human Services Survey for Medical Personnel (MBI-HHS (MP)) scale. The MBI was specifically designed for use with people working in health care. The MBI is the most widely used measure of job burnout. It has dominated the field as a research tool and, by the end of the 1990s, it had been used in 93% of the journal articles (Schaufeli &Enzmann 1998.) The 22-item self-report questionnaire covers the three domains of burnout: EE (8 items), DP (5 items), and PA (7 items). Answers were scored on a 7-point scale ranging from “never” (0) to “every day” (7) where higher scores signified higher levels of burnout (Fothergill et al., 2004). The factorial reliability and validity of the MBI has been established across cultures and occupations. The three dimensions of the MBI generated three scores for every individual respondent. The scores are computed by calculating the sum of all points for each section, where higher scores correspond to greater degrees of experiences burnout. A 2011 analysis of 84 published studies that report sample-specific reliability estimates for the three (EE, DP, PA) MBI scales found that the scales have strong reliability (Wheeler 2011, Lee 1996.) In addition to educator populations and general work populations, the MBI has been validated for the human services populations (Ahola, 2007; Gil-Monte, 2005; Maslach & Jackson, 1982; Poghosyan, Aiken, & Sloane, 2009.)
Perceived Stress
scale, ranging from 0 (Never) to 4 (Very Often). An example question item is: “How often did you feel that you were unable to control the important things in your work?” The total score is calculated by summing the responses. Individual scores on the PSS-4 can range from zero to 16 with higher scores indicating higher perceived stress. The PSS-4 was developed by Cohen and colleagues to measure the degree to which individuals perceive their life as stressful and has been widely used in the literature (Le & Young, 2017, Cohen & Williamson, 1988, Birks, McKendree, & Watt, 2009, Lebensohn, Dodds, & Benn, 2013). Despite this, the PSS has been used in many studies of health professionals and the general population and has demonstrated adequate validity and reliability (Reed at al, 2018).
Social Support
psychological health in allied health populations (i.e., sport medicine professionals, DeFreese & Mihalik, 2016).
Data Analysis
For the variables gender and specialty, a Chi-squared test will be used as both are categorical, discrete variables that will be tested against the categorical, discrete variables from the MBI-HSS scale. For the variables age and years of training, a t-test will be used as both are quantitative, continuous variables that will be tested against the categorical, discrete variables from the MBI-HSS scale. Beyond group differences that were examined, associations (i.e. bivariate correlations) among all study variables were also examined. The data analytic
procedures used to test the hypotheses include dichotomizing scores into burnout/non-burnout to consolidate data results into two categories. For the purpose of this study, we will follow the common approach of considering individuals having at least one symptom of burnout if they have high scores, as defined by the MBI-HSS interpretation key, in EE (score of 27 or higher), DP (score of 13 or higher) or reduced PA (score of 39 or higher) subscales (Dyrbye 2009).
Evidence dictates that high scores on these subscales can distinguish the clinically burned out from the non-burned out (Schaufeli 2001). This is because this approach identifies individuals whose degree of burnout places them at increased risk of potentially serious personal and professional consequences (Dyrbye 2008 & 2010, Shanafelt 2010, West 2006 & 2009).
Table 1. Dichotomy of Burnout Scores for Analyses
Burnout No Burnout
Emotional Exhaustion (EE) ≥ 27 < 27
Depersonalization (DP) ≥ 13 < 13
Personal
Accomplishment (PA)
CHAPTER 4
Results
Preliminary Data Screening
Skewness and kurtosis values for all variables were normal based on best practice guidelines for data screening. Data were missing for several of the variables, however, the missing data did not exceed 5% for any one variable so mean imputation was utilized. Data was collected from 94 participants, none of which were removed from analysis. Altogether,
preliminary screening of study data resulted in no obvious violations of the assumptions of multivariate analyses. Accordingly, all study cases were included in models testing study hypotheses. In the models, however, listwise analyses were used as not all participants had completed data for each variable.
