Any correspondence concerning this service should be sent to the repository administrator:
[email protected]
Identification number:
DOI: 10.1016/j.irbm.2014.09.002
Official URL:
http://dx.doi.org/10.1016/j.irbm.2014.09.002
This is an author-deposited version published in:
http://oatao.univ-toulouse.fr/
Eprints ID: 13952
To cite this version:
Doumbouya, Mamadou Bilo and Kamsu-Foguem, Bernard and Kenfack,
Hugues and Foguem,
Clovis
A framework for decision making on teleexpertise
with traceability of the reasoning
.
(2015) IRBM - Innovation and Research in
BioMedical engineering, vol. 36 (n° 1). pp.40-51. ISSN 1959-0318
O
pen
A
rchive
T
oulouse
A
rchive
O
uverte (
OATAO
)
OATAO is an open access repository that collects the work of Toulouse researchers and
makes it freely available over the web where possible.
A
framework
for
decision
making
on
teleexpertise
with
traceability
of the reasoning
M.B. Doumbouya
a,b,
B. Kamsu-Foguem
b,∗,
H. Kenfack
a,
C. Foguem
c aUniversityofToulouse,FacultyofLaw,2rueduDoyenGabrielMarty,31042ToulouseCedex9,FrancebLaboratoryofProductionEngineering(LGP),EA1905,ENIT-INPTUniversityofToulouse,47Avenued’Azereix,BP1629,65016,TarbesCedex,France cCentreforFoodandTasteSciences(CSGA),UMR6265CNRS,UMR1324INRA,UniversityofBourgogne,9EBoulevardJeanned’Arc,21000Dijon,France
Abstract
Thispaperprovidesamethodologicalframeworkfordecisionmakingprocesstoensureitstraceabilitygenerallyinthecontextoftelemedicine andparticularlyintheactofteleexpertise.Thisactpermitstomedicalprofessionalsand/orhealthprofessionalstocollaborateinordertotake suitabledecisionsforapatientdiagnosisortreatment.Themainproblemdealingwithteleexpertiseisthefollowing:Howtoensurethetraceability ofthedecisionsmakingprocess?Thisproblemissolvedinthispaperthroughaconceptualisationofarigorousframeworkcouplingsemantic modellingandexplicitreasoningwhichpermitstofullysupporttheanalysisandrationalefordecisionsmade.Thelogicalsemanticunderlying thisframeworkistheargumentativelogictoprovideadequatemanagementofinformationwithtraceabilityofthereasoningincludingoptions andconstraints.Thusourproposalwillpermittoformallyensurethetraceabilityofreasoningintelemedicineandparticularlyinteleexpertisein ordertofavourthequalityoftelemedicine’sprocedurechecking.Thistraceabilityistoguaranteeequitableaccesstothebenefitsofthecollective knowledgeandexperienceandtoprovideremotecollaborativepracticeswithasufficientsafetymargintoguardagainstthelegalrequirements. Anillustrativecasestudyisprovidedbythemodellingofadecisionmakingprocessappliedtoteleexpertiseforchronicdiseasessuchasdiabetes mellitustype 2.
1. Introduction
Telemedicineisakindofremotemedicalpractice,inwhich thereisthe possibilityof makingmultipleactorsworking to-gether and allowing their collaborations in the diagnosis or treatmentofadisease,bythemeansoftelecommunicationand informationtechnologies.Thetelemedicineinvolveseither pa-tientwithoneorseveralhealthprofessionals(HP)andamong themamedicalprofessional,oracollaborationbetweenagroup ofhealthprofessionals(HP)andamongthematleastone med-icalprofessional(MP).Telemedicinepermitsto[1]:
* Correspondingauthor.
E-mailaddresses:[email protected](M.B. Doumbouya),
[email protected](B. Kamsu-Foguem).
• establishadiagnosis,
• provideforariskypatientamedicalmonitoringinthe con-textofpreventionoratherapeuticmonitoring,
• requireexpertadvice,
• prepareatherapeuticdecision,
• prescribeproducts,prescribeorperformactsorservices,
• monitorapatient.
Thispractice isveryusefulinseveraldomainsof application wheremedicalexpertisesareneeded,forexample:
• Ruralarea[2],wherethereisdifficultyinhealthcarefor remote rural areasbecause theyare unableto attract, af-fordorretainspecialityproviders.Sotelemedicinecanhelp solving theseissuesby allowing access tospecialists re-gardlessoflocation.
• Corrections[3],inthisareatelemedicineallowsprison fa-cilitiestodeliverhighmedicalqualitywithoutthecostand dangers ofinmatetransportationandtheneedforclinical specialisttoenterthefacility.
Therearealsomanyfieldsoftelemedicineapplicationsuchas schools,mobilehealth,disasterrelief,industrialhealth,. . .
Thepracticeof telemedicine isdividedintothesefiveacts listedbelow[1]:
1. teleconsultation:adoctorgivesaremoteconsultationtoa patient,thelattercanbeassistedbyahealthprofessional. The patientand/or thehealthprofessional gives informa-tion for their side, the remote doctor then performs the diagnosis.
2. teleexpertise:adoctorseeks remotelytheopinionof one ormoreofhiscolleaguesonthebasisofthediagnosticand therapeutic needs tofoster concretediscussionsaimed at solvingthemedicalproblemsrelatedtoapatient’scare. 3. telemonitoring:adoctormonitorsandinterpretsremotely
apatient’smedicalparameters.Therecordingandthedata transmissioncanbeautomatedorperformedbythepatient himselforbyahealthcareprofessional.
4. teleassistance:adoctorattendsremotelyotherhealth pro-fessionalperformingamedicalact.
5. medical regulation: this is specific to the French tele-medicinespecificationwheredoctorsofcentre15establish byphonefirstdiagnosistodetermineandtriggerthebest answersuitabletothenatureofthecall.
Inthispaperweareinterestedintheteleexpertiseactwhich isusedbyhealthcareprovidertomakeandtakedecisions con-cerningapatient’streatment.Becauseimportantdecisionsare madeinthisact,thentheresponsibilityofeachparticipantis en-gaged.Currently,duetothelackofinteroperabilityofHospital InformationSystem(HIS)orabsenceofcomputerisedpatient recordsinfacilities,thetraceabilityofdecisionsand informa-tion that are used for decisions is ensured by atelemedicine informationsystem.Withinthistelemedicineinformation sys-tem,it issomeformstobecompleted thatcanbe specificto certainspecialities. Thecontentisstructuredaccordingtothe processinthemedicalprocedure. Thishelpsassistingthe ap-plicantinmakingitsrequestforanopiniontotheexpert,andto facilitatetheprocessingoftheapplicationbytheexpert.Some formscan sometimesperform by calculations for knowledge discoveryin databases. Unfortunately,some healthproviders notalwaystakethetimetocompletetheseforms.Butwhatever the means of communicationused, the most important point isthe traceability of decisions. Thisisour problem,in other words,howtoensurethetraceabilityofthedecisionstakenby healthproviders?
To achieve this goal, we propose in this paper two main contributions.First,thepaperpresentsthearchitecturethatwe proposetoshowtheinteractionbetweenparticipantsandsome ontological concepts.This architectureincludesan important componentcalledargumentativelogic.Thiscomponentisused inourarchitecturetoensurethetraceabilityofthedecisionsin
teleexpertisetofavourthecheckingofthetelemedicine’s pro-ceduresquality.Second,thepaperwillfocusonthecomponent wherewedetailedbyausecaseitspurpose.
