Effects of a Patient Education Support
Program on Pramlintide Adherence
Gayle M. Lorenzi, RN, CDE, Susan M. LaRue, RD, CDE, and Susan Eno Collins RD, CHES
INTRODUCTION
R
ecent scientific discoveries have provided new treatment options for managing diabe-tes, and resultant glycemic control has improved through the years.1 However, according to data from the 2003–2004 National Health and Nutrition Examination Survey, only 56% of the population with diabetes has achieved glycemic control defined as having an A1C level of < 7%.1,2Treatment efficacy and health outcomes are heavily influenced by medication adherence.3–5 Unfortunately, adherence to pre-scribed medications across multiple chronic diseases, including diabe-tes, is about 50%.6 A retrospective analysis of patients remaining on oral antidiabetic agents for 6–24 months showed medication adher-ence rates of 36–93%, and reports of medication adherence for insulin ranged from 60 to 80%.7,8 Adherence to diabetes medications is linked to improved clinical outcomes,9,10 whereas lack of adherence is associ-ated with a significantly higher risk of all-cause hospitalizations and mortality.11
Adherence to diabetes treatments may require patients to make signifi-cant lifestyle and behavior changes over time and to adjust to ongoing treatment modifications. Rubin8 identified six factors that influence adherence to diabetes treatment: comprehension of the treatment regimen, perception of benefits, potential side effects, medication
costs, regimen complexity, and the patient’s emotional well-being. In addition, it has been demonstrated that as complexity, cost, and dura-tion of treatment increase, adherence decreases.4 However, in a health care system that focuses primarily on acute care, integration of strategies that foster medication adherence in patients coping with chronic disease is limited.12 Efforts to adequately address the challenges that affect medication adherence can often be pre-empted by time and resource limitations. Opportunities exist to bridge the gap between what is pre-scribed and what is actually taken.
Pramlintide: Bridging a Gap
Pramlintide is a synthetic analog of amylin, a hormone normally co-secreted from pancreatic β-cells with insulin in response to meals.13,14 Pramlintide acetate for injection is approved by the U.S. Food and Drug Administration for the treat-ment of patients with type 1 or type 2 diabetes who use mealtime insulin.15 Pramlintide has multiple mechanisms of action16–18 that decrease postpran-dial glycemia, resulting in improved glycemic control with less insulin and the potential for weight loss.18–21
The addition of pramlintide to an established insulin regimen necessitates dynamic adjustments in which the patient and the health care provider rely on self-monitoring of blood glucose (SMBG) and toler-ability data to guide pramlintide titration and insulin adjustment. As therapy begins, daily glucose patterns may be altered, and hyper-glycemia may result from initial insulin reduction. Subsequently, knowledge of how to manage side effects (e.g., satiety at mealtimes and transient nausea), awareness of realistic glycemic control and weight loss targets, and aid in communicat-ing with family members become important.
Early post-marketing prescription data revealed that ~ 50% of patients prescribed pramlintide discontinued therapy within the first 2 months.22 Despite receipt of product education from their health care providers, patients reported difficulty initiating
I N B R I E F
and continuing to use pramlintide. Data collected from early pram-lintide users indicated that lack of sufficient weight loss, side effects, complicated dosing, and perceived lack of effectiveness accounted for 57% of the reasons for product dis-continuation (Figure 1).
We hypothesized that an ancil-lary, third-party support program that targeted the educational needs of patients new to pramlintide could facilitate learning and positively affect adherence to therapy. The program used variable communica-tion opcommunica-tions (e.g., telephone, print, and Internet) and was designed to complement the education provided by patients’ health care providers. This article provides a discussion of the motivators and barriers associ-ated with initiation of pramlintide therapy; describes the development of a patient support program; and reviews the impact of the program on adherence to pramlintide therapy.
METHODS Program Overview
The pramlintide support pro-gram (Symlin Support Propro-gram [SSP]) was developed by Amylin Pharmaceuticals, Inc., to address the treatment expectations and man-agement issues that patients often
experience when using pramlintide. The SSP was created primarily to support patients initiating therapy and secondarily to provide education and support to patients on established therapy by augmenting the educa-tion provided by their health care providers. Program goals included 1) providing a framework to support safe and effective initiation of therapy, 2) filling a recognized gap in patient education and support, and 3) facili-tating continued use of therapy.