Demographic Variables and Descriptive Statistics
Table 2 contains relevant demographic statistics of participants. The ratio of male to female was 1:1.8. The mean age of participants was 30.72 with a standard deviation (SD) of 4.25 years. The average number of years in training was 2.36 (SD= 1.02). The average number of hours worked per week was 63.95 (SD= 10.94). About a third of the sample specialized in pediatrics 33 (35.1%) followed by specialization in Psychiatry 8 (8.5%). All other specialties averaged 2.46 participants and 7 participants chose “other” listing the following specialties: Ear, Nose and Throat, Orthopedic Surgery, Otolaryngology and Internal Medicine-Pediatrics
Combined. Specialties not listed in “other” were categorized into one of three sub-specialty groups (Table 8): sub-group 1 being residents who primarily work with terminally ill or dying patients (Pathology, Radiation Oncology, Neurology, Nuclear Medicine, Surgery,
Dermatology, Medical Genetics, Physical Medicine and Rehabilitation, Urology and Psychiatry;
n=14) and sub-group 3 being residents who primarily works with patients over long periods of time/follow-ups (Allergy and Immunology, Internal Medicine, Pediatrics, Family Medicine, Ophthamalogy and Preventative Medicine; n=43). Descriptive statistics, including the Pearson correlation and p-value scores are presented in Tables 3 and 4. Response options were
dichotomized into having burnout or not having burnout based on whether or not participants met the “high” score criteria from the MBI-HSS interpretation key. Relative to response options, participants reported high levels of burnout dimensions as well as high levels of perceived stress. Perceived social support had reported responses that were high relative to response options. Descriptive statistics were comparable to previous published work on burnout and engagement.
Results in Accordance with Hypotheses
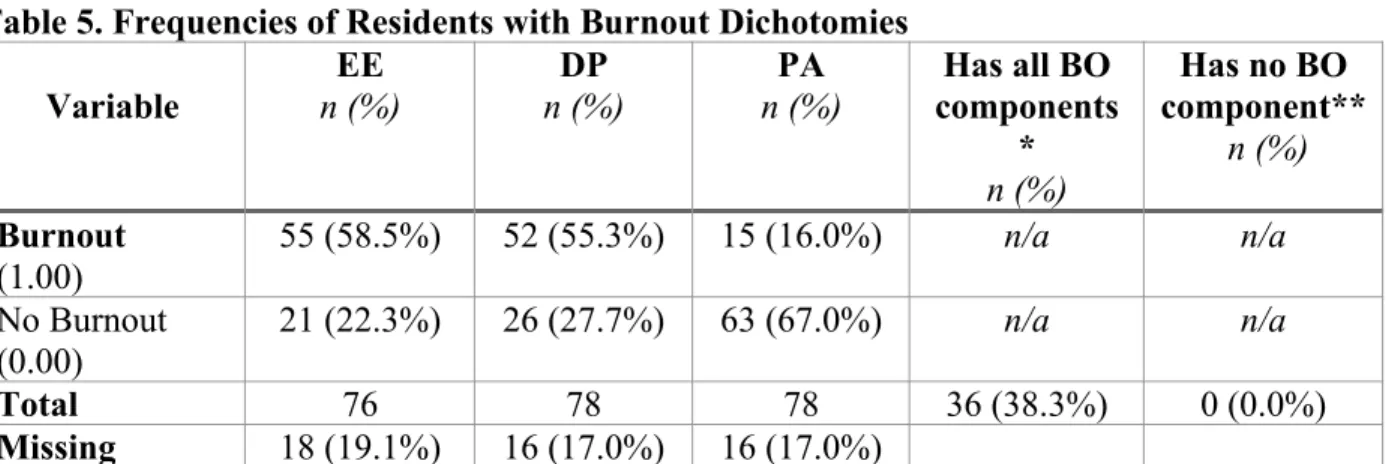
Hypothesis 1, which suggested that at least one dimension of burnout would be prevalent in at least half (50%) of the sample population was supported by the data. Every medical resident (100%) in the study exhibited elevated levels of at least one dimension of burnout: EE, DP or PA. Emotional exhaustion is having feelings of being exhausted and overextended due to the depletion of emotional resources. Depersonalization is characterized by the negative, cynical, and detached response to other people including colleagues and patients and reduced personal
accomplishment is the tendency to evaluate oneself negatively and feelings of unhappiness and dissatisfaction with one’s accomplishment on the job (Maslach et al., 1996). Out of these
participants, 38.3% exhibited elevated levels of all three components of burnout, as seen in Table 5.
and DP (EE= <.005, DP= .001) were significant at the 0.01 level (Table 4). However, the burnout value PA was not significantly associated with the perceived stress scale as the p-value was only p=.158.
