0095-1137/97/$04.0010
Copyright © 1997, American Society for Microbiology
Development of a Method for Direct Quantification of
Cytomegalovirus Antigenemia by Flow Cytometry
BERTHE-MARIE IMBERT-MARCILLE,1* NELLY ROBILLARD,2ANNE-SOPHIE POIRIER,1 MARIANNE COSTE-BUREL,1DIEGO CANTAROVICH,3NOEL MILPIED,4
ANDSYLVIANE BILLAUDEL1
Virology Laboratory1and Flow Cytometry Department,2Institute of Biology of Nantes University Hospital,
Institute for Transplantation and Research in Transplantation,3and Clinical Haematology
Department,4Nantes University Hospital, 44035 Nantes Cedex 01, France
Received 20 March 1997/Returned for modification 16 June 1997/Accepted 10 July 1997
Cytomegalovirus (CMV) antigenemia was directly detected in polymorphonuclear leukocytes (PMNLs) from transplant recipients by using flow cytometry (FC). Two fixation and permeabilization methods and seven anti-CMV monoclonal antibodies (MAbs) were evaluated. 1C3, SL20, and NEA-9221 MAbs were more effica-cious. The antigenemia detection threshold of FC was 0.05% positive PMNLs, and percentages correlated well with DNA viral load and the appearance of clinical symptoms.
Cytomegalovirus (CMV) infection is a frequent complica-tion following transplantacomplica-tion and is one of the commonest opportunistic infections in AIDS patients. Among the different techniques used to confirm active infection, determination of pp65 antigenemia has the advantage of directly quantifying the viral load, which generally correlates well with CMV disease (5, 6, 14, 21, 22). However, the detection of positive cells is subjective and demands very careful and time-consuming mi-croscopic observation (5). One approach to overcome these major hurdles might be to automate immunofluorescence de-tection. Conclusive trials have been carried out with image cytometry (12, 16), requiring highly specialized equipment and still taking considerable time. Another approach is flow cytom-etry (FC), which was successfully adapted to CMV antigen detection in some reported studies (15), although most of these have been carried out on cells infected in vitro or on cells isolated from bronchoalveolar lavage samples (2).
We present here the results of a method for the direct quantification of CMV antigenemia in polymorphonuclear leu-kocytes (PMNLs) by FC (antigenemia FC), which were com-pared with those of techniques for determining viremia and qualitative and quantitative DNAemia.
Sixty EDTA blood samples, obtained from 25 renal and 8 bone marrow transplant CMV-seropositive recipients, were evaluated by antigenemia FC. All specimens were processed within 4 h after collection. Leukocytes (53105) obtained after erythrocyte lysis or MRC-5 fibroblasts were fixed and perme-abilized by two technical procedures run in parallel. In the paraformaldehyde-Tween method (19), the cell pellet was re-suspended in 1% paraformaldehyde (Mercks, Nogent sur Marne, France) with 0.2% Tween 20 (Sigma, Saint-Quentin en Yvelines, France) and incubated overnight at 4°C. In the para-formaldehyde-methanol method (18), the cell pellet was se-quentially incubated with 1% paraformaldehyde for 15 min at 4°C, washed once in phosphate-buffered saline, resuspended in cold 80% methanol, and kept at220°C overnight.
