0095-1137/95/$04.0010
Copyrightq1995, American Society for Microbiology
Monitoring Levels of Human Cytomegalovirus DNA
in Blood after Liver Transplantation
EMMANUEL DROUET,1* RONALD COLIMON,2SUSAN MICHELSON,3NADINE FOURCADE,4
ALAIN NIVELEAU,1,5CHRISTIAN DUCERF,4ANDRE´ BOIBIEUX,6
MICHE` LE CHEVALLIER,5
ANDGE´ RARD DENOYEL1
Unite´ d’Infectiologie, Institut Pasteur de Lyon, 69365 Lyon, Cedex 07,1Laboratoire de Virologie, Hoˆpital Pontchaillou,
350336 Rennes Ce´dex,2Unite´ d’Immunologie Virale, Institut Pasteur, 75015 Paris,3Service de Chirurgie Digestive et
Unite´ de Transplantation4and Service des Maladies Infectieuses et Tropicales,6Hoˆpital de la Croix-Rousse, 69317
Lyon, Cedex 04, and De´partement de Pathologie Cellulaire, Institut Pasteur de Lyon, Lyon, Ce´dex 07,5France
Received 11 April 1994/Returned for modification 7 June 1994/Accepted 26 October 1994
We evaluated a semiquantitative PCR assay prospectively in 40 liver transplant recipients as an aid in making a prompt diagnosis of cytomegalovirus (CMV) infection. For 2 months after transplantation, clinical specimens from patients were tested weekly by PCR, virus isolation from peripheral blood and urine, and CMV serology. The incidence of active CMV infection was 70%. The levels of CMV DNA determined by hybridization of PCR samples and densitometric scanning of blots were assigned a score of 1 to 4 by comparison with four external standards amplified in parallel and corresponding to a range of 80 to 80,000 genomes. The first detection of CMV in blood by PCR occurred at a mean of 15 days, and high-level PCR scores of 3 or 4 were obtained 21 days after transplantation, whereas viremia occurred 33 days after transplantation. Significantly higher levels of CMV DNA were seen in patients with CMV disease (P< 0.05) than in asymptomatic patients. The prevalence of symptomatic CMV infection was 30%. The positive predictive value of PCR was 48%, while the negative predictive value was 100%. After treatment, the clearance of CMV DNA was always observed and the disappearance of symptoms occurred concomitantly with undetectable PCR signals.
Cytomegalovirus (CMV) has been shown to be an important pathogen in liver transplant recipients (for a review, see refer-ence 5), and active CMV infection occurs in 20 to 60% of all patients. Most studies report a 60 to 80% incidence of infec-tion, and such an infection is associated with considerable morbidity (5, 19). Since CMV disease occurs early after trans-plantation and can be related to well-defined risk factors (21), investigation of prophylactic strategies is warranted to reduce the incidence and severity of CMV disease after liver grafting. Antiviral therapy with ganciclovir, which suppresses CMV rep-lication and improves the outcome of CMV disease (14), has increased the need for early diagnosis. CMV viremia is con-sidered the best predictor of CMV disease in transplant recip-ients and is a reliable marker for initiating antiviral treatment to prevent the progression of infection to a severe form of the disease (12). The rapidity of diagnosis of CMV infection can be further improved by demonstrating the presence of viral anti-gens (22) or viral nucleic acids (17) in peripheral blood leuko-cytes (PBLs). PCR has been shown to be a reliable procedure for detecting CMV DNA in blood (2), monitoring CMV in-fections and disease (7) in transplant recipients, and under-standing CMV pathogenesis (6), but its value as a predictor of CMV infection and disease has been questioned because of the lack of PCR quantitation.
In the prospective study described here, we evaluated a semiquantitative PCR (4) for detecting CMV DNA in PBLs from liver transplant recipients. This technique was also eval-uated as a means of providing an early diagnosis, allowing prompt therapeutic intervention in the course of disease.
