ABSTRACT
CREWS, JOHN HUNTER. Development of a Shape Memory Alloy Actuated Robotic Catheter for Endocardial Ablation: Modeling, Design Optimization, and Control. (Under the direction of Dr. Gregory Buckner).
Atrial fibrillation is the most common cardiac arrhythmia, afflicting more than 2
million Americans. Symptoms include shortness of breath, fatigue, chest pain, stroke, and
even death. Treatment options consist of pharmacological, surgical, and electrophysiological
(ablation catheter-based) approaches. The ideal treatment would combine the effectiveness of
surgical methods with the minimally invasive attributes of catheter-based approaches.
However, commercially available catheters possess a number of limitations that hinder their
effectiveness. This dissertation focuses on the design optimization and control of a robotic
ablation catheter, internally actuated using shape memory alloys (SMAs), that overcomes
many of the limitations of existing ablation catheters.
The robotic ablation catheter is constructed from serially connected bending segments
actuated by internal SMA tendons. Each bending segment contains four SMA actuators that
contract upon heating and produce bending moments. The multiple actuators and segments
provide greater navigability for the physician. Coupled with the catheter’s
computer-controlled capabilities, this robotic catheter has the potential to improve success rates and
reduce procedure times in the treatment of AF, while simultaneously reducing healthcare
costs and radiation exposure to patients and medical staff.
The kinematics and inverse kinematics of the robotic catheter are developed in two
coordinate systems: three-dimensional Cartesian coordinates and generalized coordinates
2
generalized coordinates, while catheter tip measurements are made in Cartesian coordinates,
motivating the need for transformations between the two.
The catheter’s bending mechanics are described using a circular arc model, while
SMA actuation is modeled using free energy techniques. Two specific cases are considered:
single-tendon SMA actuation and antagonistic SMA actuation. Both cases are modeled using
COMSOL Multiphysics Modeling and Simulation Software and are experimentally
validated.
Design optimization of the robotic catheter is accomplished using the COMSOL
models and genetic algorithms (GAs). The geometry and material properties of each model
are parameterized and used as design variables in the GA. Both single-objective and
multi-objective cases are considered. The single-multi-objective problem optimizes the catheter’s radius
of curvature, a measure of its navigability. The multi-objective problem optimizes radius of
curvature and “pushability”, a quality related to catheter stiffness.
The computationally efficient hysteretic recurrent neural network (HRNN) is
implemented into a sliding mode control algorithm for the position control of SMA actuators.
The method is derived for a constant stress SMA actuator and demonstrated experimentally.
The control algorithm is extended to variable stress SMA actuators, the situation encountered
in the robotic catheter. Simulation results are presented for a single SMA actuator, and the
Development of a Shape Memory Alloy Actuated Robotic Catheter for Endocardial Ablation: Modeling, Design Optimization,
and Control
by
John Hunter Crews
A dissertation submitted to the Graduate Faculty of North Carolina State University
in partial fulfillment of the requirements for the degree of
Doctor of Philosophy
Mechanical Engineering
Raleigh, North Carolina
2011
APPROVED BY:
_______________________________ ______________________________
Gregory D. Buckner Paul I. Ro
Committee Chair
ii
DEDICATION
iii
BIOGRAPHY
John Crews was born and raised in Lexington, VA, where the only thing to do was
run. He came to North Carolina State University as an undergraduate to continue running. He
met his wife Amy at NCSU, who also ran for the cross country and track and field teams.
After receiving his B.S. in Mechanical Engineering in 2007, John interned in the summer at
the Johns Hopkins University Applied Physics Lab, where he realized (belatedly) that he
wanted to be a computer science major. In the fall of 2007, John began his doctoral degree in
Mechanical Engineering under the direction of Dr. Gregory Buckner. He continues to run,
iv
ACKNOWLEDGMENTS
I would like to thank Dr. Gregory Buckner for giving me with the opportunity and
freedom to pursue my interests. He supported me throughout the process, allowed me to
teach a class, and always pushed me to be my best. If I ever become a professor, it will
largely be due to his guidance and the insistence that he has the best job in the world.
I would like to thank my doctoral committee members: Dr. Scott Ferguson, Dr. Paul
Ro, and Dr. Ralph Smith. I truly have the best committee (maybe second to Jennifer
Hannen’s committee) and appreciate everyone’s guidance. Not only are they outstanding
committee members but also outstanding teachers, and their classes heavily influenced my
research and my career.
I thank all members of the Electromechanics Research Lab: J.P. Lien, Jennifer
Hannen, Qiaoyin Yang, Michael Mattson, and especially Shaphan Jernigan, Brian Owen, and
Andy Richards, who have helped me along the way. I am deeply indebted to Brian Owen,
who has bailed me out more times than I like to admit and never once complained when I
asked for a diagram. I am also sincerely grateful to Arun Veeramani, who was the ideal role
model early in my graduate career and showed me what hard work really is.
Above all I would like to thank my parents and my brothers, who always supported
me whenever I had a (supposedly) great idea. My parents pushed me to pursue what I love
and provided guidance along the way. My older brother Charlie never complained about
v
TABLE OF CONTENTS
LIST OF TABLES ... x
LIST OF FIGURES ... xi
Chapter 1. Introduction ... 1
1.1 Motivation ... 1
1.2 Commercial ablation catheters ... 4
1.3 Overview of the SMA actuated robotic catheter ... 6
1.4 Prior Work ... 10
1.4.1 Modeling and control of SMAs ... 10
1.4.2 Optimization of SMAs ... 11
1.5 Research objectives ... 12
1.6 Dissertation outline ... 13
Chapter 2. Flexible Catheter Kinematics ... 16
2.1 Introduction ... 16
2.2 Coordinate transformations for a single-segment catheter ... 19
2.2.1 Transformation from Cartesian to generalized coordinates ... 20
2.2.2 Transformation from generalized to Cartesian coordinates ... 24
2.3 Coordinate transformations for a two-segment catheter ... 26
2.3.1 Transformation from generalized to Cartesian coordinates ... 28
2.3.2 Transformation from Cartesian to generalized coordinates ... 30
vi
2.4.1 Distal location (catheter tip) ... 32
2.4.2.1 Solution using conjugate gradient algorithm ... 34
2.4.2.2 Solution using genetic algorithms ... 35
2.4.2 Distal location (catheter tip) and direction ... 38
2.4.2.1 Solution using the conjugate gradient algorithm ... 40
2.4.2.2 Solution using genetic algorithms ... 41
Chapter 3. Finite Element Modeling of the SMA Actuated Robotic Catheter ... 43
