BRAF
V600E Mutational Status in Pediatric Thyroid Cancer
Lauren E. Henke,
BA,
1Stephanie M. Perkins,
MD,
1John D. Pfeifer,
MD, PhD,
2Changquing Ma,
MD, PhD,
2Yumei Chen,
MD,
2Todd DeWees,
PhD,
1and Perry W. Grigsby,
MD1,3*
INTRODUCTION
Data from the National Cancer Institute Surveillance, Epidemi-ology, and End Results registry demonstrate a rising incidence of thyroid cancer in patients under the age of 20 [1–3]. Children with thyroid cancer tend to present with more advanced disease than their adult counterparts [4–6]. At presentation, the incidence of lymph node involvement in children (40–90%) is roughly double that of adults (20–30%). Distant metastases are present in 20–30% of children at diagnosis, compared to 2% in adults [7]. However, overall survival in the pediatric population remains excellent with 30-year overall survival rates of 90–99% [7]. Most pediatric patients are treated with surgery followed by radioactive Iodine131[7–9]. Due to the more advanced stage at presentation in children, extensive and repeated treatment is often required [7,8,10].
Thyroid cancer in children is in many ways a distinct disease from thyroid cancer in adults. Currently, there is no clear explanation for the dissimilarities in clinicopathologic outcomes of thyroid cancer in pediatric and adult populations. Histologically, papillary thyroid cancer (PTC) is the most prevalent type of thyroid malignancy in both children and adults [11]. Mutations in the BRAFgene are common in patients with PTC. The majority of these mutations involve a transversion from T to A at nucleotide 1799, leading to a valine to glutamic acid change in codon 600. This results in theBRAFV600Emutation (termedBRAFmutation hereafter). In adult patients, this mutation occurs in around 50% of patients, although reports vary from 29–83% in the literature [12–14]. Previous reports specific to pediatric patients have shown a lower prevalence of this point mutation in childhood thyroid carcinoma, although the numbers of patients tested were limited [7,15–17]. It has been suggested that differences in the biomolecular profiles of thyroid carcinoma, such as presence or absence of the BRAF mutation, might account for some of the differences between childhood and adult thyroid cancers [11,15–18].
This retrospective analysis of pediatric papillary thyroid carcinoma (PTC) aimed to determine the prevalence of the BRAF mutation and review the clinicopathologic outcomes of pediatric patients treated at our institution. Specifically, age, gender,
race, tumor characteristics, and BRAF mutational status were analyzed for possible correlations with outcome.
METHODS
Patient Identification and Clinicopathologic Data
Collection
Formalin-fixed, paraffin-embedded (FFPE) thyroid tissue from 27 pediatric thyroid cancer patients was obtained from the Thyroid Cancer Tumor Registry. Patients less than 22 years of age at diagnosis diagnosed between 1973 and 2005 were included for analysis. All patients were treated and evaluated with curative intent at the Mallinckrodt Institute of Radiology at Washington University School of Medicine. Patients with PTC, follicular variant of PTC, and trabecular thyroid carcinoma were included. Patients with medullary thyroid cancer were excluded. Treatment data were obtained by review of the medical record and/or by direct communication with the patient or parents. Data abstracted from patient records included histological subtype, treatment records, and clinicopathologic outcomes. Review of records indicated that none of these individuals had any history of external beam radiation exposure. This retrospective study was performed under a protocol approved by the Washington University Institutional Review Board (protocol number 201010705), with waiver of consent. The determination ofBRAFmutational status was made after surgical Background.Clinical outcome of papillary thyroid carcinoma
(PTC) in children differs significantly from that of adults. There is no clear explanation of this difference although previous studies have demonstrated a lower prevalence of theBRAFV600Emutation in PTC of children. However, data are limited due to the rarity of this diagnosis.BRAFV600Emutation prevalence and its relationship with outcome in pediatric PTC remain unclear.Procedure. BRAFV600E
mutational status was determined in 27 PTC patients less than 22 years of age using restriction fragment length polymorphism (RFLP) analysis. The relationship betweenBRAFV600Emutation status, patient and tumor characteristics as well as progression-free survival (PFS) were analyzed. Results.BRAFV600E was present in 63% of patients and occurred more often in male patients versus females (P¼0.033). Presence of the mutation did not correlate with any
difference in extent of disease at diagnosis, tumor size, capsular invasion, vascular invasion, soft tissue invasion, or margin status. At 10 years, PFS forBRAFV600Epositive versus negative patients was
55.5% versus 70.0%, respectively (P¼0.48). Overall survival was 100% and median follow-up was 13.9 years.Conclusions.This study of pediatric PTC demonstrates thatBRAFV600E mutations occur in children at a rate comparable to adults. We found a correlation of
BRAFV600Ewith the male gender, but no evidence that the mutation
correlates with more extensive or aggressive disease. This analysis suggests that differences in disease course of PTC in children versus adults are not strongly dependent upon the presence of theBRAFV600E
mutation. Pediatr Blood Cancer 2014;61:1168–1172.
