1 Introduction: Tobacco use is the leading cause of preventable disease worldwide. Although
smoking has declined in some developed countries, the global burden of tobacco-related
mortality is shifting to vulnerable populations in low- and middle-income countries. Tobacco use
among adolescent females in this population is becoming a growing concern. A systematic
review of the literature was undertaken to assess public health programs that aim to address the
issue of tobacco use in adolescent females at the community level in low- and middle-income
countries.
Methodology: A systematic review of the literature from 2010 to February 2014 was undertaken
to determine how many studies and what types of studies have been published that focus on
community level interventions in female adolescents in four countries representative of the
current tobacco epidemic: Turkey, India, Korea, and Argentina. The search was limited to
Pubmed, Web of Science, and Global Health online databases. Studies adhered to strict
eligibility criteria to eliminate studies not pertinent to adolescent female tobacco use. Studies
were stratified into tiers based on the type of study discussed. Further examination of the studies
revealed the aspect and determinant of the tobacco epidemic addressed in each study.
Results: Twenty-seven studies were included in the systematic review after undergoing
qualitative analysis based on eligibility and search criteria. Of these 27 studies, 22 were
descriptive studies. The most common strategy addressed was monitoring tobacco use and
prevention strategies, including determining prevalence rates in relation to the presence of other
factors.
Conclusion: This systematic literature review indicated there are limited studies on current
community level interventions. From this, a conclusion can be made that more studies of all
2 middle-income countries. In addition, more articles documenting interventions at the community
level need to be published to provide adequate literature on this issue to guide future public
3 INTRODUCTION
The tobacco epidemic is a major public health issue facing the world today. According to
the World Health Organization (WHO) (2013a), tobacco use is the leading cause of preventable
disease worldwide. The face of this tobacco epidemic is ever-changing. No longer is smoking
associated with higher economic status, as it was for most of the 1900s. Today, tobacco use is
becoming more common among vulnerable populations of lower socioeconomic status,
including populations in most low- and middle-income countries. Many factors are contributing
to this transformation, and new public health strategies and programs at all levels are needed to
prevent tobacco use in the vulnerable populations most at risk for succumbing to this public
health epidemic. A variety of approaches that anticipate and respect the diverse values, beliefs,
and cultures of these new communities at risk would help to decrease tobacco use in these
populations (Public Health Leadership Society, 2002). Defeating this epidemic would fulfill one
of the most important aspects of the Public Health Code of Ethics: addressing the fundamental
causes of disease to prevent adverse health consequences and outcomes (Public Health
Leadership Society, 2002).
The purpose of this paper is to demonstrate the need for community level public health
programs aimed at tobacco use in adolescent females in low- and middle-income countries. First,
this paper will provide an overview of the tobacco epidemic and its public health effects to
explain the urgency of the issue, along with summarizing the variety of tobacco products
available, explaining the determinants contributing to this epidemic, identifying adolescent
females in low- and middle-income countries as the population at risk, and explaining current
tobacco control interventions. A systematic review of the literature will assess how public health
4 tobacco use in adolescent females. To answer this question, literature will be reviewed to identify
the number of published studies detailing community level efforts to attack tobacco use in
adolescent females. The studies identified will then be reviewed to assess the effectiveness of the
programs by determining if any significant finding can be taken from the study. Lastly, this
review will attempt to identify common themes among the results in the research regarding the
determinant and tobacco strategy addressed. The review will focus on four low- and
middle-income countries: Korea (also described as South Korea or the Republic of Korea in the
literature), India, Argentina, and Turkey; all of which are at risk in this epidemic and are relevant
examples of other countries where adolescent females face a similar threat.
Effects of Tobacco Use
The addictive properties of nicotine and the negative health effects of tobacco use are
widely documented. Tobacco use is the leading global cause of death, causing six million deaths
a year, and also adds significant strain to the healthcare system, costing more than a half a trillion
dollars globally each year (WHO, 2013a). Beginning in the 1950s and 1960s, causal
relationships between smoking and cancer and respiratory illnesses began to develop (United
States Department of Health and Human Services (USDHHS), 2014). Since this time, smoking
and tobacco use have been the topic of numerous US Surgeon General Reports and various
reports issued by the WHO, along with studies too numerous to mention that link tobacco use to
increased mortality, cancers, cardiovascular disease, respiratory illnesses, birth defects, and
reproductive disorders (USDHHS, 2014). To confound the health issues associated with tobacco
use, nicotine, which is in tobacco, has been proven to have addictive properties. These addictive
properties cause those that initiate tobacco use to become dependent and prevent them from
5 associated with negative health consequences. Smokeless tobacco products, such as tobacco
chew, snuff, and other culture specific products like Gutkha used in India, cause mouth and oral
cancers. In addition, nonsmokers that are exposed to secondhand smoke are also at risk for
negative health consequences. Over 600,000 deaths worldwide are contributed to exposure to
secondhand smoke every year (WHO, 2013a). These data demonstrate that the morbidity and
mortality associated with tobacco use have resulted in a public health epidemic
Types of Tobacco Products
Understanding the numerous tobacco products available is critical in understanding the
breadth of this epidemic. Tobacco products are products made entirely or partly of leaf tobacco
as raw material, which are intended to be smoked, sucked, chewed or snuffed (WHO, 2014b).
All contain the highly addictive ingredient, nicotine. Smoked products have expanded beyond
traditional cigarettes. The goal of these products is to be less expensive to gain users that
normally could not afford traditional cigarettes, including youth and other populations that
traditionally have not been tobacco users. Bidis, little cigars, and kreteks (clove cigarettes) are all
similar to traditional cigarettes and often include flavors that are aimed at appealing to youth.
Bidis and kreteks are most often used in Asia. However, these inexpensive products are also
exported to other low- and middle-income countries (State of Connecticut, 2010). Little cigars
look like cigarettes and include filters unlike traditional cigars (State of Connecticut, 2010).
Various forms of loose tobacco that allow the user to construct the cigarette are sold at lower
costs than manufactured cigarettes. Finally, hookah is a pipe used to smoke Shisha, a
combination of tobacco and fruit or vegetable that is heated and where the smoke is filtrated
6 Smokeless tobacco products include a broad category of products that are intended to be
sucked, chewed, or snuffed (State of Connecticut, 2010). Chewing tobacco comes in the form of
loose leaf, plug, or twist, and involves chewing on the product that is placed in between the gum
and cheek. Snuff is finely ground tobacco that can be dry, moist, or in sachets. Although some
forms of snuff can be used by sniffing or inhaling into the nose, most smokeless tobacco also
users place the product in their cheek or between their gum and cheek. Users then suck on the
tobacco and spit out the tobacco juices, which is why smokeless tobacco is often referred to as
spit or spitting tobacco (Eriksen, Mackay & Ross, 2012).