Thisintegratedapproachincludesasemanticformalisation ofcollaborativeinformationmodelsthatassistsmedicalactors atalllevelstoshareknowledgeandintegrateethicalneedsin their telemedicine services: thisshowsthe novelty and origi-nalityofourworki.e.integratingsemanticmodellingandlaws conceptsforaidingindecisionmaking.
2. Objective
Themainpurposeofthispaperistoproposea methodolog-icalframework coupling semantic modelling and argumenta-tion for aiding medical professionalintheir decision making process.Infact, theproposedframeworkwill permitto med-icalprofessionals tomanage medical informationconcerning their patients.Sobyourproposal wewant togive innovative solutions in the practice of telemedicine which will lead to increasetelemedicineprograms’effectiveness.Infactour pro-posalcombines conceptualgraphsandDung’s argumentation system (argumentative logic).With thisapproach, we aim to propose arigorousmodellingframeworksinceitincludes ar-gumentativereasoningwhichhaveamathematicalfoundation andconceptualgraphsbasedonontologicalmechanisms.This argumentativelogicwillpermittoensurereasoningtraceability inastructuredmannerwhiletheontologicalmodels (concep-tualgraphs)willpermitreasoningvisualisation(bytheuseof CoGuisoftware)andseemoreensuringsemantic interoperabil-ity.Bymakingthistooleasytousewecanencouragemedical professionalstochange their habitsbyusing thesenew tech-nologiesinthepracticeofmedicalacts.Weaimalsotoprovide atoolwhichwillpermitastrongcommunicationamong medi-calprofessionalsandinthesameoccasiontoshareknowledge and experiences. For example, when a medical professional cannottake decisionsinfront of specificdiagnosis, byusing thesystemhecanmakesomequeriesinordertoknowifthere hasbeen asimilarcaseinthe past.Ifyes,thenhe canknow whatdecisionshavebeentakenforthisdiagnosis,ifno,hecan thencontactothermedicalprofessionalswhoarespecialisedin aparticulardomainandhaveathoroughunderstandingto re-motelyshareexperienced knowledge during the teleexpertise activity.
3. Stateoftheart
Inthissection,westartwithastateofthearttoshowwhat hasbeenalreadydonefortheargumentationandthetraceability ofthedecisionsintheliterature.
3.1. Relatedwork
Inourteammanyworksdealingwithconceptualgraphsfor visualknowledgerepresentationhavebeenachieved.However, the global researchapproaches are not the sameand each is useful for different purposes. The work of Potes Ruiz et al.
[4]proposesamethodologicalframeworkforexperience feed-backprocessesandintheirapproachtheycombineconceptual graphswithassociationrulesmining.Themainobjectiveisto analyse the knowledge extracted from industrial information systems in order toimprove the management of the mainte-nanceactivity.Thisapproachisquitesimilartoourssince,the proposedframework permits tomanage andgenerate knowl-edgefrom informationbasedonpastexperiences,inorderto make suitable decisionsinaparticular context.However,the workofPotesRuizetal.[4]didnotintendtoaddressgeneral aspects of the qualityof collaborative decision making.The work of Kamsu-Foguemetal.[5]proposes amethodological frameworkforaformalverificationapproachofmedical proto-colsandintheirapproachtheycombineconceptualgraphswith computationaltreelogic.Theaimistoformalisemedical pro-tocoldefiningtemporalreasoningpathsforthemonitoringand preventionof specificdiseases(e.g.nosocomialinfections).It doesnotcoveraspectsrelatedtotheremotecollaboration,but wesharethegoalofdevelopingthemeanstofacilitatethe un-derstanding of reasoning steps.In thoseterms, our approach combines conceptualgraphs withargumentativereasoning in themedicalcollaborationsetting.Sothismustmakeitpossible clearlyandnoticeablytoidentifytheargumentationsdrawnup orreceivedbythecollaborativemedicalteam.Theexchangeof expertiseunderthisnewframeworkwillthereforehelpto sus-taintraceablereasoninginstrumentsandimproveworkquality inthecollaborativesituations,suchas intheteleexpertise be-tweenmedicalprofessionalslocatedatremotesites.
Someworks havebeen donebythe authorsof [6] tohelp healthcareproviderstotakedecisionforapatient’streatment. In theirworktheypresented atool calledVirtual Staff which permitsto havecooperative diagnosis inordertomake deci-sions.TheVirtualStaff permitsdecisionstraceabilityby keep-ing trackof thehistoryof their characteristicelements based onpatientslifeline[6].ThisVirtualStaff isbasedonaSOAP (Subjective, Objective, Assessment, Plan)model [6,7]which permits to the doctors to structure their reasoning and also on a QOC(Question–Options–Criteria) model [6,8]for sup-porttodecision-making.Globallyintheirapproachtheyhave adatabasecalledNautilusDB, fromthisbasistheybuild on-tologiesthataretransformedintoRDF1format.Thentheyuse asearch enginecalledCORESE [9] tonavigate into this on-tology. CORESE interface allowsphysicians to visualise the ontologyandvalidateitbyerrorsdetectionandalsobythe cor-rectionsuggestion.CORESEalsoprovidesanenvironmentfor responsestoqueriesontheontology.Eveniftheirproposal of-fers argumentation ondecisionsandtraceability, butit is too heavytobuildinthewaythattherearedifferentformsofgraphs namelySOAP,QOCusingtheontologygeneratedfroma medi-caldatabase.Thecommonpointswithourproposalisthattheir architectureiscomposedbyontologies,conceptualgraphs han-dledby CORESE andawillingness toexplain the reasoning inanargumentativemanner.UnfortunatelywithCORESEonly conceptualgraphsmodellingfactsarevisualisedandthereisno
1 ResourceDescriptionFramework.
waytovisualisethereasoningprocess.Inourapproachwe pro-poseawaytovisualisethereasoningbytheuseofCOGUI[10] softwareincludingpurposestoeditconstraints,ruleswhichaid inreasoning.Weproposetousetheargumentativelogicto rein-forcetheirformalsemanticsonexplicitelementsfor decision-making, whilst investigating real impact of possible options. Finally inourproposition weintroduce alegalpointof view inthe defined ontologieswhichwill allow toidentify the re-sponsibilityofeachparticipantintheactofteleexpertise.
K.-L. Skillenetal.proposedin[11]anapproachbasedon semantic technologiesfor usermodellingandpersonalisation techniques. Their proposal is adapted for pervasive environ-mentinwhichtheycreateontologicalusermodelsand devel-opedasemanticrule-basedmechanismforthepersonalisation ofcontext-awareservice.TheserulesarecreatedwithSWRL2in
Protégé[12].Thisapproachissomewhatsimilartooursinthe sensethattheyusesemanticmodellingandreasoningoptions. ButtocreatetherulestheyneedadditionalplugininProtégé, thismeansthattheyneedmorethanonelanguage(SWRLfor the rules and OWL3 for the ontological models) whereas in CoGui the rules creator are natively included, thus onlyone languagetohandlebothrulesandontologicalmodels.Astheir approachisbasedonHelp-On-Demandservices,itcanbeused fordecisionaidinginthetelemedicineservices.
3.2. Telemedicineoverview
Telemedicine is the fact to use information systems and telecommunicationin ordertodelivermedical careremotely. Nowadayswiththerisingofnewtechnologies,telemedicineis becomingarealcentreofinterestwithregardtotheresearch do-main.Assaidintheintroduction,telemedicineisbuiltaround fivemainacts.Inthesefiveacts,fourofthemaremore impor-tantnamely:teleconsultation,teleexpertise,telemonitoringand teleassistance.ThesefouractsareillustratedinFig. 1below.
