C
URRENTO
PINIONEndoscopic stitching: techniques and indications
Ryan Law and John A. Martin
Purpose of review
Endoscopic suturing has evolved dramatically over the past decade. Early suturing devices had significant limitations preventing widespread use. Newer devices, though not perfect, have overcome many of these limitations. The purpose of this review is to discuss the techniques and current indications for endoscopic suturing.
Recent findings
In addition to technological advances, the indications for endoscopic suturing continue to increase in number. Recent literature has demonstrated successful use of endoscopic suturing for the treatment of procedural adverse events such as leaks, perforations, and fistulas, but newer indications such as anchoring of self-expandable metal stents and bariatric therapy, both primary and secondary, have also been proven to be successful.
Summary
The availability of endoscopic suturing will likely increase in the coming years and will not be limited to expert centers. Currently available devices require technical expertise but are improved over previous devices. Keywords
endoscopic suturing, tissue closure
INTRODUCTION
Endoscopic suturing is an innovative and minimally invasive technique that can be used for a variety of gastrointestinal indications. This technique has obvious advantages over surgical intervention, including shorter hospital stays, reduced postproce-dure pain, faster recovery, and lack of visible scar-ring. A variety of endoscopic suturing devices have been described over the past several years, including the EndoCinch [1] and Eagle Claw devices [2], but each has had notable limitations preventing wide-spread use. Currently, the only Food and Drug Administration (FDA)-approved endoscopic sutur-ing device is the OverStitch Endoscopic Sutursutur-ing System (Apollo Endosurgery, Austin, Texas, USA). This endoscopic platform has overcome many limita-tions of previous devices and is currently being used for approximation of tissue defects, primary and secondary bariatric interventions, and to anchor stents within the gastrointestinal lumen.
TECHNIQUE
The OverStitch is a single-use device that attaches directly to a dual-channel gastroscope (GIF-2T160; Olympus America, Center Valley, Pennsylvania, USA) and allows placement of full-thickness sutures in an interrupted or running pattern. This device
can deploy both absorbable and nonabsorbable sutures with the ability to reload additional suture material while maintaining direct endoscopic visualization, a major advancement over previous endoscopic suturing devices [3].
The OverStitch device mounts over the scope tip in a cap-like fashion. This cap includes the suture arm, which moves in an arc-like manner, and the anchor exchange channel. The suture arm is con-nected to and controlled by a hand lever that attaches near the hand controls of the endoscope. The suture cartridge is passed through an operating channel and contains suture material attached to a pointed tissue anchor. The tissue anchor attaches to the suture arm and serves to drive suture material through the tissue of interest when suturing. If full-thickness sutures are desired, a helix device is also included in the kit. This accessory can be passed through the alternate operating channel and used to
Department of Medicine, Division of Gastroenterology and Hepatology, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA
Correspondence to John A. Martin, MD, 676 North St. Clair Street, Suite 1400, Chicago, IL 60611, USA. Tel: +1 312.259.1639; e-mail: j-martin3 @northwestern.edu
Curr Opin Gastroenterol2014, 30:457–462 DOI:10.1097/MOG.0000000000000112
‘corkscrew’ into the tissue of interest for tissue retraction and placement of full-thickness sutures. Finally, a cinching device is utilized to secure the sutures.
INDICATIONS
The current indications for endoscopic suturing include tissue closure, bariatric interventions, and anchoring of stents.
Tissue closure (fistulae/leaks/perforations,
endoscopic mucosal resection/endoscopic
submucosal dissection, peroral endoscopic
myotomy)
Endoscopic suturing is an ideal technique for closure of tissue defects within the gastrointestinal lumen, irrespective of the cause. Much of the cur-rent body of literature is identified in small case series or case reports, and, in some cases, animal models.
