PULSATILE DRUG DELIVERY
A K Dhadwe1*, C P Rathod, S M Vadvalkar, G R Shendarkar, P H Bhosale and Patil K G.
Department of Pharmaceutics and Pharmaceutical Technology Nanded Pharmacy College,
Shyam Nagar Nanded, Maharashtra, India.
ABSTRACT
The release of the drug as a pulse after a lag time has to be designed in
such a way that a complete and rapid drug release follows the lag time.
Various systems like capsular systems, osmotic systems, single and
multiple-unit systems based on the use of soluble or erodible polymer
coating and use of rupturable membranes have been dealt with in the
article. It summarizes the latest technological developments,
formulation parameters, and release profiles of these systems.In the
present work Eudragit S 100 alone is used for coating. Batches were
coated in different percent weight gain from 1-7 percent. These coated
tablets showed increase in the lag time with increase in the coating
level. The lag time increases from 2 to 8 hrs for the coating of 1-7 %
respectively. This study was utilized to optimize the formulation. The
present work concludes that there is a constant need for new delivery
systems that can provide increased therapeutic benefits to the patients. Pulsatile drug delivery
is one such system that, by delivering drug at the right time, right place, and in right amounts,
holds good promises of benefit to the patients suffering from chronic problems like arthritis,
asthma, hypertension, etc.
KEYWORDS: Modified release oral tablet; Single pulsatile drug; Sustain action; Challenges; Approaches; Market status.
INTRODUCTION
Modified release dosage forms represent the most popular form of controlled drug delivery
systems due to the obvious advantages of oral route of drug administration. Modified release
product can be defined as a system where his principle rationale for the use of pulsatile
Volume 4, Issue 5, 2599-2613. Research Article ISSN 2277– 7105
Article Received on 19 March 2015,
Revised on 08 April 2015, Accepted on 29 April 2015
*Correspondence for Author
A K Dhadwe
Department of
pharmaceutics and
pharmaceutical
technology Nanded
Pharmacy College, Shyam
Nagar, Nanded,
release is for the drugs where a constant drug release, i.e., a zero-order release is not desired.
“The drug release characteristic of time. Course and/or location are chosen to accomplish therapeutic or convenience objective not offered by conventional dosage forms” Terbutaline
Sulphate should be delivered when it is needed in minimum required dose. For Terbutaline
Sulphate to follow the circadian rhythm in asthma the reasonable and acceptable delivery
system capable of releasing the drug in a pulsatile fashion is needed. Therapy with modified
release dosage form with zero order release theoretically leads to controlled and constant
levels of drug in plasma throughout the day.
Advantages of pulsatile drug delivery
1. Extended day time or nighttime activity.
2. Reduced side effects.
3. Reduced dosage frequency.
4. Reduction in dose size.
5. Improved patient compliance.
6. Lower daily cost to patient due to fever dosage units are required by the patient in
therapy.
