FROM ORAL TO NASAL
Aim: This study was undertaken to assess the possibility of redirect-ing the growth pattern by usredirect-ing rapid maxillary expansion and a light-force chin cup for a short period of time, with limited patient cooperation, during the pre-growth and growth-spurt stages. Meth-ods: The study included a series of 60 patients, 24 males and 36 females from 7 to 14 years of age, with crossbite or midfacial defi-ciencies. Treatment involved wearing a chin cup 24 hours a day to force mouth closure during rapid maxillary expansion activation, which was 2 turns per day to rapidly expand the midpalatal suture and enhance nasal breathing. Lateral cephalograms and intraoral and facial photographs were taken 2 years before treatment, at the time of rapid maxillary expansion, 3 weeks following rapid maxillary expansion activation, 3 months after the cessation of rapid maxillary expansion activation, and 1 to 3 years post–rapid maxillary expansion activation. Results: Despite the severity, the crossbite would always improve within 21 days following rapid maxillary expansion activa-tion. The cephalograms and photographs demonstrated forward movement of the nasal bridge and maxilla, with backward rotation of the mandible. The bite depth remained nearly the same as pretreat-ment. Conclusion: The results suggested that 24 hours of light-force chin cup wear, while expanding the midpalatal suture, is the major factor to force mouth closure and enhance nasal breathing. As a result, there is advancement of the maxilla, avoidance of tongue encroachment upon the mandible, and deceleration of horizontal mandibular growth. World J Orthod 2006;7:236–253 (print version).
T
raditionally, orthodontists haveconcen-trated on treating Class III patients as primarily mandibular prognathism and have largely ignored the maxilla. There is no question that relative maxillary defi-ciency is part of the picture, creating an upward and for ward rotation of the mandible on closure. However, rapid max-illary expansion (RME) does have a salu-tary effect. One can redirect, but not
retard, growth by changing an individual’s breathing pattern from an oral to a nasal
approach.1,2 Most Class III and midfacial
deficient patients are mouth breathers. This results in excessive lingual inclination of the mandibular incisors and labial incli-nation of the maxillary incisors. The tongue always lies on the floor of the mouth and forces mandibular growth
faster than maxillary growth.3–6 Several
1Private practice of Orthodontics,
San Gabriel, California, USA. CORRESPONDENCE Dr Jenny Chen Chung 1728 S San Gabriel Boulevard San Gabriel, CA 91776 USA
studies have demonstrated that condylar growth can be influenced only to a limited
degree.3–6 The earlier the clinician starts
to bend the mandible downward and back-ward, the greater the chance of increasing mandibular growth horizontally, unless mandibular growth can continue to be held steady. Once the force is removed, the
growth behavior resumes.7,8 Maxillary
retrusion is considered responsible for the malocclusion; the aim has been to advance the maxilla by or thopedic
means.9,10 Most studies have used
pro-tractors to protract the maxilla, but these have also rotated the mandible in a back-ward and downback-ward direction and increased the lower facial height and bite depth. This result is not favorable in
high-angle cases.11–14 Sutural growth seems
more adaptable than condylar growth. Redirecting the growth pattern should work better than retarding mandibular growth. The development of the sutural system surrounding the maxillary complex implies that skeletal changes can be best obtained at a young age, when the growth activity of the suture in the pterygoid
region is still high.15–23 The purpose of this
study was to explore optimal treatment methods and timing in Class III midfacial deficiencies, mandibular prognathism, and high-angle Class III cases, to test this hypothesis.
MATERIAL AND METHODS
The study sample included 24 males and 36 females of Chinese ethnic origin, from 7 to 14 years of age, with moderate to severe midfacial deficiencies, maxillary
retrognathism, mandibular prognathism, and/or a combination of the 3. All pat-ients were from the author’s private prac-tice. All subjects were treated with similar mechanotherapy and followed for more than 1 year. Four sets of photographs and cephalograms were taken: Pre-RME activation; 21 days following RME activa-tion; 3 months after the end of RME acti-vation; and more than 1 year after the end of RME activation.