Multiple authors have identified successful closure of gastrointestinal fistulae using endolumi-nal sutures [4–7]. Kantsevoy and Thuluvath [6] first reported placement of three interrupted sutures using the OverStitch device for closure of a refrac-tory gastrocutaneous fistula after failed closure attempts using gluing agents and through-the-scope (TTS) endoclips. A similar report from Europe described similar success with endoscopic suturing for a chronic percutaneous endoscopic gastrostomy (PEG)-related gastrocutaneous fistula in a patient
with AIDS [4]. Stanichet al. [7] reported the use of
endoscopic suturing in a patient with a PEG tube to reduce an enlarged stoma. Removal of the PEG tube was not feasible as the tract had not matured. In this case, the authors describe a unique procedure in which they placed a single running suture to create a ‘mucosal wrap’ to decrease the stoma size and minimize leakage of gastric contents. Treatment of nongastric fistulae has also been described. Bonin
et al.[5] described successful closure of a refractory 10 mm esophagopleural fistula that occurred follow-ing Boerhaave syndrome. A three-stitch runnfollow-ing suture was placed with no evidence of contrast extravasation; however, a small contrast leak was observed on esophagram 4 weeks later. Repeat endo-scopic suturing, with the adjunctive use of argon plasma coagulation for tissue disruption and fibrin glue to aid in sealing the defect, was ultimately successful. Anecdotal evidence from the author’s institution suggests that endoscopic suturing is also successful for closure of acute perforations and post-surgical leaks despite no formal reports available in the literature.
The use of endoscopic mucosal resection and endoscopic submucosal dissection continues to increase worldwide. Both techniques allow resec-tion of luminal gastrointestinal lesions; however, these techniques often leave behind a sizable mucosal defect (Fig. 1a–c). Currently, many endo-scopists rely on TTS endoclips for closure of these defects, but endoscopic suturing also appears to be a
viable option. Kantsevoy et al. [8&
] have recently described the use of endoscopic suturing in 12 patients for closure of large mucosal defects follow-ing endoscopic submucosal dissection. The authors
used a single running suture (n¼8) or 2–4
inter-rupted sutures (n¼4) to successfully close lesions
within the stomach and colon with a mean size of more than 4 cm. No adverse events were encoun-tered, either immediate or delayed.
Tissue closure using endoscopic sutures may also be feasible following natural orifice translumi-nal endoscopic surgery, although no human studies
are available. Chiuet al.[9] have recently published
a study using a porcine model in which full-thick-ness gastric resection was performed and followed by successful closure using endoscopic sutures. This study also utilized the master and slave transluminal endoscopic robot and aimed to study whether a completely endoscopic approach could be success-ful for treatment of gastric submucosal tumors. The results suggest that closure of natural orifice trans-luminal endoscopic surgery-related defects can be attained with endoscopic suturing for either intra-luminal or extraintra-luminal procedures.
Kurian et al. [10] have described closure of an
esophagotomy that occurred during a peroral endo-scopic myotomy procedure for treatment of acha-lasia. This case describes an inadvertent full-thickness defect that occurred during creation of the mucosotomy with successful tissue closure in two layers (mucosal, circular muscle) using endo-scopic suturing. Although this case demonstrates the utility for treatment of an adverse event, it seems plausible that endoscopic suturing could also be
KEY POINTS
Endoscopic suturing is a rapidly evolving field of therapeutic endoscopy.
Currently, only one FDA-approved endoscopic suturing device is available and is capable of placing
interrupted or running sutures.
The current indications for endoscopic suturing include postprocedure adverse events (perforations, leaks, and fistulas), anchoring of self-expandable metal stents, and bariatric interventions, both primary and secondary.
useful for submucosal tunnel closure upon
com-pletion of the myotomy. Rajanet al.[11] described
the use of tunnel closure after submucosal endos-copy with mucosal flap technique was performed in a porcine model to obtain full-thickness gastric biopsies. Although not a peroral endoscopic myotomy procedure, the creation and closure of the tunnel are almost identical. Following gastric biopsy, the submucosal tunnel was successfully
closed in all animals (n¼12) using 2–4 interrupted
sutures.