7. Drug adducts to suit circadian rhythm of body function or disease.
8. Drug targeting to specific sites like colon.
9. Protection of mucosa from irritating drugs.
1. Commercial products
Table no.I Commercial products of Pulsatile DDS
Technology Mechanism Proprietary name and
dosage form API Disease
OROS® Osmotic mechanism Covera-HS®; XL tablet Verapamil HCl Hypertension
CODAS® Multi particular pH dependent system
Verelan® PM; XL
release capsule Verapamil HCl Hypertension
DIFFUCAPS® Multi particulate system Innopran®; XL tablet Verapamil HCl,
Propranolol HCl Hypertension
Table no.II Name of Material & supplied company
Sr.no. Chemical Ingredient Supplier
1 Drug [ Terbutaline Sulphate ] Shimoga Chemicals Pvt. India. 2 Microcrystalline cellulose Ideal Cures Ltd., Mumbai.
3 Sodium starch glycolate Signet Chemicals Pvt Ltd, Mumbai.
4 Eudragit S 100 Evonik Pvt.Ltd.Mumbai.
5 Magnesium stearate Loba Chemicals, Mumbai
7 Potassium dihydrogen phosphate S. D. Fine chemicals, Mumbai
8 Acetone S. D. Fine chemicals, Mumbai
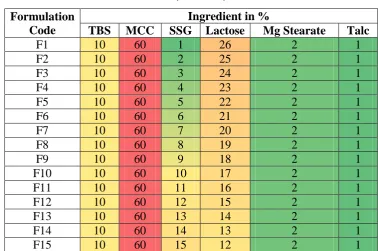
[image:3.595.106.485.134.385.2]2. Formulation of core tablet
Table .no. III Formulation of core tablet (Formula) Formulation
Code
Ingredient in %
TBS MCC SSG Lactose Mg Stearate Talc
F1 10 60 1 26 2 1
F2 10 60 2 25 2 1
F3 10 60 3 24 2 1
F4 10 60 4 23 2 1
F5 10 60 5 22 2 1
F6 10 60 6 21 2 1
F7 10 60 7 20 2 1
F8 10 60 8 19 2 1
F9 10 60 9 18 2 1
F10 10 60 10 17 2 1
F11 10 60 11 16 2 1
F12 10 60 12 15 2 1
F13 10 60 13 14 2 1
F14 10 60 14 13 2 1
F15 10 60 15 12 2 1
The core tablets were prepared with selected excipients by direct compression on single
punch tablet compression machine. Accurately weighed quantities of drug and other
ingredients like sodium starch glycolate, lactose, and magnesium stearate were mixed by
triturating in glass mortal-pestle. The blend was directly compressed at weight of 150 mg
using 7 mm diameter punch. The compositions of the formulation batches containing
different ratios of polymers chosen on trial and error basis. (Swarbrick, J. 2005).
3. Physical Evaluation of Powder Blend used for Preparation coare Tablet
Table no. IV Physical evaluation of powder blend used for preparation of core tablet Formulation Angle of
Repose
Bulk Density (g/cm2)
Tap Density g/cm2)
%
Compressibility
F 1 26.110.04 0.420.06 0.470.03 7.540.03 F 2 26.880.03 0.480.06 0.510.05 6.120.04 F 3 28.450.03 0.470.04 0.480.03 8.920.03 F 4 28.670.02 0.510.05 0.580.06 7.940.05 F 5 27.020.03 0.430.06 0.570.06 9.090.03 F 6 27.780.03 0.520.04 0.540.05 11.110.05 F 7 28.290.04 0.510.04 0.440.03 10.630.07 F 8 30.890.05 0.480.05 0.580.06 7.540.03 F 9 29.230.04 0.380.05 0.640.05 8.770.03
[image:3.595.84.511.576.760.2]F 11 28.770.02 0.510.05 0.580.06 7.950.05 F 12 28.320.04 0.490.04 0.440.03 10.430.07 F 13 26.020.04 0.410.06 0.470.03 7.340.03 F 14 29.230.04 0.380.05 0.640.05 8.770.03
F 15 28.900.03 0.40.04 0.70.06 8.020.03
n=3
Table no. V Evaluation of core tablets
Formu-lation
Hardness Weight
Uniformity Friability Thickness Uniformity of content
Disintegration time (sec.)
(kg/cm2) (mg) ± SD (%)
F1 4.8 148±1.12 0.621 1.5±0.3 100±1.02 63
F2 4.9 152±1.123 0.554 1.6±0.3 101±1.12 60
F3 4.8 156±1.09 0.741 1.40±0.4 101±1.04 57
F4 4.5 151±0.05 0.358 1.55±0.5 98±0.98 55
F5 4 .6 145±0.97 0.558 1.54±0.5 99±0.94 53
F6 4 .3 158±1.34 0.658 1.5±0.3 102±1.26 51
F7 4 .7 160±1.56 0.554 1.6±0.3 100±1.01 47
F8 4 .4 155±0.06 0.741 1.40±0.4 101±1.02 42
F9 4 .3 148±1.12 0.358 1.55±0.5 97±1.12 40
F10 3.9 152±1.123 0.558 1.5±0.3 98±0.99 36
F11 4.5 156±1.09 0.721 1.5±0.3 100±1.04 33
F12 4.3 151±0.05 0.348 1.6±0.3 99±0.98 31
F13 4.4 161±0.05 0.598 1.40±0.4 98±0.94 24
F14 4.6 156±1.09 0.657 1.55±0.5 100±1.26 20
F15 4.2 151±0.05 0.553 1.6±0.3 99±1.01 15
n=3
4. Dissolution study
Table no.VI Dissolution profile of core tablet formulation
Batch code % Cumulative Release/ Min.
