Original Article
Association between
IL-6
-174G/C and -572G/C
polymorphisms and risk of coronary artery
disease in a Chinese population
Yulan Gao1,2, Wei Jiang2, Quanneng Yan1, Zhiliang Li1
1Department of Cardiology, Zhujiang Hospital, Southern Medical University, Guangzhou 510280, China; 2
Depart-ment of Ultrasonography, Nanshan Affiliated Hospital of Guangdong Medical College, Shenzhen 518052, China
Received October 14, 2015; Accepted November 28, 2015; Epub January 1, 2016; Published January 15, 2016
Abstract: We have conducted a case-control study in a Chinese population, and investigate the role of two common promoter genomic variants in IL-6 (-174G/C and -572G/C) in the development of CAD in a Chinese population. A hospital-based cacontrol study was taken. A total of 275 patients with CAD and 286 control subjects were se-lected between January 2012 and December 2014. The genotyping of IL-6 -174G/C and -572G/C were performed by polymerase chain reaction (PCR) coupled with restriction fragment length polymorphism (RFLP). Using chi-square test, a significant difference was found in IL-6 -174G/C genotype distributions between patients with CAD and con-trol subjects (χ2=16.80, P<0.001). Using unconditional logistic regression analysis, we found that theCC genotype of IL-6 -174G/C was associated with an increased risk of CAD when compared with the GG genotype (OR=3.43, 95% CI=1.79-6.86; P<0.001). Moreover, the IL-6 -174G/C polymorphism was correlated with development of CAD in dominant (OR=1.82, 95% CI=1.23-2.70; P=0.002) and recessive models (OR=3.26, 95% CI=1.71-6.48; P<0.001). However, we found that IL-6 -572G/C polymorphism was not associated with an elevated increased risk of CAD in codominant, dominant and recessive models. In conclusion, we suggest that IL-6 -174G/C is associated with the development of CAD in codominant, dominant, and recessive models. Further studies with large sample size are greatly needed to confirm the findings of our study.
Keywords: IL-6, polymorphism, coronary artery disease
Introduction
Coronary heart disease is also called coronary artery disease (CAD), and this disease is the most common and malignant cardiovascular disease worldwide, including China [1, 2]. CAD is associated with high mortality and morbidity worldwide [2]. CAD is be distinguished by occlu-sive epicardial coronary artery stenosis, and this disease consequences such as myocardial infarction [3]. CAD is caused by a complex and multifactor process, hypertension, hypercho-lesterolemia, diabetes, obesity, tobacco smok-ing, alcohol drinksmok-ing, total cholesterol and LDL cholesterol [4]. However, not all individuals who expose to the same risk factors of CAD would develop CAD, which suggested that the inher-ent factors may contribute to the underlying pathogenesis of CAD [5].
The process of CAD can contribute to inflamma-tory mechanism, and cytokines are the main
Inflammation plays a critical role in the inflam-matory response, immune regulation and devel-opment of CAD through the promotion of ath-erosclerosis [6]. Interleukin 6 (IL-6) is an important member of pro-inflammatory cytoine, and it plays an important role in up-regulating the synthesis of the acute-phase proteins [7, 8]. Previous study has reported that expression of
IL-6 could predict the risk of cardiovascular dis-ease [8]. We have conducted a case-control study in a Chinese population, and investigate the role of two common promoter genomic vari-ants in IL-6 (-174G/C and -572G/C) in the devel-opment of CAD in a Chinese population. Material and methods
Patients
nosed by coronary angiography, and the CAD was defined as ≥70% stenosis of one major coronary artery, or ≥50% stenosis of the left main coronary artery. The exclusion criteria were patients who received myocardial spasms or a myocardial bridge, and suffered from auto-immune disease, congenital heart disease, childhood hypertension, type 1 diabetes melli-tus, severe kidney and liver disease as well as malignancy.