Many tobacco products that are specific to certain cultures also fall under the smokeless
tobacco category. The culture of a country not only influences the type of product, but also who
uses these products. For example, India is known for many smokeless tobacco products that
contain or are derived from the areca (betel) nut or its plant, including gutkha, paan with tobacco,
and mawa. These products are more commonly used by women than men (American Cancer
Society, 2009). Most all of these contain additional flavoring(s) that add to the allure of the
product. Gutkha is rapidly becoming the most popular form of chewing tobacco among teenagers
and children because it is available in small packets that are convenient for a single use, uses
flavoring agents and scents, and is inexpensive with a cost of about 2 US cents. Khaini is the
most commonly used chewing tobacco in India; it is derived from crushing dried tobacco leaves
and mixing it with slake lime (American Cancer Society, 2009). The product is then chewed as a
quid (American Cancer Society, 2009). Finally, companies continue to develop new smokeless
products that are likely to appeal to youth, such as dissolvable tobacco products that are flavored
7
Determinants of Health and the Tobacco Epidemic
Since the tobacco epidemic is a public health issue, it must be tackled on the population
level. The population can be defined as broadly as the global society or as narrow as a
community that shares a common characteristic, such as geography or ethnicity. The first step in
tackling an issue that is affecting the health of a population, such as tobacco use, is to identify the
social and physical environments or determinants that shape the issue. Like other issues affecting
health, many determinants play a vital role in the tobacco epidemic and many of these
determinants are interrelated. These determinants can be identified by applying one of the
various frameworks for public health to the issue of tobacco use. Interventions must then be
developed that aim to modify one or more of these determinants. The ecological framework is
one such framework that provides a basis for identifying the determinants of any public health
issue. The Institute of Medicine (2003) has defined the ecological model as "a model of health
that emphasizes the linkages and relationships among multiple factors (or determinants) affecting
health.” Many ecological frameworks have been developed, but they all share a common theme
regarding the interrelationship of macro-level determinants that include policies and societal
norms and micro-level determinants, including individual characteristics or the virulence of a
disease agent, that interact along complex and dynamic pathways to produce health at a
population level (Institute of Medicine, 2002). For the purposes of this paper, the Dahlgren and
Whitehead model will be used. This model is illustrated in Figure 1 (Institute of Medicine,
2002).
As the figure illustrates, there are five factors that influence the health of a population: 1)
innate individual traits and biological factors, 2) individual behavior 3) social, family, and
8 the global, national, state, and local levels. The model demonstrates that these factors all
influence each other. The dotted lines show where there is a multi-directional flow of influence
between the different factors. The model also illustrates that over the life span of on individual,
broader issues influence health more than the individual’s characteristics. This model can be
applied to the tobacco epidemic to attempt to identify determinants of tobacco use.
Figure 1
The most important individual trait that affects tobacco use is the individual’s biological
reaction to the addictive properties of nicotine to become dependent. This affects whether a
person can stop smoking or using tobacco on their own. Certain identifiable demographic data
also fit in this group. Smoking is often associated with some common demographic
characteristics. However, these characteristics alone do not determine tobacco use, but are
influenced by the other factors in the paradigm. For example, in some communities it may be
9 population. Knowing this helps to identify the target population of an intervention, but it does
not answer the question on why this may be. Applying the rest of the framework, various
determinants can be identified that influence smoking in males in the specific population.
Individual behaviors or lifestyle factors are similar to individual traits in that they are
micro-level factors that influence health of the individual. This level includes individual attitudes
and knowledge about health and associated behaviors. Looking at the previous example of
smoking in males, one factor that may be identified at this level is that males are less likely to see
a healthcare professional that could educate them on the risks of smoking and cessation
therapies. Other factors in the model may control this healthy-seeking behavior, such as living
and working conditions that prevent access to healthcare. Individual behavior can also impact
others in the population. If a male child witnesses his father smoking, the child then may be more
likely to smoke as he gets older. Another individual lifestyle factor is how a person deals with
stress; smoking may be a behavior that an individual uses to relax and relieve stress. The reasons
for the stress would also need to be controlled and could be related to issues within the family
network, along with living and working situations.
Social, family, and community networks play a large role in determining the health of an
individual and community. As stated previously, it may be more acceptable in some social,
family, and community networks for one to smoke. These networks also may influence the type
of tobacco product used, as evidenced by the use of culture specific products. Certain networks
may affect different health behaviors at different levels. The family network may have more or
less influence than one’s peers or social network, depending on the behavior. Cultural norms that
10 that spread beyond the these networks would fall under the outer layer of the model (Ruderman,
2013).
Many living and working conditions are represented in Figure 1. This macro-level factor
encompasses many areas; all of which are pertinent to addressing the tobacco epidemic. It may
be acceptable among people in certain occupations to smoke, while other occupations may not
allow smoking while on the job. For occupations where it is acceptable to smoke, not only is the
smoker’s health likely to be negatively impacted, but also those of their non-smoking co-workers
that may be exposed to secondhand smoke in the workplace. Public health programs and
healthcare services may provide necessary information regarding tobacco risks, prevention and
cessation strategies, but not all members of the community may have access to these services due
to economic barriers or barriers associated with the physical environment, such as no access to
transportation or easily accessible roads from their home to where the healthcare services are
located.
The highest level that determines the health of population is indicated by the outer circle
in Figure 1. This level includes the broad social, cultural, economic, health and environmental
conditions and policies at the global, national, state, and local level that shape public health.
These conditions include the regulatory actions taken by the government that affect health.
Governments that increase taxes on tobacco products can deter tobacco use by making the
products financially unattainable, with a goal of decreasing tobacco use and improving the health
of the society. Government policies many also limit areas where one can smoke to decrease
secondhand smoke exposure to others, while also making harder for those that currently smoke
to continue to do so. However, some countries may have a lack of resources to implement
11 can allow tobacco use in its population to go unchecked. Large scale marketing and educational
messaging also make up the larger social environment and can have a large effect on determining
the health of the population. In regards to tobacco use, tobacco companies use marketing tactics
to normalize tobacco use within a community, while educational messaging regarding the
dangers of tobacco use attempt to counteract these tactics (WHO, 2013b).
Ecological models are necessary in public health because they provide a starting point for
determining the issues that influence a health. Once one of the models is applied, it is clear that
the health determinants may vary depending on the behavior and community at risk. All levels of
determinants, along with their interrelationships, must be identified to develop adequate
intervention programs that improve the health of the public (Institute of Medicine, 2003).