0 1 2 3 4 5
F1 0 20±0.98 47±0.65 78±0.98 89±0.99 99±0.99
F2 0 27±0.59 59±0.95 86±1.01 91±1.05 98±0.82
F3 0 29±0.85 41±0.68 73±1.02 84±1.05 99±0.88
F4 0 35±0.86 67±0.87 79±1.9 97±0.97 -
F5 0 21±0.68 59±0.69 80±0.99 98±0.86 -
F6 0 33±0.67 52±0.95 79±0.96 98±0.98 -
F7 0 37±0.95 66±0.87 83±0.89 99±1.04 -
F8 0 35±0.96 74±0.57 89±0.95 98±1.09 -
F9 0 45±0.92 78±0.65 99±1.08 - -
F10 0 38±0.94 69±0.54 93±1.02 - -
F11 0 42±1.09 77±0.89 99±1.0 - -
F12 0 47±0.83 81±0.97 98±1.05 - -
F13 0 68±0.87 99±0.92 - - -
F14 0 79±0.97 97±0.98 - - -
Fig.no.I Dissolution profile for core tablet 5. FORMULATION OF COATING SOLUTION
Table no.VII Formulation of coating solution.(Formula)
Coating Material CT 1 CT 2 CT 3 CT 4 CT 5 CT6 CT7
Eudragit S100 (%) 1 2 3 4 5 6 7
Avg.% Wt Gain 1 2 3 4 5 6 7
Di-butyl phthalate
(%) 2 2 2 2 2 2 2
Solvent (ml) 100 100 100 100 100 100 100
The core tablets were coated with a polymethacrylate co-polymer with pH dependent
solubility.
A. COATING OF TERBUTALINE SULPHATE CORE TABLET
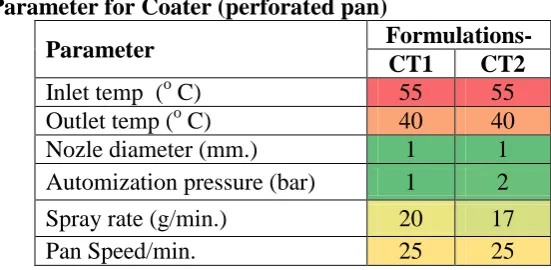
Coating was carried with help of spray gun .The parameter are shown in following tablet.
Table no.VIII Parameter for Coater (perforated pan)
Parameter Formulations-
CT1 CT2
Inlet temp (o C) 55 55
Outlet temp (o C) 40 40
Nozle diameter (mm.) 1 1
Automization pressure (bar) 1 2
Spray rate (g/min.) 20 17
Pan Speed/min. 25 25
6. RESULT DISCUSSION
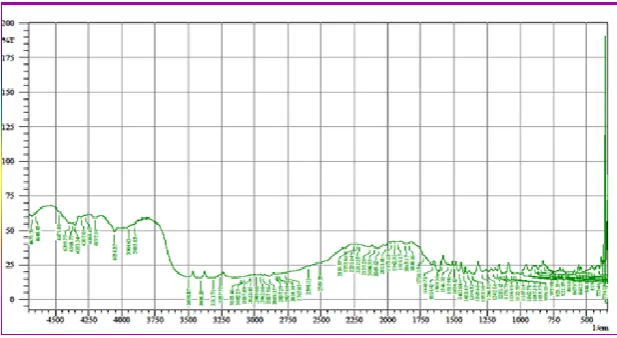
A. FTIR studies: The FT-IR spectra of pure drug was taken by preparing KBr pellets. (Disk method) Scanning Range: 4000 – 500 cm -1
[image:5.595.151.427.541.676.2]Table No.IX: Interpretation IR
Fig. no.II FT-IR Spectrum of Terbutaline Sulphate.