Animportantworkhasbeendonebytheauthorsof[13]in whichtheygiveasystematicreviewofreviewsoftelemedicine. Intheirwork,theyshowthattelemedicinehaspositiveeffects. Andthesepositiveeffectsconcerntherapeuticeffect,health ser-vice improvement, and the use of technical services such as ICTs4[13].Wetalkaboutonlythehealthandthetechnical out-comes.
Eveniftheeffectivenessoftelemedicineisdemonstratedit seems that it still limited and inconsistent in many domains [13].Forexampleintherapeuticactions,thetelemonitoringfor heartfailurehasitslimitsintermsofimprovingeffectiveness andinfluencinghealings[13,14].Theelementsdescribingthat evidenceonthelimitsandtheinconsistencies oftelemedicine concern decision support tools, chronic diseases, computer-based cognitive behavioural therapyand so on. Forthe tele-expertisepointofviewmanyeffortsarecurrentlybeingmade concerningtoolsusedinitspractice.
2 SemanticWebRuleLanguage. 3 WebOntologyLanguage.
Fig. 1. Main acts of telemedicine.
4. Materialsandmethods
In this section we show the different steps followed to achieveourgoal, namelythe proposedcommunication archi-tecture and the explanation of the abstract argument-based framework for decision making called argumentative logic. We introduce this abstract framework in our work because, it will permit us to achieve our goal, namely: ensuring for-mallythetraceabilityofthereasoningforcheckingthequality oftelemedicine’s procedures.Inadditionbytheuseof Cogui software,the reasoning could bevisualised easilywhichis a value-addedcontrarytothepreviousworks.
4.1. Proposedarchitecture
E. Nagebaet al. [15] proposeda methodology for know-ledge-based framework construction inpervasive computing. Thismethodologycontainsaknowledgemeta-model descrip-tionandformalisationthatcanbeinstantiatedindifferent sce-narios and contextual situations. The described knowledge-baseddesignmethodologyprovidesaframeworkfor problem solvinganddecisionmakinginagivendomain.Inparticularthe authorsshowedatechnicalandempiricalresultintelemedicine domainfor the purpose of organisational assessment and de-velopment.Butintheirworktheydonotshowthattheir pro-posal guarantees the traceability of decisions. Thus the pro-posedworkinthispaper willpermittoovercome thisfailure andtovisualiseeasilythereasoning.Weaddinourarchitecture
an additional component called argumentative logicin order toguaranteethetraceabilityofdecisionsforensuringformally the decisionprocesstraceability infavouringthe checkingof telemedicine’sproceduresquality.
Inthisarchitectureweproposeamethodologicalframework coupling:
• semanticmodelling
• explicitreasoning
• ontology(includingmedicalandlegalconcepts)modelled byconceptualgraphs.
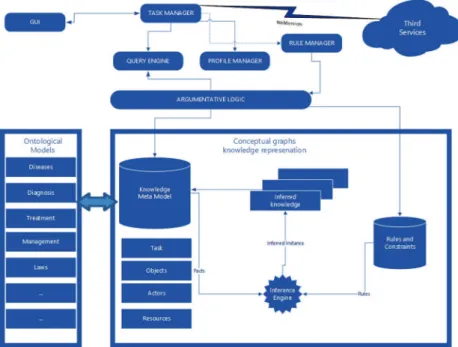
The proposed architecture is depicted in Fig. 2 below. It representsourproposed architectureinwhichthecomponent developingandimplementingargumentativelogicisakindof middleware between the GUI and the knowledge base. This componentisbuiltfromthedefinitionandpropertiesrelatedto Dung’sargumentationsystem(Section4.2.2).Itretrievesdata fromtheknowledgebaseaccordingthemedicalprofessionals’ queriesandcomputesacceptedorrejectedadvicesintheactof teleexpertise.Theargumentativelogiccomponentlikewise al-lowsthegenerationofaframeworkforsharingofexperiences, analysesandproposalsbetweenremotemedicalprofessionals.
Our architecture iscomposed of eleven maincomponents listedbelow:
• GUI: auser friendly interface whichpermitsthe user to accessthesystemfunctionalities.
Fig. 2. System architecture.
• Thirdservices:itincludesseveralservicessuchas hospi-tals, clinic,medicalcentre,PMR5hostwherepatientdata arestoredandorganisationsuchassocialsecurity.
• Queryengine:itisalreadyincludedinCoGuisoftware.It permitstoqueryandgetresponsefromtheknowledgebase foraidingmedicalexpertsinthedecisiontaking.
• Profilemanager:ithandlesuserprofile.Itpermitsto in-formthetaskmanagerwhichuserisconnectedinorderto loadinformationconcerningthisuser.
• Rulemanager:itiscontactedbythetaskmanagertoapply rulesonaspecificquery.
• Argumentative logic: itis thecomponent whichensures the traceability of the decisions in a structured manner. And as previouslysaid,it retrievesdatafrom the knowl-edgebaseaccordingthemedicalprofessionals’queriesand computesacceptedorrejectedadvicesintheactof teleex-pertise.Thiscomponentwillbedetailedmorepreciselyin thenextsection.
• Ontological models: the ontological models are used in eHealth to make medical decision support systems [15]. Ontologies are instruments used in the knowledge engi-neeringcommunityforconceptsandinterrelations specifi-cation[16,17].Ontologiesarealsousedforcontext mod-elling, management in pervasive environment and they permit tosolve semanticinteroperability[18,19]. Ontolo-giesarestillanemergingresearchanddevelopmentareafor telemedicinetasksupport[20].Inourarchitecture, ontolog-icalmodels are definedby diagnosis,management, laws, diseases,etc.Thediseasesontologywasconstructedby in-formationcollected inICD6-10[21].The authorsof [22]
5 PersonalMedicalRecord.
6 InternationalClassificationofDiseases.
designedanontologyincorporatingcorelegalconceptsthat weintegratedintoourarchitecture.
• Knowledgemetamodel:itisasetofgenericand domain-independentontologicalmodelsandtheassociationswhich connectthesemodels[15].In ourarchitecturethe knowl-edge meta-model includes Task, Objects, Actors, Re-sources.
• Inferenceengine:itpermitstoperformrule-based reason-ing.TheinferenceengineisincludednativelyinCoGui.
• Rulesandconstraints:itisakindofdatabasewherethe rulesandconstraintsaredefined.In CoGuithisisdefined byRules,NegativeconstraintsandPositiveconstraints.
• Taskmanager:allthetasksviatheGUIaredonebythe task manager. Indeed it permits to access the query en-gineinordertoqueryandgetresponsefromtheknowledge base.Andalsowhenqueryingtheknowledgebase,thetask managercancontact therule managerfor applying some rulesandthespecifiedrequest.Itcanconnecttothe Inter-netviawebservicesoversecureHTTPS7connectionstoget patientmedicalrecordandsomeadditionalinformationif needed.ThereturnformatofthewebservicesisinXML8 [23]forensuringthesyntacticalinteroperability.
4.2. Abstractargument-basedframeworkfordecisionmaking: Argumentativelogic
The argumentative logic as said previously is a rigorous frameworkwhichpermitsdecisionsjustificationwith traceabil-ityofreasoningincludingoptionsandconstraints.
7 HyperTextTransferProtocolSecure. 8 ExtensibleMarkupLanguage.
4.2.1. Differenttypesofarguments
AccordingtoAmgoudandPrade[24],therearetwotypesof arguments,namely:
• epistemic arguments:based on believes andthemselves groundedonlyonbelieves.