MATERIALS AND METHODS
Patients.Between April 1990 and April 1992, 68 consecutive patients (ages, between 15 and 67 years; mean age, 44.9 years) received liver transplants at the Hoˆpital de la Croix-Rousse in Lyon, France. Twenty-eight of these patients were excluded from the study because of death unrelated to CMV within 3 weeks after transplantation or because of incomplete documentation. The causes of incom-plete documentation were as follows: (i) data were missing from several clinical files (X rays, temperature curves, associated infections), (ii) too few samples were obtained, and (iii) there were gaps in the follow-up of patients. The 40 remaining patients were followed up for 2 months, with blood and urine samples being taken every 5 days for the first 2 months and then every 15 days during a subsequent 2-month follow-up. Immunosuppressive therapy consisted of pred-nisolone, azathioprine, and cyclosporine A. No patients received second trans-plantations during follow-up. CMV-seronegative patients grafted with liver from seropositive donors received per-operative anti-CMV immunoglobulins (CMV Ig’s; 30,000 units) and intravenous acyclovir (800 mg every 8 h for 6 days, depending on renal function) and then high-dose oral acyclovir (3,200 mg/day for 3 months) prophylaxis. Rejection episodes were documented by percutaneous liver biopsy and were treated with methylprednisolone or with anti-OKT3 mono-clonal antibody in cases of severe rejection. CMV antibody status was deter-mined in all recipients and, whenever possible, in the transplant donor before transplantation.
Technical procedures.All technical procedures have been described previ-ously in detail (4) and are given here only briefly.
(i) PBL sampling.Five-milliliter samples of heparinized blood were obtained from each patient, and the PBLs were separated by the dextran method. They were then washed in minimum essential medium supplemented with 2% fetal calf serum and counted.
(ii) Virus isolation.Virus isolation from PBLs and urine was performed by two methods: the conventional tube culture method and isolation by centrifugation (1,0003g for 10 min at 48C) into 24-well, flat-bottom culture plates (8). Foci were detected with monoclonal antibody E13 (Clonatec, Paris, France) directed against CMV immediate-early antigens by indirect immunofluorescence (9).
(iii) Primers and Southern blot hybridization probe.Two 25-base primers (upstream primer, 59-GGA TCC GCA TGG CAT TCA CGT ATG T-39; down-stream primer, 59-GAA TTC AGT GGA TAA CCT GCG GCG A-39) were synthesized. These primers frame a 406-bp region delimited by BamHI and EcoRI restriction sites within the HindIII-X fragment (noncoding region in the USfragment of the CMV genome).
(iv) PCR assay.Samples of PBLs for PCR analysis were suspended at a concentration of approximately 1,000 cells perml in PCR buffer (50 mM KCl, 10 mM Tris-HCl [pH 8.4], 2.5 mM MgCl2) with nonionic detergent (0.5% Tween 20) and proteinase K (100mg/ml; Boehringer, Mannheim, Germany) (10). Ali-* Corresponding author. Mailing address: Service de Bacte´riologie
et Virologie, Faculte´ de Pharmacie de Grenoble, 38706 La Tronche Cedex, France. Phone: (33) 76 63 71 00. Fax: (33) 76 51 86 67.
389
on May 15, 2020 by guest
http://jcm.asm.org/
quots (10ml) of each PBL sample were subjected to DNA amplification in 100 ml of reaction buffer (10) for 30 cycles (reaction times were 1 min at 558C for annealing, 1 min at 728C for primer extension, and 30 s at 958C for denaturation). The following measures were taken to ensure the validity of the results. (i) The precautions taken to avoid carryover of the PCR product included physical separation of the pre-PCR and post-PCR mixtures, the use of positive-displace-ment pipettes, and the avoidance of aerosols (11). (ii) Contamination by plas-mids containing the CMV insert was excluded. (iii) Negative controls, including leukocyte DNA samples as well as a reaction mixture without DNA, were run in each experiment. (iv) Amplification in parallel of a beta-globin gene (16) in patient leukocyte DNA was used to control for amplification inhibitors in the samples.
(v) Analysis of the PCR products.Aliquots (10ml) of each PCR-amplified product were electrophoresed in agarose, transferred to nylon membranes (Hy-bond N1; Amersham International, Amersham, United Kingdom) by the South-ern technique, and hybridized by using an intSouth-ernal probe as described previously (4). As a control of internal consistency and for semiquantitative analysis of the PCR product, six reference standards were included in each PCR experiment. These standards were prepared by adding known amounts of purified CMV AD169 DNA (equivalent to approximately 0.8 to 80,000 CMV genomic copies) to DNAs from 104
MRC-5 cells. For objective evaluation, Southern blots were analyzed on a computer image processing system specifically designed for den-sitometric measurement (Biocom 200; Biocom, Les Ulis, France). The specific band resulting from each PCR-positive specimen was assigned a score of 1 to 4 on the basis of the band’s intensity compared with four points on the standard curve of dilutions: 80, 800, 8,000, and 80,000 CMV genomic copies, respectively. The absence of inhibitors, which could eventually interfere with the PCR, was ascertained by adding small amounts of CMV DNA (80 genomic copies) to PBL lysates from PCR-negative individuals. Scores of 1 and 2 were designated low level, and those of 3 and 4 were designated high level. Technical assistants processed the specimens blinded with respect to culture and patient information. The time delay before hybridization results were obtained was about 30 h. For high levels of CMV DNA in blood, inspection of the ethidium bromide-stained gel yielded results in about 5 h.
