Factors predicting early improvement in semen parameters following varicocele surgery
6
0
0
Full text
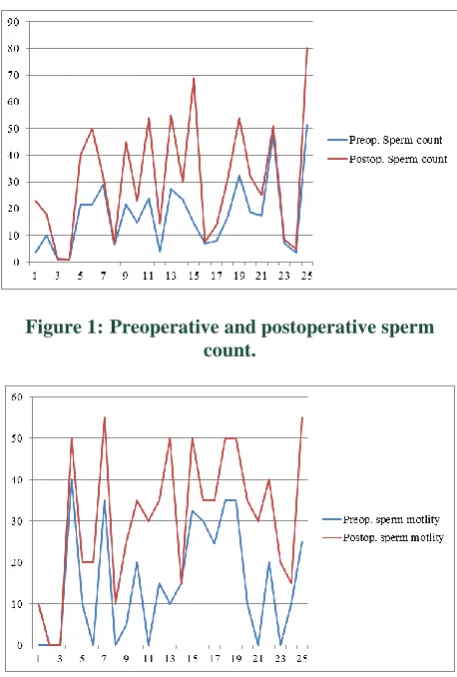
Figure
Related documents