Bariatrics
Recent literature supports the use of endoscopic suturing for primary bariatric therapy, revision of prior surgical procedures, and the treatment of adverse events related to bariatric surgery.
In recent years two small series have yielded promising results utilizing endoscopic suturing techniques for primary intervention in patients with
medically complicated obesity. Brethaueret al.[12]
initially published a feasibility study in 2010 that enrolled 18 patients from two tertiary care medi-cal centers to undergo transoral gastric volume reduction. This technique, termed the TRIM (Transoral Gastric Volume Reduction
) procedure, involved placement of plications within the gastric fundus and body. The TRIM pro-cedure was successfully performed in all 18 patients with no procedure-related adverse events. Data regarding decreases in mean weight, BMI, and waist circumference were presented by the same authors after 12 months [13]. In the 1-year follow-up period patients demonstrated a mean weight loss
of 11 kg (10 kg), mean decrease in BMI of 4 kg/m2
(3.5 kg/m2), and decrease in mean waist
circum-ference of 12.6 cm (9.5 cm). Decreases in mean SBP
(15.2 mmHg) and DBP (9.7 mmHg) measurements were also noted. Despite the positive findings, com-plete or partial release of the gastric plications was evident upon repeat endoscopic evaluation, suggesting limited durability. Of note, these pro-cedures were performed using the RESTORe Sutur-ing System device (Bard-Davol, Warwick, Rhode Island, USA), an improved version of the Endocinch device, which is no longer being marketed. More recently, Abu Dayyehet al. [14&&
] have described an endoscopic sleeve gastroplasty, as an alternative to surgical sleeve gastrectomy, in four patients for primary treatment of obesity. This procedure was performed by placing full-thickness, interrupted sutures throughout the length of the stomach using the OverStitch device. The sutures were placed in parallel apposing the anterior and posterior gastric walls, leading to creation of a gastric sleeve on the
FIGURE 1. (a) Large tubulovillous rectal adenoma draping between the distal valves of Houston, (b) luminal defect following complete endoscopic mucosal resection, (c) endoscopic suture closure of the luminal defect utilizing four interrupted sutures.
lesser curvature of the stomach. A mean number of
26 (SD2) sutures were required to form the length
of the sleeve. Repeat upper endoscopy at 3 months in two individuals demonstrated an intact gastric sleeve. This technique was successful in a small group of patients with minimal adverse events, thereby confirming proof of concept; however, long-term data regarding sustained weight loss has not been published.
Endoscopic suturing may also be helpful for patients with weight regain or insufficient weight loss following Roux-en-Y gastric bypass (RYGB) surgery. Prior data have suggested that increased gastrojejunal stomal diameter is a risk factor for
weight regain after RYGB (P<0.005) [15]. This
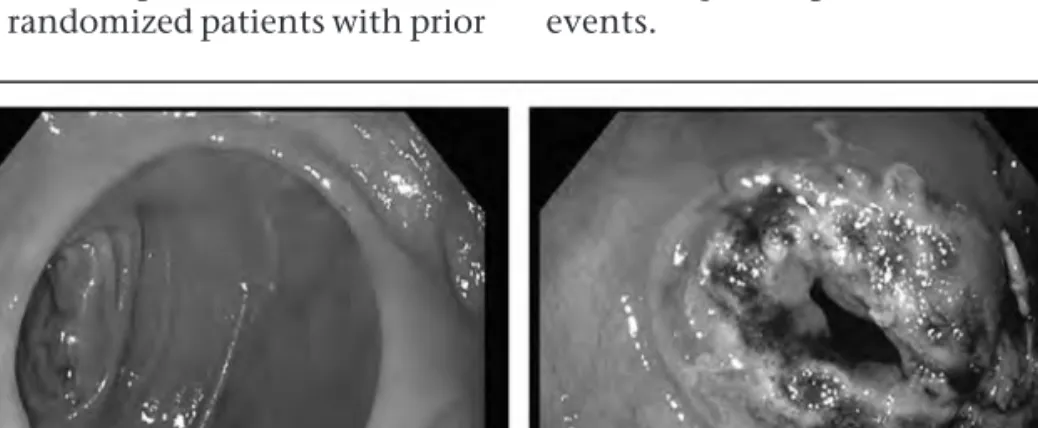
find-ing has provided an avenue to use endoluminal therapies with a goal of decreasing stoma size (Fig. 2). To date, two US studies have identified
benefit using endoscopic suturing for outlet
reduction, including a multicenter, randomized, sham-controlled trial [1,16]. The study by Jirapinyo
et al. [1] reported 100% technical success in 25 patients with a reduction in the gastrojejunal anas-tomotic diameter to less than 12 mm (mean 6 mm, range 3–10 mm) and reduction in pouch size. The mean anastomotic diameter prior to intervention was 26.4 mm (range 18–40 mm). A mean of three interrupted sutures, using the OverStitch device, was necessary to achieve this 77% reduction in endoluminal stomal diameter. This technique involved placement of sutures in a distal-to-proximal fashion followed by placement of sutures in the distal pouch for pouch reduction when indi-cated. Successful weight loss was noted at 3-month, 6-month, and 12-month follow-up visits with mean weight loss of 11.5, 11.7, and 10.8 kg, respectively.
