International Community Access
to Child Health Program: 10 Years
of Improving Child Health
Rachel A. Umoren, MB, BCh, MS, a Mohamed A. Mohamed, MD, b Koye A. Oyerinde, MD, c Yvonne E. Vaucher, MD, d Ann T. Behrmann, MD, e Michael Canarie, MD, f Rajesh Dudani, MD, g Mirzada Kurbasic, MD, MS, h
Molly J. Moore, MD, i Alcy R. Torres, MD, j Manuel Vides, MD, MS, k Donna Staton, MD, MPHl
CATCH (Community Access to Child Health) Programs both in the United States and now internationally (ICATCH) have gained enormous popularity. This report chronicles the successful implementation of the Program worldwide. It speaks to the power of small investments in good ideas put forward by providers of hands on care everywhere. The history of success reported here is also demonstrated by the remarkable increase in applications, while the resources made available have only allowed for a relatively flat number of funded programs. When success is obvious and cost effective, why not do more?
Jay Berkelhamer, Editor, Global Health
Feature
Gaps in health care delivery routinely contribute to childhood morbidity and mortality in low- and low-middle–income countries (LLMICs).1 To address these gaps,
global organizations like the World Health Organization partner with national ministries of health to find sustainable solutions. Although generally successful, this high-level approach does not directly engage local providers who have ideas for contextual and culturally appropriate solutions but lack the technical, financial, or other necessary resources to implement projects that promote child health in their own communities.2
In 2006, the American Academy of Pediatrics (AAP) Section on International Child Health, which seeks to promote efforts
to improve and maintain the health and well-being of children throughout the world, 3 launched
the International Community Access to Child Health (ICATCH) program.4 The ICATCH program,
modeled on the successful Community Access to Child Health program, 5 has provided 66 small
grants to health workers in low-resource settings to implement clinical and educational projects that improve the physical, mental, and social wellbeing of children. In addition, ICATCH provides guidance on project design and implementation. Pediatrician members of the Section on International Child Health and the ICATCH review team collaborate with grantees by sharing expertise and resources, starting with the application process, through implementation, and beyond the 3-year funding period. Managed by a diverse team of volunteer pediatricians with expertise in global health, ICATCH receives part-time AAP administrative support. ICATCH grants are financed primarily through donations from AAP members, with additional support from outside donors and foundations.
ICATCH GUIDING PRINCIPLES
ICATCH is based on the principle that local child health workers
aDepartment of Pediatrics, University of Washington, Seattle,
Washington; bDepartment of Pediatrics, Washington University,
Washington, District of Columbia; cCatholic Health Initiative St. Alexius
Health, Minot, North Dakota; dDepartment of Pediatrics, University
of California, San Diego, San Diego, California; eSchool of Medicine
and Public Health, University of Wisconsin, Madison, Wisconsin;
fDepartment of Pediatrics, Yale University, New Haven, Connecticut; gDepartment of Pediatrics, University of Arizona, Tucson, Arizona; hDepartment of Pediatrics, University of Louisville, Louisville, Kentucky; iDepartment of Pediatrics, University of Vermont, Burlington, Vermont; jDepartment of Pediatric Neurology, Boston University, Boston,
Massachusetts; kUniversidad Dr. Jose Matias Delgado, Antiguo
Cuscatlán, La Libertad, El Salvador; and lSection on International Child
Health, American Academy of Pediatrics, Los Altos Hills, California
DOI: https:// doi. org/ 10. 1542/ peds. 2017- 2848
Accepted for publication Apr 4, 2018
Address correspondence to Donna Staton, MD, MPH, International Community Access to Child Health, Section on International Child Health, American Academy of Pediatrics, 141 NW Point Blvd, Elk Grove Village, IL 60007. E-mail: icatch@ aap.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they
have no financial relationships relevant to this article to disclose.
FUNDING: The International Community Access to Child Health
program is funded by the American Academy of Pediatrics.
POTENTIAL CONFLICT OF INTEREST: The authors have
indicated they have no potential conflicts of interest to disclose.
