EVALUATION OF PARAQUAT POISONING SIDE EFFECTS
Farkhondeh Jamshidi1, Ali Hassan Rahmani2 and Mitra Ekrami3*
1
Department of Forensic Medicine and Toxicology and Social Determinant of Health
Research Center, Ahvaz Jundishapur University of Medical Sciences, Iran.
2
Department of Forensic Medicine and Toxicology and Ahvaz Razi Hospital, Ahvaz
Jundishapur University of Medical Sciences, Iran.
3
Student Research Committee, Ahvaz Jundishapur University of Medical Sciences, Ahvaz,
Iran.
ABSTRACT
Introduction: Poisoning by pesticides is a public health concern in
developing countries. Paraquat is widely used as a means of suicide in
third world countries because it is available at very low cost and has
low-dose toxicity and ten milliliters of it is fatal. This study is designed
to report cases of paraquat poisoning. Material and Method: all cases
of paraquat poisoning hospitalized in Razi hospital within the period of
early 2004 to late 2014 were studied. Accordingly a checklist included
patients’ demographic data (age, gender, location, occupation, educational level, marital status), information on patients’ records
(history of a particular disease, history of using paraquat, suicide),
information on poisoning (mode of poisoning, type of use, nausea after
usage and organ damage) and information on treatment and therapy programs (the interval
between the usage and getting to the hospital, interval between the hospitalization and
receiving the first hemodialysis, patients’ treatment plan, length of hospitalization, result and
complications associated with treatment) that is filled based on the records. In order to
analyze the data using descriptive statistics including frequency tables, diagrams and numeric
indices the variables will be described. Data analysis will be done by SPSS V 18 software.
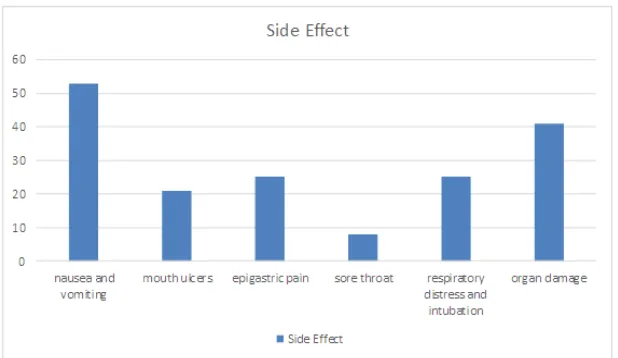
Results: The symptoms observed in patients were associated with nausea and vomiting,
mouth ulcers, sore throat, epigastric pain, respiratory distress and intubation and organ
damage that nausea and vomiting was the most common complication. Finally 58 cases
(95.1%) of the poisonings led to death and 3 patients (4.9%) were discharged with normal
Volume 5, Issue 10, 1254-1261. Research Article ISSN 2277– 7105
*Corresponding Author
Dr. Mitra Ekrami
Student Research
Committee, Ahvaz
Jundishapur University of
Medical Sciences, Ahvaz,
Iran.
Article Received on 21 Aug. 2016,
Revised on 11 Sept. 2016, Accepted on 01 Oct. 2016
condition. Conclusion: the level of deliberate poisoning with Paraquat is much higher in
single men and paraquat has high and fast mortality, thus it is important to train people to
forbid them from storing and keeping it away from the vulnerable people.
KEYWORD: Paraquat, Pesticide, Poisoning Toxicology, Suicide.