Of note, intraprocedural (n¼3) and postprocedural
(n¼6) adverse events were noted, including three
of moderate severity (one transfusion, two repeat endoscopy) [17]. A follow-up multicenter clinical trial (RESTORe Trial) randomized patients with prior
RYGB and weight regain, or inadequate weight loss, to endoscopically sutured outlet reduction or sham procedure [16]. This study confirmed the findings by
Jirapinyo et al. [1] as patients in the intervention
group demonstrated greater mean percentage
weight loss from baseline (3.5 vs. 0.4%, P¼0.021).
In the treatment arm 96% of patients achieved weight loss or weight stabilization, compared with
78% in the sham cohort (P<0.001). The suture
pattern was quite similar to the prior study; how-ever, this study utilized the EndoCinch Suturing System (C.R. Bard, Inc., Murray Hill, New Jersey, USA), a suction-based device that allows the place-ment of sutures at a relatively superficial depth compared with the full-thickness sutures available using the Overstitch. Of note, this device is not currently available for commercial use.
Endoscopic treatment of postbariatric adverse events may also be feasible using endoscopic sutur-ing techniques, although limited data have been
published to date. Jirapinyo et al. [18] described
the use of endoscopic suturing for the treatment of recalcitrant marginal ulceration in three patients with prior RYGB who failed to heal on conservative therapy (i.e., proton pump inhibitors, sucralfate). All procedures were technically successful follow-ing placement of interrupted sutures (range 1–3) through adjacent healthy tissue. Tightening of the sutures then leads to tissue eversion with mucosa-to-mucosa apposition to close the ulcer bed. All patients in this study demonstrated durable resol-ution of the original marginal ulcer. It should be noted that fibrin glue was applied to the suture line prior to completion of the procedure, further strengthening the closure. Although not described in the current literature, endoscopic suturing can also be utilized for closure of postbariatric surgery perforations, leaks, and fistulae. The technique for suture placement is similar and this provides a nonsurgical option for management of these events.
Anchoring of covered self-expandable metal
stents
Migration of covered self-expandable metal stents (SEMS) remains a major problem occurring more frequently in the absence of an anchoring substrate, such as a luminal narrowing or mass lesion. Previous endoscopic techniques to anchor SEMS, including TTS endoclips, have yielded unreliable results.
Endoscopic suturing has proven to be useful in the anchoring of covered SEMS when used within the gastrointestinal tract for benign and malignant indications (Fig. 3a–c). To date, three studies have identified the utility of this technique for prevention of stent migration [19&&
,20,21]. The available litera-ture remains quite sparse as these articles encompass only 30 patients in total, with 26 of 30 patients undergoing endoscopic suture placement to the esophageal wall. The remaining four patients had sutures placed into the gastric wall. Following SEMS placement or repositioning, the endoscopic suturing device was introduced and advanced to the level of proximal stent flange, wherein a variety of suture techniques have been used to secure the stent. Successful outcomes have been identified using interrupted sutures [19&&
,20] (ranging from 1 to 5) or dual figure-of-eight sutures [21].