The RME method used in all patients is as follows:
Initial stage
1. Fabricate and place rapid maxillary expander by placing expansion screw as close to the maxillary first molar area as possible, to enhance the mid-palatal suture opening at the palatine area (Fig 1).
2. Activate RME by 2 turns per day for 21 days, while wearing chin cup at least 21 hours per day to force mouth closure and enhance nasal breathing (Fig 2).
After the end of RME activation
1. Secure maxillary expansion jackscrew by tying with 0.014-inch ligature wire. 2. Encourage the patient to wear chin
cup at least 12 hours per day to enhance mouth closure.
3. Enforce nasal exhalation exercises. Two fingers were used to maintain clo-sure of the mouth, taking a deep breath, and then blowing air through the nostrils for as long as possible.
of RME activation
Note: If patients are still mouth-breathers after the RME phase, the chin cup needs to be worn as much as possible until patients sleep with mouths closed. Allow a grace period of 1 week from chin cup wear. During this time, parents need to monitor whether the child is sleeping with the mouth open. If this is the case, night-time chin cup wear is critical. If there is mouth closure during sleep, chin cup use is no longer required.
1. Check the photographs and cephalo-grams to decide when to remove RME and allow tongue approximation with the palate.
2. If the patient has a deep overbite, a bite block should be placed.
3. If the maxillary lateral incisors are not aligned, a maxillary lingual fixed appli-ance should be placed. Minor adjust-ments are made at 2- to 3-month intervals.
4. If the space between the maxillary incisors is closed and the maxillary arch is too wide to coordinate with the mandibular arch, make the following adjustments:
• Turn the RME jackscrew back 5 to 6 turns for the first day, then 2 turns per day for 7 days.
• Wear chin cup 21 hours per day for 7 days while performing this procedure to force mouth closure and advance the maxilla.
• Remove RME.
Pre–phase II stage
Patients need to be seen every 6 months to check body height to monitor the growth spurt for phase II treatment.
tographs and cephalograms demon-strated forward movement of the nasal bridge and maxilla, downward and back-ward rotation of the mandible, and upward and forward tipping of the palatal plane. The bite depth remained essen-tially the same as pretreatment. This is likely the result of full-time chin cup wear, which forced mouth closure and altered tongue posture to encroach on the RME and intrude the maxillary first molars and premolars. This could be the major factor in avoiding bite opening.
Three months after cessation of RME activation
Mouth closure, nasal breathing, and tongue posture help to intrude the RME, maxillary molars, and premolars. This resulted in decreasing the mandibular plane angle and advancing the maxilla. Mouth closure and lip posture are major factors in tipping the maxillary incisors lin-gually. In the majority of patients, the SN-palatal plane angle decreased slightly and the SN-occlusal plane angle increased slightly. This resulted in the downward and backward rotation of the mandible.
More than 1 year after cessation of RME activation
Most of the patients in the pre–growth spurt group had no posttreatment reten-tion. In the ensuing 1-year period, there were no crossbite relapses. The majority of the patients’ breathing patterns were altered, along with redirection of the facial pattern. In the growth-spurt group, the growth patterns were redirected and the breathing patterns altered during the
Degrees
Fig 3 SNA changes (degrees) achieved over the course of the study.
Degrees
Fig 4 SNB changes (degrees) achieved over the course of the study. 20 18 16 14 12 10 8 6 4 2 0 No. of patients –1 0 1 2 3 4 5 6 Degrees 3 weeks 3 months 1 year 2 years 7 8 9
Fig 5 ANB changes (degrees) achieved over the course of the study. 20 18 16 14 12 10 8 6 4 2 0 No. of patients –5 –4 –3 –2 –1 0 1 2 Degrees 3 weeks 3 months 1 year 2 years 3 4 5 6 7
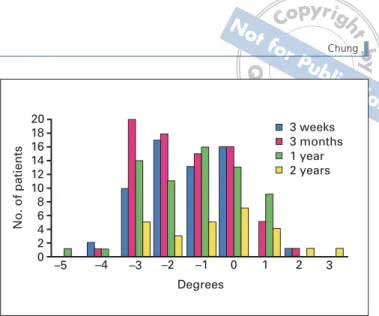
Fig 6 Sn-GoGn changes (degrees) achieved over the course of the study.