#2014 Wiley Periodicals, Inc.
Key words: BRAFmutation; BRAF V600E; pediatricBRAFmutation; pediatric thyroid carcinoma
1Department of Radiation Oncology, Washington University School of Medicine, St. Louis, Missouri;2Department of Pathology, Washington University School of Medicine, St. Louis, Missouri; 3Division of Nuclear Medicine, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, Missouri
Conflict of interest: Nothing to declare.
Correspondence to: Perry Grigsby, Department of Radiation
Oncolo-gy, Washington University School of Medicine, Campus Box 8224, 4921 Parkview Place, Floor LL, St. Louis, MO 63110.
E-mail: [email protected]
Received 6 November 2013; Accepted 18 December 2013 C 2014 Wiley Periodicals, Inc.
DOI 10.1002/pbc.24935
Published online 27 March 2014 in Wiley Online Library (wileyonlinelibrary.com).
and medical treatments were concluded and did not affect treatment decisions.
PTC Histological Classification
For all cases identified, hematoxylin and eosin stained slides were examined by study pathologists to identify areas with classic characteristics of PTC, including papillary architecture, typical PTC nuclei (enlarged, overlapping, irregular, ground-glass empty nuclei with nuclear grooves), psammoma bodies, and stromal reaction. Histologically, the 27 cases were comprised of classical (n¼21), follicular variant (n¼5), and trabecular (n¼1) subtypes classified using standard criteria [19–22]. Areas of carcinoma were marked on the glass slides to guide collection of tissue cores from the corresponding FFPE tumor blocks of the case.
DNA Extraction and
BRAF
Mutation Analysis
Two tissue cores of 1 mm diameter were extracted from the areas of tumor by means of disposable biopsy punches with plungers (Miltex1, York, PA). Samples were incubated in xylene for 3 minutes at 50˚C; xylene aspiration was followed by two washes with 100% ethanol. Subsequently, samples were incubated for 48 hours with 0.5 mg/ml proteinase K (Quiagen1, Germantown, MD), with a mid-interval addition of 0.5 mg/ml proteinase K. DNA was extracted from each sample via a commercial kit (Puregene1, Minneapolis, MN) according to the manufacturer’s instructions. Following extraction, DNA was stored at 4˚C. Polymerase chain reaction (PCR) was utilized to amplify the 215 base pair (bp)BRAF exon 15, using previously published primers and Platinum Taq DNA Polymerase (Invitrogen1, Carlsbad, CA), according to the manufacturer’s instructions. Primers (Invitrogen1) were: BRAF exon 15F (forward): 50-TCATAATGCTTGCTCTGATAGGA-30, BRAF exon 15R (reverse): 50 -GGCCAAAAATTTAAT-CAGTGGA-30. PCR conditions consisted of 35 cycles with 1 min of denaturation at 94˚C, 1 min of annealing at 51˚C, and 1 min of extension at 72˚C. Subsequently, samples were submitted to restriction fragment length polymorphism (RFLP) analysis by the enzyme TspRI (Invitrogen1), using the buffer conditions recommended by the manufacturer.TspRI cuts the wild type, 215 bp amplification product into two fragments of 120 and 95 bp. After the restriction digest, the DNA bands were resolved by agarose gel electrophoresis and visualized by ethidium bromide staining.