3.1 Introduction ... 43
3.2 SMA constitutive model ... 45
3.2.1 COMSOL model... 51
3.2.2 Single-crystal model validation ... 53
3.2.3 Polycrystalline model validation ... 55
3.3 Single-tendon SMA actuator ... 59
3.3.1 Circular arc bending model ... 60
3.3.2 COMSOL model... 62
3.3.3 Experimental validation ... 64
3.3.4 Sensitivity analysis ... 69
3.3.5 Parameter sweeps ... 70
3.4 Antagonistic SMA actuators ... 76
3.4.1 Circular arc bending model ... 79
3.4.2 COMSOL model... 79
vii
3.4.4 Sensitivity analysis ... 88
3.4.5 Monte Carlo analysis ... 89
3.4.6 Parameter sweeps ... 93
3.5 Summary ... 102
Chapter 4. Design Optimization of the Robotic Catheter ... 103
4.1 Introduction ... 103
4.2 General optimization problem... 103
4.2.1 Single-objective optimization... 104
4.2.2 Multi-objective optimization ... 105
4.3 Genetic algorithms ... 106
4.3.1 GA design overview ... 107
4.3.2 Single-objective GA implementation ... 110
4.3.3 Multi-objective GA implementation ... 111
4.4 Optimization of a single tendon catheter ... 112
4.4.1 Single-objective GA optimization results (single tendon) ... 115
4.4.2 MOGA optimization results (single tendon) ... 117
4.5 Optimization of catheter with antagonistic actuators ... 120
4.5.1 Single-objective GA optimization results (antagonistic tendons) ... 120
4.5.2 MOGA optimization results (antagonistic tendons) ... 122
4.6 Summary ... 124
Chapter 5. SMA Actuator Control ... 126
viii
5.2 Sliding mode control ... 127
5.3 Hysteretic recurrent neural networks ... 130
5.3.1 Network topology ... 131
5.3.2 Constrained weight optimization ... 134
5.4 SMC of a constant-stress SMA actuator ... 136
5.4.1 The plant ... 137
5.4.2 The model... 138
5.4.3 The observer ... 139
5.4.4 Control algorithm implementation ... 140
5.4.5 Experimental setup ... 144
5.4.6 Results ... 147
5.4.6.1 HRNN weight optimization ... 147
5.4.6.2 Simulation results... 149
5.4.6.3 Experimental results ... 151
5.5 SMC of a variable-stress actuator ... 153
5.5.1 Variable-stress response ... 154
5.5.2 Control algorithm implementation ... 156
5.5.3 Results ... 157
5.5.3.1 HRNN weight optimization ... 157
5.5.3.2 Simulation results... 160
5.5.4 Extension to antagonistic tendons ... 163
ix
Chapter 6. Conclusions ... 166
6.1 Future work ... 167
x
LIST OF TABLES
Table 3.1 SMA constitutive model parameters for the single-crystal model ... 54
Table 3.2 SMA constitutive model parameters for the polycrystalline model ... 56
Table 3.3 Single-tendon actuator model sensitivity to pre-strain ... 69
Table 3.4 Default values for single-tendon model perturbation ... 70
Table 3.5 Antagonistic actuation Model sensitivity to pre-strain ... 88
Table 3.6 Default values for antagonistic model perturbation ... 93
Table 4.1 Design variables and bounds ... 114
Table 4.2 Optimal design variables and objective function for the single-objective optimization of a single tendon ... 116
Table 4.3 Optimal design variables and objective function for the single-objective optimization of a single tendon ... 119
Table 4.4 Optimal design variables and objective function for the single-objective optimization of a antagonistic actuation ... 122
Table 4.5 Optimal design variables and objective functions for the multi-objective optimization of antagonistic actuation ... 124
xi
LIST OF FIGURES
Figure 1.1 Electrical differences in heart with normal sinus rhythm (a) and heart with atrial
fibrillation (b) [2]... 1
Figure 1.2 Incisions and excisions for Cox Maze I [8] ... 2
Figure 1.3 Lesions created using multiple discrete ablation points (shown in red) [13] ... 3
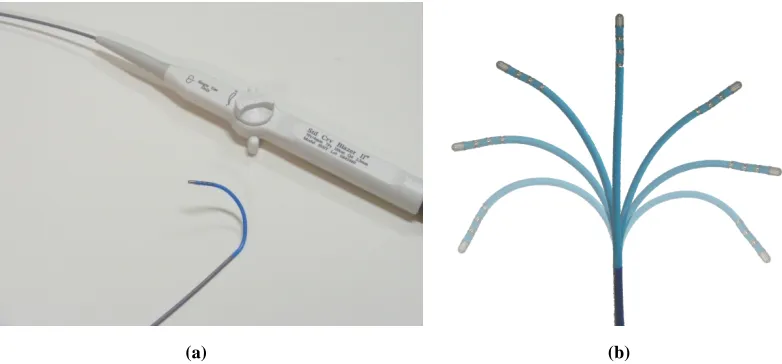
Figure 1.4 Conventional steerable ablation catheter: (a) catheter tip and handle; (b) planar bending ... 5
Figure 1.5 Commercially available robotic catheter systems: (a) Niobe II [15]; (b) Sensei system [16] ... 6
Figure 1.6 Robotic catheter prototype: (a) schematic; (b) photograph; (c) laser cut SMA actuator ... 7
Figure 1.7 Electrophysiology lab with robotic catheter system installed ... 8
Figure 1.8 Robotic catheter system components ... 9
Figure 2.1 Robotic catheters: (a) single bending segment; (b) two bending segments ... 16
Figure 2.2 Generalized coordinates for robotic catheter ... 17
Figure 2.3 Vertical coordinate system for a catheter with multiple segments ... 18
Figure 2.4 Time-lapsed photography of the catheter bending with circular arc references [19] ... 19
Figure 2.5 Geometry for catheter bending less than 90o ... 20
Figure 2.6 Geometry for catheter bending greater than 90o ... 22
Figure 2.7 Simulation of catheter motion: fixed distal segment (90o) and rotating proximal segment ... 26
xii
Figure 2.9 Two-segment catheter with coordinate systems and rotation ... 29
Figure 2.10 Multiple catheter solutions that reach a given 3D tip location ... 33
Figure 2.11 Flowchart for conjugate gradient algorithm ... 34
Figure 2.12 CG results for a reference distal location: (a) cost; (b) resulting geometry... 35
Figure 2.13 GA results for a reference distal location: (a) cost; (b) resulting geometry ... 37
Figure 2.14 Desired distal location and direction: (a) general case of a catheter located in the left atrium; (b) simplified case for the vertical catheter setup ... 38
Figure 2.15 CG results for a reference distal location and normal: (a) cost; (b) resulting geometry ... 41
Figure 2.16 GA results for a reference distal location and normal: (a) cost; (b) resulting geometry ... 42
Figure 3.1 Flexible beam actuated by SMA: (a) single actuator case; (b) antagonistic actuator case ... 44
Figure 3.2 Thermo-mechanical coupling of SMA crystalline phases ... 46
Figure 3.3 Stress-strain response of a SMA actuator attached to a flexible beam ... 47
Figure 3.4 Effects of the SMA model parameters that govern the phase fraction transition probabilities ... 49
Figure 3.5 Stress-strain validation for a the single-crystal model: (a) 24 oC; (b) 45 oC; (c) 75 o C; (d) 95 oC ... 55
Figure 3.6 Stress-strain validation for a the polycrystalline model (N=5): (a) 24 oC; (b) 45 oC; (c) 75 oC; (d) 95 oC ... 57
Figure 3.7 Stress-strain validation for a the polycrystalline model (N=25): (a) 24 oC; (b) 45 o C; (c) 75 oC; (d) 95 oC ... 58
Figure 3.8 Stress-strain validation for a the polycrystalline model (N=50): (a) 24 oC; (b) 45 o C; (c) 75 oC; (d) 95 oC ... 59
xiii
Figure 3.10 Experimental test rig for bending model validation: (a) photograph of the entire setup; (b) illustration of the collets showing slots to control actuator offset from the neutral axis ... 65
Figure 3.11 Comparison between the radius of curvature for the single-crystal model, polycrystalline model, and the experimental data for four actuator offsets: (a) 0.67 mm; (b) 1.05 mm; (c) 1.42 mm; (d) 1.92 mm ... 66
Figure 3.12 Comparison between the radius of curvature for the single-crystal model, polycrystalline model, and the experimental data for four pre-strains: (a) 4.0 %; (b) 4.5 %; (c) 5.0 %; (d) 5.5 % ... 68
Figure 3.13 Simulated bending model dependence on the elastic modulus of the beam: (a) radius of curvature; (b) stress-strain response... 71