Tobacco Advertising, Promotion, and Sponsorship Activities
Tobacco advertising, promotion, and sponsorship (TAPS) activities play out in the social
environment and influence tobacco use (WHO, 2013b). Many activities comprise TAPS beyond
the traditional marketing that is done via various media, including television, radio, billboards,
the internet, and print outlets that falsely associate tobacco use with desirable qualities, such as
youth, energy, glamour and sex appeal (Eriksen et al., 2012). Tobacco companies often sponsor
various popular events aimed at youth, including sporting and music events (WHO, 2013b).
Companies will offer free samples of their products to get people addicted and will distribute
coupons or offer inexpensive products to populations with low economic resources (Eriksen et
al., 2012). Companies will also give away non-tobacco items with the logos of their products. In
many low- and middle-income countries, these products would normally be financially
unattainable for the person to whom they are given. Often these free tobacco and non-tobacco
12 bars (WHO, 2013b). Tobacco packaging and products are developed to specifically allure certain
populations into using tobacco (WHO, 2013b). All of these widespread activities attempt to
flood the marketplace to make it appear that tobacco is just like any other advertised consumer
product and to help people view the companies favorably, which in turn counteracts any
educational messages to the contrary (WHO, 2013b).
Through TAPS activities, tobacco companies seek to normalize and glorify tobacco use
in various populations and communities. While TAPS activities are still targeted to current users,
TAPS activities also encourage tobacco use in new markets and new populations, especially
youth at age an age prior to likely have initiated use and women in low- and middle-income
countries (Eriksen et al., 2012). Both of these populations are likely to not be current users and
are viewed by the industry as new potential markets. Young people are especially vulnerable to
becoming tobacco users. Tobacco companies count on these new users becoming addicted to the
product, guaranteeing a steady amount of customers for many years. Adolescents are at a critical
transitional phase in their lives. TAPS activities communicate messages that using tobacco
products will satisfy their social and psychological needs, such as popularity, peer acceptance
and positive self-image (Eriksen et al., 2012). Exposure to TAPS usually occurs at before age 11
and increases positive views of tobacco and curiosity about tobacco use (WHO, 2013b). The
exposure to TAPS also makes tobacco use seem less harmful than it actually is and influences
beliefs and perceptions that tobacco use is common; this increases the likelihood that adolescents
will start to smoke or use other forms of tobacco (WHO, 2013b). In order to remain successful,
TAPS activities need to have greater influence than other determinants in the social environment,
including anti-tobacco educational campaigns and government regulations. This necessity
13 TAPS activities are increasingly targeting females. Women in many low- and
middle-countries have not used tobacco traditionally, are viewed by the tobacco industry as an enormous
potential emerging market because of their increasing financial and social independence and
have been targeted them accordingly. As a result of these TAPS endeavors, smoking among
women is expected to double worldwide from 2005 to 2025 (WHO, 2013b). Many cigarette
brands have been specifically developed to appeal and be marketed exclusively to this market.
Existing brands have also been restyled for the same reason. In addition to the exclusive
marketing that increases their attractiveness to women by associating tobacco use with increased
independence and beauty, these products have characteristics, such as different diameters and
lengths than a traditional cigarette, and packaging that make the product more appealing to
women (State of Connecticut, 2010). In South Korea, the development of specific brands of
cigarettes for women alone increased smoking rates among women from 1.6% to 13% between
1988 and 1998 (WHO, 2013b).
Populations at risk in the Current Tobacco Epidemic
As countries in the developed world have successfully begun to implement successful
tobacco control and regulatory strategies, along with educating their populations about the
hazards of tobacco use, smoking has declined in some higher- and middle- income countries.
Large scale regulatory policies, along with education of the negative health outcomes, have
successfully helped to transform the social norm of tobacco use and smoking that was previously
common in these countries. However, tobacco use is still on the rise globally (WHO, 2013a) and
the global burden of tobacco-related mortality is shifting to vulnerable populations in low- and
14 low- and middle-income countries. By 2030, it is estimated that 80% of the world’s 8 million
tobacco-related deaths will occur in these countries (WHO, 2013a).
Tobacco use among females is becoming a growing concern in this global epidemic. In
all WHO regions except Europe, girls aged 13–15 years old are using tobacco at higher rates
than women aged 15 and older (Eriksen et al., 2012). This could be a reflection of aggressive
tobacco industry marketing to girls, particularly in the low- and middle-income countries. The
high rates amongst girls is very concerning, as these data suggest potential substantial increases
in tobacco use for women in the near future (WHO, 2013b). In some countries, such as
Argentina, the smoking rates for girls aged 13 to 15 years is already higher than their male
counterparts (Eriksen et al., 2012). Smoking among women is expected to double worldwide
from 2005 to 2025 (WHO, 2013a). The most effective public health programs address tobacco
use prior to initiation (WHO, 2013b), which is most often prior to age 18 (USDHHS, 2014).
Strategies for Controlling the Tobacco Epidemic
To address this global epidemic, WHO developed the Convention Framework for
Tobacco Control (CFTC), a treaty based on evidence that was signed by 168 countries in 2004.
The CFTC recognizes the global tobacco epidemic and outlines policies that governments at the
country level must undertake to decrease the demand for tobacco use and address the tobacco
supply (WHO, 2014). The framework went into effect in 2005. All aspects of the tobacco
epidemic are focuses of the framework, including developing a regulatory strategy to address all
of the complex factors of the tobacco epidemic. Some of these factors include marketing,
exposure to secondhand smoke, and sales to minors (WHO, 2014b). In 2008, WHO began
promoting six proven, demand-reduction strategies, collectively called MPOWER, that were
15 support government implementation of the provisions of the CFTC, including in developing
countries where the tobacco industry actively seeks new markets. The six strategies are:
1. monitoring tobacco use and prevention policies
2. warning about the dangers of tobacco
3. protecting people from tobacco smoke
4. enforcing bans on tobacco advertising, promotion, and sponsorship (TAPS)
5. offering to help persons dependent on tobacco quit tobacco use
6. raising tobacco taxes (WHO, 2013b).
All of these actions are designed to attack the tobacco epidemic on at the country
population level through enactment of policies designed to have the greatest impact in decreasing
the prevalence of tobacco use. About 2.3 billion people in 92 countries are currently covered by
at least one government policy recommended by the CFTC for at least one of these areas (WHO,
2013b). In addition, in 2012, Turkey became the first country to implement programs at the
highest level of achievement of the CFTC for all MPOWER strategies.
The news has not all been positive in regards to the CFTC and MPOWER. Legal
challenges and litigation in many countries have prevented government policies from being
realized. For example, in the US, legal action taken by tobacco companies has killed regulations
mandating new graphic warning labels on tobacco products that are recommended in the CFTC.
The US is not alone. Other countries, including, but not limited to, Argentina, India, Turkey, and
Ireland, have faced similar legal challenges to the regulations and policies around tobacco
control measures, such as establishment of smoke-free public places and bans on certain TAPS
activities (Eriksen et al., 2012). Some countries, such as Korea, have yet to sign and
16 active role in broad tobacco control policies (WHO, 2013b). Low- and middle-income countries
often lack the financial and public health system resources to implement such expansive policies
required by the CFTC (Zabert et al., 2010).