To cite: Umoren RA, Mohamed MA, Oyerinde KA, et al.
are best positioned to understand the health challenges in their communities and are uniquely qualified to address them. The following prerequisites must be met for proposals to qualify for funding:
• funded programs must be led by local child–health care providers or educators from LLMICs;
• proposals must improve clinical services for children or provide health education for children, parents, or health care providers and should not solely be focused on research;
• collaboration with community-based organizations, government, schools, or businesses within the target community is strongly encouraged because this
enhances likelihood of uptake and sustainability; and
• proposals must have strong potential for sustainability beyond the grant period and replication in other communities.
THE ICATCH PROCESS
The ICATCH process is designed to be straightforward and accessible to health providers in low-income settings.6 Each fall, a call for
proposals is widely distributed via AAP and other Web sites targeting global health educators and pediatricians in low- and middle-income countries, LISTSERVs, social media, etc. Application materials are downloadable from the ICATCH Web site (www. aap. org/ icatch) along with a detailed instruction booklet. The application is submitted by e-mail rather than an online process specifically to enable those without regular Internet access to apply. Applications meeting all
prerequisites are scored on merit
each year, depending on funding availability. ICATCH grantees are linked with a US-based pediatrician with global health experience who serves as a resource throughout the 3 years of the grant. All funded applicants, as well as those selected to revise and reapply, receive individualized feedback. ICATCH grants need to include simple, straightforward ways to monitor outputs and evaluate project outcomes. A mandatory annual report requires careful self-evaluation of project successes and failures and offers another opportunity for collaboration between grantees and advisors. Project directors who encounter significant challenges in
implementation are encouraged to work with their project advisors to modify plans and overcome obstacles.
ICATCH FUNDED PROJECTS
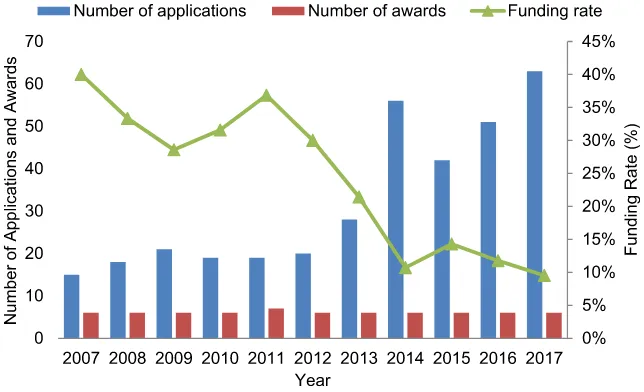
From 2007 to 2017, ICATCH grants have supported 66 innovative programs in 37 countries, primarily
decreasing from 40% in 2007 to 10% in 2017. See Fig 1.
No preference is given to a specific region or country, but several countries have received multiple awards. For example, 11% of total ICATCH grants have been given to projects in Uganda. Although country classifications and ICATCH grant criteria regarding limiting grant applications to countries designated as LLMICs have changed over time, 82% of ICATCH projects have been conducted by project directors living in countries that are currently classified by the World Bank as LLMICs. In a review of funded grants from 2011 to 2017, 31% of codirectors also resided in LLMICs. ICATCH projects have addressed a wide variety of health needs, including nutrition education, newborn care, immunizations, oral health, autism screening, safety, and the unique needs of adolescents. See Table 1.