Blinded prescription data that was compliant with patient pri-vacy principles (Health Insurance Portability and Accountability Act [HIPPA]) was used to quan-tify adherence to therapy. In this study, adherence was defined as the extent to which the patient contin-ued therapy and was a composite assessment of therapy persistence and compliance. Persistence was defined as timely prescription refills as calculated from the prescribed dose and was measured as the time between the first prescription and end of the last prescription filled. Compliance was defined as the degree of continued and accurate use and was measured by the amount of product dispensed relative to the dose prescribed. Noncompliance was calculated by comparing total days of medication supply to length
of therapy. To quantify therapy persistence, pharmacy data were used to identify and compare a test group and non-test group. Test group participants were patients “new-to-product” (pramlintide) who enrolled in the support program during this evaluation period. The non-test group was composed of a randomly selected subset of patients, matched for age and sex, who were in the prescription database and were also “new-to-product” but were not enrolled in the program.
Development of Program Content
To help identify the key motivators and barriers to either starting or maintaining therapy, in-depth tele-phone interviews were conducted with current and former pramlintide users (n = 15) and diabetes care specialists (physicians or certified diabetes edu-cators, n = 25). Patients were recruited via flyers sent to community-based endocrinologists and diabetes educators. Interested patients were instructed to independently contact the third-party market research firm conducting the interviews to ensure compliance with HIPPA principles. The physicians and diabetes educa-tors were recruited from outreach telephone calls to relevant commu-nity-based clinical practices and from an existing advisory panel of corpo-rate thought-leaders.
Program content was devel-oped to address the motivators and barriers identified by the patients described above and from clinical observations from diabetes health care professionals experienced in the use of pramlintide (Table 1).22 For patients starting therapy, motivators and barriers were influenced by the practicalities of daily care, whereas maintaining therapy was influenced by a desire for improved health and a greater sense of personal control.
[learning from the experiences of others], skills training to increase competency, expectation setting, and personal goal setting and reinforce-ment) were incorporated into the program to facilitate knowledge acquisition, comprehension, self-efficacy, and behavioral change. Health literacy principles (e.g., attention to word choice, sentence structure, content flow, amount of new information, and visual layout), commonly considered in the devel-opment of education materials, were considered during development of the SSP.
The SSP provided patients with opt-in opportunities for personal communication with program staff (telephone calls), as well as multiple print communications. Registered nurses employed by a third-party call center (Pharmaceutical Product Development [PPD], Raleigh-Durham, N.C.) were responsible for telephone interactions with patients. These nurses received specific product and program implementa-tion training and had prior clinical practice and call center experience. The guidance and coaching provided to patients were nonprescriptive and
consistent across the multiple types of patient contact.
Use of proactive telephone contact was based on the premise that timely and relevant education, combined with personal commu-nication, would facilitate a more positive and enduring treatment experience.23 Frequency of personal contact was based on patient need and duration of therapy, with open access for questions or assistance and reminders to support diabetes self-management efforts. For the patient new to therapy, the proactive telephone calls provided pertinent product information, problem-solving strategies, and guidance regarding early expectations of therapy. Subsequent telephone calls from the SSP staff addressed issues more specific to continued use of the therapy, as well as reminders about general diabetes management principles.
Patients were encouraged to call with questions or concerns that arose between scheduled telephone calls, and ad hoc queries were addressed using uniform and repro-ducible information. Patients were referred back to their health care providers for issues related to indi-vidual treatment management and
questions that were beyond the scope of the program. Complementary information was delivered via print and electronic media (e.g., newslet-ters), starter and welcome kits, and a program Web site. Program content, regardless of delivery method, was consistent with the pramlintide product label.
Implementation
Patients learned about the no-cost program from their health care providers or independently via the Symlin Web site (www.symlin.com). Enrollment in the program could be accomplished via the Web site, by calling a toll-free number, or by sending in a business reply card. Once a patient had opted in to the program, contact was initiated by an SSP nurse.
During the initial call, the nurse assessed individual goals for ther-apy, reviewed treatment benefits, described product actions, and rein-forced prescribed dosing. The nurse also reviewed early expectations of therapy, including the potential for transient symptoms (e.g., blood glu-cose elevations, a sense of fullness, and nausea).