286 controls were randomly selected from indi-viduals who came to receive a health check-up in the physical examination center of our hospi-tal. The controls were confirmed to be free of arterosclerotic lesions confirmed by angiogra-phy, and free of a history of CAD.
[image:2.629.96.533.94.171.2]The social-demographic and clinical character-istics of patients with CAD and controls were collected by a structured questionnaire or med-ical records. The clinmed-ical information from medi-cal records included hypertension, diabetes mellitus, total cholesterol (TC), low-density lipo-protein cholesterol (LDL-c) and high-density lipoprotein cholesterol (HDL-c) as well as triglyc-eride (TG). The demographic information from a self-designed questionnaires included sex, age, tobacco smoking, alcohol drinking, diabe-tes and hypertension. The study was carried out with the permission of the Institutional Review Board of our hospital. Written informed consents were obtained from all participants. Ethical approval for this study conformed to the standards of the Declaration of Helsinki.
Table 1. Primers and restriction enzymes for IL-6 -174G/C and -572G/C polymorphisms
Gene polymorphism SNP Primers Length of digested fragment Restriction enzyme
IL-6 -174G/C rs1800795 5’-GGAGTCACACACTCCACCT-3’ 229 bp hsp92II
5’-CTGATTGGAAACCTTATTAAG-3’
IL-6 -572G/C rs1800796 5’-GAGACGCCTTGAAGTAACTG-3’ 163 bp MbiI
5’-GAGTTTCCTCTGACTCCATCGCA-3’
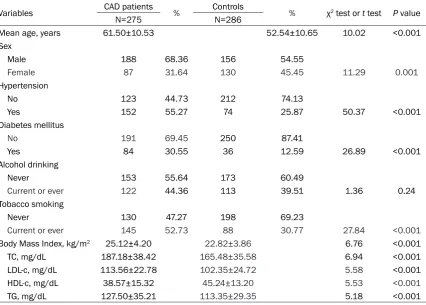
Table 2.Demographic and clinical characteristics of included cases and control subjects
Variables CAD patients % Controls % χ2 test or t test P value
N=275 N=286
Mean age, years 61.50±10.53 52.54±10.65 10.02 <0.001
Sex
Male 188 68.36 156 54.55
Female 87 31.64 130 45.45 11.29 0.001
Hypertension
No 123 44.73 212 74.13
Yes 152 55.27 74 25.87 50.37 <0.001
Diabetes mellitus
No 191 69.45 250 87.41
Yes 84 30.55 36 12.59 26.89 <0.001
Alcohol drinking
Never 153 55.64 173 60.49
Current or ever 122 44.36 113 39.51 1.36 0.24
Tobacco smoking
Never 130 47.27 198 69.23
Current or ever 145 52.73 88 30.77 27.84 <0.001
Body Mass Index, kg/m2 25.12±4.20 22.82±3.86 6.76 <0.001
TC, mg/dL 187.18±38.42 165.48±35.58 6.94 <0.001
LDL-c, mg/dL 113.56±22.78 102.35±24.72 5.58 <0.001
HDL-c, mg/dL 38.57±15.32 45.24±13.20 5.53 <0.001
[image:2.629.103.530.206.511.2]Genetic analysis
All subjects were asked to provide 5 mL periph-eral venous blood samples before receiving cisplatin-based chemotherapy. DNA was extracted from peripheral blood samples which collected from patients and controls using the TIANamp Blood DNA Kit (Tiangen, Beijing, China) according to instructions. The genotyp-ing of IL-6 -174G/C and -572G/C were per-formed by polymerase chain reaction (PCR) coupled with restriction fragment length poly-morphism (RFLP). The PCR fragments of the investigated polymorphisms were subsequent-ly digested with their specific restriction enzyme (Table 1). The PCR reaction conditions were began with an initial denaturation at 95°C for 5 min, followed by 30 cycles of denaturation at 94°C for 60 s, annealing at 60°C for 60 s, and extension at 72°C for 60 s, and a final exten-sion at 72°C for 10 min. Digestion products were separated by electrophoresis on ethidium bromide stained agarose gel and visualized under UV light.
