Arrhythmia/electrophysiology
Familial clustering of lone atrial fibrillation in patients
with saddleback-type ST-segment elevation in right
precordial leads
M. Juhani Junttila
1*, M.J. Pekka Raatikainen
1, Juha S. Perkio
¨ma
¨ki
1, Kui Hong
2, Ramon Brugada
3,
and Heikki V. Huikuri
11
Department of Internal Medicine, Division of Cardiology, University of Oulu, PO Box 5000, Oulu 90014, Finland; 2
Baylor College of Medicine, Houston, TX, USA; and3Montreal Heart Institute, Montreal, Canada
Received 7 September 2006; revised 28 November 2006; accepted 21 December 2006; online publish-ahead-of-print 22 January 2007
AimsWe recently identified a large family with a high prevalence of lone atrial fibrillation (AF) and saddleback-type ST-segment elevation in leads V1–3, without a history of ventricular arrhythmias or syncope. On the basis of this finding, we studied whether there is a relationship between saddleback ST-elevation and lone AF.
Methods and resultsWe examined 168 (mean age 50+8 years, 130 males) lone AF patients and 541 (mean age 50+6 years, 274 males) healthy subjects. The prevalence of saddleback ST-elevation was higher in the lone AF group than the control group (10 vs. 0.4%,P,0.001). None had a coved-type ST-elevation in baseline ECG or during drug challenge with ajmaline or flecainide (n¼13), a family history of sudden cardiac death, ventricular tachyarrhythmias, syncope, or any other features diagnos-tic to the Brugada syndrome. Familial clustering of lone AF (i.e. AF in.30% of first-degree relatives) was more common among the subjects with saddleback ST-elevation (24 vs. 7%,P¼0.03).
ConclusionSaddleback-type ST-segment elevation is a relatively common finding among patients with lone AF. The familial clustering of the disorder indicates that genetic factors may be involved in the pathogenesis of the ECG abnormality and lone AF in these patients.
KEYWORDS
Atrial fibrillation; Inherited arrhythmias; Electrocardiogram
Introduction
Lone atrial fibrillation (AF) is defined as an arrhythmic dis-order in patients with no clinical or echocardiographic evi-dence of cardiopulmonary disease or any other secondary cause of AF. The patients are typically under 60 years of age and have a favourable prognosis with respect to thrombo-embolism and mortality. Several population-based studies have recently noted a familial aggregation of AF and a high risk of lone AF in individuals with parental AF.1–4 Although the knowledge of the mechanisms of AF has increased markedly during recent years, the molecular and genetic backgrounds of the initiation and perpetuation of AF are largely unknown.5 In particular, more data on
the potential role of genetic factors in the pathogenesis of AF are needed.
Elevation of the ST-segment in the right precordial ECG leads V1–3 has been previously linked to the Brugada
syn-drome.6Brugada syndrome is a hereditary cardiac ion chan-nelopathy, which predisposes the patients not only to ventricular tachyarrhythmias (VT) and sudden cardiac death (SCD), but also to supraventricular arrhythmias
including AF.7–9 However, saddleback-type ST-segment elevation (type 2 and 3 Brugada ECG abnormalities) has also been observed in healthy subjects without any VT or family history of SCD.10–15 These ECG abnormalities seem to be benign and have been considered as normal var-iants.10–16Given the association between the Brugada syn-drome and AF and the anecdotal data10 from our
laboratory that saddleback-type ST-segment elevation in right precordial leads V1–3 may predispose to AF, we
decided to investigate whether there is a relationship between saddleback-type ST-segment elevation and lone AF. Our hypothesis was that saddleback-type ST-segment elevation would predispose patients to familial AF but not to syncope, VT, and SCD.