20 18 16 14 12 10 8 6 4 2 0 No. of patients –5 –4 –3 –2 –1 0 1 2 Degrees 3 weeks 3 months 1 year 2 years 3 4 5 6 7 8 –6 –7
Fig 7 SN-palatal plane changes (degrees) achieved over the course of the study.
20 18 16 14 12 10 8 6 4 2 0 No. of patients –5 –4 –3 –2 –1 0 1 2 Degrees 3 weeks 3 months 1 year 2 years 3 4 5 6 7 –6 –7
Fig 8 SN-occlusal plane changes (degrees) achieved over the course of the study.
Millimeters
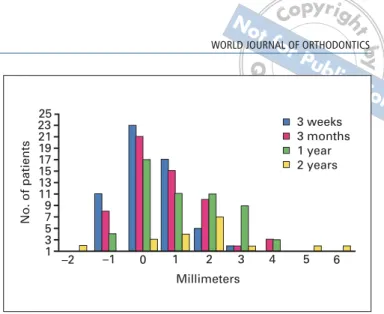
Fig 9 Wits changes (mm) achieved over the course of the study.
Millimeters
Fig 10 Go-menton changes (mm) achieved over the course of the study. 20 18 16 14 12 10 8 6 4 2 0 No. of patients –6 –5 –4 –3 –2 –1 0 1 Degrees 3 weeks 3 months 1 year 2 years 2 3 4 5 –7 –9
Fig 11 Gonial angle changes (degrees) achieved over the course of the study.
of therapy and up to 3 years following the cessation of RME activation. The photos and cephalograms demonstrate that the breathing pattern changed from an oral to a nasal approach, and the growth pat-tern was also redirected.
PATIENT K.W.
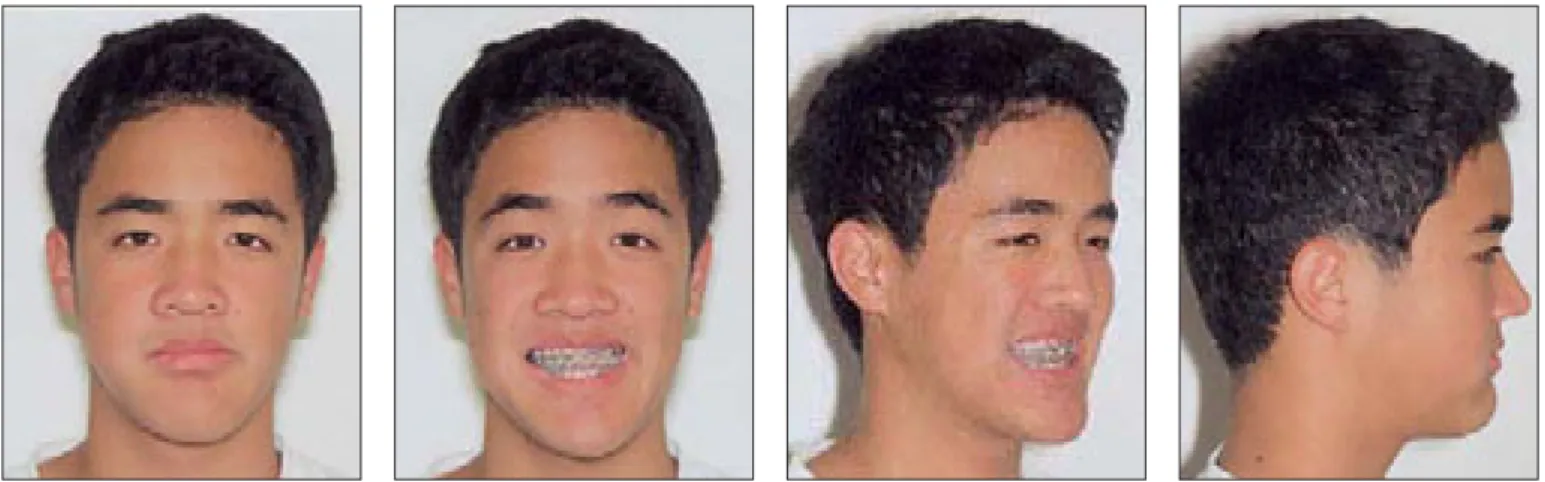
This patient had a Class III malocclusion with anterior and posterior crossbite. Measurements were: Wits, –12 mm; SNA, 75 degrees; ANB, –7.5 degrees; IMPA, 72 degrees; reverse overjet, –4 mm in centric occlusion and –1 mm in centric relation. This indicated the presence of maxillary retrognathism and mandibular prog-nathism. There were 9 congenitally miss-ing teeth: 4 third molars, 4 second premo-lars, and the maxillary left first premolar. Figures 12 to 24 show the pretreatment, treatment, posttreatment intraoral, extra-oral, and radiographic views (complete cephalometric tracings for this article are available on the Journal website at www.quintpub.com).