Statistical analysis
Continuous variables and categorical variables were expressed as the mean ± standard devia-tion (SD) and frequencies (n) and percentages (%), respectively. Whether IL-6 -174G/C and -572G/C gene polymorphisms confirmed with Hardy-Weinberg equilibrium (HWE) was ana-lyzed by Fisher’s exact test. A multivariate logis-tic model was performed to analyze the asso-ciation between IL-6 -174G/C and -572G/C polymorphisms and risk of CAD, and the results were expressed by odds ratios (OR) and its
cor-responding 95% confidence intervals (CIs). The homozygote of the most frequent genotype was taken as the reference group of all genes. All statistical analyses were performed using SPSS 16.0 software (SPSS, Chicago, IL, USA). A
P value less than 0.05 was considered as sta-tistically significant.
Results
The demographic and clinical information of included patients with CAD and control sub-jects were shown in Table 2. The mean age of CAD patients and controls were 61.50±10.53 and 52.54±10.65 years, respectively. There were 188 (68.36%) males and 87 (31.64%) females in CAD patients, and 156 (54.55%) males and 130 (45.45%) females in controls. Compared with control subjects, some risk fac-tors were observed significantly more prevalent in CAD patients, such as age (χ2=10.02,
P<0.001), sex (χ2=11.29, P=0.001), hyperten-sion (χ2=50.37, P<0.001), diabetes mellitus (χ2=26.89, P<0.001), tobacco smoking (χ2= 27.84, P<0.001), body mass indexes (t=6.76,
P<0.001), TC (t=8.94, P<0.001), LDL-c (t=5.58,
P<0.001), HDL-c (t=5.53, P<0.001) and TG (t=5.18, P<0.001).
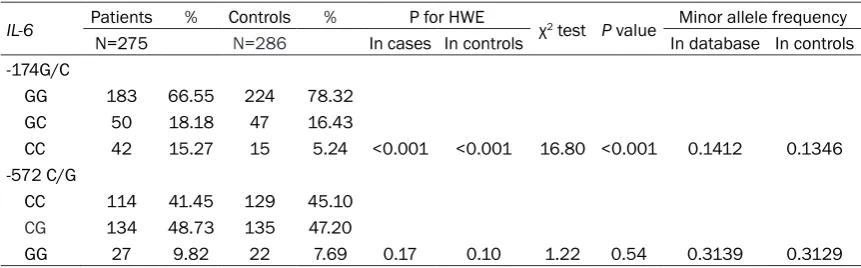
The genotype distributions of IL-6 -174G/C and -572G/C genes were shown in Table 3. The fre-quencies of GG, GC and CC genotypes in IL-6
-174G/C were 183 (66.55%), 50 (18.18%) and 42 (15.27%) cases in CAD patients, respective-ly; and were 224 (78.32%), 47 (16.43%) and 15 (5.24%) cases in the controls, respectively. The frequencies of CC, CG and GG genotypes in IL-6
[image:3.629.98.529.104.238.2]-572G/C were 114 (41.45%), 134 (48.73%) and
Table 3. Genotype distributions of IL-6 -174G/C and -572G/C gene polymorphisms between patients with CAD and control subjects
IL-6 Patients % Controls % P for HWE χ2 test P value Minor allele frequency
N=275 N=286 In cases In controls In database In controls
-174G/C
GG 183 66.55 224 78.32
GC 50 18.18 47 16.43
CC 42 15.27 15 5.24 <0.001 <0.001 16.80 <0.001 0.1412 0.1346
-572 C/G
CC 114 41.45 129 45.10
CG 134 48.73 135 47.20
GG 27 9.82 22 7.69 0.17 0.10 1.22 0.54 0.3139 0.3129
27 (9.82%) cases in CAD patients, respectively; and were 129 (45.10%), 135 (47.20%) and 22 (7.69%) cases in controls, respectively. By chi-square test, a significant difference was found in IL-6 -174G/C genotype distributions between patients with CAD and control subjects (χ2=16.80, P<0.001). The genotype distribu-tions of IL-6 -174G/C in CAD patients and con-trols were deviated from HWE (Both P values for HWE <0.001), while IL-6 -572G/C were not (P value for CAD cases =0.17; P value for con-trols =0.10). The minor allele frequencies of
IL-6 -174G/C and -572G/C in controls were in line with those in NCBI databases.