Figure 3.14 Simulated bending model dependence on the radius of the beam: (a) radius of curvature; (b) stress-strain response ... 72
Figure 3.15 Simulated bending model dependence on the radius of the SMA actuator: (a) radius of curvature; (b) stress-strain response... 73
Figure 3.16 Simulated bending model dependence on the offset from the neutral axis: (a) radius of curvature; (b) stress-strain response... 73
Figure 3.17 Simulated bending model dependence on the pre-strain: (a) radius of curvature; (b) stress-strain response ... 75
Figure 3.18 Simulated bending model dependence on the thermal boundary condition: (a) radius of curvature; (b) stress-strain response; (c) final temperature distribution; (d) final distribution of austenite phase fraction ... 76
Figure 3.19 Three-dimensional bending decoupled into two planar bending problems ... 78
Figure 3.20 Simplified one-dimensional system for a flexible beam actuated by antagonistic SMA tendons ... 79
Figure 3.21 One-dimensional COMSOL model for antagonistic actuation ... 80
Figure 3.22 Antagonistic experimental test rig: (a) photograph; (b) schematic of the four different collets ... 83
xiv
Figure 3.24 Comparison between the radius of curvature for the single-crystal model, polycrystalline model, and the experimental data for four actuator offsets: (a) 0.8 mm; (b) 1.05 mm; (c) 1.42 mm; (d) 1.92 mm ... 85
Figure 3.25 Close-up of the radius of curvature for two offsets: (a) 1.42 mm; (b) 1.92 mm . 86
Figure 3.26 Comparison between the radius of curvature for the single-crystal model, polycrystalline model, and the experimental data for four pre-strains: (a) 2.3%; (b) 2.74%; (c) 3.62%; (d) 4.06% ... 87
Figure 3.27 Results of the Monte Carlo analysis: (a) distribution of pre-strain corresponding to one turn (0.45%); (b) distribution of pre-strain corresponding to 11 turns (5.0%); (c) distribution of radius of curvature for one turn (0.45% pre-strain); (d) distribution of radius of curvature for 11 turns (5.0% pre-strain) ... 91
Figure 3.28 Comparison between 95% confidence intervals predicted from Monte Carlo analysis and experimental data for two offset distances: (a) 1.05 mm; (b) 1.42 mm ... 92
Figure 3.29 Simulated bending model dependence on the elastic modulus of the beam: (a) radius of curvature; (b) strain response for the active actuator; (c) stress-strain response for the inactive actuator ... 94
Figure 3.30 Simulated bending model dependence on the radius of the beam: (a) radius of curvature; (b) stress-strain response for the active actuator; (c) stress-strain response for the inactive actuator ... 96
Figure 3.31 Simulated bending model dependence on the radius of the SMA actuator: (a) radius of curvature; (b) strain response for the active actuator; (c) stress-strain response for the inactive actuator ... 97
Figure 3.32 Simulated bending model dependence on the offset from the neutral axis: (a) radius of curvature; (b) strain response for the active actuator; (c) stress-strain response for the inactive actuator ... 98
Figure 3.33 Simulated bending model dependence on the pre-strain: (a) radius of curvature; (b) stress-strain response for the active actuator; (c) stress-strain response for the inactive actuator ... 100
xv
Figure 4.1 General flow chart of a GA... 109
Figure 4.2 Flow chart for single-objective GA ... 111
Figure 4.3 GA results for the single-objective optimization of a single SMA actuator: (a) average fitness of the population; (b) fitness of the best individual in the population ... 115
Figure 4.4. MOGA results for the single SMA actuator: (a) population number vs. generation; (b) evolution of the Pareto frontier; (c) final Pareto frontier ... 118
Figure 4.5 GA results for the single-objective optimization of antagonistic SMA actuation: (a) average fitness of the population; (b) fitness of the best individual in the population ... 121
Figure 4.6 MOGA results for antagonistic SMA actuation: (a) population number vs. generation; (b) evolution of the Pareto frontier; (c) final Pareto frontier ... 123
Figure 5.2 HRNN architecture ... 133
Figure 5.3 SMA tendon actuating a suspended mass ... 137
Figure 5.4 Constant-stress SMA tendon ... 138
Figure 5.5 Monotonicity of reference temperature: only one reference temperature achieves the desired displacement ... 141
Figure 5.6 Overview of control scheme ... 142
Figure 5.7 SMC for constant-stress SMA actuator ... 144
Figure 5.8 Experimental setup for measuring SMA hysteresis: (a) photograph; (b) schematic ... 145
Figure 5.9 Experimental training data acquired from the SMA test rig: (a) input current; (b) SMA surface temperature; (c) SMA displacement ... 146
Figure 5.10 Evolution of the augmented cost function and the error cost function ... 148
xvi
Figure 5.12 Simulation results for the SMC: (a) displacement; (b) input current; (c)
temperature ... 150
Figure 5.13 Close-up of the simulated response of the SMA actuator: (a) displacement; (b) temperature ... 151
Figure 5.14 Experimental tracking results for the constant-stress SMA actuator ... 152
Figure 5.15 Experimental input current for the constant-stress SMA actuator ... 153
Figure 5.16 Single SMA tendon attached to a flexible beam ... 154
Figure 5.17 Comparison of hysteresis plots for simulated data and HRNN prediction: (a) input current; (b) temperature; (c) recovered strain for constant-stress case; (d) recovered strain for variable-stress case ... 155
Figure 5.18 SMC for variable-stress SMA actuator ... 157
Figure 5.19 Simulated variable-stress data for HRNN training: (a) input current; (b) temperature; (c) bending angle... 158
Figure 5.20 Evolution of the augmented cost function and the error cost function ... 159
Figure 5.21 Comparison of hysteresis plots for simulated data and HRNN prediction: (a) ascending transitions; (b) descending transitions ... 160
Figure 5.22 Simulated response for the SMC: (a) bending angle; (b) input current ... 161
Figure 5.23 Comparison between the PID and SMC: (a) bending angle; (b) input current.. 162
Figure 5.24 Antagonistic SMA tendons attached to a flexible beam ... 163
Figure 5.25 Comparison between trained HRNN and experimental data for antagonistic SMA actuators ... 164
Figure 6.1 Cross section of a manually actuated catheter ... 168
Figure 6.2 Extending the SMA tendon length beyond the active segment of the catheter: (a) current prototypes where the SMA length is the constrained to the bending segment; (b) example of prototype with SMA tendons than extend into the rigid segment; (c) another example of longer SMA tendon ... 169
1
Chapter 1. Introduction
1.1 Motivation
Atrial fibrillation (AF) is the most common cardiac arrhythmia, afflicting over 2.2
million Americans with 160,000 new cases diagnosed each year [1]. The disease is
associated with shortness of breath, fatigue, chest pain, stroke, and even death. AF is
characterized by random electrical impulses in the atria, disrupting the heart’s normal
rhythm. The electrical pathways associated with normal sinus rhythm and atrial fibrillation
are shown in Figure 1.1.