Fixed and permeabilized cells were washed and incubated
for 45 min at 37°C with a saturating amount (0.5 to 1mg) of each anti-CMV monoclonal antibody (MAb); immunoglobulin G1 (IgG1), IgG2a, and IgG3 isotype controls (Caltag/Tebu, Marnes la Coquette, France); or anti-CD15 MAb (Immuno-tech, Marseille, France). Seven commercially available anti-CMV MAbs were used. NEA-9221 (DuPont de Nemours/ NEN Products, Les Ulis, France), of the IgG2a subclass, and E13 (Arge`ne-Biosoft, Varihles, France), of the IgG1 subclass, recognize immediate-early antigens of 72 kDa; 2A2 (Arge `ne-Biosoft), of the IgG1 subclass, recognizes early antigen; 1C3 (Arge`ne-Biosoft) and the two pooled MAbs, C10 and C11, in Clonab CMV (Biotest, Dreieich, Germany), both from the IgG1 subclass, recognize the lower matrix phosphoprotein pp65; and finally, SL20 (Arge`ne-Biosoft), of the IgG3 subclass, and NEA-9220 (DuPont de Nemours), of the IgG1 subclass, are directed against other late antigens, which have not yet been clearly identified. Cells were then washed and incubated for 30 min at 4°C with fluorescein isothiocyanate (FITC)-F(ab9)2goat anti-mouse IgG (Bioatlantique, Nantes, France). All incubation and wash steps were done in phosphate-buff-ered saline supplemented with 20% human AB serum in order to obtain Fc receptor saturation and thus limit nonspecific binding.
Several controls were run in parallel (9): PMNLs from pa-tients without active infections and mock-infected MRC-5 fi-broblast monolayers served as negative controls, and MRC-5 fibroblast monolayers cultured for 4 days with the AD169 ref-erence strain (at a multiplicity of infection between 0.01 and 0.1) served as positive controls.
Samples were analyzed on a FACSCalibur flow cytometer (Becton Dickinson, Mountain View, Calif.). At least 50,000 PMNLs or 10,000 MRC-5 fibroblasts were gated by light scat-ter (PMNL gates were assessed for accuracy when appropriate by using CD15 staining) and collected in a list mode manner. Data analysis was performed with Cell Quest software (Becton Dickinson). The percentages of positive cells and the mean fluorescence intensities were determined on forward side scat-ter versus FITC fluorescence dot plots (for PMNLs) or FITC fluorescence histograms (for MRC-5 fibroblasts), using a re-gion defined according to isotype control analysis.
For all patients, viremia (by the shell vial assay [7]) and qualitative DNAemia in leukocytes were also determined in parallel, as previously described (10). In some of these pa-* Corresponding author. Mailing address: Laboratoire de Virologie,
Institut de Biologie du Centre Hospitalier Universitaire de Nantes, 9 Quai Moncousu, 44035 Nantes Cedex 01, France. Phone: (33) 02-40-08-41-01. Fax: (33) 02-40-08-41-14. E-mail: [email protected] .fr.
2665
on May 15, 2020 by guest
http://jcm.asm.org/
tients, the DNA viral load in leukocytes was also quantified (11), using the commercially available CMV hybrid capture system (Murex, Chatillon, France) according to the manufac-turer’s recommendations.
No nonspecific labeling, with the exception of MAb NEA 9220, was noted when mock-infected MRC-5 fibroblasts were incubated with anti-CMV MAbs (data not shown) or when
[image:2.612.147.470.69.394.2]isotype controls were run on AD169-infected MRC-5 fibro-blasts (Fig. 1). Six of the seven MAbs recognized CMV anti-gens on infected MRC-5 fibroblasts (Fig. 1), and the percent-ages of positive cells were higher with MAbs detecting immediate-early antigens. Both methods of fixation and per-meabilization yielded similar results (data not shown). Our results agreed with those previously reported for E13 and
FIG. 1. Fluorescence histograms of CMV-infected MRC-5 fibroblasts stained with different anti-CMV MAbs ( ) overlaid with related isotype control histograms (——, for IgG1;z z z z z, for IgG2a; and - - - - -, for IgG3). Pos cell, percentage of antigen-positive cells; fluo mean, mean fluorescence intensity; FL1-H, FITC fluorescence intensity. The bars represent the proportion of positive cells.