Subsequent telephone calls included information related to dose titration, the influence of
concomi-Table 1. Barriers and Motivators to Starting and Maintaining Pramlintide Therapy
Starting
Pramlintide Therapy MaintainingPramlintide Therapy Barriers • Lack of health care provider support/education
• Frustration: different routine/considerations • Unanticipated hyperglycemia
• Injection burden/treatment complexity • Unexpected side effects
• Additional injections • Side effects
• Therapy disappointment
• Impact of changes on family dynamics • Suboptimal dosing; fewer benefits realized • Life demands
Motivators • Health care provider knowledge • Realistic expectations
• Hope for improvement
• Adjustment period/need for flexibility • Insulin/appetite changes
• Weight loss
• Improved glucose levels, less flux • Improved A1C
• Perceived benefits of therapy
• Increased sense of control of diabetes • Weight loss
tant medications, care and storage of the medication, and travel tips. Repetition of important informa-tion and acknowledgment of small changes made by patients were key strategies used to encourage self-efficacy (confidence in one’s ability to adhere to therapy) and promote assimilation of new information and self-care behaviors. The nurse acknowledged psychosocial con-cerns and made proactive efforts to reassure patients that feelings and concerns about treatment issues and frustration with disease management or worsening diabetes commonly accompany changes in a treatment or management routine. Telephone interactions continued to reinforce dosing frequency and timing, the importance and use of SMBG results to assess treatment efficacy, and concomitant insulin adjustment under the guidance of a health care provider.
All patients received educational materials and newsletters on a prede-termined schedule regardless of their participation in the proactive telephone-based portion of the SSP. Print materials provided reinforce-ment, emphasized problem-solving strategies, provided reminders about realistic expectations of therapy, and shared motivational strategies that were aligned with the identified motivators and barriers associated with the duration of therapy.
Evaluation
The program’s effectiveness was determined by assessing its impact on patients’ willingness and ability to start and maintain pramlintide therapy. Surveys were used to obtain qualitative feedback from SSP par-ticipants and health care providers. The participant surveys were included in the December 2008 (survey 1) and July 2009 (survey 2) program newslet-ters and assessed satisfaction and self-reported behavior changes over
time. Health care provider satisfaction was assessed using an anonymous survey mailed in April 2008 and January 2009 to providers who were diabetes specialists based on their clinical practice.
The initial program evalu-ation period was from March 2007 through October 2008 and included 162 and 1,157 partici-pants in the test (enrolled in the SSP) and non-test (not enrolled in the SSP) groups, respectively. De-identified prescription data mostly from retail pharmacies for the period March 2007 through July 2009 were obtained from SDI (a health care analytics company; Plymouth Meeting, Pa.) to validate the previous results; 223 and 1,201 participants were included in the test and non-test groups, respectively. The test and non-test groups were compared using a large sample z test for comparing two proportions; one-sided P values were reported and used to test for significant differ-ences at the P = 0.05 level.
RESULTS
Most patients who enrolled in the SSP were referred by their health care pro-viders, had type 2 diabetes, and were using mealtime insulin via injections or continuous infusion. Reasons cited for enrolling included 1) being told by their health care provider that the program would be helpful, 2) a desire to learn more about how the therapy worked, and 3) to learn how to better optimize and integrate the therapy into their diabetes care routine.
During enrollment, patients were asked two questions about whether they had received previous educa-tion about the product: 1) “Did you receive patient education materials either from your health care provider or from the product Web site?” and 2) “When you were at your health care provider’s office, did anyone explain to you the importance of
using the product exactly as pre-scribed and working closely with your health care team to carefully add the product to your mealtime insulin therapy?” Approximately 88% of the patients indicated receipt of some training about pramlintide before contacting the SSP, and 80% indicated that they had received product-specific education materi-als from their health care provider or via the product Web site. Despite previous receipt of product-specific education, health care providers recommended and patients sought the SSP to obtain additional educa-tion support.