(vi) Serology.CMV serology was performed by two techniques: (i) Comple-ment fixation and (ii) solid-phase enzyme-linked immunosorbent assay (ELISA) for IgG and IgM (Vironostika anti-CMV; Organon Teknika, Boxtel, The Neth-erlands). Quantification of IgG by ELISA was performed by the limiting dilution technique. Serum samples with IgG titers of,100 were considered negative.
Definitions. (i) Seroconversion.Seroconversion was defined as a fourfold or greater rise in CMV antibody titer.
(ii) Active CMV infection.Active CMV infection was defined when CMV was isolated by culture from a body fluid specimen (blood, bronchoalveolar lavage, urine) or by seroconversion or the presence of CMV-specific IgM. Active infec-tion in an initially seronegative patient was considered a primary infecinfec-tion. When it occurred in a seropositive patient, it was designated non-primary infection, meaning either reactivation of endogenous CMV or a new infection in a previ-ously CMV-immune host.
(iii) Symptomatic CMV infection and CMV syndrome.CMV infection was considered symptomatic (designated ‘‘CMV disease’’) when active infection oc-curred in association with clinical symptoms. CMV syndrome was defined as a CMV infection associated with fever of unknown origin of.38.58C for more than 5 days, leukopenia of,2,000/mm3
, or thrombocytopenia of,100,000/mm3 .
(iv) CMV hepatitis.CMV hepatitis was considered when CMV was detected by culture in liver tissue or when typical CMV inclusion bodies were detected with or without inflammation in a liver tissue specimen; if any liver function abnormalities (increase of.30% in aspartate aminotransferase, alanine amino-transferase, alkaline phosphatase, gammaglutamylamino-transferase, or bilirubin levels) occurred on 2 consecutive days or if there was a response to anti-CMV therapy (this corresponds to an improvement in liver functions after ganciclovir treat-ment after other causes of hepatitis, such as a relapse of hepatitis C virus infection, were excluded).
(v) CMV pneumonitis.CMV pneumonitis was defined as a respiratory syn-drome with dyspnea, tachypnea, hypoxia, and pulmonary infiltrates on chest radiographs as well as isolation of CMV from bronchoalveolar lavage specimens and exclusion of infection with another pathogen. In all patients, alternative causes of symptoms were excluded by appropriate cultures, serology, and echog-raphy. Additional radiologic procedures and biopsies were done if necessary.
Therapy.Ganciclovir was administered at 5 mg/kg of body weight twice daily only to patients with CMV disease.
Statistics.Sensitivity was determined by dividing the number of patients with CMV infection and a PCR score of 3 or 4 by the total number of patients with CMV infection. Specificity was determined by dividing the number of patients without CMV infection who had PCR scores of 0 to 2 by the total number of patients without CMV infection. Statistical studies were performed by the Exact Trend Test (Jonckheere-Terpstra [JT] test) with the Mehta algorithm (2a). Student’s t test was used for statistical comparisons of symptomatic and asymp-tomatic patients. A probability of,0.05 was considered statistically significant.
RESULTS
General outcome. Table 1 summarizes the biological fea-tures and the clinical data for the 40 liver transplant recipients. During the first 2 months after transplantation CMV infection occurred in 28 patients (70%; 22 with a significant increase in CMV antibodies and 6 with seroconversion). In the patients with symptomatic and asymptomatic CMV infection, the mean times to seroconversion or a significant increase in CMV an-tibodies were 47.1 days (range, 25 to 55 days) and 48.1 days (range, 40 to 60 days) postransplantation, respectively.
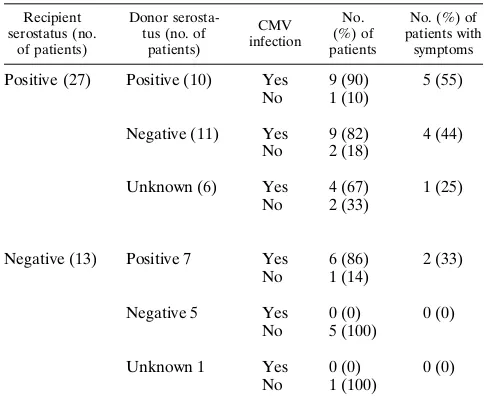
[image:2.612.314.555.93.526.2]The occurrence of CMV infection according to the CMV antibody status of the liver donor and recipient is summarized
TABLE 1. Biological features of and clinical data for the 40 liver recipients
Group and patient no.