Figures 12a, 12b, and 13 show that there was no RME and chin cup treat-ment during the control period of 2 years. The crossbite and mouth-breathing pat-tern remained; the mandible grew for-ward and downfor-ward, which enhanced the concave facial pattern.
Figure 12c reveals that the maxilla and nasal bridge were advanced, the mandible rotated backward and down-ward, and the crossbite corrected during the 22 days of RME and chin cup treat-ment. Figures 12d, 12e, and 14 show that the growth pattern was altered with mouth closure and nasal breathing dur-ing the 3-year period followdur-ing the RME treatment.
tern existed until shortly before RME. The mandible was rotated for ward and upward prior to treatment, which enhanced the concave facial pattern.
Figure 25c shows that the maxilla and nasal bridge were advanced, the mandible rotated backward and down-ward, and the crossbite corrected in 22 days of RME. Figures 25c, 25d, and 27 show that the growth pattern was altered with mouth closure and nasal breathing by 3 years after the RME. There was no other treatment, only RME. The teeth aligned automatically, and a good over-bite and overjet with an acceptable facial profile was achieved prior to the patient’s growth spurt (Figs 28 to 35).
PATIENT E.W.
This patient had a Class III malocclusion with maxillary retrognathism, a deep over-bite combined with anterior and posterior crossbite; both centric occlusion and cen-tric relation were –5 mm reverse overjet.
Figures 36a, 36b, and 37 show that there was no RME and chin cup treat-ment in the 1-year control period. The crossbite and mouth-breathing pattern remained after this period. The mandible grew forward and downward and the maxilla grew slightly for ward, which resulted in a more concave facial pattern. Figures 36c and 38 show that the growth pattern was altered with mouth clo-sure and nasal breathing at 4 years follow-ing RME treatment. Although the patient’s mandible still grew faster than the maxilla, with a very strong pogonion, her facial pro-file and occlusion are acceptable.
Records for an additional case (Figs W-1 to W-14) can be found on the WJO website at www.quintpub.com.
a b c
Fig 12 (Cephalometric tracings web only) Patient K.W. (a) Two years pre-RME treatment. Age: 11 years 3 months. (b) Right before RME treat-ment. Age: 13 years 3 months. (c)
Twenty-two days following RME activa-tion. Age: 13 years 4 months. (d)Four months after the end of RME activa-tion. Age: 14 years 8 months. (e) Thirty-four months after the end of RME acti-vation. Age: 16 years 1 month.
Fig 13 Patient K.W. Cephalometric composite of the 2 years pretreatment.
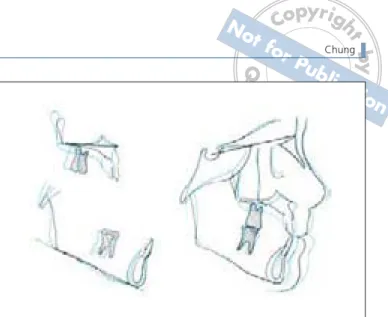
Fig 14 Patient K.W. Cephalometric composite of pretreat-ment (black), 22 days following RME activation (blue), and 34 months after the end of RME activation (purple).