The overall effect of these various barriers is that, despite the CFTC and the development
of the MPOWER strategies, tobacco use is still on the rise globally, especially among women
and girls. Even in Turkey, which is an exemplary country by WHO standards, prevalence rates
for current tobacco and cigarette use in females aged 13 to 15 years continues to rise. In 2009,
the prevalence rates for current tobacco use and cigarette use in this population were 7.4% and
5.2% respectively (WHO, 2009), which was higher than similar data from 2003, prior to the roll
out of MPOWER. Previous rates for current tobacco use and cigarette use were 4.4% and 3.5%,
respectively (WHO, 2009).
These facts beg the question of what other programs can be implemented to confront
tobacco use. Although government-wide policies are normally the most cost-effective way of
having an impacting the health of the highest number of people in a society, local public health
programs have the ability to make a large impact in the local communities where they are
performed and provide a stop gap until high-level governments can take necessary actions. Local
programs also help to put the focus on the specific populations at risk, whereas broad policies
can fail to address the other problems or needs contributing to a behavior in all of the jeopardized
populations. As was demonstrated in the Dahlgren and Whitehead ecological model of health,
determinants of health occur at every level in the society, from the individual to the community
to the broad society. A one step approach will not modify all of these factors. Even if the cases
where the government has or does in the future execute broad policies to influence health, local
17 the Public Health Code of Ethics, “identifying and promoting the fundamental requirements for
health in a community are of primary concern to public health” (Public Health Leadership
Society, 2002). Requirements can vary greatly among communities that make up larger societies,
such as countries, and they need to be adequately addressed in the community affected.
To assist with the design of community-based public health programs, a systematic
review of the literature will assess how public health programs at the community level in low-
and middle-income countries are tackling the issue of tobacco use in adolescent females. To
answer this question, literature will be reviewed to identify the number of published articles
detailing community level efforts to attack tobacco use in adolescent females. The studies found
will then be reviewed to assess the effectiveness of the programs by determining if any
significant finding can be taken from the study. Lastly, this review will attempt to identify
common themes among the results in the research regarding the determinant and tobacco
strategy addressed. The review will focus on four low- and middle-income countries: Korea (also
described as South Korea or the Republic of Korea in the literature), India, Argentina, and
Turkey, all of which are at risk in this epidemic and are relevant examples of other countries
where adolescent females face a similar threat.
METHODOLOGY
Data Sources and Search Strategy
The main data sources for this systematic review of studies of community level public
health activities targeting the use of tobacco in adolescent females in Turkey, India, Korea, and
Argentina were the electronic databases: Pubmed, Web of Science and Global Health. These
18 Medline and the two other databases were used because they would include any articles
published in journals from foreign countries that are not included in the Pubmed database.
Searches were conducted online with MeSH (medical subject headings) search terms for
the subject matter and target population, along with key word searches for each country. The
MeSH search terms included smoking cessation (also includes prevention and prevalence),
tobacco use, and adolescent female (defined as 13 to 18 years of age per MeSH), along with each
country name. The search phrase was (smoking cessation OR tobacco use) AND (adolescent
female) AND (Turkey OR India OR Korea OR Argentina). Korea was used to capture all studies
related to South Korea or the Republic of Korea. The same search was conducted across each
database and the last search was conducted on April 18, 2014. The search was limited to articles
and studies in humans from scholarly journals published from 2010 to February 2014.
The four countries included in the search were selected due to being representative of the
tobacco epidemic in adolescent females. They are all low- and middle-income countries, where
data has shown that tobacco use in adolescent females should be of concern. As the literature
review has described, smoking and tobacco use continue to rise in adolescent girls in Turkey,
tobacco use is higher in adolescent girls than boys in India, smoking rates among woman are
expected to double in Korea by 2025, and more girls are smoking than boys in Argentina. The
income level of these countries is also relevant. Low- and middle-income countries are more
likely to have limited resources and government support to fully realize broad population based
interventions (Zabert et al, 2010) and these issues are likely to be similar across countries in the
19
Eligibility Criteria
Studies that were selected from the initial search results for inclusion in the systematic
analysis adhered to specific eligibility requirements to minimize selection bias. The inclusion
criteria included:
• published 2010 to present
• available in full text on line via electronic resources
• published or translated in English
• included adolescents, defined as 13-18 years of age, in the study population
• included females in the study population
• conducted in India, Turkey, Argentina and/or Korea
• described an effect of a study conducted at the community level.
Studies were excluded based on the following criteria:
• did not include females or did not include any data specific for females
• included only adults, defined as older than 18 years of age
• did not take place in at least one of the four countries specified in the search strategy
• investigated only the health or pharmacologic effects of smoking and other tobacco use
• included immigrant populations
• studied drug therapies for tobacco cessation
• documented tobacco use as a gateway for other risk behavior
• discussed a duplicative study result that was already included.
These exclusion criteria were chosen because these types of studies were not the focus of this
systematic review. For example, studies that only included participants over the age of 18 were
20 significantly different than adolescents. Studies of immigrant populations were excluded, since
the cultures of the new countries where the population migrated or the cultures of the countries
from which the population migrated would likely affect the perceptions and attitudes of tobacco
products and usage. Research on the health and pharmacologic effects of nicotine and tobacco
were excluded, since these have been well documented in other literature reviews and research.
These criteria were applied first to the titles of the studies in the search results, which
included initially 299 studies. A study was removed from the result list if there was a clear
indication from the title that the study did not meet the meet the eligibility criteria. Next the
abstracts were reviewed in the same manner. Finally, the methods and results sections of each
study were reviewed in the same manner against the eligibility criteria to develop the final list of
studies for the data extraction. These reviews resulted in 27 articles that underwent data
extraction based on stratified criteria.