Donor/recipient
CMV status Symptom(s)
a CMV
antibodyb Isolationc
Group I
1 1/1 CS SI, IgM B
2 1/1 AR, P SI B, BAL
3 1/2 P SC, IgM B, BAL
4 2/1 P SI B, BAL
5 1/1 AR, H SI U, (L)
6 1/1 H SI U, (L)
7 2/1 AR, P SI B, BAL
8 1/1 CS SI, IgM B
9 2/1 CS SI, IgM B
10 2/1 CS SI B
11 ?/2 CS SC, IgM B
12 ?/1 P SI U, BAL
Group II
13 1/1 a SI, IgM U
14 ?/1 a SI U (2)
15 1/2 a SC, IgM U
16 1/1 a SI U
17 2/1 a SI, IgM U (2)
18 2/1 a SI U
19 ?/1 a SI U (3)
20 2/1 a SI U (3)
21 1/2 a SC, IgM U
22 2/1 a SI U
23 1/1 AR, a SI U
24 ?/1 a SI, IgM U (2), B
25 1/2 a SC, IgM U (2)
26 2/1 a SI, IgM U
27 1/1 a SI U (2)
28 1/2 a SC, IgM U
Group III
29 2/2 n Neg Neg
30 2/2 n Neg Neg
31 2/1 n Pos Neg
32 1/2 n Neg Neg
33 2/2 n Neg Neg
34 ?/2 n Neg Neg
35 2/2 n Neg Neg
36 1/1 n Pos Neg
37 2/2 n Neg Neg
38 ?/1 n Pos Neg
39 ?/1 n Pos Neg
40 2/1 n Pos Neg
a
Abbreviations: CS, CMV syndrome; AR, acute rejection; P, pneumonitis; H, hepatitis; a, asymptomatic; n, uninfected.
b
Serology results: SI, significant increase; SC, seroconversion; Neg, CMV seronegative; Pos, CMV seropositive.
c
Abbreviations: B, peripheral blood leukocytes; BAL, bronchoalveolar lavage; U, urine; L, liver. Numbers in parentheses indicate the number of times that CMV was isolated from the indicated specimen.
on May 15, 2020 by guest
http://jcm.asm.org/
in Table 2. The overall rate of infection in patients without acyclovir treatment was 79% (22 of 28), of whom 45% (10 of 22) were symptomatic.
The levels of CMV DNA in patients with symptomatic CMV infection (group I) (Fig. 1A) were assessed. CMV DNA was detected in the blood of all patients in this group. On the basis of the day of transplantation, positive PCR results appeared at a mean of 15 days (range, 5 to 25 days) and reached levels of 3 to 4 at a mean of 21.6 days after transplantation (range, 10 to 40 days), whereas viremia was detected at a median of 33 days (range, 20 to 45 days) after transplantation. The mean duration of CMV DNA in blood in this group was 29.6 days (range, 5 to 45 days), and the mean duration of high-level CMV DNA in blood was 17.9 days (range, 5 to 40 days). All patients were treated with ganciclovir at a mean of 2.9 days (range, 0 to 15 days) after the clinical onset of CMV infection. This resulted in low-level or zero-level CMV DNA in blood at a mean of 7.7 days (range, 5 to 15 days) after the beginning of treatment. All patients except patient 7 recovered from CMV disease; patient 7 died of pneumonitis (Fig. 2A and B).
The levels of CMV DNA in patients with asymptomatic CMV infection (group II) (Fig. 1B) were assessed. CMV DNA was detected in the blood of all 16 patients at a mean of 15.9 days (range, 5 to 30 days) after transplantation. Moderate (level 3) or high (level 4) CMV DNA levels were observed in 12 patients at a mean of 21.2 days (range, 15 to 30 days) after transplantation. In this group, the levels of CMV DNA in blood decreased spontaneously without treatment. CMV DNA at levels 3 and 4, when present, persisted for,15 days except in six patients (patients 13, 15, 19, 21, 22, and 24), in whom it persisted at a high level for a mean of 18.3 days (range, 15 to 30 days) before decreasing spontaneously without antiviral treatment. Among these six patients, patients 21, 22, and 24 experienced hepatitis 4 to 5 months after transplantation. Nei-ther viremia, CMV DNA in blood, nor viral inclusions were detected during the episodes of hepatitis. Nevertheless, ganci-clovir therapy was administered, which improved symptom-atology, and liver enzyme levels returned to normal. PCR performed retrospectively on embedded liver tissue sections from these patients yielded positive results. Other causes of liver dysfunction were excluded.