The majority of ICATCH-funded projects include community (85%) and provider education (65%). Half
FIGURE 1
TABLE 1 ICATCH-Funded Projects by Country
Continent Country ICATCH-Funded Projects
Asia Afghanistan “Daireyeh Waledin” (Circle of Parents)
Bangladesh Promotion of Child Health in Primary School Cambodia Floating Gardens for Health and Prosperitya
Dental Treatment for Children With Cleft Lip and Palate in Cambodiaa Implementing Helping Babies Breathe in Remote Floating Villages China Rural Children With Diarrhea: Primary Care
Dietary Assessment for Intake of Vitamin A Using Semi-quantitative Food Frequency Questionnaire
Healthy Children ‐ Healthy Community Parent Education for Child Passenger Safety
India Home‐Based Care Program for Infants in Krishnagiri, India Newborn Resuscitation Training
Indonesia Improving, Understanding, and Implementation of IMCI: Urban Community Health Workers Improve Understanding of GOBI FFF
Laos Good Nutrition
Myanmar Targeted Vaccination Opportunities for Children, Hepatitis‐B Preventiona Pakistan Maternal Education to Improve Weaning Diet of Infants in Karachia
Trained Nurses Detect Cases of Child Malnutrition
Improving Child Health Through Maternal Education: The Helping Hands Project Philippines TB DOTs for Kids
Bagong Barangay Project
Vietnam Vietnam - First Aid for Childcare Givers and Teachers (VIET-FACTs)
Africa Angola Sickle Cell Education and Screening for Angolan Adolescents
Botswana HIV/AIDS Education for School Staff
Ethiopia Training Community Health Workers in Ethiopia to Recognize the Signs of Neonatal Illness Using Videosa
Ghana Community Malaria Prevention Project Child Protection in Ghana
Strengthening Community Awareness of Pediatric Poisoning in Ghana Kenya Hospital Linkage With Community Child Health in Kisii, Kenya
Improving Access to Health Care for Street Children Peer Navigators Supporting HIV Treatment for Street Youtha Lesotho General Pediatrics Nurse Training in Lesothoa
Liberia Enhanced Well Child Care for Adolescent Mothers and Infants Developing a Model Medical Home for Liberian Children
Malawi Training Program for Management of Neurodisabled Malawian Children Teenager Support Line, Malawi
Establishing a Pediatric Triage System to Improve Child Health in Mangochi District Hospitala Mozambique Supplemental Nutrition for Infants With Failure‐to‐Thrive in Mozambiquea
Nigeria Balanced Early Nutrition for Development (BEND) Support for Adolescents With HIV in Boarding Schoola Rwanda Growing Health (GH): Hospital-based Farm and Nutritiona South Africa Turn INH Preventive Therapy Into Reality
Uganda The Kayunga Newborn Project
Childhood Epilepsy in Northern Uganda: Children as Health Workers Tackling Malnutrition Through Peer Education in Schools Promoting Adolescent Medicine in Uganda
Community Empowerment in Health‐Plus, Mukonoa
Supporting School‐Centered Asthma Programme (SCAPE) in a Boarding School in Central Ugandaa
School Gardening for Healthy Child Growth and Learninga Zambia Zambian Health Evaluation and Education Project
Asthma Project
Europe Bosnia and Herzegovina Autism Education and Screening
Romania Safe Baby Project
health (12%), child health (19%), adolescents and street youth (17%), and parents (16%). See Fig 2.
ICATCH FUNDING HAS LED TO SUSTAINABLE PROJECTS AND PARTNERSHIPS
ICATCH projects have a high completion rate. In 2017, of the 66 projects funded, 49 of 54 (91%) projects continued for the full 3 years with a submission of a final report, and there were 12 projects in progress. Although modest in amount, ICATCH grants have resulted in the implementation of sustainable and high impact health care projects. Examples of projects that have proven to be sustainable include the following:
- a project codirected by Nakakeeto and Vaucher in 2007 on
“Strengthening Capacity to Care for High Risk Newborns in Rural Uganda: The Kayunga Experience”
informed the Ugandan Ministry of Health Newborn Care Initiative; - a 2011 project codirected by Remetic
and Kurbasic on autism education and early screening led to regional awareness, strong community
capacity building for staff and skills training for patients at a newly established General Adolescent Health Clinic at the Mulago National Referral and Teaching Hospital for Makerere University, Uganda.
BENEFITS BEYOND THE GRANT PERIOD
ICATCH is uniquely positioned to extend professional support to grantees beyond the grant period. For example, grantees have received support to cofacilitate grant-writing workshops at the 2010, 2013, and 2016 International Congress of Pediatrics meetings and to participate in a week-long International Quality Improvement and Leadership Institute workshop. Grantees become part of a growing network of current and past grantees, presenting their work
encourage collaboration among global health faculty and those working in similar fields or facing similar challenges, building the capacity of grantees to be successful in leveraging in-kind support and funding from other sources and strengthening the connections between institutions and communities.
CONCLUSIONS
In 2017, ICATCH celebrated 10 years of successful collaboration with children’s health care providers in low- and middle-income countries. ICATCH grants empower local providers to identify challenges, offer solutions, and organize their communities to achieve better health. Although the increasing competitiveness of ICATCH grants reveals the need for expansion of the program, ICATCH’s decade of success reveals how professional medical organizations can leverage modest funding with volunteer professional support to improve global child health.