TABLE 1. Percentage of antigen-positive PMNLs after incubation with various anti-CMV MAbs as determined by FC analysis
Anti-CMV MAb
Percentage interval (median) of antigen-positive PMNLs for:
Patients without active CMV infectionsa(40 specimens) Patients with active CMV infectionsb(20 specimens)
Paraformaldehyde-Tween Paraformaldehyde-MetOHc Paraformaldehyde-Tween Paraformaldehyde-MetOH
IgG1 isotype control ,0.05 ,0.05 ,0.05 ,0.05
IgG2a isotype control ,0.05 ,0.05 ,0.05 ,0.05
IgG3 isotype control ,0.05 ,0.05 ,0.05 ,0.05
NEA-9221 0.01–0.09 (0.04) 0.02–0.10 (0.05) 0.07–0.65 (0.24) 0.06–0.85 (0.32)
1C3 ,0.05 ,0.05 0.14–1.15 (0.50) 0.19–1.50 (0.75)
SL20 ,0.05 ,0.05 0.05–0.66 (0.15) 0.05–0.88 (0.30)
C10/C11 0.01–0.08 (0.01) 0.01–0.07 (0.01) 0.04–0.20 (0.06) 0.06–0.21 (0.07)
2A2 ,0.05 ,0.05 ,0.05 ,0.05
NEA-9220 0.01–0.09 0.02–0.11 0.01–0.10 (0.02) 0.01–0.12 (0.02)
E13 ,0.05 ,0.05 0.01–0.07 (0.01) 0.01–0.07 (0.01)
aAs assessed from negative viremia and negative DNAemia. bAs assessed from positive viremia and/or positive DNAemia. cMetOH, methanol.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:2.612.59.557.561.702.2]NEA-9221, with the exception of NEA-9220, which exhibited nonspecific staining (20).
Optimizing cytometry protocols is a very important step in allowing detection of viral antigens present at low frequencies, i.e., 102 to 106(12), and located intracellularly in leukocytes. Both selected techniques for PMNL preparation used reagents
which provide good stabilization of permeabilized membranes and increase the indirect fluorescence of intranuclear antigen (17, 18). To allow accurate and reproducible quantification of positive cells present at a concentration of 0.05%, at least 50,000 events have to be analyzed (1, 8).
The results obtained in 20 samples from 10 renal transplant recipients with active infections confirmed by laboratory tests (i.e., positive DNAemia associated or not with positive vire-mia) (Table 1) demonstrate the superiority of MAbs NEA-9221, 1C3, and SL20 and also the greater effectiveness of the paraformaldehyde-methanol method. With the other MAbs, no labeling was obtained, with the exception of the pooled C10-C11, which was only found to be positive in 10 of 20 specimens. No nonspecific labeling occurred on PMNLs from infected patients (Table 1 and Fig. 2) with isotype controls. The mean fluorescence intensity of these three antibodies on infected PMNLs showed a bimodal expression in the case of MAb SL20, a raised unimodal expression in the case of NEA 9221, and a low unimodal expression in the case of 1C3 (Fig. 2). The reproducibility of our method (Table 2) was evaluated in two separate experiments (each in triplicate), using samples from three infected patients. The standard deviation was con-sistently below 0.05%, whichever leukocyte preparation method was used. Increasing the number of PMNLs analyzed to 150,000 events yielded the same percentages of positive cells as 50,000 events did (data not shown). For PMNLs from pa-tients without active infections (40 specimens), the percentage of positive cells, labeled with 1C3 or SL20 MAb, was below 0.03%, corresponding to the background fluorescence ob-tained with isotype controls (Table 1). For MAb NEA-9221, a weak labeling (Table 1) was sometimes observed, which was not related to the subclass, IgG2a, of this antibody (Fig. 2).