The levels of CMV DNA in the blood of patients without CMV infection (group III) (Table 1) were assessed. In this group, 104 of 116 samples (89.7% of samples) were PCR neg-ative and 10 of 116 (8.6%) had CMV DNA at a low level (PCR level 1 to 2). Only patient 32 exhibited CMV DNA at PCR level 3 (two samples), which returned spontaneously to level 0 within 5 days.
PCR levels in symptomatic versus asymptomatic patients.
[image:3.612.334.523.66.538.2]For each follow-up time, an average PCR score was calculated by summing the PCR levels and dividing them by the number of patients tested at that time point. Of the 28 patients who FIG. 1. (A) PCR follow-up of liver transplant recipients with CMV disease. (B) PCR follow-up of liver transplant recipients with asymptomatic CMV infec-tion. (C) PCR follow-up of liver transplant recipients without CMV infecinfec-tion. Patients are identified by numbers on the y axis. Solid boxes, PCR level 4; hatched boxes (3), PCR level 3; hatched boxes (1), PCR level 2; open boxes, PCR level 1; horizontal line, PCR level 0; no symbol, missing data; D (patient 7), deceased.
TABLE 2. CMV infection and disease relative to donor and recipient serostatus
Recipient serostatus (no.
of patients)
Donor serosta-tus (no. of
patients)
CMV infection
No. (%) of patients
No. (%) of patients with
symptoms
Positive (27) Positive (10) Yes 9 (90) 5 (55) No 1 (10)
Negative (11) Yes 9 (82) 4 (44) No 2 (18)
Unknown (6) Yes 4 (67) 1 (25) No 2 (33)
Negative (13) Positive 7 Yes 6 (86) 2 (33) No 1 (14)
Negative 5 Yes 0 (0) 0 (0)
No 5 (100)
Unknown 1 Yes 0 (0) 0 (0)
No 1 (100)
on May 15, 2020 by guest
http://jcm.asm.org/
[image:3.612.56.298.91.291.2]experienced CMV infection, the average PCR score peaked at a higher level for the 12 symptomatic patients than for the 16 asymptomatic patients (t52.60; P,0.05). If we assume that all symptomatic patients received adequate ganciclovir ther-apy, the slope of decreasing PCR scores after the peak was significantly steeper for treated patients compared with that for untreated patients (t52.85; P,0.05).
The sensitivity of high-level PCR scores was 89% and the specificity was 91%. In the population studied, the positive predictive value of the test for CMV infection was 96% and the negative predictive value was 91% [JT (3) 5 25.224; P , 0.0001]. If we consider only the occurrence of CMV disease, the positive predictive value was 48% and the negative predic-tive value was 100%.
DISCUSSION
CMV disease occurred in only 15% (2 of 13) of the CMV-seronegative recipients, which is in contrast to an incidence of CMV disease of 88% in a previous study (19). Such a discrep-ancy could be explained by our systematic use of antiviral prophylaxis with acyclovir in our seronegative recipients re-ceiving a liver from a CMV-seropositive donor. In a recent study (13), the frequency of CMV infection after liver trans-plantation was apparently reduced by high-dose oral acyclovir, since all patients not receiving such treatment had CMV in-fection, whereas only 57% of those who received acyclovir had CMV infection. Thus, it appears that acyclovir prophylaxis was unable to reduce the incidence of CMV infection in
seroneg-ative recipients, but it did decrease the occurrence of clinical disease. The lower level of CMV infection reported in another study (13) might be attributed to the additive prophylactic effect of CMV Ig, which was prolonged for 6 weeks from the day of transplantation, whereas only high-risk patients received per-operative CMV Ig. As reported by others (5, 19), we noted no difference in the clinical symptoms stemming from primary or secondary infections.