• practical arguments:based onoptionsandare madeby bothbelievesandpreferencesorgoals.
Generallywecanhavethesetwotypesofargumentsandit is thecontextthatwilldeterminewhichonetoimplement.
4.2.2. Acceptabilitysemantics
Aboveall,wedefinewhatisadecisionframework(system) [25]alsocalledargumentation-basedframeworkAF[24]. Definition 1. An (argumentation-based) decision framework AFisacouple(A,D)where:
• Aisasetofarguments,
• Disasetofactions,supposedtobemutuallyexclusive,
• action:A→Disafunctionreturningtheactionsupported byanargument.
Definition 2. From an argumentation-based decision frame-work (A,D), an equivalentargumentation framework AF =
(A,Def)isbuiltwhere:
• Aisthesamesetofarguments,
• Def⊆A×Aisadefeatrelationsuchthat(α,β)∈Def if
action(α)6=action(β).
Definition3. LetAF=(A,Def)beanargumentation frame-work,andletB⊆A
• Bisconflict-freeiftherearenoα,β∈Bsuchthat(α,β)∈ Def.
• B defendsanargumentαiff∀β∈A,if(β,α)∈Def,then
∃γ ∈Bsuchthat(γ ,β)∈Def.
Definition4(Acceptabilitysemantics).LetAF=(D,A,Def)
beadecisionsystem,andBbeaconflict-freesetofarguments.
• BisadmissibleextensioniffitdefendsanyelementinB.
• B isapreferredextensioniffBisamaximal(w.r.t.set⊆) admissibleset.
• B isastableextension iffitis apreferredextension that defeatsanyargumentinA\B.
Bytheseacceptabilitysemanticstheauthorsof[24]identify severalarguments’statuswhicharedepictedbelow:
Definition 5 (Argument status). Let AF=(D,A,Def) be a decisionsystem,andε1,. . . ,εxitsextensionsunderagiven
se-mantics.Leta∈A.
• aisskepticallyacceptediffa∈εi,∀εi withi=1,. . . ,x.
• aiscredulouslyacceptediff∃εi suchthata∈εi.
• aisrejectediff∄εi suchthata∈εi.
Theconsequencewhichfollowsimmediatelyfromtheabove definitionisasfollows:
Property1.Let AF=(D,A,Def)bea decisionsystem,and
ε1,. . . ,εxitsextensionsunderagivensemantics.Leta∈A.
• aisskepticallyacceptediffa∈Txi=1εi
• aisrejectediffa /∈Sxi=1εi
Thecomponentoftheproposedarchitecturecalled argumen-tativelogicisbuiltfromthesedefinitionsandproperty.Inthis componentthedefinitionsandpropertiesaretransformedinto algorithms.Sowhenmedicalprofessionalsentersomequeries, theyare relayedtotheargumentativelogicwhichextracts the answersfromtheknowledge basetoshowtheaccepted argu-mentsinaspecificactofteleexpertisebasedontheunderlying algorithms.Byapplyingtheestablisheddefinitionswebuild al-gorithmsforextractingconflict-freesets,admissibleextensions andpreferredextensionsandwiththepropertieswebuildan al-gorithmforknowingtheacceptedandtherejectedargumentsin thedecisionmakingprocess.Thesealgorithmsarepartofthe argumentativelogiccomponent.
5. Analysisofresultswithcasestudyfindings
Inthissectionwewillshowanapplicabilityofthe argumen-tativelogicthankstoacasestudyinthecontextofteleexpertise.
5.1. Casestudy
Application case.The attendingphysician (orfamily doctor) ofMrsC.,a80yearsoldfemalewitha10yearshistoryofhigh bloodpressure,requestedamedicalopinionofthegeriatrician becausehispatientpresentedasub-acuteconfusionsymptoms. Physicalexaminationwasnormalapartofblurredand/or dimin-ishedvision’scomplaints.Thegeriatriciandisclosedachronic hyperglycemia[fastingbloodglucosevalueat20mmol/Land hemoglobinA1c(glycosylatedhemoglobin)higherthan14%] yielding diagnostic of unrecognizeddiabetesmellitus type2. Laboratoryanalysisdisplayedarenalimpairment(clearanceof creatinineat24ml/min/1.73 m2)withproteinuria(2 g/24 H). Firstly by the provided system the geriatrician makes some queries to knowif there has been asimilar casein the past. If yes,he could then havethe answerson how to treatsuch patient;ifno,heusesthe samesystem toaskforexpertiseto the Internist(forthe renalcomplicationof diabetesmellitus), the Ophthalmologist (for the ocular complication of diabetes mellitus) and the Diabetologist (for the management of hy-perglycemia). Theexperts’ advicesare collectedas shownin Table 1(Stakeholders’ argumentation).From the elementsof thistablethereisbuiltthegraph ofattacksaccordingthe op-tionparameterinthetable(theargumentswiththesameoption donot attackeach other).On thisgraphof attackstherewill
Table 1
Stakeholdersargumentation.
Stakeholders Reasons Options Concerns Goals
1 Internist Hedoesnotwanttomakeinvasive
in-vestigation, he prefers medication ap-proaches in this context with less of sideeffectsandthepreventionoffurther micro-vascular (eye and kidney) and macro-vascular complications of Dia-betesMellitus
ցProc Ensuringagoodqualityof lifeforthiselderlypatient
Riskreductionsuchassideeffectsand preventionoffurthermicro-vascularand macro-vascularcomplicationsrelatedto theDiabetesMellitus
2 Ophthalmologist Hewantstoperforminvasive investiga-tionsontheeyetoappreciatetheextent ofretinalveinthrombosisandthe im-portanceoftheassociatedoedema.He advocatesthenanintra-ocularinjection ofananti-oedematoustreatment
րProc Ensuringagoodqualityof lifeforthiselderlypatient
Appreciationoftheextentofretinalvein thrombosis, theimportance of associ-atedoedemaandcuring patientvisual disorders
3 Geriatrician Hewouldadminister treatment to the
patienttopreventcognitiveimpairment suchasAlzheimerdiseasecommonin theelderly
րProc Ensuringagoodqualityof lifeforthiselderlypatient
Preventionofconditionswhichleadto cognitiveimpairment
4 Diabetologist Hewouldprescribeas soonas
possi-bletreatmentstothepatientinorderto preventhislossofsight,knowinghe al-readyhasvisualdisordersandtype2 di-abeteswhichcanleadtotheblindness ofthepatient.
րProc Ensuringagoodqualityof lifeforthiselderlypatient
Avoidingpatient’slossofsight
beappliedtheargumentativelogictocomputetheacceptedand rejected arguments.Finally theGeriatrician compares the ac-ceptedargumentsandthenbysomeparameterstakesthefinal decisionsandthesedecisionswill bestoredfor future exper-tise.