Assay Validation
RFLP analysis has been used by numerous other labs to evaluate BRAFexon 15 [23–26]. We performed several steps to validate the assay for use in our own laboratory. To establish test accuracy, we compared our results with those of direct DNA sequencing by a commercial clinical reference laboratory (GenPath, Elmwood Park, NJ). For 40 cases of PTC diagnosed between 2009 and 2011 (20 cases with and 20 cases without aBRAFV600E mutation) there was 100% concordance between our test and the outside laboratory. These 40 test cases did not overlap with the 27 pediatric cases presented here. To establish the reproducibility of the assay, all 40 cases in the validation set were tested three times (in a blinded fashion); there was 100% concordance between test runs. To establish the sensitivity of the test, knownBRAFmutation positive PCR amplified DNA (at 100 nmol/ml) was diluted into BRAF negative DNA (also at 100 nmol/ml); dilution ratios were 1:0, 1:1,
1:2, 1:3, 1:5, 1:10, and 1:20 ofBRAFmutation positive to negative. These dilutions were then subjected to restriction enzyme analysis and gel electrophoresis, as previously described, and showed that the mutant allele could be reproducibly identified at a ratio of 1:5.
Treatment and Follow-Up
All patients underwent total thyroidectomy. Cervical lymphadenectomy was performed in 67% of patients, consisting of excision in 52% and modified radical neck dissection in 15%. The remaining nine (33%) had no surgical removal of neck lymph nodes. Post-operative 131I was administered to 23 patients (85%). Two additional patients were treated with131I after recurrence; therefore, 93% of patients received 131I at some point. The administered activity of131I given as initial treatment was determined based on our treatment guidelines which utilize the standard guidelines for adult patients incorporating reductions based on the weight of the child [27,28]. Our standard adult treatment recommendations during the study years included an administered activity of 25–50 millic-uries (mCi) of131I for patients who have residual normal thyroid tissue remaining resulting in minimal thyroid stimulating hormone (TSH) elevation. Patients with no lymph node involvement received 100 mCi, while lymph node positive patients receive 150 mCi. Patients with distant metastatic disease received 250 mCi, unless the disease included bulky or diffuse lung involvement, in which case the dose was reduced to 50–100 mCi. For children, dose adjustments were made on a per kg basis using the doses described above for a standard 70-kg person. Administered activity of131I ranged from 25 mCi (0.93 gigabecquerel—GBq) to 175 mCi (6.5 GBq). 131I administrations were repeated for patients with persistently positive post-treatment whole-body 131I scintigraphy. For those patients treated with 131I, cumulative administered activity ranged from 50 mCi (1.9 GBq) to 970 mCi (35.9 GBq). Post-treatment surveil-lance consisted of physical examination and laboratory studies, including TSH, triiodothyronine, and free thyroxine for all patients. Beginning in the 1990s, thyroglobulin levels and thyroglobulin antibodies were monitored for all patients.
Variables
Information regarding margin status, vascular invasion, capsular involvement, and soft tissue invasion were available for all patients. Extent of disease at presentation was known for all patients and was recorded as disease confined to the thyroid, involvement of the cervical lymph nodes, or pulmonary metastatic disease. Variables analyzed for correlation withBRAFmutational status included age at diagnosis, gender, race, extent of disease, and histologic subtype. Chi-squared analysis was used for comparison of age groups.T -tests were used for comparison of data with continuous variables, while chi-squared tests were used for dichotomous data. Statistical analyses were performed using IBM SPSS Statistics, Version 21 (SPSS, Inc., Chicago, IL).
RESULTS
Patient Characteristics
A total of 27 patients meeting the eligibility criteria with evaluable tissue underwentBRAFgene analysis. Patient and tumor characteristics are presented in Table I. Age at diagnosis ranged
from 5.8 to 21.2 years with median age of 18.6 years. All patients had at least 5 years of follow-up with a median follow-up of 13.9 years (range 5.5–38.8 years). All but two patients had tumors greater than 1.0 cm in size and 17 patients (63%) had lymph node involvement at diagnosis. Pathologic findings included thyroid capsular invasion in 56%, vascular invasion in 48%, soft tissue invasion in 37%, positive margins in 41%, and bilateral thyroid involvement in 22%. Overall, 37% of patients presented with disease confined to the thyroid, 59% had disease involving the cervical lymph nodes and 4% had pulmonary metastatic disease.