Despite the limited experience, the available data suggest that endoscopic suturing is efficacious and well tolerated as covered SEMS migration was prevented in more than 70% of cases with no peri-procedural or postperi-procedural adverse events related to suture placement. Obvious modifiable factors to further mitigate stent migration remain challeng-ing to discern. One potentially important factor proposed by Fujiiet al.[19&&
] and Riederet al.[21]
relates to the tension and depth of suture place-ment. Both groups of authors suggest that super-ficial placement may lead to suture dislodgement and stent migration; however, the risk of stent migration must be weighed against the risk of full-thickness suture placement as injury to struc-tures outside the gastrointestinal lumen are
possible. Rieder et al. encountered two cases
wherein excessive suture tension caused the suture to become free by cutting through the mucosa, similar to a cutting section placed for a perianal fistula. This finding emphasizes the importance of secure apposition without tissue strangulation. Interestingly, in both cases the stent remained well positioned despite freeing of the suture.
Although the data appear promising, further large-scale studies are needed to validate the above findings. Additionally, it should be noted that stent anchoring using endoscopic sutures can only be performed in areas within reach of a therapeutic gastroscope.
CONCLUSION
Given the increasing variety of procedural indica-tions and the rising number of publicaindica-tions
FIGURE 3.(a) Benign esophagogastric anastomotic stricture following Ivor–Lewis esophagectomy, (b) placement of a fully covered self-expandable metal stent bridging the stricture, (c) endoscopic placement of three interrupted sutures to anchor the proximal stent flare for prevention of migration.
available, it appears that endoscopic suturing is finally here to stay. The OverStitch device, the only FDA-approved device on the market, represents advancement upon prior endoscopic suturing devi-ces. The main advantages over prior devices are as follows: the ability to reload suture material without removal of the endoscope from the patient; the lack of suction-based technology, which allows more reliable depth of needle penetration; and the utiliz-ation of only one operating channel, allowing the use of tissue grasping accessories in the opposing channel. Although the results from this technique appear encouraging, it should be noted that certain limitations and drawbacks persist. This technique remains limited by availability and the need for technical expertise for successful operation. This device can be cumbersome to use, time-consuming, and is likely available only at tertiary referral centers. Additionally, OverStitch is a single-use device only compatible with a single endoscope (GIF-2T160; Olympus America, Inc., Center Valley, PA), thereby limiting its use to lesions within reach of a gastro-scope. Further iterations of endoscopic suturing devices should focus to improve upon these issues.
Acknowledgements
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDED
READING
Papers of particular interest, published within the annual period of review, have been highlighted as:
& of special interest && of outstanding interest
1. Jirapinyo P, Slattery J, Ryan MB,et al.Evaluation of an endoscopic suturing device for transoral outlet reduction in patients with weight regain following Roux-en-Y gastric bypass. Endoscopy 2013; 45:532–536.
2. Pham BV, Raju GS, Ahmed I,et al.Immediate endoscopic closure of colon perforation by using a prototype endoscopic suturing device: feasibility and outcome in a porcine model (with video). Gastrointest Endosc 2006; 64: 113–119.
3. Banerjee S, Barth BA, Bhat YM,et al.Endoscopic closure devices. Gastro-intest Endosc 2012; 76:244–251.
4. Armengol-Miro JR, Dot J, Abu-Suboh Abadia M,et al.New endoscopic suturing device for closure of chronic gastrocutaneous fistula in an immu-nocompromised patient. Endoscopy 2011; 43 (Suppl 2 UCTN):E403 – E404.