Hypothesis 3, which posited levels of social support would be negatively associated with levels of burnout in residents, was supported by the data for all three components of burnout. The p-value for emotional exhaustion (p<0.000), the p-value for depersonalization (p=0.003) and the p-value for personal accomplishment (p=0.002), were all significant at the 0.01 significance level, according to Table 4.
Hypothesis 4, where burnout levels were predicted to not differ between men and women in a sample of U.S. medical residents, was also partially supported with regards to DP and PA, as their p values (0.709 and 0.838, respectively) were both greater than the 0.05 significance level. On the other hand, there was a significant relationship between gender and EE (p= 0.029). The calculated chi-square value of EE= 4.762 was less than the critical value of 12.71 at the 0.05 significance level. The chi-square value of DP= 1.734 at the 0.05 significance level was less than the critical value of 12.71 and the chi-square value of PA= 0.482 at the 0.05 significance level was also less than the same critical value of 12.71 (see Table 6). Where the chi squared value is less than the critical value, we can accept the null hypothesis that there is no difference in burnout levels between male and females. Regarding frequencies, 100% of males and females indicated having at least one burnout symptom, and 28.6% of males and 51.9% of females indicated having all three burnout symptoms.
Hypothesis 5, which suggested that younger residents will report higher levels of burnout than older residents, was not supported by our data, as indicated in Table 4. The p-value
0.05, indicating no significance in a relationship at the 0.05 significance level. Additionally, follow-up group difference analyses did not support significant differences in age according to cut-off scores used to denote burnout prevalence.
Hypothesis 6, which stated that residents with less training years will report higher levels of burnout than more experienced residents, was not supported by our data. The p-values for number of years in training as a resident in relation to EE (p= 0.677), DP (p= 0.656) and PA (p= 0.315) were all greater than 0.05, indicating no significant relationship between the two variables at the 0.5 significance level. Similar to that of age, follow-up group difference analyses did not support any significant differences in the years of training residents have completed in
accordance with the dichotomized burnout scores used for this study.
Hypothesis 7, that assumed there will be no significant association between average number of hours worked per week and burnout, was supported by the data. Similar to hypotheses 5 and 6, the p-values for average number of hours worked per week and EE (p= 0.118), DP (p=0.487) and PA (p= 0.401) were all greater than 0.05, suggesting insignificant relationships at the 0.5 significance level.
Tables
Table 2. Demographic Frequencies for Medical Residents Sample (N = 81)
Variable n (%) M SD
Gender
Male Female Prefer not to answer
28 (29.8%) 52 (55.3%) 1 (1.1%)