BRAF
Analysis
TheBRAFmutation was present in 17 patients (63%). Mutation status was identified by RFLP, which displayed two, wild-type DNA bands (120 and 95 bp) digested by theTspRI restriction enzyme when theBRAFV600E mutation was absent, and three DNA bands (215, 120, and 95 bp) when theBRAFV600E mutation was present (heterozygote). Representative cases are illustrated in Figure 1. There was a trend towards increased presence ofBRAFmutation in patients with classical papillary histology versus follicular or trabecular variants of papillary histology (71.4% vs. 33.3%, respectively, P¼0.088). There was a statistically significant increase in the BRAF mutation in male patients versus female
patients (100% versus 52.3%, respectively,P¼0.033). There was no difference in extent of disease at diagnosis, tumor size, capsular invasion, vascular invasion, soft tissue invasion, margin status, or bilateral versus unilateral thyroid involvement based on BRAF
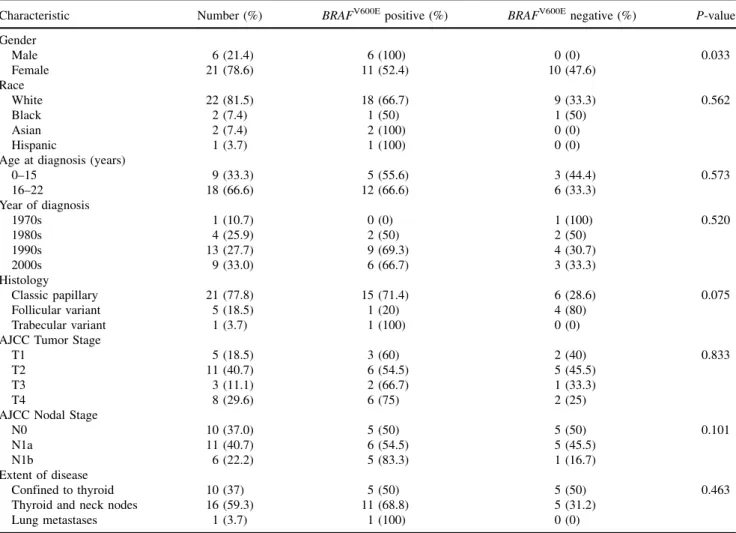
TABLE I. Patient and Tumor Characteristics
Characteristic Number (%) BRAFV600Epositive (%) BRAFV600Enegative (%) P-value Gender Male 6 (21.4) 6 (100) 0 (0) 0.033 Female 21 (78.6) 11 (52.4) 10 (47.6) Race White 22 (81.5) 18 (66.7) 9 (33.3) 0.562 Black 2 (7.4) 1 (50) 1 (50) Asian 2 (7.4) 2 (100) 0 (0) Hispanic 1 (3.7) 1 (100) 0 (0)
Age at diagnosis (years)
0–15 9 (33.3) 5 (55.6) 3 (44.4) 0.573 16–22 18 (66.6) 12 (66.6) 6 (33.3) Year of diagnosis 1970s 1 (10.7) 0 (0) 1 (100) 0.520 1980s 4 (25.9) 2 (50) 2 (50) 1990s 13 (27.7) 9 (69.3) 4 (30.7) 2000s 9 (33.0) 6 (66.7) 3 (33.3) Histology Classic papillary 21 (77.8) 15 (71.4) 6 (28.6) 0.075 Follicular variant 5 (18.5) 1 (20) 4 (80) Trabecular variant 1 (3.7) 1 (100) 0 (0) AJCC Tumor Stage
T1 5 (18.5) 3 (60) 2 (40) 0.833
T2 11 (40.7) 6 (54.5) 5 (45.5)
T3 3 (11.1) 2 (66.7) 1 (33.3)
T4 8 (29.6) 6 (75) 2 (25)
AJCC Nodal Stage
N0 10 (37.0) 5 (50) 5 (50) 0.101
N1a 11 (40.7) 6 (54.5) 5 (45.5)
N1b 6 (22.2) 5 (83.3) 1 (16.7)
Extent of disease
Confined to thyroid 10 (37) 5 (50) 5 (50) 0.463 Thyroid and neck nodes 16 (59.3) 11 (68.8) 5 (31.2)
Lung metastases 1 (3.7) 1 (100) 0 (0) AJCC, American Joint Committee on Cancer.