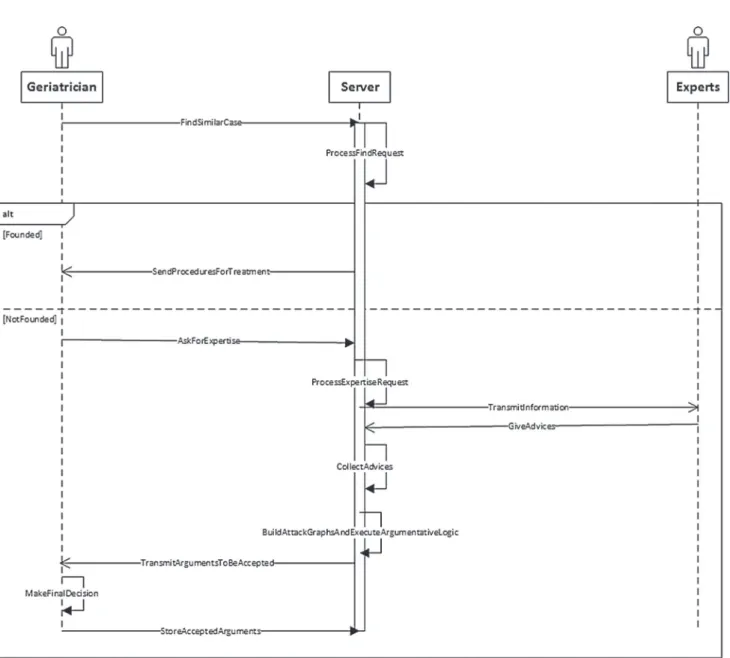
The sequence and collaboration diagrams (Figs. 3 and 4) illustrate ourcasestudy. Thesediagramsare basedonUML9
[26].
Inthesequencediagramabovethe“Experts”representsthe groupcomposedoftheOphthalmologist,Diabetologistand In-ternistwhom arecontacted forexpertise. Inthe followingwe describesomemethodstofostermoreunderstanding:
• AskForExpertise: inthismethodthe geriatricianprovides allinformationconcerningthepatient(withhisconsentof course),andtheneededremoteexperts.Bythesame occa-sionhesendstotheserverhisadvicesifonlyhecantakea decisionaccordinghisskillsandhisexperiences.
• ProcessExpertiseRequest:whentheserverreceivesthe ex-pertiserequestitcomputesittoknowtheavailable physi-ciansandthentransmitsbythemethod TransmitInforma-tion(whichisakindofmulticast)themthemedical infor-mationconcerningthepatientiftheyaccepttoparticipate inthisactofteleexpertise[27].
• GiveAdvices:theremote physiciansgivetheiradvices ac-cordingtotheparametersdescribedinTable 1.Thismethod shouldincludesomeparameterstoknowwhichphysician’s answerhasbeenreceived.
9 UnifiedModellingLanguage.
• BuildAttackGraphsAndExecuteArgumentativeLogic: this methodcreatesthe graphofattacksonwhichwill be ap-pliedtheargumentativelogictoidentifytheargumentsthat shouldbeacceptedornot.
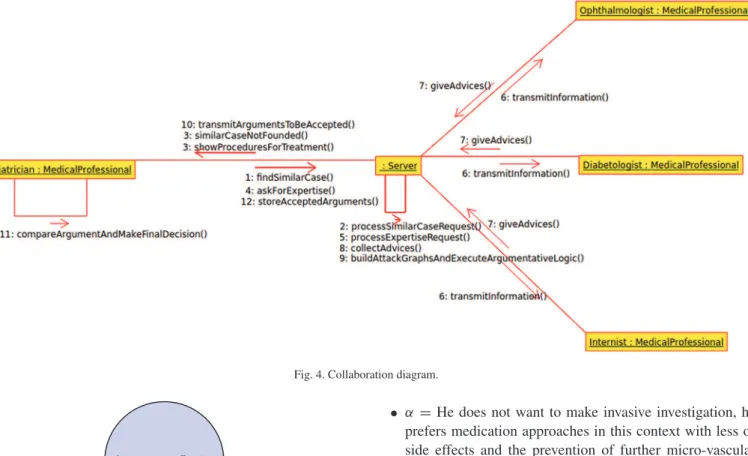
Fig. 4 representsthe collaborationdiagramthat shows the interactionbetweenthedifferententitiesof ourproposal. Un-like tothepreviousdiagram,itshowsexplicitlythe messages exchangedbetweenthedifferententities.Whenthegeriatrician asksforfindingsimilarcases,oneoftheseresponsescanbe re-turned:
• Similarcasesfounded,thentheserverreturnthedifferent procedurestofollowinordertoefficientlytreatthepatient;
• Similarcasesnotfounded,andthentheserverinformsthe geriatricianthatthereisnosuchsimilarcase.
As said previouslyinthe sequence diagram’s comments, the messagegiveAdvices() shouldhave somefunctional parame-tersinordertodistinguishthephysician fromwhom advices havebeenreceivedbytheserver.
In thefollowing, weshow thedifferentstepstofollowfor thedecisionmakingprocess.Webelievethatthereasoning el-ementssetoutinthiscasestudyishelpfulforthepurposesof illustratingtheessential dimensionsofthesuggesteddecision makingprocessonteleexpertisewithtraceabilityofthe reason-ing.Wealsosubscribetotheviewthatthedescribedelements areonlytheverynoticeablepartsofthatproposedframework, whereasothersareunderdevelopmentandnotyetconsolidated. Inotherwordswewilllinkthedifferentcomponentsandalso includeconceptualgraphsinthedesigntoeasilypermitthe vi-sualisationofthereasoning.
Fig. 3. Sequence diagram.
5.1.1. Positioningofthestakeholders
• Internistisamedicalprofessionaldealingwithadult dis-eases.Heisapolyvalentcaregiver,particularlyskilledin the multi-system disease processes. He would not make invasive investigations or treatments yet because the re-sultsof invasivetechniquesproposedare diverse(benefit, risk,patientsatisfaction,etc.)Inthisparticularcase,heis againstinvasiveinvestigationsortreatmentsyetinthis el-derlywomantakingintoaccounttheageofthepatientand the risk-to-benefitratio ofinvasive actsinthiscontexthe wouldnotmakeinvasiveinvestigations.Heprefers medica-tionapproachesinthiscontextwithlessofsideeffectsand theprevention offurthermicro-vascular(eyeandkidney) andmacro-vascularcomplicationsofDiabetesMellitus.
• Ophthalmologist is a medical professional for eye dis-eases. Hewantstoperform invasiveinvestigationsonthe eyetoappreciatetheextentofretinalveinthrombosisand the importance of the associated oedema. He advocates
thenanintra-ocularinjectionofananti-oedematous treat-ment.
• Geriatricianis amedical professional for the elder per-son.Hewouldadministertreatmenttothepatienttoprevent cognitiveimpairmentsuchasAlzheimerdiseasecommon intheelderly.
• Diabetologist is a medical professional for diabetes. He would prescribeassoonas possibletreatmentstothe pa-tientinordertopreventhis loss ofsight,knowing he al-ready hasvisualdisordersandtype2 diabeteswhichcan leadtotheblindnessofthepatient.
5.1.2. Modellinginformationavailableinstructured arguments
Themedicalprofessionalhasthechoicebetweenminimising andmaximisingdiagnosticprocedures[28]:
• Proceduresminimisation(ցProc):itlimitsthecare’s in-vasiveness, risks such as selection of resistant bacteria,
Fig. 4. Collaboration diagram.
Fig. 5. Node representation.
nosocomialinfections,adversedrugreactions,thevagaries ofinterventions,. . .andtheircosts;butdiagnosticand ther-apeuticdelaysareobserved;whichcanleadtosevere ethi-calandmedico-legalconsequences.
• Proceduresmaximisation(րProc):it permitstoreduce theriskof missingdiagnosticortherapeuticopportunities (e.g. emerging medical problem such as bacterial infec-tionwithpossiblelonger-termeffects).Howeverindividual andcollectiverisksincreasesignificantlyduetohuman er-rorsandmedicaldevicesafety.Thusmedicaldecisionsare takenbythecomparisonofthethreatsofahealthstatusto itsrelatedstrengths.