(a) (b)
2
Treatment options for atrial fibrillation include pharmacological, surgical, and
electrophysiological approaches. Pharmacological approaches are usually the first choice of
treatment, but are frequently ineffective [3] or cause significant side effects [4]. Surgical
approaches are often highly invasive, requiring “open-chest” access and cardiopulmonary
bypass. The most popular treatment for AF was developed by James Cox [5]. Known as the
“Cox Maze” procedure, it involves multiple incisions through atrial tissue to block the
conduction of electrical signals (Figure 1.2). Refinements to the original Cox Maze
procedure (Cox Maze II and III) have made it the gold standard for treating AF [6], with
success rates as high as 96% [7].
3
Electrophysiological treatments for AF are performed with cardiac ablation catheters,
requiring only small incisions to gain peripheral vascular access. However, the efficacy of
catheter-based treatments varies widely, with an average success rate of only 52% [9].
Catheter-based approaches involve ablating atrial tissue to block electrical sources and
pathways, often near the pulmonary veins [10]. The catheter tip uses either radiofrequency
(RF) alternating currents or cryogenic agents to create lesions through the atrial wall.
Depending on the patient-specific physiology, the ablation process either targets specific
points (ectopic foci), creates linear lesions, or both. Effective lesion sets mimic those
specified in the Cox Maze procedure and must be both transmural (completely penetrating
the atrial tissue) and continuous. However, linear lesions are created using a point-by-point
method, Figure 1.3, often resulting in gaps that decrease the procedural efficacy [11].
Furthermore, this point-by-point method results in long procedure times (179 min average)
[12], exposing both the patient and medical staff to long durations of fluoroscopy.
4
The ideal treatment for AF would combine the minimally invasive attributes of
catheter-based approaches with the effectiveness of surgical approaches [14]. Such a
treatment can be realized via computer-assisted catheter manipulation [10]. By improving
navigability and utilizing a computer-controlled approach, the ablation catheter would be
better suited to reach difficult locations and create continuous, linear lesions. The result
would be improved success rates, reduced procedure times, and reduced exposure to
fluoroscopy for both the patient and the medical staff.
1.2 Commercial ablation catheters
Commercially available RF ablation catheters are manually steerable in a
bi-directional sense, as shown in Figure 1.4. These catheters are capable of tracing arcs in a
single plane. Their limited degrees of freedom require electrophysiologists to spend
significant time manually advancing, rotating, and bending the catheter tip to access the
target anatomy. Furthermore, continuous linear lesions are nearly impossible to achieve using
manually actuated catheters.
5
(a) (b)
Figure 1.4 Conventional steerable ablation catheter: (a) catheter tip and handle; (b) planar bending
Two robotic catheter systems are commercially available. The Niobe Magnetic
Navigation System from Sterotaxis (St. Louis, MO) uses two external permanent magnets to
control the catheter tip, Figure 1.5a. The primary disadvantages of the Niobe system are that
it requires significant capital investments and extensive modifications to the catheter lab. The
Sensei Robotic Catheter System from Hansen Medical (Mountain View, CA) uses pull-wires
attached to external motors to deflect the catheter tip. The system consists of a large diameter
sheath (14 Fr) with two degrees of freedom and a single controllable segment on the ablation
catheter, Figure 1.5b. The disadvantages of the Sensei system are its large diameter (making
it unsuitable for pediatric cases) and the additional space needed to externally actuate the
6
(a) (b)
Figure 1.5 Commercially available robotic catheter systems: (a) Niobe II [15]; (b) Sensei system [16]
1.3 Overview of the SMA actuated robotic catheter
Our robotic catheter uses shape memory alloys (SMAs) for internal actuation. SMAs
are novel “smart materials” capable of recovering large strains upon heating. This shape
memory effect makes them ideally suited for actuation applications requiring large energy
densities. Furthermore, their biocompatibility is well-suited to in-vivo actuation applications
like endocardial ablation.
The bending segments of our robotic catheter prototype feature three main
components: SMA actuators (tendons), an axially stiff, laterally compliant central structure,
and collets (Figure 1.6). The SMA tendons are either wires (FLEXINOL actuator wires from
Dynalloy Inc., Tustin, CA) or custom laser cut strips (fabricated by Memry GmbH, Weil am
Rhein, Germany) as shown in Figure 1.6c. The collets hold the SMA actuators a fixed
distance from the neutral axis of the central structure (beam), creating a moment as the
7
can vary considerably; hence, one goal of this dissertation is to determine optimal
configurations.
(a) (b)
(c)
Figure 1.6 Robotic catheter prototype: (a) schematic; (b) photograph; (c) laser cut SMA actuator
The robotic catheter system has a number of potentially significant advantages,
8
Additionally, the robotic catheter does not significantly alter the equipment or procedures of
conventional catheter labs. Whereas the Niobe and Sensei systems both remove the
electrophysiologist from the patient’s bedside, our robotic catheter system will be utilized in
a manner similar to conventional (manually-actuated) ablation procedures (Figure 1.7). The
forward motion of the catheter will still be controlled manually, providing tactile feedback to
the operator and reducing the risk of tissue perforations.
Figure 1.7 Electrophysiology lab with robotic catheter system installed
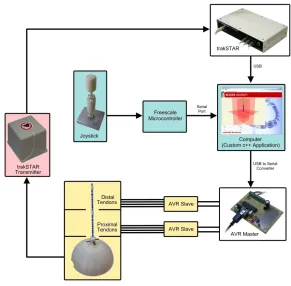
A schematic of the robotic catheter system components is shown in Figure 1.8. The
9
dissipated power (and internal temperature) of each SMA tendon. A master-slave AVR
system determines the PWM percentages for each tendon and modulates the currents by
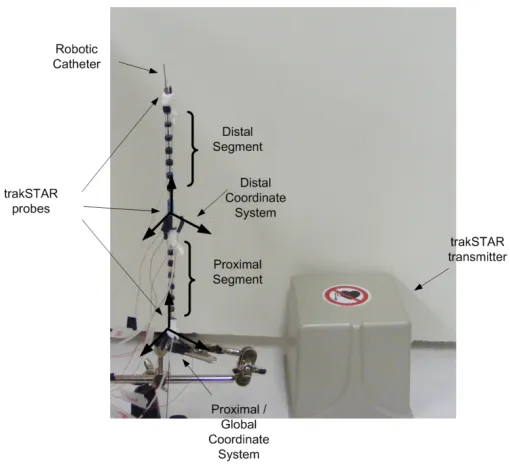
switching MOSFETs. For precise control of the catheter, accurate position measurements are
necessary. Currently, a trakSTAR 3D Magnetic Tracking System (Ascension Technology
Corporation, Burlington, VT) is used for this purpose. The trakSTAR system can
simultaneously monitor the 3D locations and orientations of up to four points on the catheter.