Fig. 1. BRAFV600Eevaluation. Representative analysis of FFPE thyroid tissue specimens. DNA from four samples was amplified by PCR and submitted to RFLP by incubation with the restriction enzymeTspRI. Two samples displayed mutated (V600E) digestion pattern, with three fragments of 215 bp (undigested, mutated allele), 120, and 95 bp. Two samples displayed the wild-type (Wt) digestion pattern, showing two fragments of 120 and 95 bp, respectively. M, molecular marker; // empty lane.
mutational status. There was no difference in presence ofBRAF mutation in children younger than 15 years versus children 15–21 years of age (P¼0.97). Similarly, the presence of the BRAF mutation was not significantly correlated with age as a continuous variable (P¼0.24).
Outcome
Overall survival was 100% as there were no deaths during this study period. At the time of last follow-up, 26 of 27 patients were alive with no evidence of disease. Ten patients (37%) have experienced recurrent disease. Patterns of failure consisted of recurrence in the cervical lymph nodes in eight, pulmonary metastatic disease in one and recurrence in the thyroid bed, neck and lungs in 1. Progression-free survival (PFS) at 10 years was 61.1%. There was no difference in PFS based onBRAFmutational status. At 10 years, PFS forBRAFpositive versus negative patients was 55.5% versus 70.0%, respectively (P¼0.48) (Fig. 2). There was also no difference in PFS based on patient gender. However, PFS was adversely affected by presence of positive margins (P¼0.03), soft tissue invasion (P¼0.008), bilateral disease (P¼0.03), and vascular invasion (P¼0.01). On multivariate analysis, only soft tissue invasion and vascular invasion had significant adverse effect on PFS (P¼0.03 and 0.02, respectively). We also found no difference in the cumulative administered activity of131I based onBRAFmutational status.
DISCUSSION
The presence of the BRAF mutation in adult PTC has been reported by several groups. Fewer data are available regarding its presence in pediatric PTC. We found that theBRAFmutation was present in 63% of pediatric patients. We found a statistically significant increase inBRAFpositivity in male patients. There was no correlation with BRAF status on extent of disease, patient age, or risk factors associated with PFS (i.e., margin status, capsular invasion). Additionally, there was no difference in PFS or cumulative administered131I activity based onBRAFstatus.
Examination of this mutation in pediatric thyroid carcinoma is important because it has been hypothesized that differences in
biomolecular profiles, such as presence or absence ofBRAF, might account for differences in the clinical behavior of childhood and adult thyroid cancer [15]. Previous studies have shown that the prevalence of theBRAFmutation is approximately 50% in adult PTCs, with a reported range of 28–83% [12–14]. In children, BRAF positivity has been reported with very low prevalence (0–16%) [11,12,15–17]. However, we observed theBRAFmutation in 17/27 patients (63%).BRAF incidence in childhood PTC has been reported to increase with increasing age, but we were unable to demonstrate any correlation withBRAFstatus and age [11]. Of the patients less than 15 years old, 5/8 (63%) demonstrated a positive BRAFmutation. Within adult PTC, the mutation is most commonly observed in the context of classical PTC histology [29,30]. The findings within our pediatric population were consistent with this historical observation made in adult populations.BRAFtended to occur more frequently in our pediatric patients with “classical” PTC than in patients with non-classical subtypes of PTC (71.4% vs. 33.3%), although this trend was not statistically significant. The relationship betweenBRAFstatus and gender was also analyzed in this study. Interestingly, we observed thatBRAFoccurred in 100% of male patients (6/6) and in only 52.4% of females (11/21) (P¼0.003). This male predominance is consistent with findings from Xu et al. [31].