Data extraction and categorization
Articles were stratified to tiers, a common method in systematic reviews for
categorization of the articles. Articles were either placed in Tier 1, Tier 2, or Tier 3, depending
on the type of study the article described. Cross-sectional surveys, a type of descriptive studies,
were included in Tier 1. Tier 2 included analytical studies, such as intervention trials. Tier 3
included articles that did not fit into either of these categories, including program evaluations,
mixed-design investigations, and qualitative research. The studies in each tier underwent further
categorization to determine the tobacco control strategy that was addressed in each study. Studies
were categorized according to the following strategies: monitoring tobacco use and prevention
policies, warning against the risks of tobacco use, taxing of tobacco products, helping to quit
21 activities. Monitoring tobacco use and prevention policies included studies that established
prevalence rates and determinants of use, as these are commonly detected when attempting to
monitor tobacco use and determine effective prevention policies. To streamline the
documentation of the data extraction, these categories were simplified to the following category
titles that correspond to each of the six strategies: monitoring, warning, taxation, cessation,
secondhand smoke, and TAPS. Articles were also classified to determine the level or levels of
the ecological model that were examined. Level 1 correlates with the most inner tier of the
Dahlgren and Whitehead model and Level 5 corresponds to the outer most tier as depicted in
Figure 1. Level 2 includes individual lifestyle factors, Level 2 covers social, family, and
community networks, and Lever 4 encompasses living and working conditions. Level 1 factors,
such as demographic information, were included in all of the studies. Level 1 classification was
only included in the categorization if the study went beyond basic data collection and attempted
to address one of the innate characteristics on an individual in regards to tobacco use. Significant
outcome data specifically related to adolescent females included in each study were also
extracted. Finally, the type of product studied, along with where the study took place (country
and community level) were documented for each study in each tier. Extracted data from all
studies are included in table format in the results section. The results were then reviewed to
determine which studies showed a significant outcome for female adolescents, along with
identification of common methods, strategies, and results. Studies were also assessed to
determine any discrepancies among the results across studies.
RESULTS
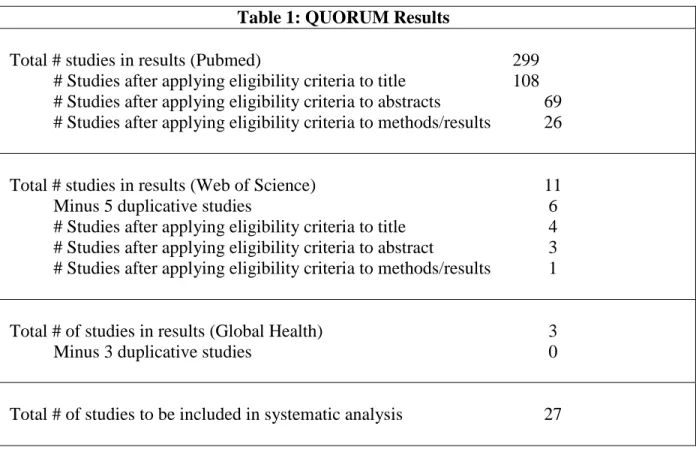
22 A detailed breakdown of the search results from initial search of databases to final
determination of inclusion for the data extraction and categorization are detailed in the following
QUORUM table (Table 1):
Table 1: QUORUM Results
Total # studies in results (Pubmed) 299 # Studies after applying eligibility criteria to title 108 # Studies after applying eligibility criteria to abstracts 69 # Studies after applying eligibility criteria to methods/results 26
Total # studies in results (Web of Science) 11
Minus 5 duplicative studies 6
# Studies after applying eligibility criteria to title 4 # Studies after applying eligibility criteria to abstract 3 # Studies after applying eligibility criteria to methods/results 1
Total # of studies in results (Global Health) 3
Minus 3 duplicative studies 0
Total # of studies to be included in systematic analysis 27
The most common cause for studies found during the original search results to not meet
the eligibility requirements during the title, abstract, or research and methods review was that the
study population only included adults or did not include the identified adolescent population.
Studies were also excluded if adult and youth data were combined, not allowing for the
determination of results for the demographic group covered by this systematic review. A
common reason for exclusion during the title search was an indication that the article described
23 Types of Studies
Table 2 includes the results of the breakdown of articles based on the tiers described in the
methodology section.
Table 2: Tier Categorization of Studies
Authors Tier 1 Cross-Sectional Surveys Tier 2 Analytical Tier 3 Other
Lee, Yun, Lee, Kim, & Jee, 2010
X
Stigler et al., 2010 X
Goenka et al., 2010 X
Sardana & Narian, 2011
X
Golbasi, Kaya, Cetindag, Capik, &
Aydogan, 2011 X Jayakrishnan, Geetha, Binukumar, Sreekumar, & Lekshmi, 2011 X Stigler, Perry, Smolenski, Arora, &
Reddy, 2011
X
Hong et al., 2011 X Das et al., 2011 X Ergruder et al., 2012 X Lim et al., 2012 X Surani and Shroff,
2012
X
Arora et al., 2012 X Mukherjee, Sinha ,
Taraphdar, Basu,& Chakrabarty, 2012
X
Arora et al., 2013 X
Jung & Chung, 2013 X Chun & Chung,
2013
X
Kim, Lee, Lim, & Kim, 2013 X Philip, Parambil, Bhaskarapillai, & Balasubramaman, 2013 X
Bhojani, Elias, & Devadasan, 2011
24 Authors Tier 1
Cross-Sectional
Surveys
Tier 2 Analytical
Tier 3 Other
Ortabag, Ozdemir, Bakir, & Tosun, 2011
X
Alderete et al., 2012 X Alderete, Erickson,
Kaplan, & Pérez-Stable, 2010
X
Alderete, Kaplan, Gregorich, &
Pérez-Stable, 2010
X
Salgado et al., 2011 X Mejia, Kaplan,
Alderete, Gregorich, & Pérez-Stable,
2013
X
Linetzky, Mejia, Ferrante, De Maio, & Diez Roux, 2012
X
Strategies and Outcomes
The detailed information extracted for the studies categorized as Tier 1 are described
25 Table 3: Data Extraction for Tier 1 Studies
Study Country, Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Lee, S., et al.
(2010)
Korea, Schools
Cigarettes Monitoring Determinants of tobacco use: past smoking
experience, parents smoking status, friends smoking status, ownership of a product with a cigarette brand logo, and intentions of smoking from close friends' cigarette offer.
No difference via gender on the influence of each determinant in smoking behavior
Level 1 and 3
Stigler et al. (2010) India, Schools Cigarettes, bidis, and chewing tobacco
Monitoring Effects of
westernization on tobacco use
Association with western influences increases tobacco use regardless of gender Level 5 Sardana & Narian, 2011 India, Schools Tobacco chew and non-tobacco chew products
Monitoring Prevalence and initiation of the use of tobacco and non-tobacco chewing products
No differences among genders in prevalence rates, but girls initiated each habit earlier
Level 2
Golbasi et al., 2011
Turkey, Schools
Cigarettes Monitoring Monitoring of prevalence and determinants
Did not have a significant number of females that smoked, unable to break down determinants specifically for females. Smoking family member and parents with low educational levels contributed to smoking in males.
26 Study Country,
Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Jayakrishnan
et al., 2011
India, Schools
Cigarettes and tobacco
Monitoring Knowledge of tobacco legislation and risks
Girls more aware of the smoking ban and links to mouth and oral cancers; results were significant.