Fig 15 Patient K.W. Two years before RME treatment. Age: 11 years 4 months. The frontal view was taken at centric relation and the profiles views were taken at centric occlusion.
Fig 17 Patient K.W. Twenty-two days following RME activation. Age: 13 years 4 months.
Fig 16 Patient K.W. Right before RME treatment. Age: 13 years 3 months.
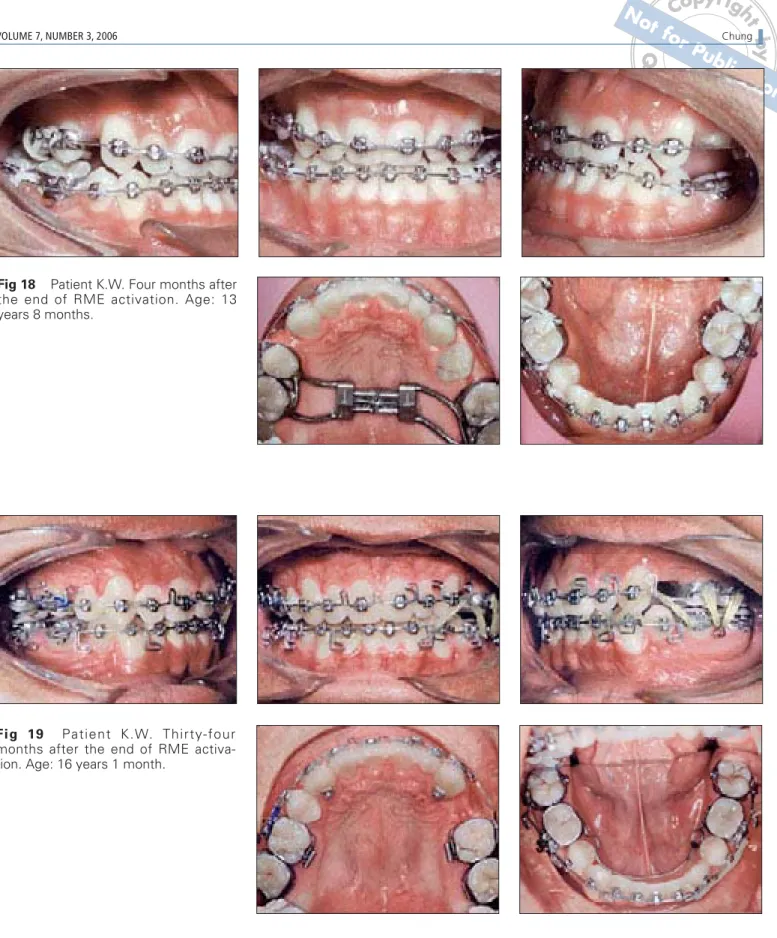
Fig 18 Patient K.W. Four months after the end of RME activation. Age: 13 years 8 months.
Fig 19 Patient K.W. Thirty-four months after the end of RME activa-tion. Age: 16 years 1 month.
Fig 20 Patient K.W. Two years before RME treatment. Age:11 years 4 months.
Fig 22 Patient K.W. Twenty-two days following RME activation. Age: 13 years 4 months.
Fig 23 Patient K.W. Four months after the end of RME activation. Age: 13 years 8 months.
a
c d
Fig 27 Patient V.S. Cephalometric composite of pre-RME treatment(black), 3 months after the end of RME activation (blue), 14 months after the end of RME activation (red), and 34 months after the end of RME activation(green).
Fig 28 Patient V.S. Two months before RME treatment, at centric rela-tion. Age: 9 years 2 months.
Fig 29 Patient V.S. Twenty-two days following RME activation. Age: 9 years 5 months.
Fig 30 Patient V.S. Three months after the end of RME activation. Age: 9 years 8 months.
Fig 31 Patient V.S. Thirty-five months after the end of RME activation. Age: 12 years 3 months.
Fig 32 Patient V.S. Two months before RME treatment. Age: 9 years 2 months.
Fig 33 Patient V.S. Twenty-two days following RME activation. Age: 9 years 5 months.
Fig 34 Patient V.S. Three months after the end of RME activation. Age: 9 years 8 months.