INTRODUCTION: One of the major concerns of human health is the deliberate
poisoning.[1] Poisoning by pesticides, that is the cause of up to a third of cases of suicide, is a
public health concern in developing countries.[2] Paraquat is an herbicide that is widely used
to eliminate the weeds.[3] More than 90 percent of deaths due to paraquat have been
associated with committing suicide.[4] It occurs mostly in developing countries and it is
reported as 20 cases per million. This amount is lower in the developed countries, such as
Japan (11 per million) United Kingdom (0.66 per million) and the United States of America
(0.004 per million).[5] Paraquat is widely used as a means of suicide in third world countries
because it is available at very low cost and has low-dose toxicity and ten milliliters of it is
fatal.[6] There are ongoing health campaigns for control and banning Paraquat. There are
activities to limit access to paraquat through keeping in warehouses monitored by the
organization and the reduced use through public education.[7] Paraquat poisoning mechanism
is in its accumulation in the lungs as the target organ. Lung injury is caused by converting
paraquat by intracellular oxidases into free oxygen radicals.[8] The most common type of
suicide with paraquat is oral consumption. Clinical symptoms of paraquat poisoning are
classified into three categories: 1) mild poisoning (less than 20 mg/kg) in which the patient
has mild gastrointestinal symptoms and is usually fully recovered, 2) severe poisoning (20-40
mg/kg) the patient develops renal failure, acute lung injury, progressive pulmonary fibrosis
and respiratory failure 2 to 3 weeks after taking that leads to death and 3) fulminant poisoning
(more than 40 mg/kg) that the patient develops multi-organ failure that leads to death within a
few hours to a few days depending on the dose and the patient’s power.[9] Various methods
are employed for the treatment of paraquat poisoning including preventing the absorption by
gastrointestinal tract, cleansing the bloodstream from toxins, preventing accumulation in the
lungs, oxygen free radicals scavenging and preventing pulmonary fibrosis.[10-12] Also cases of
immunosuppressive, radiotherapy, dialysis and hemoperfusion are mentioned[13-14]
However, effective treatment is still not confirmed and the patients’ result is usually
major public health concern and a high mortality of its poisoning is reported in the
emergency departments, this study is designed to report cases of paraquat poisoning, analyze
the various determinants of the deceased people and in case of observing preventable factors,
the intervention is proposed to the relevant authorities.
MATERIAL AND METHOD
After obtaining permission from the Ethics Committee of Ahvaz Jundishapur University of
Medical Sciences all cases of paraquat poisoning hospitalized in Razi hospital within the
period of early 2004 to late 2014 were studied. Accordingly a checklist included patients’
demographic data (age, gender, location, occupation, educational level, marital status),
information on patients’ records (history of a particular disease, history of using paraquat,
suicide), information on poisoning (mode of poisoning, type of use, nausea after usage and
organ damage) and information on treatment and therapy programs (the interval between the
usage and getting to the hospital, interval between the hospitalization and receiving the first
hemodialysis, patients’ treatment plan, length of hospitalization, result and complications
associated with treatment) that is filled based on the records. In case of incompleteness of
some records of the patients, connections were made with the patients and if it was not
possible for any reason or the patient did not have any detailed information about the
intended cases, that file was excluded from the study. All data of the deceased and survived
patients were compared. It should be noted that in order to maintain confidentiality of
patients, the file code is used rather than their names. In order to analyze the data using
descriptive statistics including frequency tables, diagrams and numeric indices the variables
will be described. Data analysis will be done by SPSS V 18 software.
RESULTS
A total of 61 patients poisoned with paraquat with a mean age of 26±22 were evaluated.
Among them 37 subjects were male and 24 subjects were female and 41 were single and 21
were marries. Also 36 patients were urban and 25 patients were rural citizens. None of the
patients had a history of suicide or the use of paraquat. The symptoms observed in patients
were associated with nausea and vomiting, mouth ulcers, sore throat, epigastric pain,
respiratory distress and intubation and organ damage that nausea and vomiting was the most
common complication. Finally 58 cases (95.1%) of the poisonings led to death and 3 patients
Figure 1. Gender Status
Figure 2. Marital Status
[image:4.596.166.432.75.242.2] [image:4.596.163.431.291.461.2] [image:4.596.144.453.505.684.2]DISCUSSION AND CONCLUSION
Paraquat is widely produced and used around the world because of its unique characteristics.