These two diagnostics procedures represent the options (ac-tions)ofourdecisionsystemthatwillpermittodeterminethe argumentswhicharefor oragainstanoption.Table 1gathers thedifferentarguments(Reason)whichwillpromoteagoaland supportaction(Option).
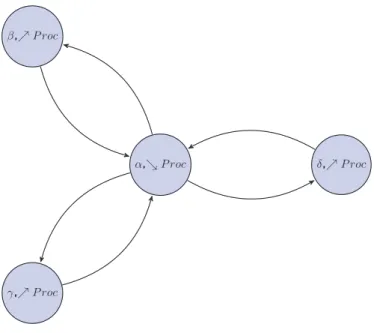
5.1.3. Graphofattacks
TheGraphofattacksconsistsofasetofnodeswithoriented linksbetweenthem.Anode isrepresentbythecouple Argu-ment,Option,thisisdepictedinFig. 5.
AccordingtoTable 1,thedifferentargumentssupportbythe stakeholdersare:
• α=He doesnotwanttomakeinvasive investigation,he prefersmedicationapproachesinthiscontextwithlessof side effects and the prevention of further micro-vascular (eyeandkidney)andmacro-vascularcomplicationsof Di-abetesMellitus,
• β=Hewantstoperforminvasiveinvestigationsontheeye toappreciatetheextentofretinalveinthrombosisandthe importanceoftheassociatedoedema.Headvocatesthenan intra-ocularinjectionofananti-oedematoustreatment,
• γ =Hewouldadministertreatmenttothepatienttoprevent cognitiveimpairmentsuchas Alzheimerdiseasecommon intheelderly,
• δ =Hewouldprescribeassoonaspossibletreatmentsto thepatientinordertopreventhislossofsight,knowinghe alreadyhasvisualdisordersandtype2diabeteswhichcan leadtotheblindnessofthepatient.
Sincethegraphsofattacks[25]aremadefromargumentswith thesameconcern,soweassumeherethatallstakeholdershave thesameconcernasfollows:Ensuringagoodqualityoflifefor thiselderly patient.Moreargumentswiththesameoptiondo notattackeachother[25].Thusthegraphofattacksobtainedis depictedinFig. 6.
Thegraphofattacksachievedabovewillpermitstoidentify thedifferentpossibleextensions(representingtheacceptability semantics) onwhichwe willbased fordecision making. Ac-cordingtotheargumentsthedifferentsetswecanhaveare:
• {∅}
• {α},{β},{γ},{δ}
• {α,β},{α,γ},{α,δ},{β,γ},{β,δ},{γ ,δ} • {α,β,γ},{α,β,δ},{α,γ ,δ},{β,γ ,δ} • {α,β,γ ,δ}
Fig. 6. Graph of attacks.
Decisionmakingprocess
Thedifferentextensionsbelowaredeterminedaccordingthe definitionsabove.
• Determinationofconflict-freesets:theconflict-freesets are:{∅},{α},{β},{γ},{δ},{β,γ},{β,δ},{γ ,δ},{β,γ ,δ}.
• Determinationof admissible extensions: theadmissible extensionsidentifiedare: ε1= {∅},ε2= {α},ε3= {β,γ},
ε4= {β,δ},ε5= {γ ,δ},ε6= {β,γ ,δ}.
• Determinationofpreferredextensions:accordingtothe definitionabovethepreferredextensionsthatwecanhave areε2= {α}andε6= {β,γ ,δ}.
SoaccordingtoDefinition5,alltheargumentsarecredulously acceptedinthiscasestudy.Andthentheyareallreturnedtothe requestingphysicianforthefinaldecision,i.e.makingachoice of“maximisingorminimisingtheprocedure”.
Inthiscasethefinaldecisionisto“maximisetheprocedure” becausethepatientisanelderlyandapriorityisgiventothe adviceprovidedbythegeriatrician whichisconducivetothe “maximisationoftheprocedure”.
6. Discussion
Generallyinthecaseoftelemedicine,patientswithdiabetes aresupportedwithtelemonitoringwhichwill ensurepatient’s daily stabilisation. However, in the case of chronic diseases such as diabetesthe telemonitoring mustbe accompaniedby teleexpertise[3] because diabetescanhaveseveraleffects on otherorgans,hencethenecessityof multidisciplinaryteamto providebettertreatmenttothepatient.
Forcultural and financial reasons somepeople are suspi-ciousof newmedical technologies. That is whythe point of viewof the patient’s familyhas consolidatedthe decision of theinternistinmakingnon-invasiveactions.However,he con-sideredfundamentaltoimplementactions(qualityoflife,
tele-dialysis, telemonitoring) for the management of this chronic disease.
Giventhat the argumentativelogicensuresthetraceability ofreasoning:thistraceabilitywillsupportthedecision-making process and its understanding for favouring the checking of telemedicine’sproceduresquality.Thusincaseofjudicial pro-ceedingstheresponsibilitiesofeachofthestakeholderswillbe identified.
The solicitationof ArtificialIntelligencetechniques to de-liverasupportfordecisionmakersattheoperational,tacticalor strategiclevelshaslikewisebeenestablishedinsome compara-bleresearchworks.Fromthat point,theprovisionofdecision supporttools isvery significant for problemsolving incrisis management efforts (e.g.environmental, financial and health crisis).Inparticular,thePANDORAsystem[29]isanadvanced learning environment that can focus more on the adaptable training services tailoredto the respectiveexperiences of the strategic decision makers.On the onehand, the strong point of the PANDORAgeneralarchitectureisthe integrationof a Timeline Reasoning Environment (Behaviour Planner, Crisis Planner,andScenarioExecutor)withanEmotionSynthesizer tosupportpersonalisation.On theotherhand,the strengthof ourproposal is toimprove collaborationbetween health pro-fessionals for the implementation of teleexpertise processes, whetherinprivateclinicsor inpublichospitals (e.g. collabo-rativeactivitiesforthemanagementofcriticalsituations).The principles upon which the telemedicine is founded, by pro-moting conditions of informationdistributionandknowledge sharing,engageincontinuouslearningandexperiential devel-opmentwithapracticalemphasisongeneratingalearning or-ganisation.
For the security andthe data privacy point of view since we arehandlingmedicaldatawhichareverysensitive, hence these constraints should be taken into consideration for the telemedicineacts.Inthisframework,themanipulationofdata andpreparationof dataneedsaninformedconsentprocessof theconcernedpatient,sothathecouldknowhowandwhathis personaldataisusedfor.Giventhatweusesecuredwebservices basedonHttpsprotocoltoretrieveremotemedicalinformation, thedatasecurity isthusguaranteedonourside.From the re-motesites, the datamustbe encrypted:thiswillthen depend onwhatsecurityprotocoltheremotesiteuses.Itisrightthatin EuropethereisnosuchsystemlikeHIPAA10whichguarantees dataprivacyandsecurity[30,31],butsomeeffortsarecurrently beingmadefortheintroductioninFranceofthePersonal Med-icalRecordcalledinFrenchDMP[32].Thesetwoconceptions havesomesimilarpointssuchasauthenticationbeforeaccess, patient’smedicaldataprotection,secureelectronictransferof medicaldata.