n/a n/a
Age 81 (86.2%) 30.72 4.25
Number of Years in Training
1 2 3 4 >4 17 (18.1%) 30 (31.9%) 22 (23.4%) 9 (9.6%) 2 (2.1%) 2.36 1.02
Avg. # of Hours Worked per Week
79 (84%) 63.95 10.94
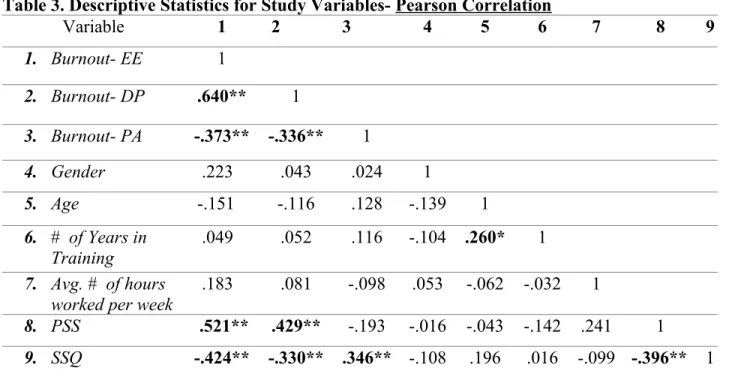
Table 3. Descriptive Statistics for Study Variables- Pearson Correlation
Variable 1 2 3 4 5 6 7 8 9
1. Burnout- EE 1
2. Burnout- DP .640** 1
3. Burnout- PA -.373** -.336** 1
4. Gender .223 .043 .024 1
5. Age -.151 -.116 .128 -.139 1
6. # of Years in
Training .049 .052 .116 -.104 .260* 1
7. Avg. # of hours worked per week
.183 .081 -.098 .053 -.062 -.032 1
8. PSS .521** .429** -.193 -.016 -.043 -.142 .241 1
9. SSQ -.424** -.330** .346** -.108 .196 .016 -.099 -.396** 1 *- Correlation is significant at the 0.05 level.
**- Correlation is significant at the 0.01 level
Table 4. Descriptive Statistics for Study Variables
Variable 1 2 3 4 5 6 7 8 9
1. Burnout- EE
2. Burnout- DP .000**
3. Burnout- PA .001** .003**
4. Gender .053 .709 .838
5. Age .193 .311 .264 .215
6. # of Years in Training
.677 .656 .315 .359 .020*
7. Avg. # of hours worked per week
.118 .487 .401 .641 .590 .784
8. PSS .000** .001** .159 .908 .748 .293 .069
9. SSQ .000** .003** .002** .336 .080 .885 .384 .002** P-Values (Significance)
Table 5. Frequencies of Residents with Burnout Dichotomies Variable EE n (%) DP n (%) PA n (%)
Has all BO components
*
n (%)
Has no BO component**
n (%)
Burnout (1.00)
55 (58.5%) 52 (55.3%) 15 (16.0%) n/a n/a
No Burnout (0.00)
21 (22.3%) 26 (27.7%) 63 (67.0%) n/a n/a
Total 76 78 78 36 (38.3%) 0 (0.0%)
Missing 18 (19.1%) 16 (17.0%) 16 (17.0%)
*-The column indicating “has all BO components” is expressive of the number of participants who met criteria for having all three burnout component symptoms.
**-The column indicating “has no BO components” is expressive of the number of participants who did not meet the criteria for any of the three burnout component symptoms.
Table 6. Chi-Squared Tests for Gender and Burnout Dichotomies
Variable Chi-Squared df P-Value
(Significance) EE
Male
Female 4.762 1 0.029*
DP
Male
Female
1.442 1 0.230
PA
Male
Female
0.703 1 0.402
*- Correlation is significant at the 0.05 level.
Table7. T-tests for Age, Number of Years in Training and Burnout Dichotomies
Variable t df P-Value (Significance)
EE
Age Number of Years in Training
1.937
0.479 7473 0.0570.472
DP
Age Number of Years in Training 0.983 0.376 76 75 0.076 0.750 PA Age Number of Years in Training
-.797
Table 8. Frequencies for Specialty Groups and Burnout Dichotomies
Variables
Sub Specialty
1-primarily works with terminally ill
or dying patients
n=23
Sub Specialty
2-primarily works with temporarily ill or problematic issues
n=14
Sub Specialty
3-primarily works with patients over long periods
of time/follow-ups
n=43
Does not have
EE(0) 7 (30.4%) 4 (28.6%) 14(32.6%)
Has EE(1) 16 (69.6%) 10 (71.4%) 29 (67.4%)
Does not have
DP(0) 8 (34.8%) 5 (35.7%) 15 (34.9%)
Has DP(1) 15 (65.2%) 9 (64.3%) 28 (65.1%)
Does not have
PA(0) 6 (26.1%) 6 (42.9%) 6 (14.0%)
Has PA(1) 17 (73.0%) 8 (57.1%) 37 (86.0%)
Total that has at least
one BO component* 22 (100.0%) 12 (100.0%) 43 (100.0%)
Total that has ALL
BO components** 16 (69.6%) 4 (28.9%) 27 (62.8%)
*-The total number of residents within each sub-group specialty who’s responses indicated that they have at least one symptom of burnout. It is also important to note that listwise analyses were used.