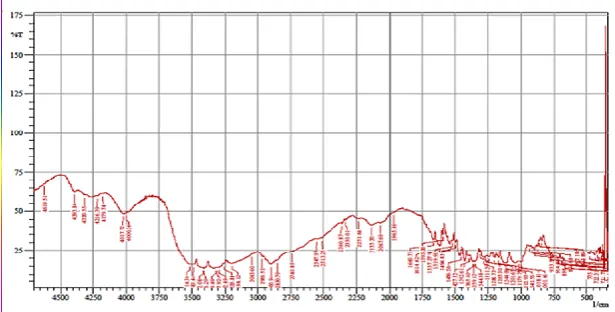
C. Drug-polymer compatibility study: The FT-IR spectra of pure drug was taken by preparing KBr pellets. (Disk method) Scanning Range: 4000 – 500 cm –
[image:6.595.143.452.476.645.2]1.SSG,MCC
Fig.no. III FT-IR Spectrum of SSG & MCC. Interpretation of FTIR data
Wave number (cm-1) Assignments
1716 C=N Stretching
1670 C=O Stretching
1568 NH Bending
2. TBS, SSG, MCC
[image:7.595.143.451.344.500.2]Fig.no IV. FT-IR Spectrum of TBS,SSG & MCC. 3. Core Tablet
Fig no. V FT-IR Spectrum of Core Tablet. 4. Eudragit S 100
[image:7.595.145.453.575.744.2]B. Determination of λmax
Determination of λmax in pH 1.2 , 7.4 and 8.1
The solution of Terbutaline sulphate in above medium was scanned from 200 to 400 nm in
order to determine the λmax for its estimation in the respective media. The UV spectrum
obtained is shown in Figure. The wavelength of maximum absorbance (λ max) was found to be
275 nm in simulated gastric fluid and 276 nm in pH 7.4 and 8.1
[image:8.595.311.510.211.334.2]
Fig.No.VII Scanning of Terbutaline Fig. No.VIII Scanning of Terbutaline Sulphate in gastric fluid (pH 1.2) sulphate in intestinal fluid (pH 7.4 & 8.1) C. Calibration curve
Calibration curve of Terbutaline in pH 1.2
Absorbance data for calibration curve of Terbutaline Sulphate in simulated gastric fluid PH
[image:8.595.86.282.211.333.2]1.2
Table no. X Calibration curve Value
Figure No. IX Calibration curve of TBS in simulated gastric fluid Calibration curve of TBS
in pH 7.4 (intestinal fluid) Sr. Concentration
(µg/ml) Absorbance
1 0 0
2 2 0.1023
3 4 0.2046
4 6 0.3036
5 8 0.3996
6 10 0.5055
7 12 0.6035
8 14 0.6991
275nm 276
Table no.XI Absorbance data for calibration curve of Terbutaline sulphate in intestinal fluid:
Fig.X Calibration curve of Terbutaline
[image:9.595.64.545.323.487.2]Sulphate in intestinal fluid pH 7.4
Table no.XII Absorbance data for calibration curve of Terbutaline sulphate in pH 8.1
Fig.XI Calibration curve of Terbutaline Sulphate in in pH 8.1
Table no.XIV Evaluation of coated tablet Coated
Formulation Hardness
Weight
variation Disintegration
time (in hr.) Thickness Friability
Uniformity of content (mg) ± SD
CT 1 4 .3 152±1.12 1 2.8±0.02 0.554 98±0.98
CT 2 4 .7 153±1.123 2 2.9±0.02 0.741 99±0.94
CT 3 4 .4 155±1.09 3 3.0±0.04 0.358 102±1.26
CT 4 4 .3 157±0.05 4 2.9±0.03 0.558 100±1.01
CT 5 3.9 159±0.97 5 3.0±0.03 0.658 101±1.02
CT6 4 159±0.98 6 3.1±0.05 0.554 987±1.12
CT 7 4 .2 162±.58 7 3.0±0.03 0.554 98±0.98
S.N. Concentration
(µg/ml) Absorbance
1 0 0
2 2 0.13
3 4 0.225
4 6 0.363
5 8 0.481
6 10 0.611
7 12 0.711
8 14 0.865
Sr.No. Concentration