A joystick provides the tracking reference for navigation purposes. Finally, a custom C++
application ties together all of the sensors and actuators and provides a platform for real-time
control.
10
Operationally, the robotic catheter system is capable of set-point regulation or
closed-loop tracking of a joystick reference or pre-determined reference path. These operational
modes correspond to specific situations encountered in catheter ablation of AF. When a
specific point needs to be ablated, the computer-controlled robotic catheter will navigate to
that location. Closed-loop tracking of a joystick reference will be used for general navigation
and when the electrophysiologist wants direct control of the catheter. Closed-loop tracking of
a reference path will be necessary to create continuous lesions based on a subset of points
specified by the electrophysiologist.
1.4 Prior Work
The development of our robotic catheter utilizes and extends previous research
involving the modeling, optimization, and control of SMAs. An overview of this prior work
is presented next.
1.4.1 Modeling and control of SMAs
Shape memory alloys are unique materials with properties that exhibit nonlinear,
hysteretic dependence on stress and temperature. Because of their high energy densities,
impressive strain recovery characteristics, and biocompatibility, they have the potential to
revolutionize robotic actuation in biomedical applications. SMAs exhibit two unique and
useful characteristics: the super-elastic effect and the shape memory effect. To date,
biomedical applications have largely utilized the super-elastic properties of SMAs [17];
11
[18]. By contrast, most biomedical technologies utilizing the shape memory effect are still in
the research and development phases. This shape memory effect, which allows SMAs to
contract by over 4% upon heating, is currently being incorporated into cardiac catheters [19],
annuloplasty bands [20], and smart inhaler systems for aerosol drug delivery [21].
The precise control of SMA actuators is complicated by rate-dependent, hysteretic
dependencies of strain, stress and temperature. To address these technical challenges, both
model-based and heuristic control algorithms have been developed. Model based control
algorithms utilize both physical models [22] and empirical models [23]. Other approaches
have relied on neural networks to compensate for hysteresis [24]. Heuristic approaches such
as proportional-integral-derivative (PID) control have also been demonstrated [25].
1.4.2 Optimization of SMAs
While the published research has focused primarily on specific modeling and control
aspects of SMAs, little attention has been paid to the design optimization of SMA-actuated
systems. The design of SMA actuators is often iterative and non-intuitive due to the
material’s complex thermo-mechanical behavior. The limited work on SMA design
optimization has either focused on the material’s super-elastic behavior [26] or is based on
empirical models [27], [28]. In [26], the authors investigate the optimal hysteresis loop
shapes for SMA’s use as an energy dissipation device, which requires modifying the
12
In [27], the authors optimize the weight of a corrugated plate actuated by SMA
subject to certain performance constraints. In [28], the authors use an exponential empirical
model [30] within a finite element model for optimization of SMA spring actuators for
endoscopes. The geometry of the springs is optimized, but the authors fail to fully quantify
the actuator’s capabilities.
1.5 Research objectives
The research summarized in this dissertation advances the development of a robotic
RF ablation catheter by optimizing the design of shape memory alloy actuated structures. The
goal is to enhance specific performance metrics through optimization of critical design
variables. Additionally, new control schemes are developed to address inherent nonlinearities
and enable the use of SMA as an actuator in precision control applications. This optimized
catheter has the potential to revolutionize the treatment of AF and other therapies (i.e.
brachytherapy for the treatment of cancer [31]). Furthermore, the design optimization and
control methods presented here are applicable to a wide range of applications involving
SMA-actuated flexible structures.
The specific aims are:
• Develop the kinematics for single-segment and multi-segment robotic catheters in
13
• Develop and validate finite element models of flexible beams actuated by SMAs for
single actuators and antagonistic actuators.
• Present methods for optimizing SMA actuated flexible beams such as the robotic
ablation catheter.
• Develop control algorithms that compensate for the hysteresis inherent in SMA
actuators.
1.6 Dissertation outline
This dissertation is organized as follows:
Chapter 2: Flexible Catheter Kinematics
This chapter provides the framework for transforming the locations of catheter segments
between two coordinate systems. Modeling the catheter’s kinematics is important for
navigation and control purposes. As will be shown, the easiest way to describe the catheter
kinematics is in terms of bending angles; however, experimental position measurements are
normally made in Cartesian coordinates. Being able to efficiently transform between the two
coordinate systems is critical for real-time control. Furthermore, it is necessary to understand
the workspace of the robotic catheter for surgical navigation and ablation purposes. This
chapter develops the transformations between the two coordinate systems for a
single-segment and a two-single-segment catheter. Additionally, the inverse kinematics and solutions are
14
Chapter 3: Finite Element Modeling of SMA Actuated Flexible Beams
This chapter develops the SMA constitutive model and bending mechanics for robotic
ablation catheters actuated by single SMA tendons and antagonistic SMA tendons. Accurate
models are essential to predicting the performance of robotic catheter designs. Veeramani
originally developed a single-crystal model of the robotic catheter [19]; here, the model is
incorporated into COMSOL Multiphysics Modeling and Simulation Software (COMSOL
Inc., Burlington, MA), a finite element software package. The bending model is simplified to
a one-dimensional problem that is validated experimentally. Additionally, a polycrystalline
model is implemented for the first time in COMSOL and experimentally validated.
Perturbation and sensitivity analyses are also presented.
Chapter 4: Design Optimization of the Robotic Catheter
The optimization of nonlinear, hysteretic materials such as SMAs is complex and
non-intuitive. By combining accurate, experimentally validated models with efficient
optimization algorithms, a simulation-based design strategy can be employed to reduce the
time spent on prototyping and experimentally evaluating iterative design concepts.
This chapter presents design optimization methods for the robotic catheter, including
single-objective and multi-objective optimization for single and antagonistic actuators. For
the single-objective optimization, the objective function to be minimized is the catheter’s
15
catheter’s radius of curvature and “pushability”. The optimal designs are found using genetic
algorithms.
Chapter 5: Control of the Robotic Catheter
Precise, real-time control of the robotic ablation catheter is necessary for procedural
efficacy. The success of the robotic catheter will be dependent on its ability to accurately
ablate locations and create continuous lesions. Both procedures require real-time control
algorithms that effectively compensate for hysteresis and are computationally efficient.