In a prospective study establishing the incidence of risk factors for and outcomes of CMV hepatitis after liver trans-plantation, Paya et al. (15) found that hepatitis occurred fre-quently in 26% of patients with CMV infection and 46% of those with CMV disease. The incidence was higher in CMV-seronegative recipients of a liver from a CMV-seropositive donor (21). In our survey, early liver involvement was markedly lower, since only two cases of posttransplantation CMV hep-atitis were observed during the first 2 months posttransplanta-tion. This deserves further evaluation in a larger group of patients, taking into consideration the incidence of retrans-plantation, since it appears to be a risk factor for CMV hepa-titis (15). Three of our patients had late liver dysfunction after an episode of CMV infection. Liver tissue examination failed to show histologic evidence of hepatitis. However, CMV DNA was detected in paraffin-embedded liver biopsy specimens. In all three cases, ganciclovir treatment was effective, raising the possibility that CMV was involved in the hepatitis. One study (15) reported that liver dysfunction occurred but that CMV could not be isolated from biopsy specimens and there was an absence of a typical histopathological picture of CMV hepati-tis. Detection of CMV DNA in liver tissue by PCR might be an accurate method of diagnosing CMV hepatitis, as recently reported for posttransplantation hepatitis (23). In the future in situ DNA amplification could be used to resolve the difficulty of using PCR to diagnose CMV hepatitis. This technique could provide new data concerning the localization of CMV at the cellular level (macrophages or hepatocytes). Furthermore, si-lent CMV infection with spontaneous resolution of a high viral load might constitute a risk factor for late CMV-related liver dysfunction, prompting a search for DNA in the liver allograft. All studies of transplant recipients agree that CMV disease is the major source of clinical complications, which underlines the need for careful virologic monitoring of CMV infection in these patients. Gerna et al. (7) found that early detection of CMV DNA by PCR was of poor clinical significance in heart transplant patients and that low DNA levels were often non-progressive. They argued that an important drawback of PCR was the lack of precise quantitation and that, consequently, this technique did not provide accurate data for the initiation of therapy. Other investigators (3) found that all viremia-positive patients were PCR positive, including those who did not de-velop CMV disease. It was concluded that while PCR is a very sensitive technique, it has a low positive predictive value (25%) for symptomatic infection. Our preliminary results (data not shown) obtained by nonquantitative PCR were in agreement with the aforementioned conclusions. We therefore focused our attention on the semiquantitative detection of the CMV DNA load by a technique that entailed the careful standard-ization of technical steps and that introduced an external stan-dard in all series so that the signals generated could be eval-uated against a given number of genomic copies (4). Although arbitrarily chosen, these indicators seemed functional for mon-itoring CMV infections (4).
Examination of PCR results for our transplant recipients showed that all patients with CMV infection experienced high, protracted CMV DNA levels, whereas uninfected patients demonstrated intermittent, transient low or moderate levels of FIG. 2. (A) Clearance of CMV DNA from blood after ganciclovir therapy in
patients experiencing CMV disease (between 20 and 40 days posttransplanta-tion).E, patient 1;w, patient 2;ç, patient 7;h, patient 10;✽, patient 11. (B) Clearance of CMV DNA from blood after ganciclovir therapy in patients expe-riencing CMV disease (between 30 and 60 days posttransplantation).E, patient 3; å, patient 4;ç, patient 5;h, patient 6;✽, patient 8;w, patient 9; ◗, patient 12.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:4.612.88.266.68.359.2]CMV DNA in their blood. Since patients were examined at regular intervals posttransplantation, we considered that cal-culation of an average PCR score by vertical addition of the DNA levels observed in each group of patients would be a useful way to evaluate the performance of DNA detection by PCR. We found that scores peaked at a significantly (P,0.05) higher level in symptomatic than in asymptomatic, infected patients. The positive predictive value of high PCR levels for CMV disease appeared to be moderate (48%), but detection of a high level of CMV DNA in blood occurred, on average, 12 days earlier than viremia. Hence, although CMV DNA in blood was detected in the absence of clinical evidence of in-fection, high and protracted PCR levels were considered to be an early warning of potential CMV disease. Since in some cases the immune system is unable to cope with acute viral infection, we believe that high PCR signals for CMV DNA might prompt closer clinical monitoring and the early institu-tion of suitable therapy.
In all but one of the infected patients, CMV DNA levels decreased, until they reached zero. As demonstrated by the slopes of decreasing PCR scores, institution of ganciclovir treatment significantly accelerated the decrease in CMV DNA levels in treated patients compared with those in infected pa-tients who overcame their disseminated CMV infection with-out overt disease. An exception was noted for patient 7, in whom CMV DNA levels decreased and then increased despite ganciclovir treatment, until fatal pneumonitis occurred. This case might have been due to a ganciclovir-resistant mutant strain of CMV. Although the occurrence of such mutants ap-peared to be low in organ transplant recipients (1), long-term prophylaxis of such patients with ganciclovir might lead to a higher level of selection of resistant mutants. Thus, prophylaxis might be restricted to patients with an early, high viral load, whatever the CMV status of the donor or the recipient, in light of the high level of morbidity in patients with secondary infec-tion.