Fig 36 Patient E.W. (a)One and one-half years pre-RME treatment. Age: 9 years 5 months. (b)Seven months pre-RME treat-ment. Age: 10 years 5 months. (c)Forty-eight months after the end of RME activation. Age: 15 years 1 month.
Fig 37 Patient E.W. Cephalometric composite of 12 months preceding RME treatment, from age 9 years 5 months(black) to 10 year 5 months (blue). This demon-strated that the mandible was growing faster than the max-illa, and in a forward and upward direction.
Fig 38 Patient E.W. Cephalometric composite of 7 months pre-RME treatment(black), 39 months after the end of RME activation(red), and 48 months after the end of RME activa-tion(green). Both the nasal bone and the maxilla advanced. The SN-palatal, the SN-occlusal, and the mandibular planes remained nearly the same or increased slightly, as compared to the pre-RME angles.
Fig 39 Patient E.W. Seven months before RME treatment. Age: 10 years 5 months.
Fig 40 Patient E.W. Forty-eight months after the end of RME activa-tion. Age: 15 years 1 month.
Fig 41 Patient E.W. Seven months before RME treatment. Age 10 years, 5 months.
Fig 42 Patient E.W. Forty-eight months after the end of RME activation. Age: 15 years 1 month.
DISCUSSION
For a period of more than 3 years, the author has treated over 80 patients with mechanotherapy similar to that illus-trated here. Patient cooperation is the major factor in achieving the optimal result. Without chin cup wear during 21 hours per day during RME activation, the result could be disastrous (Figs W-15 to W-25 on the WJO website at www.quint-pub.com). Not only would the mandible be rotated backward, there would be no or slight advancement of the maxilla. This could result in an open bite. After the cessation of RME activation, the chin
cup still needs to be worn until there is mouth closure during sleep. Nasal breathing exercises should be enforced to enhance maxillary growth. The cases here illustrate 3 severely midfacial-defi-cient mouth breathers, with good chin cup use during RME activation. The mouths were closed, the nostrils were smaller, and nasal breathing was estab-lished. Balancing facial profile with a bet-ter dentoalveolar relationship was achieved. During the 1- to 2-year control periods of these 3 patients, pre-RME and chin cup treatment, the crossbites, mouth breathing, and facial growth pat-terns showed almost no change.
Fig W-2 Patient J.C. Twenty-one days following RME activation.
Fig W-4 Patient J.C. One year after the end of RME activation.
Fig W-3 Three months after the end of RME activation.
Fig W-6 Patient J.C. Pretreatment at centric occlusion.
Fig W-7 Patient J.C. 21 days following RME activation; RME was then secured by tying expansion screw with 0.014-inch ligature wire.
Fig W-8 Patient J.C. Three months after the end of RME activation. Appli-ance was then removed.
Fig W-9 Patient J.C. More than 1 year after the end of RME activation. Bite plate was placed to avoid nocturnal bruxism and bite collapse.
Fig W-10 Patient J.C. More than 1 year after the end of RME activation.
Fig W-11 Patient J.C. Pretreatment.
Fig W-12 Patient J.C. Twenty-one days following RME activation.
Fig W-13 Patient J.C. Three months after the end of RME activation.
Fig W-16 Patient X.Y. Cephalometric composite of pre-RME treatment and 21 days following pre-RME activation with-out wearing chin cup. There was no maxilla and nasal bone advancement. The mandible rotated downward and back-ward, with an enlarged open bite.
Fig W-17 Patient. X.Y. Pretreatment intraoral views.
Fig W-18 Patient X.Y. 21 days follow-ing RME activation, without wearfollow-ing chin cup. Maxillary first molars and pre-molars elongated, which resulted in a large open bite.
Fig W-20 Patient C.H. Two and one-half years after RME and protractor treatment.
Fig W-21 Patient C.H. Cephalometric composite of pre-treatment and 2.5 years following RME and protractor treat-ment, but no chin cup use. The bite was open, with the mandible rotated in a downward and backward direction. There is no midpalatal suture opening.
Fig W-22 Patient C.H. Pretreatment extraoral views.