This chapter presents methods for controlling a single SMA actuator using hysteretic
recurrent neural networks (HRNNs). The case of a single SMA actuator under constant stress
is considered. The HRNN is used as the inverse model to provide a reference temperature
given a reference displacement. A sliding mode controller is then used on the heat transfer
model to drive the actual temperature to the reference temperature. While the actuator is
under constant stress, the extension to SMA actuators attached to a flexible beam is presented
with simulation results.
Chapter 6: Conclusion
Chapter 6 provides the conclusions and discusses possible future work. Extensions of
16
Chapter 2. Flexible Catheter Kinematics
2.1 Introduction
This chapter develops the kinematics and coordinate transformations that are
necessary for real-time control of a robotic ablation catheter. Two different systems are
considered: a single-segment catheter (Figure 2.1a) and a two-segment catheter (Figure 2.1b).
Cases involving more than two segments are simply extensions of the two-segment case.
(a) (b)
17
For robotic systems possessing multiple degrees of freedom (like the robotic ablation
catheter of Figure 1.6), it is important to succinctly describe the system kinematics.
Commercial measurement platforms such as the trakSTAR 3-D guidance system (Ascension
Technology Corp, Burlington, VT) are capable of real-time position monitoring in
three-dimensional Cartesian coordinates. For the robotic catheter, however, it is easier to design
and implement control algorithms using generalized bending coordinates (bending angle θ and orientation angle ϕ, Figure 2.2) for each catheter segment (since each possesses only two degrees of freedom). This chapter develops the transformations between the two
coordinate systems for a single-segment and a two-segment catheter. Additionally, the
inverse kinematics and solutions are presented.
18
When navigating a catheter within a human body, multiple coordinate systems are
necessary, including the moving coordinate systems (or frames) attached to each catheter
segment and the global (or fixed, inertial) coordinate system. To simplify the subsequent
derivations, a vertical setup for the robotic catheter is considered (Figure 2.3), where the
proximal and global coordinate systems are the same because the base of the catheter is
fixed.
Figure 2.3 Vertical coordinate system for a catheter with multiple segments
A single segment robotic catheter was originally designed and modeled by Veeramani
[19], [32]. He found that the catheter follows a circular arc bending model, Figure 2.4. In [3],
Ganji, et. al modeled the kinematics of a manually actuated, bi-directional catheter with a
19
experimental results, the authors in [3] validated the accuracy of the circular arc model and
the zero torsion (planar bending) assumption.
Figure 2.4 Time-lapsed photography of the catheter bending with circular arc references [19]
2.2 Coordinate transformations for a single-segment catheter
In this section, the coordinate transformations for a single-segment robotic catheter
are derived. These transformations will also be necessary for describing the geometry of
multi-segment robotic catheters. In Section 2.2.1, the transformation from experimental
measurements (in 3D Cartesian coordinates) to generalized coordinates is derived. This
transformation is important because control algorithms will be concerned with tracking errors
in generalized coordinates. In Section 2.2.2, the transformation from generalized to Cartesian
20
2.2.1 Transformation from Cartesian to generalized coordinates
Two different cases must be considered when transforming from 3D Cartesian
coordinates to 2D generalized coordinates: bending angles θ less than 90o and bending angles greater than 90o. For the case of a bending angle less than 90o, the geometry presented in Figure 2.5 is utilized.
Figure 2.5 Geometry for catheter bending less than 90o
The rotation angle is defined to be
atan2 y
x ϕ =
. (2.1)
While the bending angle θ is simply
atan z
b θ =
21 Furthermore,
a b+ =R, (2.3)
and
2 2
a= x +y . (2.4)
Combining the Euclidean norm
2 2 2
z +b =R , (2.5)
with (2.3) - (2.5) results in
(
)
22 2 2 2
z + R− x +y =R . (2.6)
Rearranging yields
2 2 2 2 2
2
x y z
R
x y
+ +
=
+ . (2.7)
Therefore,
(
)
2 2 2 2 2
atan atan 2 atan z b z R a
z x y
z x y
θ = = − + = − +
. (2.8)
22
(a) (b)
Figure 2.6 Geometry for catheter bending greater than 90o
The rotation angle remains
atan2 y
x ϕ =
. (2.9)
Defining the supplementary angle
o
180
α = −θ , (2.10)
leads to
atan z
b α =
, (2.11)
and the following relationships:
2 2 2
x +y =a , (2.12)
R b+ =a, (2.13)
23
2 2 2
z +b =R . (2.14)
Combining (2.13) and (2.14) provides
2 2 2 a z b a a +
= − . (2.15)
Substituting (2.15) into (2.11) yields
2 2 atan 2 z a z a a α = + −
. (2.16)
And from (2.12)
2 2 2 2 2
2 2 2 2
2 2 2
atan
2
2 atan
z
x y z
x y
x y
z x y
x y z
α = + + + − + + = + −
. (2.17)
Finally, the bending angle can be expressed as
2 2 2 2 2
2
atan z x y
x y z
θ π= − +
+ −
. (2.18)
In order to determine whether the bending angle is less than or greater than 90o, the following relationship is necessary. If the catheter is bending exactly 90o, then
2L z
π
24
where L is the length of the catheter. If the measured distance z 2L
π
≥ , then Equation (2.8) is
used to convert the measured (Cartesian) coordinates to generalized coordinates. If the
measured distance z 2L
π
< , then Equation (2.18) is used to convert the measured coordinates
to generalized coordinates. In summary, Equation (2.20) can be used to transform the
three-dimensional trakSTAR measurements to two-three-dimensional generalized coordinates.
(
)
2 2 2 2 2
2 2 2 2 2
atan2 2 2 atan if 2 2 atan if y x
z x y L
z
z x y
z x y L
z
x y z
ϕ π θ π π = + ≥ − + =
− + <
+ −
. (2.20)
2.2.2 Transformation from generalized to Cartesian coordinates
Calculating Cartesian coordinates from the generalized coordinates is straightforward
for both cases. For the case of o
90
θ ≤ , from Figure 2.5 it is obvious that
( )
sin
z=R θ . (2.21)
Furthermore, note the arc length relationship
L=Rθ, (2.22)
where L is again the length of the catheter. Therefore, knowing the length of the catheter
25
( )
sin L z θ θ= . (2.23)
It can also be shown that
( )
cos
x=a ϕ , (2.24)
and
( )
sin
y=a ϕ . (2.25)
Combining Equations (2.3) and (2.22) with the relationship
( )
cos
b=R θ , (2.26)
results in
( )
(
1 cos)
cos( )
L
x θ ϕ
θ
= − , (2.27)
and
( )
(
1 cos)
sin( )
L
y θ ϕ
θ
= − . (2.28)
For the case of o
90
θ > , the derivation is similar. The end result is:
(
)
sin
L
z π θ
π θ
= −
− , (2.29)
(
)
(
1 cos)
cos( )
L
x π θ ϕ
π θ
= − −
− , (2.30)
and
(
)
(
1 cos)
sin( )
L
y π θ ϕ
π θ
= − −
26
2.3 Coordinate transformations for a two-segment catheter
For a robotic catheter with multiple bending segments, the coordinate transformations
become more challenging. Figure 2.7 illustrates the motion of a 2-segment catheter with a
fixed distal segment (with respect to its own moving coordinate system) while the proximal
segment rotates. The combined motion of these segments is significantly different than that
of serial robotic manipulators, which rotate about 1 DOF revolute joints.