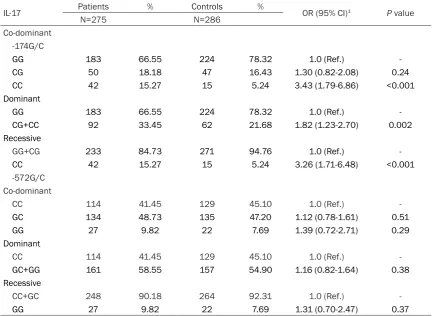
The association between IL-6 -174G/C and -572G/C gene polymorphisms and CAD risk were described in Table 4. Using unconditional logistic regression analysis, we found that the CC genotype of IL-6 -174G/C was associated with an increased risk of CAD when compared with the GG genotype (OR=3.43, 95% CI=1.79-6.86; P<0.001). Moreover, the IL-6 -174G/C polymorphism was correlated with
develop-ment of CAD in dominant (OR=1.82, 95% CI=1.23-2.70; P=0.002) and recessive models (OR=3.26, 95% CI=1.71-6.48; P<0.001). However, we found that IL-6 -572G/C polymor-phism were not associated with an elevated increased risk of CAD in codominant, dominant and recessive models.
Discussion
It is well known that polymorphisms have an important role in the regulation of gene expres-sion, and thus gene polymorphisms contribute to the differences between individuals in the susceptibility to a disease and its severity. Cytokines are modulators for immune respons-es, and the balance between proinflammatory and anti-inflammatory stimuli plays an impor-tant role in the susceptibility to atherosclerosis. Previous study have reported that the locally higher secretion and concentrations of proin-flammatory cytokines are associated with severely damages in the epithelium of blood vessels and surrounding tissues, and thus
cyto-Table 4. Association between IL-6 -174G/C and -572G/C gene polymorphisms and CAD risk
IL-17 Patients % Controls % OR (95% CI)1 P value
N=275 N=286
Co-dominant -174G/C
GG 183 66.55 224 78.32 1.0 (Ref.)
CG 50 18.18 47 16.43 1.30 (0.82-2.08) 0.24
CC 42 15.27 15 5.24 3.43 (1.79-6.86) <0.001
Dominant
GG 183 66.55 224 78.32 1.0 (Ref.)
CG+CC 92 33.45 62 21.68 1.82 (1.23-2.70) 0.002
Recessive
GG+CG 233 84.73 271 94.76 1.0 (Ref.)
CC 42 15.27 15 5.24 3.26 (1.71-6.48) <0.001
-572G/C Co-dominant
CC 114 41.45 129 45.10 1.0 (Ref.)
GC 134 48.73 135 47.20 1.12 (0.78-1.61) 0.51
GG 27 9.82 22 7.69 1.39 (0.72-2.71) 0.29
Dominant
CC 114 41.45 129 45.10 1.0 (Ref.)
GC+GG 161 58.55 157 54.90 1.16 (0.82-1.64) 0.38
Recessive
CC+GC 248 90.18 264 92.31 1.0 (Ref.)
GG 27 9.82 22 7.69 1.31 (0.70-2.47) 0.37
[image:4.629.98.531.94.410.2]kines could contribute to the development of cardiovascular disease [9, 10]. Previous stud-ies have reported that genetic polymorphisms in functional cytokines are correlated with the susceptibility to CAD [11-15]. In our study, we found that theCC genotype of IL-6 -174G/C was associated with an increased risk of CAD, and the IL-6 -174G/C polymorphism was correlated with development of CAD in dominant and recessive models.