Level 2 and 5
Hong et al., 2011
Korea, Schools
Cigarettes Monitoring Changes in prevalence of smoking from 2005 to 2009
Statistically significant decreasing trends in current smoking rate observed among small town and metropolitan city girls and smoking experience rate before 13 years of age for rural girls decreased significantly
Level 4
Das et al., 2011
India, Schools
Cigarettes Monitoring Prevalence rates and determinants
Number of females smokers too small to determine additional results beyond prevalence
27 Study Country,
Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Erguder et al., 2012 Turkey, Schools
Any Monitoring, TAPS, secondhand smoke
Prevalence rates Half of students reported they had been exposed to second hand smoking (SHS) at home and 80% reported they had been exposed to SHS in public places; three in ten students reported they had been exposed to pro-tobacco advertising in newspapers or magazines; one in ten had an object with a cigarette brand logo on it; and 7% had been offered free cigarettes by a cigarette company representative.
Level 4 and 5
Lim et al., 2012
Korea, National Quitline users
Cigarettes Cessation Cessation rates 13.4% of boys and 6.6% of girls maintained smoking cessation for 1 year; high level of self-efficacy had a preventive effect. Relapse was increased with marginal significance among girls with parents or other family members as quit supporters
Level 5
Surani & Shroff, 2012
India, Schools
Any TAPS Effects of pro- and anti-tobacco messages
Significant association found between exposure to marketing and promotions and intention to quit, but no significant relationships found between intention to quit and exposure to pro- and anti-tobacco media messages
28 Study Country,
Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Arora et al.,
2012
India, Schools
Any TAPS Effects of
tobacco use in Bollywood movies and tobacco promotional activities
Wearing a tobacco branded item increased tobacco use two-fold; those receptive to tobacco
promotions were three times more likely to use tobacco in the model that adjusted only for movie tobacco exposure. Level 5 Mukherjee et al., 2012 India, Schools
Any Monitoring Knowledge risks of tobacco use and smoking
Overall knowledge of risks higher in girls, but girls scored lower on knowledge of addiction, fetal harm, and second- hand smoke exposure Level 2 Jung & Chung, 2013 Korea, Schools Cigarettes and other smoked products
Monitoring Determinants of smoking Lower academic grades, higher disposable monetary allowance from their parents, more friends who smoked, and high smoking rate at their school-same for girls and boys
29 Study Country,
Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Chun & Chung, 2013 Korea, Schools Cigarettes and other smoked products
Monitoring Social and intrapersonal determinants of smoking Attachment to friends, smoking friends, stigma, and self-control were identified as common factors related to the onset of smoking in both male and females
Levels 2 and 3
Philip et al., 2013
India, Schools
Any Monitoring Tobacco use after intervention of prevention program consisting of anti-tobacco messages, tobacco task forces, interschool competitions, and educational handout materials for kids and school personnel.
Statistically significant
difference towards the future use of tobacco and awareness about the ill effects of passive smoking among boys and girls
30 Study Country,
Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Bhojani, Elias, & Devadasan, 2011 India, Schools
Cigarettes Monitoring Adolescent views of smoking
Female students reported
significantly higher disapproval of smoking; views of female smokers were negative for both males and females. Dominant themes defining perceptions about smokers included hostility, against family values, not aware of risks, and under stress.
Level 2
Ortabag, et al., 2011
Turkey, School nurse programs
Cigarettes Monitoring Health risk and health promoting behaviors
Girls had higher scores for health promoting behaviors, including stress management, and lower scores for smoking Level 2 Alderete et al., 2012 Argentina, School
Cigarettes Monitoring Exposure to racial insults and smoking
Those exposed to racial insults had increased smoking rates; higher rates in boys than girls
Level 2 Alderete, Kaplan, Gregorich, & Pérez-Stable, 2010 Argentina, School
Any Monitoring Determinants of type of product used
Boys used pipe tobacco more and indigenous populations were more likely to smoke hand-rolled cigarettes
31 Study Country,
Population Type of Product Strategy Addressed Outcome Measured Relevant Outcome Data Level of Determinant Salgado et al., 2011 Argentina, School
Cigarettes TAPS Association between smoking media literacy and smoking
Higher smoking media literacy had lower odds of being current smoker and lower odds of being susceptible to future smoking, but no breakdown of data specifically for girls.
Level 2
Mejia et al., 2013
Argentina, Schools
Cigarettes Monitoring Effects of gender roles on smoking
Egalitarian gender role was
associated with ever smoking in girls Level 2 Linetzky et al., 2012 Argentina, Schools
Cigarettes Monitoring, Secondhand smoke Effects of poverty on smoking After controlling for age and sex, students attending schools receiving social assistance were more likely to smoke and to purchase loose cigarettes, whereas school poverty was significantly associated with secondhand smoke exposure Level 4
No articles met the Tier 2 criteria. Table 3 categorizes the five articles that fell under Tier
3. The first was a mixed-design study that involved pre- and post-experimental phase that
included a qualitative component; the next two in Table 3 described qualitative data from
interviews or focus groups; and the last two detailed program evaluations and analysis of a
previous intervention. For the latter two, the level of determinant and strategy were documented
32 Table 3: Data Extraction for Tier 3 Studies
Study Country, Population
Type of Product
Strategy Outcome
Measured Relevant Outcome Data Level of Determina nt Kim et al.,
2013
Korea, Schools
Cigarettes Cessation Effect of smoking cessation program in girls on smoking rates
Among the 55 participants, 18 (32.7%) stopped smoking and 37 (67.3%) failed to stop after the 5 week intervention.
Level 2
Arora et al., 2013
India, Community
Any Cessation Focus group discussions that guided development of youth cessation program
Findings from these discussions indicate the importance of increasing individual
knowledge and self-efficacy in order to reduce and/or quit tobacco use, creating supportive environments through good role models and stronger policy enforcement, and the importance of a community-based setting.
Level 2, 3, and 4 Alderete, Erickson, Kaplan, & Pérez-Stable, 2010. Argentina, Community Cigarettes and ceremonial tobacco
Monitoring Effects of ceremonial tobacco use on prevention strategies Highlights the difference between secular and ceremonial motivations and behaviors suggesting ceremonial and regular tobacco use are conceptualized as separate issues in the minds of young girls and boys
Level 3
Goenka et al., 2010
India, Schools
Any Monitoring Indicator variables related to the program success
Interpreted data to provide in depth program evaluation
33 Study Country,
Population
Type of Product
Strategy Addressed
Outcome Measured Relevant Outcome Data
Level of Determina
nt Stigler et al.,
2011
India, Schools
Any Monitoring Explain the
intervention’s effects on tobacco use behaviors and intentions.