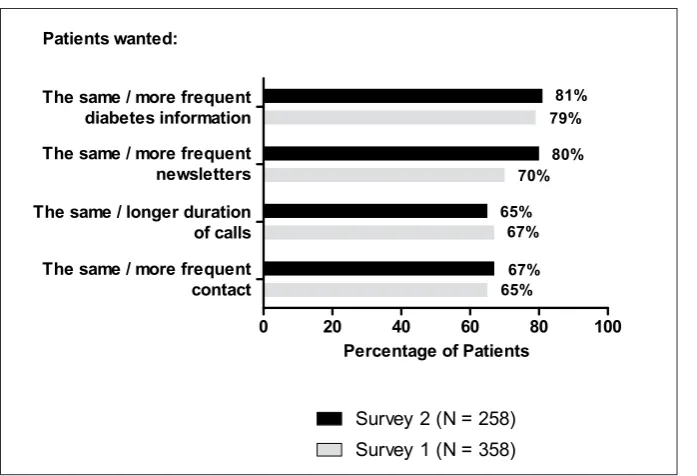
Participants reported satisfac-tion with program content, as well as with the method and frequency of contacts. Respondents to participant Survey 1 (n = 358) generally wanted the same or more frequent contact and information from the SSP in addition to the same or longer dura-tion of each contact. These findings were consistent with Survey 2 (n = 238), in which responses were the same or slightly greater than those recorded in Survey 1 (Figure 2).
Self-reports of diabetes care practices indicated that a high percentage of patients persisted with therapy through the first 3 months and continued to use pramlintide. Frequency of dosing, use of standard dose amounts, and prescription refill data, as reported by the participants, were similar across both participant surveys (Figure 3). In addition, ~ 70% of respondents indicated that the SSP assisted them in taking pramlintide, ~ 30% indicated that the SSP contributed to their using pramlintide for a longer period, and ~ 50% indicated that the SSP helped them when talking with their health care provider about pramlintide.
two-thirds were internists or pri-mary care providers. Approximately half of the respondents had certified diabetes educators on staff, and most reported seeing > 50 patients with diabetes per month. The SSP was perceived as valuable by provider
respondents who referred patients to it. However, general awareness of the SSP was low (21%) among health care provider respondents.
Participants in the test group (those who were “new-to-product” and enrolled in the SSP, n = 223)
were 74% female, with a mean age of 50.3 years. Participants in the non-test group (those who were “new-to-product” and not enrolled in the SSP, n = 1,201) were sex- and age-matched to the test group (Table 2).
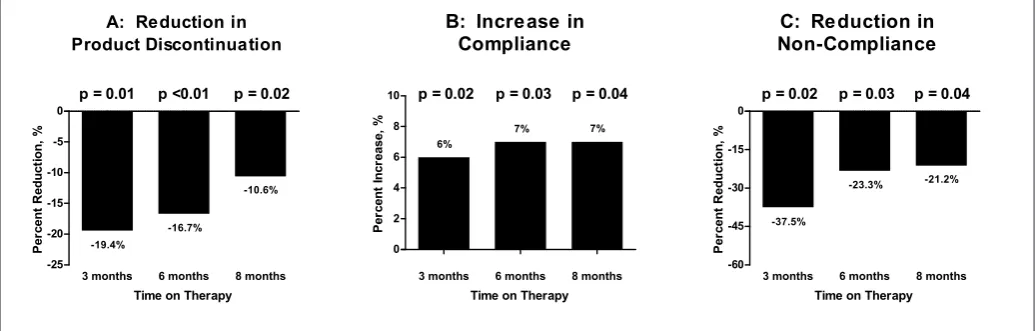
Comparison of the test and non-test groups demonstrated that participation in the SSP improved adherence to therapy. Product discontinuation (a measure of persistence) had decreased by 19.4% (P = 0.01) at 3 months, by 16.7% (P < 0.01) at 6 months, and by 10.6% (P = 0.02) at 8 months, indicating a decreasing trend but an overall increase in continued product use among those enrolled in the support program. When the test group was compared to the non-test group, compliance had increased by 6% at 3 months and by 7% at 6 and 8 months. Noncompliance in the test group had decreased by 37.5% (P = 0.02), 23.3% (P = 0.03), and 21.2% (P = 0.04) at months 3, 6, and 8, respectively, compared to the non-test group (Figure 4).