5. Bonin EA, Wong Kee Song LM, Gostout ZS,et al.Closure of a persistent esophagopleural fistula assisted by a novel endoscopic suturing system. Endoscopy 2012; 44 (Suppl 2 UCTN):E8–E9.
6. Kantsevoy SV, Thuluvath PJ. Successful closure of a chronic refractory gastrocutaneous fistula with a new endoscopic suturing device (with video). Gastrointest Endosc 2012; 75:688–690.
7. Stanich PP, Sklaw B, Krishna SG. Persistent peristomal leakage from per-cutaneous endoscopic gastrostomy successfully treated with endoscopic suturing. Endoscopy 2013; 45 (Suppl 2 UCTN):E394.
8.
&
Kantsevoy SV, Bitner M, Mitrakov AA, Thuluvath PJ. Endoscopic suturing closure of large mucosal defects after endoscopic submucosal dissection is technically feasible, fast, and eliminates the need for hospitalization (with videos). Gastrointest Endosc 2014; 79:503–507.
This study identifies successful closure of defects within the gastrointestinal lumen using endoscopic suturing.
9. Chiu PW, Phee SJ, Wang Z,et al.Feasibility of full-thickness gastric resection using master and slave transluminal endoscopic robot and closure by Over-stitch: a preclinical study. Surg Endosc 2014; 28:319–324.
10. Kurian AA, Bhayani NH, Reavis K,et al.Endoscopic suture repair of full-thickness esophagotomy during per-oral esophageal myotomy for achalasia. Surg Endosc 2013; 27:3910.
11. Rajan E, Gostout CJ, Aimore Bonin E,et al.Endoscopic full-thickness biopsy of the gastric wall with defect closure by using an endoscopic suturing device: survival porcine study. Gastrointest Endosc 2012; 76:1014 –1019.
12. Brethauer SA, Chand B, Schauer PR, Thompson CC. Transoral gastric volume reduction for weight management: technique and feasibility in 18 patients. Surg Obes Relat Dis 2010; 6:689–694.
13. Brethauer SA, Chand B, Schauer PR, Thompson CC. Transoral gastric volume reduction as intervention for weight management: 12-month follow-up of TRIM trial. Surg Obes Relat Dis 2012; 8:296–303.
14.
&&
Abu Dayyeh BK, Rajan E, Gostout CJ. Endoscopic sleeve gastroplasty: a potential endoscopic alternative to surgical sleeve gastrectomy for treatment of obesity. Gastrointest Endosc 2013; 78:530–535.
This study demonstrates efficacy of endoscopically created gastric sleeve, akin to surgical sleeve gastrectomy.
15. Abu Dayyeh BK, Lautz DB, Thompson CC. Gastrojejunal stoma diameter predicts weight regain after Roux-en-Y gastric bypass. Clin Gastroenterol Hepatol 2011; 9:228–233.
16. Thompson CC, Chand B, Chen YK,et al.Endoscopic suturing for transoral outlet reduction increases weight loss after Roux-en-Y gastric bypass surgery. Gastroenterology 2013; 145:129.e123–137.e123.
17. Cotton PB, Eisen GM, Aabakken L,et al.A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc 2010; 71:446– 454.
18. Jirapinyo P, Watson RR, Thompson CC. Use of a novel endoscopic suturing device to treat recalcitrant marginal ulceration (with video). Gastrointest Endosc 2012; 76:435–439.
19.
&&
Fujii LL, Bonin EA, Baron TH,et al.Utility of an endoscopic suturing system for prevention of covered luminal stent migration in the upper GI tract. Gastro-intest Endosc 2013; 78:787–793.
This study outlines the use of anchoring of self-expandable metal stents within the upper gastrointestinal tract.
20. Kantsevoy SV, Bitner M. Esophageal stent fixation with endoscopic suturing device (with video). Gastrointest Endosc 2012; 76:1251 –1255.
21. Rieder E, Dunst CM, Martinec DV, et al.Endoscopic suture fixation of gastrointestinal stents: proof of biomechanical principles and early clinical experience. Endoscopy 2012; 44:1121–1126.