(µg/ml) Absorbance
1 0 0
2 2 0.14
3 4 0.285
4 6 0.419
5 8 0.55
6 10 0.698
7 12 0.838
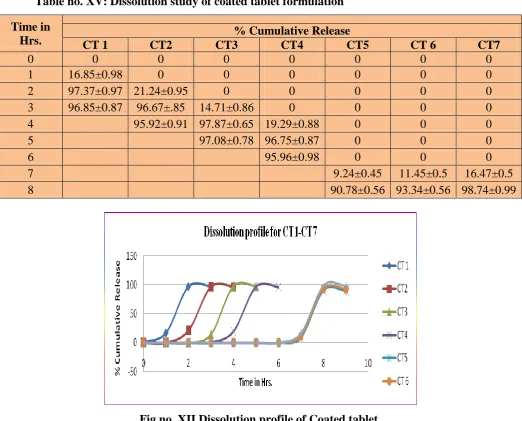
Table no. XV: Dissolution study of coated tablet formulation Time in
Hrs. CT 1 CT2 CT3 % Cumulative Release CT4 CT5 CT 6 CT7
0 0 0 0 0 0 0 0
1 16.85±0.98 0 0 0 0 0 0
2 97.37±0.97 21.24±0.95 0 0 0 0 0
3 96.85±0.87 96.67±.85 14.71±0.86 0 0 0 0
4 95.92±0.91 97.87±0.65 19.29±0.88 0 0 0
5 97.08±0.78 96.75±0.87 0 0 0
6 95.96±0.98 0 0 0
7 9.24±0.45 11.45±0.5 16.47±0.5
8 90.78±0.56 93.34±0.56 98.74±0.99
[image:10.595.37.560.78.499.2]
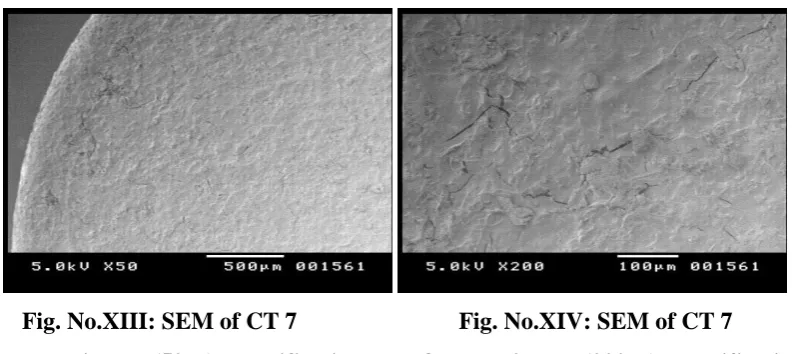
Fig.no. XII Dissolution profile of Coated tablet. D. Scanning electron microscopy
The coating of optimised batch were examined by scanning electron microscopy as shown in
figures Fig No, a illustrating the microphotographs of formulation CT 7 at lower and higher
magnification. The coated surface was spherical with no visible major surface irregularity.
Few wrinkles and inward dents were appeared on the surface of tablet . It may due to collapse
Fig. No.XIII: SEM of CT 7 Fig. No.XIV: SEM of CT 7
formulation at (50 X) magnification formulation at (200 X) magnification 7. Stability study
Accelerated stability studies (AST) was carried for optimized formulation CT5 by exposing
to 40°C/75% RH for one month and analyzed the sample at the interval of 7,14,21,28 days.
[image:11.595.100.497.68.245.2]The sample was analyzed.
Table No.XVI: AST of CT 7 formulation.
Table Sr.N0. Days % Drug remaining
% Drug remaining2
% Drug remaining3 5-8C 272 C 402 C
1 0 100 0.010 100 0.14 100 0.17
2 15 99.97 0.13 99.86 0.21 99.63 0.20
3 30 99.80 0.05 99.81 0.16 99.46 0.16
4 45 99.74 0.12 99.79 0.11 99.29 0.09 5 60 99.68 0.15 99.75 0.12 99.13 0.18
6 75 99.85±0.02 99.78±0.12 99.45±0.04
7 90 99.45±.23 99.58±0.13 99.65±0.15
CONCLUSION
Literature review of pulsatile drug delivery reveals that the dosage form releases the drug
immediately after a period of time lag. And this can be achieved by developing various
systems like capsular systems, osmotic systems, pH sensitive drug delivery system, single-
and multiple-unit systems based on the use of soluble or erodible polymer coating and use of
reputable membranes, systems with reputable coating layer, systems with erodible coating
layers. In such systems the drug release is controlled by the dissolution or erosion of the
outer coat which is applied on the core containing drug. It is useful tool for delivering
[image:11.595.93.496.393.546.2]The preclinical studies have shown that pulsatile approach of delivering antibiotic is
more effective.