**-The total number of residents within each sub-group specialty who’s responses indicated that they have all three burnout symptoms
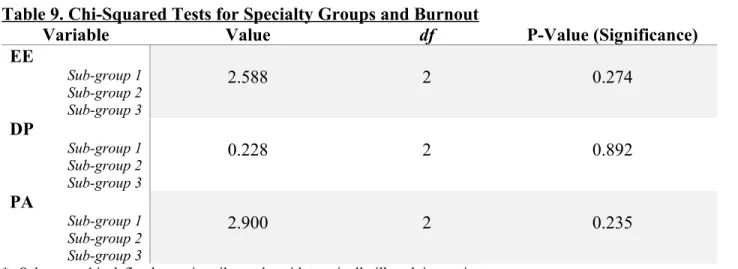
Table 9. Chi-Squared Tests for Specialty Groups and Burnout
Variable Value df P-Value (Significance)
EE
Sub-group 1 Sub-group 2 Sub-group 3
2.588 2 0.274
DP
Sub-group 1 Sub-group 2 Sub-group 3
0.228 2 0.892
PA
Sub-group 1 Sub-group 2 Sub-group 3
2.900 2 0.235
*- Sub-group 1 is defined as: primarily works with terminally ill or dying patients
Sub-group 2 is defined as: primarily works with temporarily ill or problematic issues
CHAPTER 5
Discussion
The study investigated how distinct psychosocial and demographic variables were
associated with medical resident burnout in a sample of U.S. medical residents. In line with study hypotheses, the results indicated that high levels of burnout were associated with multiple
psychosocial outcomes, including: higher levels of perceived stress (EE and DP) and lower levels of perceived social support (EE, DP and PA). Significant group differences within the dimension of emotional exhaustion were also found when participants were classified based on the binary conceptualization of gender, with females reporting higher levels of burnout than males. In addition, trends within specialty sub-groups were also found on all burnout dimensions where residents who tend to treat chronically ill or dying patients appeared to have higher
burnout levels than other specialty sub-groups. However, there were no significant group
differences found. Insignificant relationships were also found between burnout and the variables age, number of years in training and average number of hours worked per week.
that also use the MBI is limited. The prevalence of emotional exhaustion (58.5%) was higher than in previously published studies where it ranged from 42% to 50% (Prins et al., 2007), while the prevalence of depersonalization (55.3%) was within the range of 34% to 70% found in prior work (Prins et al., 2007). Study participants scored worse on personal accomplishment, with 16.0% compared to a range of 19% to 23% in previous studies (Prins et al., 2007). The prevalence of moderate to high burnout in previously published studies of residents is widely variable, ranging from 18% to 82% (Prins et al., 2007), which makes it quite notable that this study exceeded the range. It may be because the competition for residency slots has been increasing as a result of new medical schools opening since the overview study was published. As trainees strive harder to achieve the highest scores and grades, this could potentially fuel a culture of competition and stress that could undermine social support amongst peers.
Additionally, seemingly exponential growth in the expectations of medical knowledge to be learned throughout medical and residency trainings as well as new competencies to be reached present additional challenges. The rapidly growing healthcare system is also something to note, as environmental and cultural shifts pose workforce shortage threats and can cause uncertainty (Dyrbye, Liselotte, and Shanafelt. 2016). This is concerning as studies suggest that residents who feel uncertain about the future are more likely to experience burnout (Shanafelt et al., 2002).
Residents with higher reported levels of perceived stress had significantly higher burnout scores than residents with low reported levels of perceived stress and residents with high
potential to be complex when further scrutinized. Most notably, there exists a causality dilemma of what came first: burnout or the other factors. Medical residents may not feel properly
equipped for the work they are required to perform. This problem can be described as a
discrepancy between theory and practice (Tyssen et al., 2000). Although residents have acquired much medical knowledge and skills throughout their medical education and training, the
acceptance of responsibility for the outcome of medical decisions is something that residents only experience in real-life scenarios with patients. This may lead to feelings of inadequacy when dealing with how to handle various situations appropriately. Residents may believe they are less competent than others actually perceive them to be. This is sometimes known as the “imposter phenomenon” and has been found to be prevalent in many different professions, but particularly in health care workers (Arena & Page, 1992; Bernard et al., 2002; Oriel et al., 2004). Increasing levels in this phenomenon may be the cause for the rise in perceived stress, lower support and, subsequently, burnout. Better preparing residents for the responsibility of real-life scenarios prior to their matriculation into specialty practice may aid in a higher perceived self-competence. The presence of additional skilled assistance in each respective specialty may be a factor in reducing perceived stress, and subsequently, reducing burnout in residents. However, establishing causality in burnout is critical in understanding prevention tactics. Future research may need to explore experimental methods to investigate the causality of the aforementioned variables.