Figure 2.7 Simulation of catheter motion: fixed distal segment (90o) and rotating proximal segment
The inverse kinematics problem involves determining the proximal and distal angles
prox
θ , ϕprox, θdist, and ϕdist, given three simultaneous measurements: 0
[
0 0 0]
T
x y z
=
p ,
[
]
1 1 1 1
T
x y z
=
p , and 2
[
2 2 2]
T
x y z
=
p , corresponding to the Cartesian coordinates of the
27 following assumption is used: 0
[
0 0 0]
T =
p . A schematic showing these measurements
and the generalized coordinates is provided in Figure 2.8.
Figure 2.8 Two-segment catheter showing measurement vectors and generalized coordinates
In general, three coordinate systems are required to represent a two-segment catheter:
the proximal coordinate system (denoted ˆx), the distal coordinate system (denoted x%), and
the global coordinate system (denoted x). However, for the simplified vertical catheter setup
shown in Figure 2.3, only the first two coordinate systems are necessary since the proximal
28
2.3.1 Transformation from generalized to Cartesian coordinates
Given a set of four generalized coordinates θprox, ϕprox, θdist, and ϕdist, the Cartesian
coordinates of the proximal tip can be found using either Equations (2.23), (2.27), and (2.28)
or Equations (2.29), (2.30), and (2.31). For example, if the bending angle of the proximal
segment is less than 90o as determined by (2.19), its Cartesian coordinates are
( )
1 sin prox prox
L
z θ
θ
= , (2.32)
( )
(
)
( )
1 1 cos prox cos prox
prox L
x θ ϕ
θ
= − , (2.33)
and
( )
(
)
( )
1 1 cos prox sin prox
prox L
y θ ϕ
θ
= − . (2.34)
Equations (2.32) - (2.34) are expressed in global coordinates since the global
coordinate system is the same as the proximal coordinate system. For the distal segment, the
tip coordinates are computed with respect to the distal coordinate system using either
Equations (2.23), (2.27), and (2.28) or Equations (2.29), (2.30), and (2.31). For example, if
the distal bending angle is also less than 90o as determined by (2.19), the tip coordinates are
( )
2 sin dist dist
L
z θ
θ
=
% , (2.35)
( )
(
)
( )
2 1 cos dist cos dist
dist L
x θ ϕ
θ
= −
29 and
( )
(
)
( )
2 1 cos dist sin dist
dist L
y θ ϕ
θ
= −
% . (2.37)
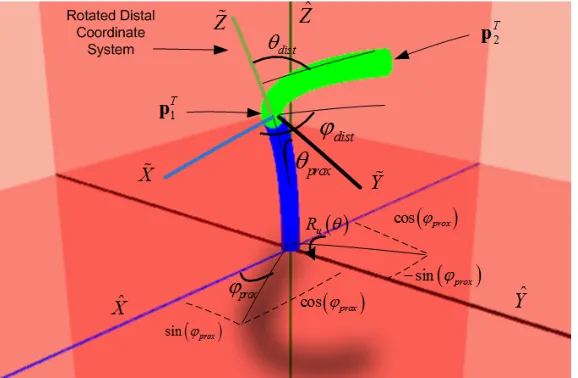
These distal tip coordinates can be transformed to the global coordinate system (also
the proximal coordinate system for the simplified vertical catheter setup). A schematic of the
coordinate systems and associated rotations is provided in Figure 2.9.
Figure 2.9 Two-segment catheter with coordinate systems and rotation
The normalized location of the proximal segment in the X −Y plane is
( )
( )
1 cos sin 0
T
prox prox
ϕ ϕ
=
u . To transform the distal coordinates to the global
30
( )
( )
(
( )
)
( )
( ) ( )
(
( )
)
( ) ( )
( ) ( )
(
( )
)
( )
(
( )
)
( ) ( ) ( )
( ) ( )
( ) ( )
( )
2 2s 1 c c s c 1 c c s
s c 1 c c 1 c c s s
c s s s c
prox
prox prox prox prox prox prox prox prox prox prox prox prox prox prox prox prox
prox prox prox prox prox
θ ϕ θ θ ϕ ϕ θ ϕ θ ϕ ϕ θ ϕ θ θ ϕ θ ϕ θ ϕ θ θ = − + − − − − − + − − u R . (2.38)
In (2.38), c
( )
refers to cos( )
, and s( )
refers to sin( )
. Using the above matrix,the Cartesian coordinates in the distal coordinate system ( 2
[
2 2 2]
T
x y z
=
p% % % % ) can be
transformed to the global coordinate system
( )
2 = +1 u θprox 2
p p R p% , (2.39)
where 2
[
2 2 2]
T
x y z
=
p and 1
[
1 1 1]
T
x y z
=
p .
2.3.2 Transformation from Cartesian to generalized coordinates
Since measurements are made in Cartesian coordinates using the trakSTAR system,
the reverse transformation (from Cartesian to generalized coordinates) is important. Given a
pair of measurements p1T =
[
x1 y1 z1]
and pT2 =[
x2 y2 z2]
and assuming[
]
0 0 0 0
T =
p , the proximal angles can immediately be found from either Equations (2.1)
and (2.8) or Equations (2.9) and (2.18). For example, if the proximal tip angle is less than
90o, the angles are
1 1 atan2 prox y x ϕ =
31 and
(
)
2 2 1 1 1 2 2 2 1 1 1
2 atan
prox
z x y
z x y
θ = +
− +
. (2.41)
The distal measurement is then transformed to its own coordinate system,
[
]
( )
1(
)
2 x2 y2 z2 θprox 2 1
−
= = u +
p% % % % R p p . (2.42)
Finally, the angles are found from either Equations (2.1) and (2.8) or Equations (2.9)
and (2.18). For example, if the distal tip angle is less than 90o, the angles are
2 2 atan2 dist y x ϕ =
, (2.43)
and
(
)
2 2 2 2 2 2 2 2 2 2 2
2 atan
dist
z x y
z x y
θ = + − + % % % % %
% . (2.44)
Equations (2.40) - (2.44) are important for transforming measurements to the
generalized coordinates for control algorithms. The above results can be extended to more
than two segments by transforming the coordinate systems one segment at a time. As noted, a
further transformation from the proximal coordinate system to the global coordinate system
will be necessary if the catheter is moving through open space, or if the global coordinate
32
2.4 Inverse kinematics
As noted in Chapter 1, the robotic catheter has three operating modes: closed-loop
tracking of a joystick reference, set-point regulation, and closed-loop path following. In the
case of set-point regulation, accurately transforming catheter measurements to variables used
in control algorithms is critical. If the proximal and distal references are known, then the
solution is consistent and Equations (2.40) - (2.44) can be used to calculate the generalized
coordinates. For certain ablation procedures, however, it is only necessary to measure,
transform, and control the distal location (the catheter tip). A solution to this case is
presented in Section 2.4.1. In Section 2.4.2, a case involving a distal measurement and a
direction normal to a surface (for example, to the tissue being ablated) is presented. In both
cases, solutions are derived using the conjugate gradient algorithm [33] and genetic
algorithms.