In conclusion, semiquantitative PCR, because of its high degree of sensitivity, could provide the first warning signal of CMV infection since it detects the viral load before other techniques do. Anti-CMV drugs, especially ganciclovir, may have serious side effects. The PCR assay for CMV DNA may therefore be valuable in reducing the number of unnecessarily treated patients without increasing the number of patients who develop severe CMV disease. Positivity by PCR could select patients at high risk of CMV disease who could then be mon-itored precisely. In the present report, high PCR levels were shown to have an excellent negative predictive value (100%) for the development of disease, as was demonstrated by others (18). Consequently, the risk of overlooking patients who need treatment is negligible. PCR performed on leukocytes is tech-nically difficult. However, it was recently shown (4, 20) that CMV DNA detection in serum or plasma correlated closely with viremia, high leukocyte viral load (4), and disease (20). The increase in the viral load with time, the kinetics of the increase, and the level that it reaches together with the steadi-ness of a high level provide useful information to clinicians. Today they are already taken into account in the design of therapeutic protocols. Experiments could be simplified by avoiding leukocyte separation or by developing an ELISA for-mat for the detection of the PCR product. In addition, PCR is adaptable to automation, thereby providing objective results as far as viral load is concerned. Finally, PCR can detect DNA in patients with localized infections (i.e., hepatic, gastrointestinal, and neurologic infections). Hence, we consider the PCR assay for CMV DNA to be a valuable tool with great promise for the early diagnosis and management of CMV disease in patients at
risk. Whatever methodology is applied, the quantification of the viral load which was applied here to CMV-associated disease can be extended to other viral infections associated with immunode-pression (acquired or induced). The use of truly quantitative techniques will allow clinicians to obtain more precise informa-tion on the state of the patients being monitored.
ACKNOWLEDGMENTS
We thank Pierre Estrabaud and Rene´ Ecochard for skillful assis-tance with the statistical part of the study and Wanda Be´al, Lucile Charpin, and Nadine Rozand for expert technical assistance.
REFERENCES
1. Boivin, G., A. Erice, D. D. Crane, D. L. Dunn, and H. Balfour. 1993. Gan-ciclovir susceptibilities of cytomegalovirus isolates from solid organ trans-plant recipients with CMV viremia after antiviral prophylaxis. J. Infect. Dis.
168:332–335.
2. Cassol, S. A., M. C. Poon, R. Pal, M. G. Naylor, J. Culver-James, and T. J.
Bowen.1989. Primer-mediated enzymatic amplification of cytomegalovirus DNA: application to the early diagnosis of CMV infection in marrow trans-plant recipients. J. Clin. Invest. 83:1109–1115.
2a.CYTEL Corporation. 1991. StatXact statistical software. CYTEL Corpora-tion, Cambridge, Mass.
3. Delgado, R., C. Lumbreras, C. Alba, M. A. Pedraza, J. R. Otero, R. Gomez,
E. Moreno, A. R. Noriega, and C. V. Paya.1992. Low predictive value of polymerase chain reaction for diagnosis of cytomegalovirus disease in liver transplant recipients. J. Clin. Microbiol. 30:1876–1878.
4. Drouet, E., S. Michelson, G. Denoyel, and R. Colimon. 1993. Polymerase chain reaction detection of HCMV in over 2000 blood specimens correlated with virus isolation and related to urinary virus excretion. J. Virol. Methods
45:259–276.
5. Dummer, J. S. 1990. Cytomegalovirus infection after liver transplantation: clinical manifestations and strategies for prevention. Rev. Infect. Dis. 12 (Suppl. 7):S767–S775.
6. Emery, V. 1993. Cytomegalovirus pathogenesis: applications of PCR, p. 209–218. In S. Michelson and S. A. Plotkin (ed.), Multidisciplinary approach to understanding cytomegalovirus disease. Elsevier Science Publishers B.V., Amsterdam.
7. Gerna, G., D. Zipeto, M. Parea, M. G. Revello, E. Silini, E. Percivalle, M.
Zavattoni, P. Grossi, and G. Milanesi.1991. Monitoring of human cytomeg-alovirus infection and ganciclovir treatment in heart transplant recipients by determination of viremia, antigenemia and DNAemia. J. Infect. Dis. 164: 488–498.