[image:3.612.60.299.69.451.2]The most useful antibody is therefore MAb 1C3, confirming the advantage of detecting late antigens (3, 5). MAb 1C3 is also used in slide detection of antigenemia, as is the C10-C11 pool (4, 6, 13, 14, 16). The weak labeling obtained with this pool on PMNLs is quite surprising; both these MAbs are directed against pp65, have the same isotype, and reacted similarly with infected fibroblasts (Fig. 1). Differences between 1C3 and C10-C11 could therefore be explained by recognition of distinct epitopes on pp65 and/or a better penetration of 1C3 into the permeabilized PMNLs. The levels of antigen expression in PMNLs from patients with active infections (maximum pro-portion of cells expressing CMV antigen51.5%) correspond to levels reported for the slide method (5, 6, 21). Much higher percentages of peripheral blood lymphocytes expressing CMV antigens had been reported previously, but these data concern peripheral blood mononuclear cells (15). For our method, the threshold of positivity was established at 0.05% for the MAbs 1C3 and SL20 and at 0.10% for MAb NEA-9221, according to
FIG. 2. Biparametric analysis of three anti-CMV MAbs and related isotype control staining on PMNLs from patients with active infections by forward angle light scatter (FSC-H) versus FITC fluorescence intensity (FL1-H). The windows identify CMV-positive (pos) PMNLs. fluo mean, mean fluorescence intensity.
TABLE 2. Reproducibility of results of antigenemia FC
Patient Fixation-permeabilization
method
Mean percentage (6SD) of positive PMNLs
MAb 1C3 IgG SL20 MAb NEA-9221
A Paraformaldehyde-Tween 0.3260.05 0.1560.02 0.2060.05
Paraformaldehyde-MetOHa 0.4360.05 0.3260.04 0.3560.01
B Paraformaldehyde-Tween 0.6160.05 0.2160.01 0.1660.05
Paraformaldehyde-MetOH 0.8360.04 0.3060.01 0.5660.04
C Paraformaldehyde-Tween 0.2560.03 0.1960.02 0.0960.05
Paraformaldehyde-MetOH 0.4260.04 0.3060.05 0.2360.04
aMetOH, methanol.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:3.612.59.558.610.718.2]reproducibility test results (Table 2) and data from patients without active infections (Table 1). The sensitivity of antigen-emia FC is therefore lower than that which can theoretically be obtained by using the slide method. Most authors have shown that low levels of antigens very rarely indicate progressive disease (5, 6, 13), especially in solid-organ transplant recipients when counts of positive cells do not exceed 50 per 100,000 PMNLs, a level which corresponds to our detection threshold (i.e., 0.05%).
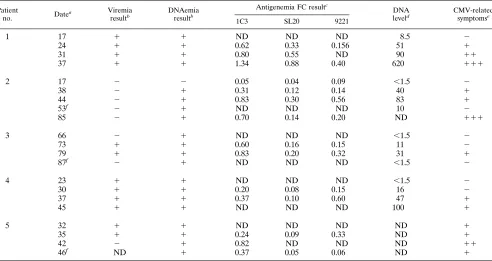
Antigenemia FC was evaluated in a clinical situation for 14 of 20 positive specimens, taken from 5 renal transplant recip-ients for whom a prospective follow-up for CMV infection had been carried out (Table 3). Progressive intensification of anti-genemia was observed with all three MAbs selected, and in patient 5 a distinct diminution was seen after ganciclovir initi-ation. There was generally good agreement between the de-gree of DNA load and the level of antigenemia detected by FC, as assessed with MAbs 1C3 and SL20, except for patient 3. With these two MAbs, the highest percentages were seen with patient 1, who had severe CMV disease (pneumonitis). With MAb NEA-9221, antigenemia detected by FC correlates less well with the DNA load, suggesting that viral antigen expres-sion may vary according to the stage of infection or of the disease. Studies on a larger scale will perhaps allow this point to be clarified. The sensitivity of detection by FC analysis proved adequate in all patients, including patient 2, for whom viremia detection was consistently negative (in spite of the fact that samples were cultured in six wells).
Quantification of antigenemia, especially when 1C3 MAb is used, can therefore be adapted to direct detection by FC. Since it is less sensitive than the slide method, our method is
prob-ably not suitable for very early detection of active infection, but it would seem promising for the quantification of the viral load in patients already screened by a method such as PCR. Studies on a larger scale are in progress, which will allow more detailed assessment of the clinical utility of antigenemia FC.
This work was supported by a clinical research grant from the Nantes University Hospital (De´le´gation a` la Recherche Clinique).