7. Conclusion
In this paper we proposed a methodological framework adapted to the telemedicine concept, particularly for the act
ofteleexpertiseinvolvingcollaborationbetweenseveralhealth professionalsandormedical professionalsfordecisions mak-ing.The designed architectureincludes animportant compo-nent called argumentative logic whichpermits to ensure the traceabilityofthedecisionsmakingprocess.Theargumentative logic has been illustrated by a use casein which many par-ticipants(internist,opthalmologist,geriatrician,diabetologist) collaboratetotaketherightdecisionstotreatthepatientwith diabetesandvisualdisorders.Inthiscasestudytheconclusion isthattheargumentssupportedbyopthalmologist,geriatrician and diabetologist (the latterssustain the Procedure maximi-sation) are accepted while the argument of the internist (for Procedureminimisation)isrejected.Thisshowsthatthe
treat-mentsthatwillbe administertothe patienthavetomaximise theprocedure.
The argumentativelogic guaranteesthe traceability of the decisionsinceitshowsthatdifferentstepswhichleadtothe de-cisionsmakingandatlastshowswhichdecisionscanbetaken. Sothat,byensuringthistraceability,itwillpermittofavourthe checkingoftelemedicine’sproceduresquality,alsobytheuse ofCoguisoftwarethereasoningcouldbeeasilyvisualised.In thisperspective,thetraceabilityconsiderationsareofrelevance forlegalproceduretoidentifyandassessthespecific responsi-bilityofeachstakeholders[33–42].
Infurtherwork,we willimplementourproposed architec-ture inordertoverifyit feasibility.Thisimplementationwill consisttoinstantiatetheproposedargumentationsystemin con-ceptualgraphswhichpermittorepresentrulesandconstraints. Theinterestofintroducingsuchformalismisdual:(i)thesame waythatitcanhandletheabstractionofthesystemby redefin-ingthe logicalframeworkofacceptability, (ii)it mayalso be anappropriatemodel torepresentthe internalstructure of ar-gumentsandgenerateconventionalinteractionspreviously in-troduced(graphof attacks).Finally,animportantprerequisite togeneratethemaximumadvantagefromourframeworkisthe developmentofanaccuratesoftwaretotheproposed architec-ture.
References
[1] French department of health. http://www.sante.gouv.fr/deploiement% 2Dde%2Dla%2Dtelemedecine%2Dtout%2Dse%2Djoue%2Dmaintenant. html.
[2]Barjis J,etal.Asustainableandaffordablesupportsystemforrural health-caredelivery,decisionsupportsystems.Elsevier;2013.
[3] DGOS,TechnicalWorkingGroup/InformationSystems,FrenchMinistry ofEmployment,LabourandHealth.Recommendationsforthe implemen-tationofatelemedicineproject,TechnicalDeployment:Urbanizationand infrastructure,March2012.
[4]Potes Ruiz P, Kamsu Foguem B, Grabot B.Generating knowledgein maintenancefromexperiencefeedback.Knowl-BasedSyst2014;68:4–20.
[5]Kamsu-Foguem B,Tchuenté-Foguem G,Foguem C.Verifyingamedical protocolwithtemporalgraphs:thecaseofanosocomialdisease.JCrit Care2014;29(4).
[6]Dieng-Kuntz R, Minier D, R˙užiˇcka M, Corby F, Corby O, Alamar-guy L.Buildingandusingamedicalontologyforknowledge manage-mentandcooperativeworkinahealthcarenetwork.ComputBiolMed 2006;36(7–8):871–92.
[7]Weed LD.Theproblemorientedrecordasabasictoolinmedical educa-tion,patientcareandclinicalresearch.AnnClinRes1971;3(3):131–4.
[8]MacLean A,Young R,Bellotti V,Moran T.Questions,options,and crite-ria:elementsofadesignrationaleforuserinterfaces.IntJHum-Comput Interact1991;6(3–4):201–50.
[9]Corby O,Dieng-Kuntz R,Faron-Zucker C.Queryingthesemanticweb withthecoresesearchengine.In:LopezdeMantaras R,Saitta L,editors. Proceedingsofthe16thEuropeanconferenceonartificialintelligence. ECAI’2004.IOSPress;August2004.p. 705–9.
[10] Cogui: a graph-based tool for building conceptual graphs. http:// www.lirmm.fr/cogui/.
[11]Skillen K-L,Chen L,Nugent CD,Donnelly MP,Burns W,Ivar Solheimb. Ontologicalusermodellingandsemanticrule-basedreasoningfor person-alisationofhelp-on-demandservicesinpervasiveenvironments.Future GenerComputSyst2014;34:97–109.
[12] Protégé:anopensourceontologyeditorandknowledge-baseframework.
http://protege.stanford.edu/.
[13]Ekeland AG,Bowes A,Flottorp S.Effectivenessoftelemedicine:a sys-tematicreviewofreviews.IntJMedInform2010;79(11):736–71.
[14]Chaudhry SI,Phillips CO,Stewart SS,Riegel B,Mattera JA,Jerant AF, etal.Telemonitoringforpatientswithchronicheartfailure:asystematic review.JCardFail2007;13:56–62.
[15]Nageba E,Rubel P,Fayn J.Towardsanintelligentexploitationof hetero-geneousanddistributedresourcesincooperativeenvironmentsofehealth. IRBM2013;34(1):79–85.
[16]Uschold M,Gruninger M.Ontologies:principles,methods,and applica-tions.KnowlEngRev1996;11:93–155.
[17]Christopoulou E,Kameas A.Usingontologiestoaddresskeyissuesin ubiquitouscomputingsystems.AmbientIntell2004:13–24.
[18]Christopoulou E, Kameas A. Gasontology: an ontology for collabo-rationamong ubiquitous computing devices.Int J Hum-Comput Stud 2005;62:664–85.
[19]Chen H,Finin T,Joshi A.Semanticwebinthecontextbrokerarchitecture. In:ProceedingsofthesecondIEEEinternationalconferenceonpervasive computingandcommunications.2004.p. 277–86.
[20]Nageba E, Fayn J, Rubel P. An ontology-based telemedicine tasks managementsystemarchitecture. ConfProcIEEEEng MedBiolSoc 2008;2008:1494–7.
[21] International classification of diseases (icd-10 version:2010. http:// apps.who.int/classifications/icd10/browse/2010/en#/D27.
[22]Breuker J,Hoekstra R.Coreconceptsoflaw:takingcommonsense seri-ously.In:Proceedingsofformalontologiesininformationsystems (FOIS-2004).IOS-Press;2004.p. 210–21.
[23] Extensiblemarkuplanguage(xml).http://www.w3.org/XML/.
[24]Amgoud L,Prade H.Usingargumentsformakingandexplaining deci-sions.ArtifIntell2009;173:413–36.
[25]Bourguet J-R,Thomopoulos R,Mugnier M-L,Abécassis J.Anartificial intelligence-basedapproachtodealwithargumentationappliedtofood qualityinapublichealthpolicy.ExpertSystAppl2013;40(11):4539–46.
[26]Roques P,Vallée F,Muller P-A.UML2enaction:del’analysedesbesoins àlaconception.Eyrolles;2007.
[27]Doumbouya MB, Kamsu-Foguem B, Kenfack H, Foguem C. Telemedicine using mobile telecommunication: towards syntactic interoperabilityinteleexpertise.TelematInform2014;31:648–59.
[28]Chalumeau M,Dubos F,Leroy S,Moulin F,Gendrel D,Bréart G.Quand etcommentdévelopperunerèglededécisioncliniqueauxurgences pédi-atriques?ArchPédiatr2008:718–20.
[29]Amedeo C, Cortellessa G, DeBenedictis R. Trainingfor crisis deci-sionmaking–anapproachbasedonplanadaptation.Knowl-BasedSyst 2014;58:98–112.