Previous studies have investigate the associa-tion between IL-6 -174G/C and -572G/C gene polymorphisms and development of cardiovas-cular disease [16-22]. Gaudino et al. indicated that IL-6 -174G/C gene polymorphism could modulate the inflammatory response to surgery and influence the development of atrial arrhyth-mias after cardiac surgery [16]. Tso et al. con-ducted a meta-analysis with twelve relevant publications, and reported that conflicting results regarding the association between stroke and IL-6 -174G/C polymorphism [17]. Galimudi et al. reported that CC genotype of
IL-6 -174G/C gene was associated with devel-opment of coronary artery disease when com-pared with GG genotype [18]. Hou et al. con-ducted a meta-analysis with 42 studies including 15,145 cases and 21,496 controls, and they reported that C allele of IL-6 -174G/C was correlated with an increased risk of CAD in Caucasians, and the C allele of -572G/C poly-morphism may decrease the risk of CAD in Chinese [19]. Li et al. found that IL-6 -174G/C and -572G/C gene polymorphisms were associ-ated with development of CAD [20]. Song et al. found that the CC genotype of IL-6 -174G/C was related to the onset of cardiovascular events [21]. In our study, we found that the IL-6 -174G/ C polymorphisms were associated with an increased risk of CAD in co-dominant, domi-nant and recessive models. The discrepancy of results in previous studies may be caused by differences in populations, study design and sample size.
Two limitations should be considered in our study. First, patients with CAD and control sub-jects were selected from only one place, and thus selection bias may exist in this study. However, the genotype distributions of IL-6
-572G/C were in line with HWE, which suggest-ed that the sample size could represent the general population. Second, the sample size of
our study is small, which could reduce the sta-tistical power to find the role of IL-6 -174G/C and -572G/C polymorphisms in the risk of CAD. In conclusion, we suggest that IL-6 -174G/C is associated with the development of CAD in codominant, dominant, and recessive models. Further studies with large sample size are greatly needed to confirm the findings of our study.
Disclosure of conflict of interest
None.
Address correspondence to: Zhiliang Li, Depart-ment of Cardiology, Zhujiang Hospital, Southern Medical University, No. 253 of Industry Road, Guangzhou 510280, China. Tel: +86-20-62782250; Fax: +86-20-62782250; Email: zhiliangli66@sina. com
References
[1] He J, Gu D, Wu X, Reynolds K, Duan X, Yao C, Wang J, Chen CS, Chen J, Wildman RP, Klag MJ, Whelton PK. Major causes of death among men and women in China. N Engl J Med 2005; 353: 1124-1134.
[2] Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Judd SE, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Mackey RH, Magid DJ, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER 3rd, Moy CS, Mussolino ME, Neu-mar RW, Nichol G, Pandey DK, Paynter NP, Reeves MJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Wong ND, Woo D, Turner MB; American Heart Association Statistics Commit-tee and Stroke Statistics SubcommitCommit-tee. Heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation 2014; 129: e28-e292.
from the American Heart Association. Circula-tion 2013; 127: e6-e245.
[4] Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor cate-gories. Circulation 1998; 97: 1837-1847. [5] Marenberg ME, Risch N, Berkman LF, Floderus
B, de Faire U. Genetic susceptibility to death from coronary heart disease in a study of twins. N Engl J Med 1994; 330: 1041-1046. [6] Ross R. Atherosclerosis-an inflammatory
dis-ease. N Engl J Med 1999; 340: 115-126. [7] Papanicolaou DA, Wilder RL, Manolagas SC,
Chrousos GP. The pathophysiologic roles of in-terleukin-6 in human disease. Ann Intern Med 1998; 128: 127-137.