8. Gleaves, C. A., C. F. Lee, L. Kirsch, and J. D. Meyers. 1987. Evaluation of a direct fluorescein-conjugated monoclonal antibody for the detection of cy-tomegalovirus in centrifugation culture. J. Clin. Microbiol. 25:1548–1550. 9. Griffiths, P. D., D. D. Panjwani, P. R. Stirk, M. G. Ball, M. Ganczarovski,
H. G. Blacklock, and H. G. Prentice.1984. Rapid diagnosis of cytomegalo-virus infection in immunocompromised patients with detection of early an-tigen fluorescent foci. Lancet ii:1242–1245.
10. Kawasaki, E. S. 1990. Sample preparation from blood, cells and other fluids, p. 146–152. In M. A. Innis, D. H. Gelfand, J. J. Sninsky, and T. J. White (ed.), PCR protocols: a guide to methods and applications. Academic Press, San Diego, Calif.
11. Kwok, S., and R. Higuchi. 1989. Avoiding false positives with PCR. Nature (London) 339:237–238.
12. Meyers, J. D., P. Ljungman, and L. D. Fisher. 1990. Cytomegalovirus excre-tion as a predictor of cytomegalovirus disease after marrow transplantaexcre-tion: importance of cytomegalovirus viremia. J. Infect. Dis. 162:373–380. 13. Mollison, L. C., M. J. Richards, P. D. Johnson, K. Hayes, W. J. Munckhof,
R. M. Jones, P. D. Dabkowski, and P. W. Angus.1993. High oral acyclovir reduces the incidence of cytomegalovirus infection in liver transplant recip-ients. J. Infect. Dis. 168:721–724.
14. Paya, C. V., P. E. Hermans, T. F. Smith, J. Rakela, R. H. Wiesner, R. A. F.
Krom, V. E. Torres, S. Sterioff, and C. J. Wulkowske.1988. Efficacy of ganciclovir in liver and kidney transplant recipients with severe cytomegalo-virus infection. Transplantation 46:229–234.
15. Paya, C. V., P. E. Hermans, R. H. Wiesner, J. Ludwig, T. F. Smith, J. Rakela,
and R. A. F. Krom.1989. Cytomegalovirus hepatitis in liver transplantation: prospective analysis of 93 consecutive orthotopic liver transplantation. J. Infect. Dis. 60:752–758.
16. Saiki, R. K., S. Scharf, F. Faloona, K. B. Mullis, G. T. Horn, H. A. Erlich,
and N. Arnheim.1985. Enzymatic amplification of beta-globin genomic sequences and restriction site analysis for diagnosis of sickle cell anemia. Science 230:1350–1354.
17. Saltzman, R. L., M. R. Quirk, and M. C. Jordan. 1988. Disseminated cyto-megalovirus infection: molecular analysis and leukocyte interactions in vire-mia. J. Clin. Invest. 81:75–81.
18. Schmidt, C. A., H. Oettle, P. Neuhaus, M. Wiens, H. Timm, F. Wilborn, and
W. Siegert.1993. Demonstration of cytomegalovirus by polymerase chain
on May 15, 2020 by guest
http://jcm.asm.org/
reaction after liver transplantation. Transplantation 56:872–874.
19. Singh, N., J. S. Dummer, S. Kusne, M. K. Breinig, J. A. Armstrong, and L.
Makowka.1988. Infections with cytomegalovirus and other herpesviruses in 121 liver transplant recipients. J. Infect. Dis. 158:124–131.
20. Spector, S. A., R. Merril, D. Wolf, and W. M. Dankner. 1992. Detection of human cytomegalovirus in plasma of AIDS patients during acute visceral disease by DNA amplification. J. Clin. Microbiol. 30:2359–2365. 21. Stratta, R. J., M. S. Shaefer, R. S. Markin, P. Wood, E. M. Kennedy, A. N.
Langnas, E. C. Reed, G. L. Woods, J. P. Donovan, T. J. Pillen, R. M. Duckworth, and B. W. Shaw.1989. Clinical patterns of cytomegalovirus
disease after liver transplantation. Arch. Surg. 124:1443–1449.
22. Van den Berg, A. P., I. J. Klompmaker, E. B. Haagsma, A.
Scholten-Samp-son, C. M. Bijleveld, J. Schirm, M. Van der Giessen, M. J. H. Slooff, and T. H. The.1991. Antigenemia in the diagnosis and monitoring of active cytomegalovirus infection after liver transplantation. J. Infect. Dis. 164:265– 270.
23. Wolff, M. A., K. M. Rand, H. J. Houck, M. E. Brunson, R. J. Howard, and
M. R. Langham.1993. Relationship of the polymerase chain reaction for cytomegalovirus to the development of hepatitis in liver transplant recipi-ents. Transplantation 56:572–576.