ACKNOWLEDGMENT
This dissertation would not have been possible without the guidance and the help of several
individuals. Would like to thanks for excellent guidance of Dr. S. M.Vadvalkar, Principal of
Nanded Pharmacy College, Nanded. Whose encouragement I will never forget.
REFRENCES
1. Abraham S., Srinath, M.S., Development of modified pulsincap drug delivery system of
metronidazole for drug targeting. Ind J Pharm Sci, 2008; 24-27.
2. Ahuja A and Baboota, S., Chronomodulated drug delivery of salbutamol sulphate for
nocturnal asthma. Ind J Pharm Sci, 2008; 351-57.
3. Ahuja A and Baboota, S., Chronomodulated drug delivery of salbutamol sulphate for
nocturnal asthma. Ind J Pharm Sci, 2008; 351-57.
4. Akhgari A., Sadeghi. F., Garekani. H.A., Combination of time-dependent and
pH-dependent polymethacrylates as a single coating formulation for colonic delivery of
indomethacin pellets. Int J Pharm, 2006; 320.137-142.
5. Arora A., Ali, J., Alka, A., Pulsatile drug delivery: An approach for controlled drug
delivery. Ind J Pharm Sci, 2008; 295-301.
6. Banker G.S. and Anderson, N.R., Tablets. In; Lachman L, Lieberman, H.A. and Kanig,
J.L., The theory and practice of industrial pharmacy, 3rd ed. Varghese Publishing House,
1987; 297-299, 300, 317.
7. Banker SG, Anderson R.N., Tablets. In, Lachman L, Liberman AH, Kanig LJ. Text book
of the theory and practice of industrial pharmacy, 3rd edition. Mumbai, Varghese
Publication House, 1991; 317-324.
8. Barzegar J. M., Siyahi-Shadbad, M., Design and evaluation of delayedrelease osmotic
capsule of acetaminophen. Iran J Pharma Sci Spring. 2006; 2.65-72.
9. Bin L., Chun L.Z., Wen.G., A novel system for three-pulse drug release based on “tablets
in capsule” device J contr Rel, 2008; 352. 159-164.
10.Bolton S., Pharmaceutical Statistics practical and Clinical Aplications., In Optimization
Techniques., Marcel Dekker Inc., 2000; 832-568.
12.Bussemer T., Peppas. N.A., Bodmeier. R., Evaluation of the swelling, hydration and
rupturing properties of the swelling layer of a rupturable pulsatile drug delivery system.
Eur J Pharm Biopharm, 2003; 56: 261-270.
13.Cartensen J. T., Drug stability:Principle and practice. 2nd Edn, Marcel dekker, New York,
1995; 538-550.
14.Chourasia M.K., Jain S.K., Pharmaceutical approach to colon targeted drug delivery
systems, J Pharm Sci, 2002; 6: 33-66.
15.Clark’s Analysis of Drug and Poison Anthony C Moffal, M David, Pharmaceutical press,
3rd Edn,Vol.2,1606.
16. Dashevsky A., Mohamad. A., pH-independent pulsatile drug delivery system based on
hard gelatin capsules and coated with aqueous dispersion Aquacoat_ ECD. Eur J Pharm
Biopharm, 2006; 64. 173-179.
17.Efentakis M., Koligliati. S., Vlachou. M., Design and evaluation of a dry coated drug
delivery system with an impermeable cup, swellable top layer and pulsatile release. Int J
Pharm, 2006; 311. 147–156.
18.Evangelos K., Emmanouel. G., Dimitrios. B., Application of PVP/HPMC miscible blends
with enhanced mucoadhesive properties for adjusting drug release in predictable pulsatile
chronotherapeutics. Eur J Pharm Biopharm, 2006; 64. 115-126.
19. Fan T.Y., Wei.S.L., Yan.W.W., Chen.D.B., Li.J., An investigation of pulsatile release
tablets with ethylcellulose and Eudragit L as film coating materials and cross-linked
polyvinylpyrrolidone in the core tablets. J control Release, 2001; 77. 245–251.