Product persistence in the test and non-test groups also was evalu-ated by age and sex. Patients ≥ 35
years of age in the test group (n = 203) tended to have higher gains in persistency when compared to equivalent age-groups in the non-test group (n = 1,095). Of note, data from patients < 35 years of age did not demonstrate the tendency toward improved persistency in the test group (n = 20) compared to the non-test group (n = 106). No differences between sexes were seen between the test and non-test group results at months 3, 6, or 8.
DISCUSSION
Adherence to prescribed medica-tion regimens is relevant to clinical practice and remains problematic across disease states.6,24 The impact of nonadherence transcends patient out-Figure 2. Program evaluation: patient satisfaction.
Figure 3. Program evaluation: self-reported behavior changes.
comes and negatively affects provider services, health system access, and coverage issues, as well as the health of the general population.6 Chronic diseases, especially those for which treatment requires lifestyle adaptation and daily decision-making, result in a higher patient burden that can inter-fere with adherence to the prescribed therapy. In addition, factors associ-ated with a treatment, such as the frequency and complexity of the treat-ment, side effects, and monitoring requirements, can influence patient behaviors and treatment choices.3,8,25
The SSP was developed to assist patients new to pramlintide in integrating this therapy into their established diabetes regimen. The goal was to provide information appropriate to patients’ specific stage of therapy. Initially, program infor-mation addressed potential issues associated with therapy initiation. As therapy continued, information was more reflective of the duration
of therapy and potential associated issues.
The SSP was designed to aug-ment, rather than replace, the education provided by the pre-scribing health care provider. The program was developed and funded by Amylin Pharmaceuticals, Inc., and implemented by a third-party call center that provided education and support to enrollees. As such, the SSP offered health care providers a no-cost resource for their patients that was independent of and unen-cumbered by the time or resource constraints that often challenge rou-tine clinical practice.
Social cognitive strategies were incorporated to encourage learn-ing and support self-care behavior change. Proactive education and coaching assisted participants with problem recognition and solution, and attention to daily care issues, such as frequency of dosing, method of administration, and lifestyle
chal-lenges, supported patients’ efforts to integrate the therapy into their diabetes routine. Clinical decision-making or issues beyond the scope of the program were referred back to participants’ health care providers, thus reinforcing the importance of close collaboration between partici-pants and their providers.
Not surprisingly, participation in the SSP did not affect persis-tency in patients < 35 years of age. Although the number of participants in this age-group was inadequate to determine a causal relationship, it is important to recognize generational differences in how information is obtained and used. This age-group generally seeks information using more immediate means (e.g., the Internet) to access knowledge that is specific to their current questions or concerns.26
Prescription data provided an objective measure of adherence to therapy. Participation in the SSP resulted in increased persistency (as measured by product discontinu-ation), increased compliance, and decreased noncompliance to therapy when the test group was compared to the non-test group. However, there are limitations to the use of these data. First, prescriptions filled elsewhere (e.g., via mail order) were Table 2. Patient Characteristics
Test Group Non-Test Group
Sex Male (%) Female (%)
26 74
25 75
Average age (years) 50.3 50.4
not included in the prescription data used for this analysis. Second, esti-mates of dose amount and frequency were based on the patients’ type of diabetes and may have differed from the prescribed amount and frequency of dosing. And finally, this analysis assumed that if the product was dispensed, it was taken, and this assumption may not have been completely accurate.
Frequent evaluation of patient education and intervention pro-grams is necessary to meet changing needs and ensure relevance over time. Health care provider and participant feedback, along with pre-scription data assessments, guided modifications in the program con-tent, frequency, and type of contact to better meet expressed needs and desires. In addition, implementation processes were continually enhanced to increase call efficiency for callers and program staff, and efforts were made to increase program awareness among health care professionals.
CONCLUSION
Adherence to prescribed therapies is a global problem that jeopardizes patient health and health outcomes. The addition of a new therapy to an established medication regimen requires patient education that addresses routine use, side effects, and realistic expectations of the treatment. The SSP was developed to improve adherence for patients using pram-lintide therapy by acknowledging and addressing motivators and barriers unique to their stage of therapy.