2.4.1 Distal location (catheter tip)
Consider the case where the desired reference location (associated with the catheter
tip) is 2, 2, 2, 2,
T
ref = x ref y ref z ref
p . The goal is to minimize the error between the measured
tip location 2
[
2 2 2]
T
x y z
=
p and the reference:
( )
2,ref = +1 u θprox 2
33
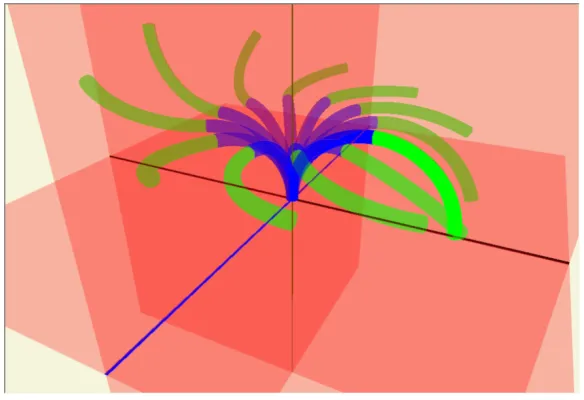
The vector equation (2.45) provides three equations (x2,ref =x2,y2,ref =y2, and z2,ref =z2)
with four unknowns (the generalized coordinates θprox, ϕprox, θdist, and ϕdist). Therefore, multiple solutions exist, as shown in Figure 2.10.
Figure 2.10 Multiple catheter solutions that reach a given 3D tip location
Equation (2.45) is a system of nonlinear equations that can be solved using any
number of numerical optimization algorithms. Since multiple solutions exist, an additional
criterion (namely minimizing catheter stress in terms of bending angle) is added. Therefore,
the solution to (2.45) is the minimum of the cost function
( )
(
)
(
)
(
(
( )
)
)
2 22, 1 2 2, 1 2
T
ref prox ref prox prox dist
J =γ p − p +Ru θ p% p − p +Ru θ p% +θ +θ , (2.46)
34
2.4.2.1 Solution using conjugate gradient algorithm
The conjugate gradient (CG) algorithm is best known for its efficiency in solving
matrix equations. However, the algorithm may also be used to minimize nonlinear equations.
Given an initial guess q0 = θ0prox ϕprox0 θdist0 ϕdist0 , the initial search direction is
( )
0 0
J
= −∇
d q . For a given convergence tolerance ε , the algorithm proceeds as follows in Figure 2.11.
Figure 2.11 Flowchart for conjugate gradient algorithm
To demonstrate this algorithm, it is assumed that each catheter segment has unit
35
set to 10-4, and the weighting parameter γ is initialized to 50. From a starting point of
[
]
0
0 0 0 0T
=
q , the cost at each iteration is shown in Figure 2.12a. After 190 iterations,
the minimum is q*= 60.12o 45.03o 36.07o 44.8oT, resulting in a catheter tip location
of 2
[
1.02 1.02 1.03]
T =
p , as shown in Figure 2.12b. The final cost is 1.57. The 190
iterations took 0.047 seconds on a 2.83 GHz processor.
(a) (b)
Figure 2.12 CG results for a reference distal location: (a) cost; (b) resulting geometry
2.4.2.2 Solution using genetic algorithms
While the conjugate gradient algorithm can be reasonably efficient (as demonstrated
in the previous section), global optimization is not guaranteed. In order to overcome some of
these limitations and obviate the need for gradient computations, an optimal solution can be
36
randomly initialized. At each iteration, the “fittest” individuals (as measured by the lowest
cost function (2.46)) are evolved using a crossover operation and a mutation operation. The
crossover rate is 60% and the probability of mutation is 40%. While the mutation rate is high
[34], it increases the likelihood of finding a global optimum. In the crossover operation, two
individuals (parents) are combined to produce two new individuals (offspring) according to
(
)
(
)
1 1 1 1k k k
s v w
k k k
t v w
r r r r + + = + − = − +
q q q
q q q , (2.47)
where qkv is the th
v individual in the population at iteration k, and r is a random number
between 0 and 1. The two new offspring replace the two least fit individuals in the
population. In the mutation operation, one of the parameters in the parent is randomly
replaced to produce a child. For example,
1
, , ,
k k k k
s θprox v ϕprox v θdist ϕdist v
+
=
q % , (2.48)
where θ%dist is a random value. The child again replaces one of the least fit individuals in the population. A more detailed description of genetic algorithms is provided in Chapter 4.
To demonstrate the approach, the same reference location is used, 2,
[
1 1 1]
T ref =
p .
The weighting parameter γ is again set to 50. The initial population consists of 100 individuals, and the convergence criterion is an iteration limit of 2000. While this number
may seem disproportionately large compared to the CG algorithm, the CG requires additional
37
inconclusive. After 2000 iterations, the minimum is
* o o o o
60.92 31.26 52.15 82.67 T
=
q , which produces a distal location of
[
]
2 0.99 1.00 1.01
T =
p . The cost of the fittest individual in the population is shown in
Figure 2.13a, and the final geometry of the solution is shown in Figure 2.13b.
(a) (b)
Figure 2.13 GA results for a reference distal location: (a) cost; (b) resulting geometry
Figure 2.13a shows that the genetic algorithm quickly finds a suitable solution in
approximately the first 50 iterations. The results indicate that an additional stopping criterion
based on the cost function or the gradient of the cost function needs to be introduced. These
results demonstrate the suitability of the GA for finding solutions to the inverse kinematics.
The 2000 iterations took 0.328 seconds on a 2.83 GHz processor, which is 0.16 ms per
38
2.4.2 Distal location (catheter tip) and direction
Certain situations will not only require an exact distal tip location but also that the
catheter tip be oriented in a specific direction. For example, the catheter tip may have to be
oriented precisely normal to the tissue being ablated, Figure 2.14a. In this case, the catheter
tip will have an orientation (unit vector) in the reverse direction of the tissue normal. A
simplified example for the vertical catheter setup is shown in Figure 2.14b.
(a) (b)
Figure 2.14 Desired distal location and direction: (a) general case of a catheter located in the left atrium; (b) simplified case for the vertical catheter setup
From Figure 2.14b the generalized coordinates are
0 0 0 0
90 0 90 0
prox prox dist dist
θ ϕ θ ϕ
= =
![Figure 1.1 Electrical differences in heart with normal sinus rhythm (a) and heart with atrial fibrillation (b) [2]](https://thumb-us.123doks.com/thumbv2/123dok_us/1343259.1167204/19.612.158.469.356.605/figure-electrical-differences-heart-normal-rhythm-atrial-fibrillation.webp)
![Figure 1.3 Lesions created using multiple discrete ablation points (shown in red) [13]](https://thumb-us.123doks.com/thumbv2/123dok_us/1343259.1167204/21.612.171.456.451.604/figure-lesions-created-using-multiple-discrete-ablation-points.webp)