Paraquat is one of the most common herbicides used in agriculture that can cause severe
poisoning in humans and animals. The most important paraquat targe is the lungs but several
studies have reported neural poisoning among the individuals in contact with it.[16] In
paraquat poisoning the respiratory, cardiovascular, central nervous, endocrine, digestive, skin
and generally all body systems are affected depending on the taken dosage. However, the
poisoning effects of this poisoning usually start with lung involvement and then then appear
as the respiratory distress syndrome. The poisoning starts with the ingestion of +20 mg/kg of
body weight and usually the serum levels greater than 1.0 mg/ml within and more than 0.1
mg/ml will lead to death within 24 and 48 hours.[17] Studies have shown that pulmonary
fibrosis caused by paraquat can be prevented or delayed by some antioxidants, melatonin,
iron chelators and blood pressure medication such as Captopril in recent years. Also
apoptosis induction in cells by angiotensin and Angiotensinogen has been reported. Recent
studies have shown that these medicines and Captopril in particular have anti-fibrotic and
apoptosis inhibition in lung alveolar epithelial cells.[18-20] However, the thing that is more
important than any other subject is the knowledge of the complications caused by paraquat
poisoning and familiarity with the morbidities and mortalities caused by this toxic substance
and obviously performing epidemiological studies with a greater range can increase the level
of awareness of this type of poisoning. As has been observed in the results, most people who
attempted suicide by paraquat have been in the range of less than 30 years oldand it has be
more applied by single male urban citizens that have deliberately used edible paraquat. The most important observed symptoms have been nausea and vomiting and observed patients’
mortality was 95.1%. Although the obtained data present a good knowledge of paraquat poisoned patients’ conditions, it is necessary to address the studied conducted by other
researchers to further understand the side effects and compare them with other paraquat
poisoned patients. For example Afzali wt al (2007) studied the effect of methylprednisolone
and cyclophosphamide combined therapy on edible paraquat poisoning. During the two-year
study of 45 patients with edible paraquat poisoning admitted to Sina hospital in Hamedan it
was observed that 20 subjects had moderate to severe poisoning. The mean ages of the first
and second group were 25 and 26. There were 3 female and 8 male subjects in the first group
and one female and eight male subjects in the second group. The rate of mortality was 81.8
and 33.3% in the first and second groups.[21] In fact most patients were male in their study as
methylprednisolone and cyclophosphamide the mortality rate is significantly reduced.
Sabzghabaee et al (2010) carried out a study on mortality due to paraquat poisoning. In this
study all patients who had referred to the emergency room of University Hospitals of Esfahan
Medical sciences were analyzed. A total of 29 patients were studied. The mortality rate in the
hospital was 55.2%. There was a significant relationship between patients’ nausea and their
treatment outcome.[22] Their mortality rate was much lower than the present study that is
associated with the dosage, the duration of getting to hospital and support measures. Many
studies are carried out in other countries for example Seok et al (2009) studied edible
Paraquat poisoning in people who had consumed it to commit suicide. In this study, 250
patients including 143 men and 107 women were studied. Patients were classified into the
purchased and available paraquat subgroups. Women had used the purchased paraquat more
than men (66% vs. 22%). The number of single men was higher than single women (23.9%
vs. 9.3%) and they were more divorced or living separate lives (11.3% vs. 4.6%). 38.4% of
people had selected paraquat deliberately and consciously and 61.6% had not selected it
deliberately. Therefore, two third of people had not spent money on it and used it because of
its availability Thus it is necessary to control the availability of paraquat.[15] In fact, this study
has addressed access to paraquat that is not addressed in the present study but the results
obtained in their study are consistent with the present study including the fact that most of the
subjects were male and single. More attention to the present study and the reviewed studies
suggest that the level of deliberate poisoning with Paraquat is much higher in single men and
paraquat has high and fast mortality, thus it is important to train people to forbid them from
storing and keeping it away from the vulnerable people. Also the obtained information
indicates that the international organizations should challenge the production and distribution
of this toxin with novel approaches.
REFERENCES
1. Rahmani H, Javadi I, Shirali S. Respiratory Complications Due to Sulfur Mustard
Exposure. International journal of current research and academic review. 2016 Jun; 4(6):
143.
2. Bertolote JM, Fleischmann A, Eddleston M, Gunnell D. Deaths from pesticide poisoning:
a global response. Br J Psychiatry, 2006; 189: 201-3.
3. Paraquat dichloride. International Programme on Chemical Safety. October 2001.
5. Onyon LJ, Volans GN. The epidemiology and prevention of paraquat poisoning. Hum
Toxicol. 1987; 6: 19–29.
6. Emsley, John. Molecules of Murder: Criminal Molecules and Classic Cases. Royal
Society of Chemistry Publishing, 2008; 195.