[8] Il’yasova D, Ivanova A, Morrow JD, Cesari M, Pahor M. Correlation between two markers of inflammation, serum C-reactive protein and in-terleukin 6, and indices of oxidative stress in patients with high risk of cardiovascular dis-ease. Biomarkers 2008; 13: 41-51.
[9] Chen Y, Zhong M, Liang L, Gu F, Peng H. Inter-leukin-17 induces angiogenesis in human cho-roidal endothelial cells in vitro. Invest Ophthal-mol Vis Sci 2014; 55: 6968-6975.
[10] Ray A, LaForge KS, Sehgal PB. On the mecha-nism for efficient repression of the interleu-kin-6 promoter by glucocorticoids: enhancer, TATA box, and RNA start site (Inr motif) occlu-sion. Mol Cell Biol 1990; 10: 5736-5746. [11] Zhang M, Cai ZR, Zhang B, Cai X, Li W, Guo Z,
Ma L. Functional polymorphisms in interleu-kin-23 receptor and susceptibility to coronary artery disease. DNA Cell Biol 2014; 33: 891-897.
[12] He F, Teng X, Gu H, Liu H, Zhou Z, Zhao Y, Hu S, Zheng Z. Interleukin-6 receptor rs7529229 T/C polymorphism is associated with left main coronary artery disease phenotype in a Chi-nese population. Int J Mol Sci 2014; 15: 5623-5633.
[13] Satti HS, Hussain S, Javed Q. Association of in-terleukin-6 gene promoter polymorphism with coronary artery disease in Pakistani families. ScientificWorldJournal 2013; 2013: 538365. [14] Elsaid A, Abdel-Aziz AF, Elmougy R, Elwaseef
AM. Association of polymorphisms G(-174)C in
IL-6 gene and G(-1082)A in IL-10 gene with tra-ditional cardiovascular risk factors in patients with coronary artery disease. Indian J Biochem Biophys 2014; 51: 282-292.
[15] Chao L, Lei H, Fei J. A meta-analysis of interleu-kin-10-1082 promoter genetic polymorphism associated with atherosclerotic risk. Neurol In-dia 2014; 62: 130-136.
[16] Gaudino M, Andreotti F, Zamparelli R, Di Castelnuovo A, Nasso G, Burzotta F, Iacoviello L, Donati MB, Schiavello R, Maseri A, Possati G. The -174G/C interleuk6 polymorphism in-fluences postoperative interleukin-6 levels and postoperative atrial fibrillation. Is atrial fibrilla-tion an inflammatory complicafibrilla-tion? Circulafibrilla-tion 2003; 108 Suppl 1: II195-II199.
[17] Tso AR, Merino JG, Warach S. Interleukin-6 174G/C polymorphism and ischemic stroke: a systematic review. Stroke 2007; 38: 3070-3075.
[18] Galimudi RK, Spurthi MK, Padala C, Kumar KG, Mudigonda S, Reddy SG, Aiyengar MT, Sahu SK, Rani SH. Interleukin 6(-174G/C) vari-ant and its circulating levels in coronary artery disease patients and their first degree rela-tives. Inflammation 2014; 37: 314-321. [19] Hou H, Wang C, Sun F, Zhao L, Dun A, Sun Z.
Association of interleukin-6 gene polymor-phism with coronary artery disease: an updat-ed systematic review and cumulative meta-analysis. Inflamm Res 2015; 64: 707-720. [20] Li L, Li E, Zhang LH, Jian LG, Liu HP, Wang T.
IL-6-174G/C and IL-6-572C/G polymorphisms are associated with increased risk of coronary artery disease. Genet Mol Res 2015; 14: 8451-8457.
[21] Song Y, Gu HD, He Y, Wang JW. Role of IL-6
polymorphism on the development of cardio-vascular events and coronary artery disease in patients receiving hemodialysis. Genet Mol Res 2015; 14: 2631-2637.