Fig W-23 Patient C.H. Intraoral views at 2.5 years post-RME and protractor treatment. No suture opened, and the mandible rotated downward and back-ward, with a big open bite.
Fig W-24 Patient C.H. Pretreatment extraoral views.
tant factor to force mouth closure and enhance nasal breathing. Through the approach of encouraging nasal breathing to advance the maxilla, the patients' crossbites were corrected within 21 to 23 days. In addition, the case photos and radiographs demonstrated that the growth patterns were redirected and breathing patterns were altered to a nasal approach. These results were con-sistently maintained at more than 3 years posttreatment.
ACKNOWLEDGMENTS
I would like to thank Dr Tom Graber for inspiring me to s t a r t t re a t m e n t o f C l a s s I I I p a t i e n t s a t a pre–growth spurt age. I would also like to thank Mr Clyde Zeng for his assistance in the organization of this manuscript.
REFERENCES
1. Graber TM, Swain B. Current Orthodontic Con-cepts and Techniques. Philadelphia: Saunders, 1977:365–451.
2. Enlow DH. Handbook of Facial Growth. Phila-delphia: Saunders, 1975: 271–280. 3. Asano T. The effects of mandibular retractive
force on the growing rat mandible. Am J Orthod Dentofacial Orthop 1986;90:464–474. 4. Sugawara J, Asano T, Endo N, Mitani H.
Long-term effects of chincap therapy on skeletal pro-file in mandibular prognathism. Am J Orthod Dentofacial Orthop 1990;98:127–133. 5. Sakamoto T, Iwase I, Uka A, Nakamura S.
Roentgenocephalometric skeletal changes dur-ing and after chin cup treatment. Am J Orthod 1984;85:341–350.
6. Vardimon A, Graber TM, Voss L, Muller TP. Functional orthopedic magnetic appliance (FOMA) III—Modus operandi. Am J Orthod Dentofacial Orthop 1990;97:135–148.
mask therapy. Am J Orthod Dentofacial Orthop 2002;122:349–352.
11. Cate ART, Freeman E, Dickinson JB. Sutural development: Structure and its response to rapid expansion. Am J Orthod 1977;71:622–636. 12. Haas AJ. The treatment of maxillary deficiency
by opening the midpalatal suture. Angle Orthod 1965;35:200–217.
13. Haas AJ. Rapid expansion of the maxillary den-tal arch and nasal cavity by opening the mid-palatal suture. Angle Orthod 1961;31:73–90. 14. Haas AJ. Palatal expansion: Just the beginning
of dentofacial orthopedics. Am J Orthod 1970;57:219–255.
15. Mew JRC. Facial form, head posture and the protection of the pharyngeal space. In: McNa-mara JA, Ribbens KA, Raymond PH (eds). Clini-cal Alteration of the Growing Face. Ann Arbor: Michigan Monograph Craniofacial Series. Vol 14, 1983:179–191.
16. Pearson LE, Learson BL. Rapid maxillary expan-sion with incisor intruexpan-sion: A study of vertical control. Am J Orthod Dentofacial Orthop 1999; 115:576–582.
17. Wertz RA. Changes in nasal airflow incident to rapid maxillary expansion. Angle Orthod 1968; 38:1–11.
18. Akkaya S, Gulsen A, Taner-Sarisoy L, Balos B. Evaluation of the effects of maxillary expansion on the nasopharyngeal area. World J Orthod 2002;3:211–216.
19. Baccetti T, Franchi L. Treatment timing for rapid maxillary expansion. Angle Orthod 2001:71; 343–350.
20. Biederman W. Rapid correction of Class III mal-occlusion by midpalatal expansion. Am J Orthod 1973;63:47–55.
21. Timms DJ. Rapid Maxillary Expansion. Chicago: Quintessence, 1981:15–125.
22. Nazan K, Ceylanoglu C. Changes in lip, cheek, and tongue pressures after rapid maxillary expansion using a diaphragm pressure trans-ducer. Angle Orthod 2003;73:662–668. 23. Chung JC. When is the best time to treat Class
III female patients? World J Orthod 2001;2: 297–322.