ACKNOWLEDGMENTS
We acknowledge the work and
Continent Country ICATCH-Funded Projects
Central America and Caribbean Belize Protecting Smiles for Healthier Futures in Southern Belize Dominican Republic Improving Child Health in the Community
El Salvador Improving Healthcare and International Collaboration Diagnosis and Referral of Undernourished Children
Community Public Health Collaborative in Los Abelines, El Salvador
Guatemala Training the Next Generation of Frontline Health Workers for Child Health in Guatemalaa Haiti Health Care for Haiti’s children
Community Health Worker Outreach to Rural Elementary Schools Programa Hydroxyurea to Treat Sickle Cell Disease in Haitia
Nicaragua Mobile Health Kits for Use in Vulnerable Communities
South America Bolivia Tsimane’ Territory Multi‐Media Public Health Education to Prevent Childhood Illnessa Ecuador Sonrisa’s Children’s Oral Health and Nutrition Project
ADHD, attention-deficit/hyperactivity disorder; DOT, directly observed treatment; GOBI FFF, growth monitoring, oral rehydration and diarrhea, breastfeeding, immunization, preventable infectious diseases, family planning/spacing, food supplementation, female education; IMCI, integrated management of childhood illness; INH, isoniazid; TB, tuberculosis.
a In-progress project. TABLE 1 Continued
FIGURE 2
REFERENCES
1. Maru DS, Andrews J, Schwarz D, et al. Crossing the quality chasm in
resource-limited settings. Global Health. 2012;8:41
2. Kerry VB, Mullan F. Global Health Service Partnership: building health professional leadership. Lancet. 2014;383(9929):1688–1691
3. Jilani SM. International child health program marks 10 years, calls for proposals. AAP News, April 28, 2014. Available at: http:// www. aappublications. org/ content/ 35/ 5/ 24. 2. Accessed August 2, 2018
4. Duncan B, Mandalakas AM, Staton DM, Anders B, Behrmann A, Kurbasic M. ICATCH: become a change agent. In:
Berman S, Palfrey JS, Bhutta Z, Grange AO, eds. Global Child Health Advocacy: On the Front Lines. Elk Grove Village, IL: American Academy of Pediatrics; 2013:309–313
5. Hutchins VL, Grason H, Aliza B, Minkovitz C, Guyer B. Community Access to Child Health (CATCH) in the historical context of community pediatrics. Pediatrics. 1999;103(6, pt 3):1373–1383
6. Duncan B, Mandalakas A, Staton D, et al. Child healthcare workers in resource-limited areas improve health with innovative low-cost projects. J Trop Pediatr. 2012;58(2):120–124 ABBREVIATIONS
AAP: American Academy of Pediatrics
ICATCH: International
Community Access to Child Health
LLMIC: low- and low-middle–
DOI: 10.1542/peds.2017-2848 originally published online September 5, 2018;
2018;142;
Pediatrics
Moore, Alcy R. Torres, Manuel Vides and Donna Staton
Ann T. Behrmann, Michael Canarie, Rajesh Dudani, Mirzada Kurbasic, Molly J.
Rachel A. Umoren, Mohamed A. Mohamed, Koye A. Oyerinde, Yvonne E. Vaucher,
Improving Child Health
International Community Access to Child Health Program: 10 Years of
Services
Updated Information &
http://pediatrics.aappublications.org/content/142/4/e20172848
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/142/4/e20172848#BIBL
This article cites 4 articles, 0 of which you can access for free at:
Subspecialty Collections
alth_sub
http://www.aappublications.org/cgi/collection/international_child_he
International Child Health following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2017-2848 originally published online September 5, 2018;
2018;142;
Pediatrics
Moore, Alcy R. Torres, Manuel Vides and Donna Staton
Ann T. Behrmann, Michael Canarie, Rajesh Dudani, Mirzada Kurbasic, Molly J.
Rachel A. Umoren, Mohamed A. Mohamed, Koye A. Oyerinde, Yvonne E. Vaucher,
Improving Child Health
International Community Access to Child Health Program: 10 Years of
http://pediatrics.aappublications.org/content/142/4/e20172848
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.