[30]Khansa L, Cook DF, James T, Bruyaka O. Impact of hipaa provi-sionson thestock market valueof healthcare institutions, and infor-mationsecurityandotherinformationtechnologyfirms.ComputSecur 2012;31(6):750–70.
[31]Iossifova AR, Meyer-Goldstein S. Impact of standards adoption on healthcaretransactionperformance:thecaseofhipaa.IntJProdEcon 2013;141(1):277–85.
[32]Cécile M.Ledossiermédicalpersonnel(dmp):autopsied’unprojet am-bitieux?MédDroit2009:24–41.
[33]Kamsu-Foguem B. Systemic modeling in telemedicine. Europ Res Telemed(RechEuropTéléméd)June2014;3(2):57–65.
[34]Kamsu-Foguem B. An ontological view in telemedicine. Europ Res Telemed(RechEuropTéléméd)June2014;3(2):67–76.
[35]Kamsu-Foguem B,Foguem C.Could telemedicineenhancetraditional medicinepractices?EuropResTelemed(RechEuropTéléméd) Septem-ber2014;3(3):117–23.
[36]Kamsu-Foguem B,Tchuenté-Foguem G,Foguem C.Usingconceptual graphsforclinicalguidelinesrepresentationandknowledgevisualization. InformSystFront2014;16(4):571–89.
[37]Kamsu-Foguem B,Diallo G,Foguem C.Conceptualgraph-based knowl-edge representation for supporting reasoning in African traditional medicine.EngApplArtifIntell2013;26(4):1348–65.
[38]Kamsu-Foguem B,Foguem C.AdversedrugreactionsinsomeAfrican herbalmedicine:literaturereviewandstakeholders’interview.IntegrMed ResSeptember2014;3(3):126–32.
[39]Tafin-Kampé K,Kamsu-Foguem B.Acuteosteomyelitisdueto Staphylo-coccusaureusinchildren:Whatisthestatusoftreatmenttoday?Pediatr InfectDis2013;5(3):122–6.
[40]Kamsu-Foguem B,Tchuenté-Foguem G,Allart L,Zennir Y,Vilhelm C, Mehdaoui H,etal.User-centeredvisualanalysisusingahybridreasoning hybridreasoningarchitectureforintensivecareunits.DecisSupportSyst 2012;54(1):496–509.
[41] Kamsu-Foguem B,Foguem C.Telemedicineandmobilehealthwith in-tegrativemedicineindevelopingcountries.HealthPolicyTechnol2014.
http://dx.doi.org/10.1016/j.hlpt.2014.08.008.
[42] Kamsu-Foguem B,Tchuenté-Foguem G,Foguem C.Conceptualgraph operationsforformalvisualreasoninginthemedicaldomain.IRBM2014.
http://dx.doi.org/10.1016/j.irbm.2014.04.001.
MamadouBiloDOUMBOUYA:HeisaPhDstudentatthe Uni-versityofToulouseandheisaffiliatedtotwounitsofresearchnamely theInstituteofPrivateLawofandtheProductionEngineering Lab-oratory (LGP) of National Engineering School of Tarbes (ENIT). Hereceived his Research Master Degreefrom the University Paul SabatierofToulouseandtheNationalSchoolofelectrical engineer-ing,electronics,computerscience,hydraulicsandtelecommunication ofToulouse(ENSEEIHT)in2011.Hisresearchactivitiesdealwith Telemedicinegenerallyandteleexpertiseparticularly.Hisworkis fo-cusedinArtificialintelligence,semanticmodellingforimprovingthe collaborationbetweenremotemedicalprofessionalswhiletakingin considerationtheethicside.
BernardKAMSUFOGUEM:HehasaPhDin Computer Sci-enceandEngineeringfromtheUniversityofMontpellier2in2004. Hegot the “accreditation to supervise research”, abbreviated HDR fromUniversityofToulousein 2013.Hehasobtainedthestatusof VisitingProfessoratinternationaluniversities:UnitedKingdom(e.g. OxfordBrookesUniversity,Oxford),Finland(e.g.AaltoUniversity, HelsinkiUniversityofTechnology,VTTTechnicalResearchCentre ofTampere,UniversityofOulu,ÅboakademiofTurkuUniversity). His current interests are in Knowledge Discovery and Data Min-ing,KnowledgeRepresentation,FormalVisualReasoning,
Ontology-basedSemanticAnalysis,KnowledgeExploitationforremote Collab-oration,DecisionSupportSystemsandIntelligentSystems. Applica-tiondomainsincludeindustrialContinuousImprovement processes, Telemedicine servicesand HealthInformation Systems.Heisa re-viewerforalargenumberofinternationalscientificjournalssuchas Computers in Biologyand Medicine, KnowledgeManagement Re-search&Practice,InteractingwithComputers,Sensors,Engineering ApplicationsofArtificialIntelligenceandKnowledge-BasedSystems. Heisamemberofthethematicgroup:e-HealthofInterOP-VLab (In-ternationalVirtualLaboratoryforEnterpriseInteroperability).
HuguesKENFACK:HeistheDeanofthefacultyLawandvice president foracademic affairsatToulouse’s University.He hasthe statusofVisitingProfessoratAmericanuniversities:SaintLouis Uni-versitySchoolofLaw–USA(2009,2011,2013,2014)andSanDiego UniversitySchoolof Law–USA(2013).ProfessorofLawin Uni-versityofToulousesince2004(PhDinLaw,UniversityofToulouse I (1996)),heis particularlyexpertin LawofObligationsand Con-tracts, BusinessLegalInstruments,PaymentandCreditInstruments and International Law(Trade, Financial, Distribution, Commercial, BankruptcyandForeignInvestment).Hehadotheradministrative po-sitionsatnationaluniversities:memberofthespecialist’scommissions attheUniversityofPoitiers,NantesandLaMartinique.Heismember ofjurypanel(BarExaminationandAdmissionofnotaries).Hehas ed-itorialcharges:editorial-in-ChiefoftheTransportationLawChronicle andCo-EditorinChiefoftheCommercialLeaseChronicle.
ClovisFOGUEM:HeisanInternalMedicineandGeriatric medi-caldoctorandhasundertakenaPhDon‘OlfactionandElderly:study oftheolfactory(CNI)andtrigeminal(CNV)sensitivitiesinteractions inageriatricpopulation;constantsandpathologicalspecificities’.He isalsoparticularlyinterestedinneurodegenerativediseases(as Parkin-sondiseaseorLewy Bodydementia),elderly epilepsyandwhether pathogenicinflammatoryorautoimmuneresponsescancontributeto thesedisordersintheelderly.Moreoverheisalsointerestedin medi-calknowledgerepresentationandmedicalclinicdesignguidelines.For hisworkon‘OlfactionandElderly’, DrC.Foguemwaslaureateof HealthResearchAwardforemerginghealthresearchersfromthe cor-poratefoundation‘GroupePasteurMutualité’in2011.Heisgrounded inmedicalresearchapplicationsofInformationandCommunications Technology.FormerFaculty ofMedicine’sClinicalInstructor,heis nowHospitalPractitionerinFrance.Heispeer-reviewerofmany sci-entistjournalsamongwhich:ClinicalInterventionsinAging; Degen-erativeNeurologicalandNeuromuscularDisease;International Med-icalCaseReportsJournal;NeuroscienceandNeuroeconomics; Clin-icalMedicineInsights;JournalofthePancreas;International Schol-arsJournals(ISJ); CancerTherapy; Indian JournalofCritical Care Medicineand,AfricanJournalofEnvironmental Scienceand Tech-nology.