Findings suggest programs should increase knowledge about the negative health and social consequences, clarify the meanings that surround tobacco use for young people in India, help youth identify alternatives to meet certain needs (e.g., to look ‘cool,’
‘fashionable,’ or ‘western’), and build strong social norms, or environments where tobacco use is not acceptable
34 Discussion of Results
The results show that the most common studies conducted were cross-sectional surveys, which
comprised 22 of the 27 articles reviewed. Five additional studies were grouped in into Tier 3, while no
studies in this review documented new analytical studies. Two of the five studies in Tier 3 provided
further analysis of an intervention study and data that were previously published. Schools were the most
frequent place where the cross-sectional surveys took place. Considering the target population of
adolescent females, this was to be expected. India was the most common country, with populations within
India investigated in 12 studies. Populations in Turkey were only highlighted in 3 of the studies. This was
unexpected due to Turkey’s recognition by the WHO for achieving the highest standard in all six
MPOWER strategies. However, due to the strong governmental focus in Turkey, the government may be
being carrying out their own studies and programs, but are not reporting the results in the literature. Six
studies detailed interventions in Korea, including a country-wide tobacco prevalence and surveillance
survey. This result shows that despite not signing the CFTC, the country is still implementing
broad-based strategies to address the tobacco epidemic.
The overwhelming most common strategy that was addressed in Tier 1 was monitoring. The
majority of these studies established prevalence rates in relation to various determinants of health. This is
likely due to the fact that all four countries have all started to monitor tobacco use in youth on a country
level (Eriksen et al., 2012). Many of these studies detailed various analyses from these government
implemented surveys. Differences in prevalence of tobacco use were noted across countries. A study in
Argentina was the only one that discussed hand-rolled cigarettes and pipe tobacco (Alderete,
Kaplan, Gregorich, & Pérez-Stable, 2010). This could suggest that this use is more common in
Argentina or it could be because the study was conducted in indigenous populations that are
likely to be poorer and only have access to this type of product. It is unclear from the results of this
review if this would be true of indigenous populations in other countries. Several of the studies
35 Many of the studies in Tier 1 identified various determinants at all levels of the ecological model
that affect tobacco use among adolescent girls. Protective factors include high self-efficacy, knowledge
regarding the risks of tobacco use, and strong family norms opposing tobacco use. Common factors
identified that contribute to tobacco use are inadequate stress management, peer influence, low level
education of parent, smoking parent, and low socioeconomic status. Interesting to note, Jayakrishnan et
al. (2011) showed that girls were more aware of the risks of tobacco use. However, Mukherjee et al.
(2012) demonstrated conflicting results regarding risks of addiction, fetal harm, and exposure to
secondhand smoke.
Several of the studies addressed TAPS, cessation, and secondhand smoke. As suspected from the
literature review, the studies in this review show that TAPS influences tobacco use in this population.
Owning a branded tobacco item or witnessing tobacco use in movies was found to be associated with
higher levels of tobacco use. However, one study in Argentina demonstrated that high media literacy may
counteract the effect of TAPS activities (Salgado et al., 2011), but no data was available regarding this
factor and girls. Cessation and secondhand smoke with were also strategies found in the studies in this
review. A study in Korea demonstrated the usefulness of a national Quitline (Lim et al., 2012), while also
providing useful information on the role family members play in helping adolescents to quit smoking.
The study found that re-initiation of tobacco use was more likely in adolescents with a family member as
a quit supporter. The studies showed that exposure to secondhand smoke occurred at home and in schools
associated with higher poverty levels.
Several of the Tier 1 studies did not provide adequate data for adolescent girls beyond the basic
demographic data of the study. Das et al. (2011) did not have sufficient number of female study
participants to include a breakdown of results based on gender. Other studies presented results that were
adjusted for gender differences in the study populations.
The qualitative studies in Tier 3 did not provide reliable data for this discussion. However, the
two articles in Tier 3 that provided further analysis of a randomized controlled trial of prevention program
36 articles provided the best evidence and analysis found in this review to guide future programs
implemented at the school level, including important information on the results of the intervention among
adolescent females in India. The prevention program consisted of behavioral classroom curricula, school
posters, a parental involvement component, and peer-led activism. The program demonstrated success;
the intervention group were significantly less likely than were students in the control group to exhibit
increases in cigarette smoking or bidi smoking over the 2-year study period. Members of the intervention
group were also less likely to intend to smoke or chew tobacco in the future. The mediation analysis of
the study included in Tier 3 identified protective factors to tobacco use common to other articles found in
this systematic review. These factors provide the groundwork for identifying effective strategies aimed at
preventing and stopping tobacco use in this population at risk, adolescent females.
Limitations of Results
Limitations are associated with any research, including systematic reviews. The most obvious is
that the search was limited to recent timeframe, which may have excluded previous programs that might
have been efficacious prior to 2010. Another likely limitation is that the search results were not checked
by a third party. This may have caused errors in the categorization of studies, along with an error in the
original number of studies to be included in the review. However, due to the relatively small number of
studies found for this specific population and the heterogeneous nature of the data extracted, this likely
would not have had a major effect on the overall results of the review. The number of studies found may
have been low because of the social status of females in these countries. Although the status of women
and girls is on the rise in most countries, there could be a lag time between when this is demonstrated in
research and study protocols. In addition, progress in the status of women is not the same across all low-
and middle-income countries, including those countries chosen for this systematic review. The finding of
primarily descriptive studies is associated with its own limitations. These types of studies have limited
37 CONCLUSION/RECOMMENDATION
Findings in this review support several recommendations. First, more studies of all types
need to be completed to determine how to best tackle this epidemic in adolescent females. The
results of this systematic review show that the public health community is in the beginning
stages of addressing this issue, as evidenced by the majority of studies attempting to identify the
various determinants affecting tobacco use. Although common factors were identified here, more
published descriptive studies are necessary to help identify the most relevant factors contributing
to or preventing tobacco use in this population at all levels of the ecological model. Once the
relevant factors are established, analytical studies should be designed that investigate specific
interventions focused on these factors. An increase in the published research of any tobacco
control programs implemented at the community level is also required, regardless of the
enactment of country-wide policies or whether the program is implemented by the private or
government sector. Finally, this review identified one specific intervention program, Project
MYRTI, which can provide a starting point for developing successful programs aimed at
38 REFERENCES
Alderete, E., Monteban, M., Gregorich, S., Kaplan, C., Mejia, R., & Perez-Stable, E. 2012. Smoking and exposure to racial insults among multiethnic youth in Jujuy, Argentina. Cancer Causes & Control, 23(1), 37-44. Retrieved from
http://link.springer.com/article/10.1007%2Fs10552-012-9906-0
Alderete, E., Erickson, P., Kaplan, C., & Pérez-Stable, E. 2010. Ceremonial tobacco use in the Andes: implications for smoking prevention among indigenous youth. Anthropology & Medicine, 17(1), 27-39. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2863150/
Alderete, E., Kaplan, C., Gregorich, C., & Pérez-Stable E. 2010. Use of alternative tobacco products in multiethnic youth from Jujuy, Argentina. Journal of Environmental Public
Health. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2841245/
American Cancer Society, Inc. 2009. Tobacco use in India: an evil with many faces. Retrieved from http://www.cpaaindia.org/infocentre/acs/eng/Tobacco%20Abuse.pdf.