Participants who reported their gender as female reported a significantly higher amount of emotional exhaustion burnout than residents who reported their gender as male. The study found no evidence of gender differences regarding depersonalization and personal
However, as females have been reported to experience more psychological distress and
psychosocial complaints than males, based on a study that used data from the National Survey of Families and Households (Simon, 2002), it may be of interest to explore how marriage and family responsibilities play a factor in social support levels in addition to mere gender
differences. Thus, examining marital status and whether a resident lives alone or with family, as well as whether these relational factors may change during the residency period, may be of interest to explore in future research, factors not examined in this current study.
Age and years of training were found to have no significant relationship to burnout scores. However, with a larger sample size, it is likely that age would become significantly associated with emotional exhaustion, i.e., older residents or those longer in training would report less emotional exhaustion than younger residents or those shorter in training. The results of this study were inconsistent with past research, where the majority of residents fulfilling the criteria for burnout were in their first year of residency (Prins et al., 2007; Martini et al., 2004). It may be that burnout levels have become increasingly more common over time, and the reason we no longer see a difference in burnout levels amongst different ages and levels of training is because the risk for burnout has risen for all residents, not just the medical residents at the beginning of their career. After studies conducted following the implementation of the
Residents who were categorized as primarily tends to treat chronically ill or dying patients, (sub category 1) had the highest prevalence of burnout in this study based on statistical trends alone, though no group differences were statistically significant. This is in somewhat agreeance of past literature, such as two Finnish studies (Korkeila et al. 2003; Olkinuora et al., 1990) which revealed that burnout was found more in physicians who treat incurable, chronically ill, or dying patients as opposed to those who treat patients with more favorable prognoses. Other studies revealed that the highest prevalence of burnout was found in the “front-line” specialties of EM, family practice, and general internal medicine (Shanafelt, Boone, and Tan et al. 2012), although past research on specialty sub-divisions is limited and inconsistent. Our sub category 3 included family practice and internal medicine, however, EM, or emergency medicine, was placed in a different sub category (1) for the purpose of this study. Perhaps more standard and well-known grouping categories for specialty type may aid in future research comparison abilities. There seems to exist a dilemma regarding the basis on which to categorize specialties, as many specialties fall into more than one category. Two factors that may be of interest in future research are specialty categorizations based on length of commitment to patients and stress levels related to specialty responsibilities. These groups may also differ across various medical
networks- whether they will be working in a private practice or solely as a hospitalist. Further research is needed to determine differences within practice locations. Transparency of long-term training objectives, dependent on specialty-type, especially those related to progressive
Being able to identify the factors that contribute to resident burnout may enable a residency program to alter its curriculum or training environment in an effort to prevent or ameliorate this condition. Due to the high prevalence and negative effects of resident burnout, research is needed to determine other associated or contributory factors and to determine
effective intervention strategies to prevent or treat burnout during residency training. Consistent with Edilwich and Brodsky’s burnout model, nearly all of the residents who participated in this study had indicated either nonexistent or unsuccessful coping strategies in replenishing their depleting reservoir. Stressors were causing a rate of depletion in residents that exceeded the rate of replenishment with coping strategies. After a period of time, the individuals’ reserves dropped below critical levels which resulted in what we know as the extremely high levels of burnout. Both stressors and coping strategies in this model need to be further explored. It may also be beneficial for future researchers to look into experimental methods. Testing potential burnout intervention methods against the standard psychosocial health practices (i.e., standard of care) of resident training programs may allow researchers to see if burnout interventions may diminish pre-existing burnout levels. Areas for future studies should include more specifically analyzing the effects of having additional, readily available skilled supervisors during training, work-home interference, specializing in primary care that works with patients over long, extended periods of time, and significant others that may play a role in the development of burnout.
Limitations
allowed their residents to participate. Nevertheless, they do represent programs in a variety of settings and all regions of the United States. Repeating the study with an incentive may increase response rates across different specialty types and may provide more responses overall.
Advertising the study as an examination of specialty group differences may also help improve response rates, as more residents may feel the need to help contribute to the diversity of the study. This sample size limitation may also have been the reason for some insignificant results whose p-values were borderline significant.