7. Bismuth C, Garnier R, Dally S, Fournier PE, Scherrmann JM. Prognosis and treatment of
paraquat poisoning: a review of 28 cases. J Toxicol Clin Toxicol, 1982; 19: 461-74.
8. Dinis-Oliveira RJ, Duarte JA, Sánchez-Navarro A, et al. Paraquat poisonings:
mechanisms of lung toxicity, clinical features, and treatment. Crit Rev Toxicol, 2008; 38:
13-71.
9. Lee HL, Lin HJ, Yeh ST, Chi CH, Guo HR. Presentations of patients of poisoning and
predictors of poisoning-related fatality: findings from a hospital-based prospective study.
BMC Public Health, 2008; 8: 7.
10.Meredith TJ, Vale JA. Treatment of paraquat poisoning in man: methods to prevent
absorption. Hum Toxicol. 1987; 6: 49–55.
11.Lock EA, Smith LL, Rose MS. Inhibition of paraquat accumulation in rat lung slices by a
component of rat plasma and a variety of drugs and endogenous amines. Biochem
Pharmacol. 1976; 25: 1769–1772.
12.Kitazawa Y, Matsubara M, Takeyama N, Tanaka T. The role of xanthine oxidase in
paraquat intoxication. Arch Biochem Biophys. 1991; 288: 220–224.
13.Webb DB, Williams MV, Davies BH, James KW. Resolution after radiotherapy of severe
pulmonary damage due to paraquat poisoning. Br Med J. 1984; 288: 1259–1260.
14.Okonek S, Hofmann A, Henningsen B. Efficacy of gut lavage, hemodialysis and
hemoperfusion in therapy of paraquat or diquat intoxication. Arch Toxicol. 1976; 36:
43–51.
15.Su-Jin Seok, Hyo-Wook Gil, Du-Shin Jeong, Jong-Oh Yang, Eun-Young Lee, Sae-Yong
Hong. Paraquat Intoxication in Subjects Who Attempt Suicide: Why They Chose
Paraquat. Korean J Intern Med. Sep 2009; 24(3): 247–251.
16.Pourahmad J, Hosseini MJ, Bakan S, Ghazi Khansari M. Hepatoprotective activity of
angiotensin-converting enzyme (ACE) inhibitors, captopril and enalapril, against paraquat
toxicity. Pestic Biochem Phys. 2011; 99(1): 105–110.
17.Bove´ J, Prou D, Perier C, Przedborski S. Toxin-Induced Models of Parkinson’s Disease.
Neuro Rx. 2005; 2(3): 484–494.
18.Eizadi-Mood N, Sabzghabaee AM, Badri S. Paraquat Poisoning: What the Acute Care
19.Chandler DB, Hyde DM, Giri SN. Morphometric estimates of infiltrative cellular changes
during the development of bleomycininduced pulmonary fibrosis in hamsters. Am J
Pathol, 1983; 112: 170-7.
20.Wang R, Ramos C, Joshi I, Zagariya A, Pardo A, Selman M, et al. Human lung
myofibroblast-derived inducers of alveolar epithelial apoptosis identified as angiotensin
peptides. Am J Physiol, 1999; 277: L1158-64.
21.Song L, Wang D, Cui X, Shi Z, Yang H. Kinetic alterations of angiotensin-II and nitric
oxide in radiation pulmonary fibrosis. J Environ Pathol Toxicol Oncol, 1998; 17: 141-50.
22.Ohishi T, Saito H, Tsusaka K, Toda K, Inagaki H, Hamada Y, et al. Erratum to
"Anti-fibrogenic effect of an angiotensin converting enzyme inhibitor on chronic carbon
tetrachloride- induced hepatic fibrosis in rats". Hepatol Res., 2002; 22: 322.
23.Afzali S, Gholyaf M. The Effectiveness of Combined Treatment with Methylprednisolone
and Cyclophosphamide in Oral Paraquat Poisoning. Arch Iranian Med, 2008; 11(4):
387–391.
24.Sabzghabaee A M, Eizadi-Mood N, Montazeri K, Yaraghi A, Golabi M. Fatality in