REFERENCES
1.Bender, J., K. Unverzagt, D. Walker, W. Lee, D. Van Epps, D. Smith, C. Stewart, and L. Bik To.1991. Identification and comparison of CD34-posi-tive cells and their subpopulations from normal peripheral blood and bone marrow using multicolor flow cytometry. Blood77:2591–2596.
2.Elmendorf, S., J. McSharry, J. Laffin, D. Fogleman, and J. Lehman.1988. Detection of an early cytomegalovirus antigen with two-color quantitative flow cytometry. Cytometry9:254–260.
3.Gerna, G., M. Revello, E. Percivalle, M. Zavattoni, M. Parea, and M. Bat-taglia. 1990. Quantification of human cytomegalovirus viremia by using monoclonal antibodies to different viral proteins. J. Clin. Microbiol.28:2681– 2688.
4.Gerna, G., D. Zipeto, M. Parea, M. G. Revello, E. Silini, E. Percivalle, M. Zavattoni, P. Grossi, and G. Milanesi.1991. Monitoring of human cytomeg-alovirus infections and ganciclovir treatment in heart transplant recipients by determination of viremia, antigenemia and DNAemia. J. Infect. Dis.164: 488–498.
5.Gerna, G., M. G. Revello, E. Percivalle, and F. Morini.1992. Comparison of different immunostaining techniques and monoclonal antibodies to the lower matrix phosphoprotein (pp65) for optimal quantitation of human cytomeg-alovirus antigenemia. J. Clin. Microbiol.30:1232–1237.
6.Ghisetti, V., A. Barbui, E. Donegani, M. Bobbio, P. Caimmi, S. Pansini, G. Zattera, A. Pucci, M. di Summa, and G. Marchiaro.1996. Comparison of polymerase chain reaction and pp65 antigen test for early detection of human cytomegalovirus in blood leukocytes of cardiac transplant recipients. Clin. Microbiol. Infect.1:195–202.
7.Griffiths, P. D., P. R. Stirck, M. Ganczakowski, D. D. Panjwani, M. G. Ball, H. A. Blacklock, and H. G. Prentice.1984. Rapid diagnosis of
cytomegalo-TABLE 3. Sequential laboratory results for patients with CMV disease
Patient
no. Datea
Viremia resultb
DNAemia resultb
Antigenemia FC resultc
DNA leveld
CMV-related symptomse
1C3 SL20 9221
1 17 1 1 ND ND ND 8.5 2
24 1 1 0.62 0.33 0.156 51 1
31 1 1 0.80 0.55 ND 90 11
37 1 1 1.34 0.88 0.40 620 111
2 17 2 2 0.05 0.04 0.09 ,1.5 2
38 2 1 0.31 0.12 0.14 40 1
44 2 1 0.83 0.30 0.56 83 1
53f 2 1
ND ND ND 10 2
85 2 1 0.70 0.14 0.20 ND 111
3 66 2 1 ND ND ND ,1.5 2
73 1 1 0.60 0.16 0.15 11 2
79 1 1 0.83 0.20 0.32 31 1
87f 2 1
ND ND ND ,1.5 2
4 23 1 1 ND ND ND ,1.5 2
30 1 1 0.20 0.08 0.15 16 2
37 1 1 0.37 0.10 0.60 47 1
45 1 1 ND ND ND 100 1
5 32 1 1 ND ND ND ND 1
35 1 1 0.24 0.09 0.33 ND 1
42 2 1 0.82 ND ND ND 11
46f
ND 1 0.37 0.05 0.06 ND 1
aDays after renal transplantation. b1, positive;2, negative; ND, not done.
cExpressed as the percentage of positive PMNLs (prepared with paraformaldehyde-methanol) after deducting related isotype control data. ND, not done. dExpressed in picograms per 106leukocytes. ND, not done.
e2, none;1, mild;11, moderate;111, severe. fPatient treated with ganciclovir during period of follow-up.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:4.612.62.554.82.343.2]virus in immunocompromised patients by detection of early antigen foci. Lancetii:1242–1244.