Methods
Lone AF population
The lone AF population was selected among 220 consecutive patients admitted into Oulu University Hospital for treatment of acute AF or catheter ablation of AF during the years 2002 and 2003. A total of 168 patients of them consented to the study. Their mean age was 50+8 years (range 20–63 years), and 130 (77%) of them were male. All subjects with a history of any cardiovascular, pulmonary (e.g. asthma), or metabolic
&The European Society of Cardiology 2007. All rights reserved. For Permissions, please e-mail: [email protected]
*Corresponding author. Tel:þ358 8 3154447; fax: þ358 8 3155599.
E-mail address: [email protected].fi
doi:10.1093/eurheartj/ehl474
by guest on September 16, 2016
http://eurheartj.oxfordjournals.org/
(e.g. hyperthyroidism and diabetes) diseases or with hypertension were excluded. Other exclusion criteria were electrical or medical cardioversion within 30 days before the examination, history of thoracic surgery or radio frequency catheter ablation, permanent pacemaker, and any of the following echocardiographic findings: depressed left ventricular systolic function (ejection fraction
,50%), abnormal wall motion of the left ventricle, septal hypertro-phy (.15 mm), left atrial (LA) size.50 mm, and significant valve abnormality. The study protocol was approved by the local insti-tutional Ethics Committee and written informed consent was obtained from all study subjects.
Control population
The control population was selected among the subjects who had initially participated in the ‘Opera’ study.17 In the Opera study, 300 women and 300 men between 40 and 60 years of age were ran-domly selected from the National Social Insurance Register. The sub-jects underwent a thorough physical examination, 12-lead ECG transthoracic echocardiography, and extensive laboratory tests in Oulu University Hospital during the years 1991 and 1992 to ensure that they had no cardiovascular, pulmonary, or metabolic disorders or documented arrhythmias.17All subjects with antihypertensive or cardiac medication were excluded and 541 consented to the current study. The mean age of the control subjects was 50+6 years (range 46–60), and 274 (51%) of them were male.
Analysis of ECGs
Two independent investigators reviewed all the 12-lead ECGs (paper speed 50 mm/s and 1 mV/10 mm standard gain). The ECG criteria devised by the Study Group of the Molecular Basis of Arrhythmias of the European Society of Cardiology were used to identify the sub-jects with saddleback-type ST-segment elevation concomitant to type 2 and 3 Brugada ECG patterns.18The diagnosis saddleback-type ST-segment elevation was made when both investigators agreed on the classification of the ECG abnormality.
The authors of the Brugada syndrome consensus report rec-ommended the use of diagnostic drug challenge with a class IC anti-arrhythmic agent to unmask the coved-type ST-segment elevation among the subjects with type 2 or 3 ECG changes in the baseline ECG.16 Therefore, a diagnostic drug challenge with flecainide (150 mg or 2 mg/kg over 10 min) or ajmaline (50 mg or 1 mg/kg over 5 min) was offered to all the subjects with a saddleback-type ST-segment elevation and a history of AF episodes. Thirteen sub-jects (76%) consented to the test.
Clinical characteristics and family history of patients with lone AF
The family history of AF, syncope, and VT was evaluated by a mailed questionnaire. The information was verified by phone conversation and original patient records were acquired from the referring hospi-tals and primary care physicians. The time of the first AF episode, total number of symptomatic AF episodes, and a complete family history of documented AF episodes were obtained from all patients. The family history of AF was considered positive if at least one of the first-degree family members (i.e. parents, siblings, or children) had had ECG-documented AF episode(s). A clear family history of AF, suggesting autosomal dominant inheritance, was defined as docu-mented AF in.30% of the first-degree family members.