The importance onBRAFstatus as it relates to disease outcome in adult patients is debated [32]. While some reports have demonstrated more aggressive clinical features and worse progno-sis for patients with the mutation, others have not. A large study of 429 adult patients with PTC by Gouveia et al. [32] demonstrated that while 73.2% of patients tested positive for theBRAFmutation, there was no correlation withBRAFmutation and extent of disease, lymphovascular invasion, positive margins, or extranodal extension on multivariate analysis. However, a study of 219 adult PTC patients by Xing [12] showed thatBRAFpositivity was significantly associated with an increased risk of tumor recurrence. Due to the uncertainty of the prognostic value ofBRAFmutational status, there are no current recommendations to alter management based on BRAFtesting results.
In addition to being a retrospective analysis, there are other limitations to our data. Like other analyses of this relatively rare pediatric disease, our study was limited by small sample size. Although detailed treatment and follow-up data were available for this patient set, the small number of total patients makes it difficult to draw statistically significant conclusions about the effects of the BRAFmutation as an independent variable on such outcomes as progression free or overall survival. Additionally, we did not test for other common mutations, aside from theBRAFmutation, such as theRET/PTCrearrangement that often occurs in pediatric PTC, which could have enriched our analysis [12,16,33]. Although limited by the factors mentioned, our analysis also has several strengths. The lengthy follow-up time (median 13.4 years) and ample treatment data available ensured that all late events such as recurrence or retreatment were captured by and included in our analysis. All patients were treated at a single institution and none of the patients had any history of prior radiation exposure.
To conclude, our study demonstrated that theBRAFmutation occurs in children with PTC at a rate comparable to adults. We also found a correlation ofBRAFwith the male gender, an observation that has been noted previously in the adult literature. Finally, although theBRAFmutation occurred frequently in our population, we found no evidence that the mutation is correlated with a more
Fig. 2. Progression-free survival based onBRAFmutational status.
extensive or aggressive disease process. Therefore, our analysis does not support the hypothesis that differences in the biological behavior of adult and pediatric thyroid carcinomas are strongly dependent upon the presence of theBRAFmutation.
REFERENCES
1. McClellan DR, Francis GL. Thyroid cancer in children, pregnant women, and patients with Graves’ disease. Endocrinol Metab Clin North Am 1996;25:27–48.
2. Hogan AR, Zhuge Y, Perez EA, et al. Pediatric thyroid carcinoma: Incidence and outcomes in 1753 patients. J Surg Res 2009;156:167–172.
3. Holmes L, Hossain J, Opara F. Pediatric thyroid carcinoma incidence and temporal trends in the USA (1973–2007): Race or shifting diagnostic paradigm? ISRN Oncol 2012;2012:1–10.
4. Neiva F, Mesquita J, Paco Lima S, et al. Thyroid carcinoma in children and adolescents: A retrospective review. Endocrinol Nutr 2012;59:105–108.
5. O’Gorman CS, Hamilton J, Rachmiel M, et al. Thyroid cancer in childhood: A retrospective review of childhood course. Thyroid 2010;20:375–380.
6. Kiratli PO, Volkan-Salanci B, Gu¨nay EC, et al. Thyroid cancer in pediatric age group: An institutional experience and review of the literature. J Pediatr Hematol Oncol 2013;35:93–97.
7. Rivkees SA, Mazzaferri EL, Verburg FA, et al. The treatment of differentiated thyroid cancer in children: Emphasis on surgical approach and radioactive iodine therapy. Endocr Rev 2011;32:798–826. 8. Grigsby PW, Gal-or A, Michalski JM, et al. Childhood and adolescent thyroid carcinoma. Cancer
2002;95:724–729.
9. Demidchik YE, Demidchik EP, Reiners C, et al. Comprehensive clinical assessment of 740 cases of surgically treated thyroid cancer in children of Belarus. Ann Surg 2006;243:525–532.
10. Zimmerman D, Hay ID, Gough IR, et al. Papillary thyroid carcinoma in children and adults: Long-term follow-up of 1039 patients conservatively treated at one institution during three decades. Surgery 1988;104:1157.
11. Yamashita S, Saenko V. Mechanisms of disease: Molecular genetics of childhood thyroid cancers. Nat Clin Pract Endocrinol Metab 2007;3:422–429.