8.Gross, H.-J., B. Verwer, D. Houck, and D. Recktenwald.1993. Detection of rare cells at a frequency of one per million by flow cytometry. Cytometry 14:519–526.
9.Horan, P., K. Muirhead, and S. Slezak.1990. Standards and control in flow cytometry, p. 397–414.InM. Melamed, T. Lindmo, and M. Mendelsohn (ed.), Flow cytometry and sorting, 2nd ed. Wiley-Liss, New York, N.Y. 10. Imbert-Marcille, B.-M., N. Milpied, M. Coste-Burel, B. Richet, P. Moreau,
J.-L. Harousseau, and S. Billaudel.1995. Clinical and practical value of human cytomegalovirus DNAemia detection by semi-nested PCR, for BMT recipients’ follow-up. Bone Marrow Transplant.15:611–617.
11. Imbert-Marcille, B.-M., D. Cantarovich, V. Ferre´-Aubineau, B. Richet, J.-P. Soulillou, and S. Billaudel.1997. Usefulness of DNA viral load quantifica-tion for CMV disease monitoring in renal and pancreas/renal transplant recipients. Transplantation63:1476–1481.
12. Jiwa, N., W. Mesker, J. Ploem-Zaaijer, W. van Dorp, T. The, and A. Raap. 1994. Quantification of low frequency white blood cells expressing human cytomegalovirus antigen by image cytometry. Cytometry16:69–73. 13. Landry, M. L., and D. Ferguson.1993. Comparison of quantitative
cytomeg-alovirus antigenemia assay with culture methods and correlation with clinical disease. J. Clin. Microbiol.31:2851–2856.
14. Mazzulli, T., R. H. Rubin, M. J. Ferraro, R. T. D’Aquila, S. A. Doveikis, B. R. Smith, T. H. The, and M. S. Hirsch.1993. Cytomegalovirus antigenemia: clinical correlations in transplant recipients and persons with AIDS. J. Clin. Microbiol.31:2824–2827.
15. McSharry, J. J.1994. Uses of flow cytometry in virology. Clin. Microbiol. Rev.7:576–604.
16. Ploem-Zaaijer, J. J., W. E. Mesker, G. J. Boland, W. C. Sloos, F. M. Van de Rijke, N. M. Jiwa, and A. K. Raap.1994. Automated image cytometry for detection of rare viral antigen-positive cells in peripheral blood. Cytometry 15:199–206.
17. Pollice, A., J. McCoy, S. Shackney, C. Smith, J. Agarwal, D. Burholt, L. Janocko, F. Hornicek, S. Singh, and R. Hartsock.1992. Sequential parafor-maldehyde and methanol fixation for simultaneous flow cytometric analysis of DNA, cell surface proteins, and intracellular proteins. Cytometry13:432– 444.
18. Schimenti, K., and J. Jaccobberger.1992. Fixation of mammalian cells for flow cytometric evaluation of DNA content and nuclear immunofluores-cence. Cytometry13:48–59.
19. Schmid, I., H. Uittenbogaart, and J. Giorgi.1991. A gentle fixation and permeabilization method for combined cell surface and intracellular staining with improved precision in DNA quantification. Cytometry12:279–285. 20. Schols, D., R. Snoeck, J. Neyts, and E. De Clercq.1989. Detection of
immediate early, early and late antigens of human cytomegalovirus by flow cytometry. J. Virol. Methods26:247–254.
21. The, T. H., M. van der Ploeg, A. P. van den Berg, A. M. Vliegler, M. van der Giessen, and W. J. van Son.1992. Direct detection of cytomegalovirus in peripheral blood leukocytes—a review of the antigenemia assay and poly-merase chain reaction. Transplantation54:193.
22. Van den Berg, A. P., I. J. Klompmaker, E. B. Haagsma, A. Scholten-Samp-son, C. M. A. Bijleveld, J. Schirm, M. Van der Gissen, M. J. H. Slooff, and T. H. The.1991. Antigenemia in the diagnosis and monitoring of active cytomegalovirus infection after liver transplantation. J. Infect. Dis.164:265– 270.