The pramlintide support program provided timely instruction, sup-ported self-monitoring and self-care efforts, promoted communication between patients and providers, and reinforced behavioral changes to positively affect medication adherence. Further study of patient support programs such as the SSP is needed to better understand the
enduring impact of these programs on medication adherence.
REFERENCES
1Hoerger TJ, Segel JE, Gregg EW,
Saaddine JB: Is glycemic control improving
in U.S. adults? Diabetes Care 31:81–86, 2008
2American Diabetes Association:
Standards of Medical Care in Diabetes—
2010. Diabetes Care 33 (Suppl. 1):S11–S61,
2010
3Osterberg L, Blaschke T: Adherence to
medication. N Engl J Med 353:487–497, 2005
4McDonald HP, Garg AX, Haynes RB:
Interventions to enhance patient adherence to medication prescriptions: scientific review.
JAMA 288:2868–2879, 2002
5Krueger KP, Berger BA, Felkey B:
Medication adherence and persistence: a
comprehensive review. Adv Ther 22:313–356,
2005
6World Health Organization: Adherence
to long-term therapies: evidence for action. Geneva, World Health Organization, 2003. (ISBN 92 4 154599 2; NLM classification: W 85)
7Cramer AJ: A systematic review of
adherence with medications for diabetes.
Diabetes Care 27:1218–1224, 2004
8Rubin RR: Adherence to pharmacologic
therapy in patients with type 2 diabetes. Am J
Med 118 (Suppl. 5A):27S–34S, 2005
9Pladevall M, Williams IK, Potts LA,
Divine G, Xi H, Lafata JE: Clinical outcomes and adherence to medication measured by claims data in patients with diabetes.
Diabetes Care 27:2800–2805, 2004
10Rozenfeld Y, Hunt JS, Plauschinat
C, Wong KS: Oral antidiabetic medication adherence and glycemic control in managed
care. Am J Manag Care 14:71–75, 2008
11Ho PM, Rumsfeld JS, Masoudi FA,
McClure DL, Plomondon ME, Steiner JF, Magid DJ: Effect of medication nonadher-ence on hospitalization and mortality among
patients with diabetes mellitus. Arch Intern
Med 166:1836–1831, 2006
12World Health Organization: Innovative
care for chronic conditions: building blocks for action [article online]. Available from http://www.who.int/diabetesactiononline/ about/iccc_ch2.pdf. Accessed 19 November 2009
13Young AA, Vin W, Gedulin BR, Pittner
R, Janes S, Gaeta LSL, Percy A, Moore CX, Koda JE, Rink TJ, Beaumont K: Preclinical pharmacology of pramlintide in the rat:
com-parisons with human and rat amylin. Drug
Res Rev 37:231–246, 1996
14Koda JE, Fineman M, Rink TJ, Dailey
GE, Muchmore DB, Linarelli LG: Amylin
concentrations and glucose control. Lancet
339:1179–1180, 1992
15Amylin Pharmaceuticals: Symlin
pre-scribing information, July 2008, San Diego, Calif.
16Fineman MS, Koda JE, Shen LZ,
Strobel SA, Maggs, DG, Weyer C, Kolterman OG: The human amylin analog, pramlintide, corrects postprandial hyperglucagonemia
in patients with type 1 diabetes. Metabolism
51:636–641, 2002
17Kong MF, Stubbs TA, King P,
MacDonald IA, Lambourne JE, Blackshaw PE, Perkins AC, Tattersall RB: The effect of single doses of pramlintide on gastric emptying of two meals in men with IDDM.