20.Ghimire M., Fiona.J,. David.G.W., Alexander.B.M., In-vitro/in-vivo correlation of
pulsatile drug release from press-coated tablet formulations: A pharmacoscintigraphic
study in the beagle dog Eur J Pharm Biopharm, 2007; 67.515-513.
21.Hardman J.G., Limbird, L,E., Gillman, A.G., Goodman & Gilman's the pharmacological
basis of therapeutics - 11th eds, Mc graw hill medical publishing devision, New York,
2006; 735.
22.Indian Pharmacopoeia.Govt. of India. Ministry of Health and Family Welfare, The Indian
Pharmacopoeial commission, Ghaziabad. Vol I, 2007; 182-183.
23.Intra. J., Justin .M., Hoang Q. M., Aliasger K. S., Pulsatile release of biomolecules from
polydimethylsiloxane (PDMS) chips with hydrolytically degradable seals. J. control
24.James W., Pharmaceutical preformulation: the physicochemical properties of drug
substances. In: Aulton M.E. (Ed.), Pharmaceutics: The Science of dosage Form Design,
2nd ed., Churchill Livingstone, 2002; 133-135.
25.Kulkarni A. R., Mastiholimath.V.S., Dandagi.P.M., Jain.S.S., Gadad.A.P., Time and pH
dependent colon specific, pulsatile delivery of theophylline for nocturnal asthma. Int J
Pharm, 2007; 328: 49-56.
26.Mahajan A.N., Pancholi S.S., Formulation and evaluation of timed delayed capsule
device for chronotherapeutic delivery of terbutaline sulphate, Ars Pharm, 2010; 50:
215-223.
27.McConville J.T., Ross,A.C., Chambers, A.R., Geoff, S., Florence,A.J.,Howard, N.E.
2004, The effect of wet granulation on the erosion behavior of a HPMC-lactose tablet,
used as rate controlling component in a pulsatile drug delivery capsule formulation. Eur J
Pharm Biopharm., 57 541–549.
28.Parmar R.D., Vidysagar G., Patel D.P., Patel C.J., Patel B.D. Parikh R.K., Pulsatile drug
delivery system an overview, Int JPharm Sci Nanotech, 2009; 2: 605-613.
29.Pawar A., Sharma.S., Low density multiparticulate system for pulsatile release of
meloxicam. Int J Pharm, 2006; 313: 150-158.
30.Pawar R. D., Parikh R.K., Pulsatile Drug Delivery Systems: An Overview, Int. J Pharm.
Sci. and Nanotech. 2009; 2(3): 605-614.
31.Reinberg A., Smolensky, M.H., Biologic Rhythms in Clinical and LaboratoryMedicine,
In: Y. Touiotu, E. Haus, Night and shift work and transmeridian and space flights,
Springer-Verlag, Heidelberg, 1992; 242–255.
32.Rowe R. C., Sheskey, P. J., Weller, P. J., Handbook of Pharmaceutical Excipients. Fourth
ed., Pharmaceutical Press, 2003; 108-112.
33.Rowe R. C., Sheskey, P. J., Weller, P. J., 2003, Handbook of Pharmaceutical Excipients.
Fourth ed., Pharmaceutical Press, 581- 586.
34.Sachin S. and Neeraj, K., Pulsatile drug delivery: current scenario, review. CRIPS, 2007;
8: 27-33.
35.Satit P., Srisagul S., Development of pulsatile release tablets with swellingand rupturable
layers , Journal of Controlled Release, 2004; 95: 147– 159.
36.Schellekens C.A, Stellaard. F., Mitrovic. D., Stuurman.F.E., Kosterink.J.G.W., Frijlink.
H.W. Pulsatile drug delivery to ileo-colonic segments by structured incorporation of
37.Smolensky M.H. ,Halberg, F., Circadian rhythm in airway patency and lung volumes, in:
J.P. McGovern, M.H. Smolensky, A. Reinberg (Eds.), Chronobiology in Allergy and
Immunology, C.C. Thomas, Springfield, ll, 1977; 117–138.
38.Smolensky M.H., Lemmer B., Reinberg A.E., The chronobiology and chronotherapy of
allergic rhinitis and bronchial asthma, Adv. Drug Deliv. Rev. 2007; 59: 852–882.
39.Sungthongjeen S., Puttipipatkhachorn S., Paeratakul O., Development of pulsatile release