Arora M, Tewari, A., Dhavan, P., Nazar, G., Stigler, M., Juneja, N., Perry, C., & Reddy, K. 2013. Discussions with adults and youth to inform the development of a community-based tobacco control programme. Health Education Research, 28(1), 58-71. Retrieved from http://her.oxfordjournals.org/content/28/1/58.long
Arora, M., Mathur, N., Gupta, V., Nazar, P., Reddy, S., & Sargent, D. 2012. Tobacco use in Bollywood movies, tobacco promotional activities and their association with tobacco use among Indian adolescents. Tobacco Control, 21, 482-487. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3420563/
Bhojani, U., Elias, M., & Devadasan, N. 2011. Adolescents’ perceptions about smokers in Karnataka, India. BMC Public Health, 11:563. Retrieved from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3150267/
Chun J. & Chung, I. 2013. Gender differences in factors influencing smoking, drinking, and their co-occurrence among adolescents in South Korea. Nicotine & Tobacco Research, 15(2), 542-551. Retrieved from http://ntr.oxfordjournals.org/content/15/2/542.long
Das, S., Ghosh, M., Sarkar, M., Joardar, S., Chatterjee, R., & Chatterjee, S. 2011. Adolescents speak: why do we smoke? Journal of Tropical Pediatrics, 57(6), 476-48 0. Retrieved from http://tropej.oxfordjournals.org.libproxy.lib.unc.edu/content/57/6/476.full
39 Eriksen, M., Mackay, J., Ross, H. 2012. The tobacco atlas. Atlanta, Georgia: American Cancer
Society, Inc.
Goenka, S., Tewari, A., Arora, M., Stigler, M., Perry, C., Arnold, S., Kulathinal, S., & Reddy, K. 2010. Process evaluation of a tobacco prevention program in Indian schools—methods, results and lessons learnt. Health Education Research, 25(6), 917–935. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3003490/
Golbasi, Z., Kaya, D., Cetindag, A., Capik, E., & Aydogan, S. 2011. Smoking Prevalence and Associated Attitudes among High School Students in Turkey. Asian Pacific Journal of Cancer Prevention, 12, 1313-1316. Retrieved from
http://www.apocpcontrol.org/page/apjcp_issues_view.php?sid=Entrez:PubMed&id=pmid :21875288&key=2011.12.5.1313
Hong, N., Kim, Ke., Park, S., Kim, J., Bae, J., Lee, W., & Kim Ki. 2011. Trends in cigarette use behaviors among adolescents by region in Korea.Journal of Preventive Medicine & Public Health, 44(4), 176–184. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3249254/
Institute of Medicine. 2003. Who will keep the public healthy? Health professionals for the 21st century. Washington, DC: The National Academies Press.
Institute of Medicine. 2002. The future of the public’s health in the 21st century. Washington, DC: The National Academies Press.
Jayakrishnan, R., Geetha, S., Binukumar, B., Sreekumar, & Lekshmi K. 2011. Self-reported tobacco use, knowledge on tobacco legislation and tobacco hazards among adolescents in rural Kerala State. Indian Journal of Dental Research, 22, 195-9. Retrieved
from http://www.ijdr.in/text.asp?2011/22/2/195/84280.
Jung, M. & Chung, D. 2013. Evidence of social contextual effects on adolescent smoking in South Korea. Asia Pacific Journal of Public Health, 25(3), 260-270. Retrieved from
http://aph.sagepub.com/content/early/2012/10/08/1010539512461667
Kim, J., Lee, C., Lim, E., & Kim, G. 2013. Smoking cessation and characteristics of success and failure among female high-school smokers. Japan Journal of Nursing Science, 10(1), 68-78.
Lee, S., Yun, J., Lee, J., 2 Kim, I., & Jee, S. 2010. The Korean prediction model for adolescents' future smoking intentions. Journal of Preventive Medicine & Public Health, 43(4), 83– 291. Retrieved from http://jpmph.org/DOIx.php?id=10.3961/jpmph.2010.43.4.283
40 342-345. Retrieved from
http://www.sciencedirect.com/science/article/pii/S0306460311003698
Linetzky, B., Mejia, R., Ferrante, D., De Maio, F. & Diez Roux, A. 2012. Socioeconomic status and tobacco consumption among adolescents: a multilevel analysis of Argentina’s Global Youth Tobacco Survey. Nicotine & Tobacco Research, 14(9), 1092-1099. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3529606/
Mejia R., Kaplan C, Alderete, E., Gregorich, S., & Pérez-Stable, E. 2013. Influence of gender role attitudes on smoking and drinking among girls from Jujuy, Argentina. Preventive Medicine, 57(3), 194-197. Retrieved from
http://www.sciencedirect.com/science/article/pii/S0091743513001746
Mukherjee, A., Sinha, A., Taraphdar, P., Basu, G., & Chakrabarty, D. 2012. Tobacco abuse among school going adolescents in a rural area of West Bengal, India. Indian Journal of Public Health, 56, 286-9. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/23354139
NBCnews. 2010. FDA compares dissolvable tobacco to candy. Accessed at:
http://www.nbcnews.com/id/35255473/ns/health-addictions/t/fda-compares-dissolvable-tobacco-candy/.
Ortabag, T., Ozdemir, S., Bakir, B., & Tosun, B. 2011.Health promotion and risk behaviors among adolescents in Turkey. The Journal of School Nursing, 27, 304-315.
Page, R., Park, S., Suwanteerangkul, J., Park, H., Kemeny, M. & Philips, L. 2012. Cross-cultural analysis of cognitive attributions of smoking in Thai and South Korean adolescents. Journal of School Health, 82(2), 57-64.
Philip. P., Parambil, N., Bhaskarapillai, B., & Balasubramanian, S. 2013. Evaluation of a
specially designed tobacco control program to reduce tobacco use among school children in Kerala. Asian Pacific Journal of Cancer Prevention, 14, 3455-3459. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/23886127
Public Health Leadership Society. 2002. Principles of the ethical practice of public health. Retrieved from http://phls.org/CMSuploads/Principles-of-the-Ethical-Practice-of-PH-Version-2.2-68496.pdf.
Ruderman, M. 2013. An introduction to the ecological model in public health. [Powerpoint slides] Retrieved from http://www.jhsph.edu/research/centers-and-institutes/womens-and-childrens-health-policy-center/eco-model/Transcript-Ecological-Model.pdf