12. Xing M. BRAF mutation in thyroid cancer. Endocr Relat Cancer 2005;12:245–262.
13. Fagin JA, Mitsiades N. Molecular pathology of thyroid cancer: Diagnostic and clinical implications. Best Pract Res Clin Endocrinol Metab 2008;22:955–969.
14. Elisei R, Ugolini C, Viola D, et al. BRAFV600E mutation and outcome of patients with papillary thyroid carcinoma: A 15-year median follow-up study. J Clin Endocrinol Metab 2008;93:3943–3949. 15. Penko K, Livezey J, Fenton C, et al. BRAF mutations are uncommon in papillary thyroid cancer of young
patients. Thyroid 2005;15:320–325.
16. Kumagai A. Low frequency of BRAFT1796A mutations in childhood thyroid carcinomas. J Clin Endocrinol Metab 2004;89:4280–4284.
17. Lima J. BRAF mutations are not a major event in post-chernobyl childhood thyroid carcinomas. J Clin Endocrinol Metab 2004;89:4267–4271.
18. Suchy B, Waldmann V, Klugbauer S, et al. Absence of RAS and p53 mutations in thyroid carcinomas of children after Chernobyl in contrast to adult thyroid tumours. Br J Cancer 1998;77:952–955. 19. Furlan JC, Bedard YC, Rosen IB. Role of fine-needle aspiration biopsy and frozen section in the
management of papillary thyroid carcinoma subtypes. World J Surg 2004;28:880–885.
20. Kurian EM, Dawlett M, Wang J, et al. The triage efficacy of fine needle aspiration biopsy for follicular variant of papillary thyroid carcinoma using the Bethesda reporting guidelines. Diagn Cytopathol 2011;40:E69–E73.
21. Sujoy V, Pinto A, Nose´ V. Columnar cell variant of papillary thyroid carcinoma: A study of 10 cases with emphasis on CDX2 expression. Thyroid 2013;23:714–719.
22. Ghossein R, Livolsi VA. Papillary thyroid carcinoma tall cell variant. Thyroid 2008;18:1179–1181. 23. Lee X, Gao M, Ji Y, et al. Analysis of differential BRAFV600E mutational status in high aggressive
papillary thyroid microcarcinoma. Ann Surg Oncol 2008;16:240–245.
24. Oler G, Ebina KN, Michaluart P, et al. Investigation of BRAF mutation in a series of papillary thyroid carcinoma and matched-lymph node metastasis reveals a new mutation in metastasis. Clin Endocrinol 2005;62:509–511.
25. Park SY, Park YJ, Lee YJ, et al. Analysis of differential BRAFV600E mutational status in multifocal papillary thyroid carcinoma. Cancer 2006;107:1831–1838.
26. Zatelli MC, Trasforini G, Leoni S, et al. BRAF V600E mutation analysis increases diagnostic accuracy for papillary thyroid carcinoma in fine-needle aspiration biopsies. Eur J Endocrinol 2009;161:467–473. 27. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009;19:1167– 1214.
28. Silberstein EB, Alavi A, Balon HR, et al. The SNMMI Practice Guideline for Therapy of Thyroid Disease with 131I 3.0. J Nucl Med 2012;53:1633–1651.
29. Kimura ET, Nikiforova MN, Zhu Z, et al. High prevalence of BRAF mutations in thyroid cancer: Genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res 2003;63:1454–1457.
30. Puxeddu E. BRAFV599E mutation is the leading genetic event in adult sporadic papillary thyroid carcinomas. J Clin Endocrinol Metab 2004;89:2414–2420.
31. Xu X, Quiros RM, Gattuso P, et al. High prevalence of BRAF gene mutation in papillary thyroid carcinomas and thyroid tumor cell lines. Cancer Res 2003;63:4561–4567.
32. Gouveia C, Can NT, Bostrom A, et al. Lack of association of BRAF mutation with negative prognostic indicators in papillary thyroid carcinoma: The University of California, San Francisco, Experience. JAMA Otolaryngol Head Neck Surg 2013;139:1164–1170.
33. Nikiforova MN, Ciampi R, Salvatore G, et al. Low prevalence of BRAF mutations in radiation-induced thyroid tumors in contrast to sporadic papillary carcinomas. Cancer Lett 2004;209:1–6.