Diabetologia 41:577–583, 1998
18Chapman I, Parker B, Doran S,
Feinle-Bisset C, Wishart J, Strobel S, Wang Y, Burns C, Lush C, Weyer C, Horowitz M: Effect of pramlintide on satiety and food intake in obese subjects and subjects with type 2
diabe-tes. Diabetologia 48:838–848, 2005
19Weyer C, Gottlieb A, Kim DD, Lutz K,
Schwartz S, Gutierrez M, Wang Y, Ruggles JA, Kolterman OG, Maggs DG: Pramlintide reduces postprandial glucose excursions when added to regular insulin or insulin
lis-pro in subjects with type 1 diabetes. Diabetes
Care 26:3074–3079, 2003
20Maggs DG, Fineman M, Kornstein
J, Burrell T, Schwartz S, Wang Y, Ruggles JA, Kolterman OG, Weyer C: Pramlintide reduces postprandial glucose excursions when added to insulin lispro in subjects with
type 2 diabetes: a dose-timing study. Diabetes
Metab Res Rev 20:55–60, 2004
21Karl D, Philis-Tsimikas A, Darsow T,
Lorenzi G, Kellmeyer T, Lutz K, Wang Y, Frias J: Pramlintide as an adjunct to insulin in patients with type 2 diabetes in a clinical practice setting reduced A1C, postprandial
glucose excursions, and weight. Diabetes
Technol Ther 9:191–199, 2007
22Data on file. San Diego, Calif., Amylin
Pharmaceuticals
23Roter DL, Hall JA, Merisca R,
Nordstrom B, Cretin D, Svarstad B: Effectiveness of interventions to improve
patient compliance: a meta-analysis. Med
Care 36:1138–1161, 1998
24Berg JS, Dischler J, Wagner DJ,
Palner-Shevlin N: Medication compliance:
a healthcare problem. Ann Pharmacother 27
(Suppl. 9):S1–S24, 1993
25Claxton AJ, Cramer J, Pierce C: A
systematic review of the associations between dose regimens and medication compliance.
Clin Ther 23:1297–1310, 2001
26Skiba D, Barton A: Adapting your
teaching to accommodate the Net
genera-tion of learners. Online J Issues Nurs Vol. 11,
2006. Available from www.nursingworld.org/ MainMenuCategories/ANAMarketplace/ ANAPeriodicals/OJIN/TableofContents/ Volume112006/No2May06/tpc30_416076. aspx. Accessed on 12 January 2009
SUGGESTED READINGS
Anderson RM, Patrias R: Getting out ahead: the Diabetes Concerns Assessment
form. ClinicalDiabetes 25:141–143, 2007
Bodenheimer T, Davis C, Holman H: Helping patients adopt healthier behaviours.
Delamater AM: Improving patient
adher-ence. Clinical Diabetes 24:71–77, 2006
Doonan PT, MacDonald TM, Morris AD, for the DARTS/MEMO Collaboration: Adherence to prescribed oral hypoglycemic medication in a population of patients with type 2 diabetes: a retrospective cohort study.
Diabet Med 19:279–284, 2002
Holman RR, Farmer AJ, Davies MJ, Levy JC, Darbyshire JL, Keenan JF, Paul SK for the 4-T Study Group: Three-year efficacy
of complex insulin regimens in type 2 diabe-regimens in type 2
diabe-tes. N Engl J Med 361:1736–1747, 2009
Kocurek B: Promoting medication adher-ence in older adults . . . and the rest of us.
Diabetes Spectrum 22:80–84, 2009 Koro CD, Bowlin SJ, Bourgeois N, Fedder DO: Glycemic control from 1988– 2000 among U.S. adults with diagnosed type
2 diabetes. Diabetes Care 27:17–20, 2004
Krueger KP, Felkey BG, Berger BA: Improving adherence and persistence: a review and assessment of interventions and descrip-tion of steps toward a nadescrip-tional adherence
initiative. J Am Pharm Assoc 43:668–679, 2003
Lee WC, Balu S, Cobden D, Joshi AV, Pashos CL: Prevalence and economic conse-quences of medication adherence in diabetes:
a systematic literature review. Manag Care
Interface 19:31–41, 2006
Lin EHB, Ciechanowski P: Working with patients to enhance medication adherence.
Clinical Diabetes 26:17–19, 2008
National Council on Patient Information
and Education: Enhancing Prescription
Medicine Adherence: A National Action Plan. Bethesda, Md., National Council on Patient Information and Education, 2007
Piette JD: Cost-related medication underuse: a window into patients’
medica-tion-related concerns. Diabetes Spectrum
22:77–80, 2009
Simpson RJ: Challenges for improving
medication adherence. JAMA 296:2614–2616,
2006
Gayle M. Lorenzi, RN, CDE, is a community health project manager
at the University of California at San Diego. Susan M. LaRue, RD, CDE, is a clinical education specialist at Amylin Pharmaceuticals, Inc. Susan Eno Collins, RD, CHES, is a senior vice president at The HealthEd Group.