Genetic screening
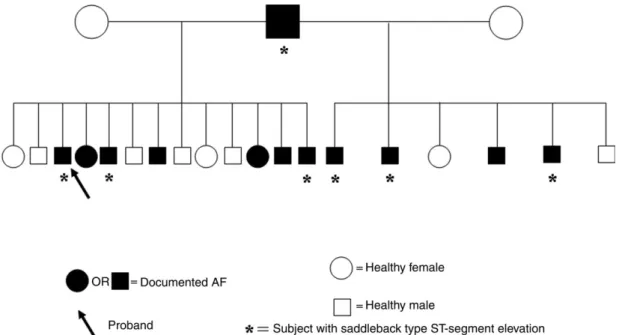
One family with 19 siblings had an extraordinary high occurrence of lone AF and saddleback-type ST-segment elevation (Figure 1). In this family, the SCN5A gene that has been previously described in the Brugada syndrome was screened from the affected proband of the family.18 Genomic DNA was isolated from peripheral blood leuco-cytes using the commercial kit (Gentra System, Puregene,
Minneapolis, MN, USA). Exons of the SCN5A were amplified and ana-lysed by direct sequencing, using primers designed from the pub-lished gene sequence. Polymerase chain reaction products were purified with a commercial reagent (ExoSAP-IT, USB, Cleveland, OH, USA) and directly sequenced from both directions with an ABI PRISM 3100-Avant Automatic Sequencer (Foster City, CA, USA).
Statistical analyses
The data were analysed using SPSS 10.1 software (SPSS Inc., Chicago, IL, USA). The statistical significance of the differences between the populations was analysed with a two-sided Mann– Whitney non-parametric test. A pre-specified value of P,0.05 was considered statistically significant.
Results
Prevalence of saddleback-type ST-segment elevation ECGs
The prevalence of saddleback-type ST-segment elevation
(Figure 2A) was significantly higher among the patients
with lone AF (17/168, 10%, 95% CI: 6–15%) than the healthy control subjects (2/541, 0.4%, 95% CI: 0–0.9%) (P,0.001) (Figure 3). None of the patients with lone AF had coved-type ST-segment elevation (malignant type 1 Brugada ECG) at baseline ECG or after drug challenge with flecainide (n¼8) or ajmaline (n¼5) (Figure 2B).
Clinical characteristics
The clinical characteristics and echocardiographic data are presented in Table 1. With respect to the patients with lone AF, there were no differences in the duration of AF history (P¼0.17), age at AF onset (P¼0.10), total number of symptomatic AF episodes (P¼0.73), fractional shortening (P¼0.79), or LA size (P¼0.77) between the subjects with saddleback ST-elevation and those with normal ECG.
Family history of AF and genetic screening
Many patients with lone AF and saddleback-type ST-segment elevation had familial clustering of lone AF. Overall, 59% of the patients with the saddleback ST-elevation and lone AF had at least one of their first-degree family members (i.e. parents, siblings, or children) with ECG-documented AF epi-sode(s). In those patients with lone AF but no ECG abnorm-alities, the family history for lone AF was positive in 36% of the cases (P¼0.07). A clear family history of AF (.30% of first-degree relatives with AF episodes) was significantly more common among the patients with the saddleback ST-elevation (24 vs. 7%,P¼0.03). In one large family with 19 siblings, 11 had AF and six of them also exhibited the saddleback-type ST-segment elevation (Figure 1). The pedi-gree suggests an autosomal dominant pattern of inheri-tance. Genetic analysis of the proband in this particular family did not identify any mutations in the SCN5A gene. Therefore, all known or unknown mutations in this gene that may cause the Brugada syndrome have been excluded in this family. None of the patients with lone AF and the benign Brugada-type ECG had personal or family history of SCD, life-threatening ventricular arrhythmias, or syncope.
by guest on September 16, 2016
http://eurheartj.oxfordjournals.org/
Discussion
In the present study, the prevalence of saddleback-type ST-segment elevation (types 2 and 3) was significantly higher among patients with lone AF than in healthy control subjects. Many patients with saddleback-type ST-segment elevation abnormality exhibited familial clustering of lone AF. These findings suggest that (i) there may be a link between the electrophysiological mechanism(s) underlying saddleback-type ST-segment elevation and lone AF and (ii) genetic factors may be involved in the pathogenesis of AF in these patients.
Saddleback-type ST-segment elevation and AF
In agreement with our hypothesis, we found that the prevalence of saddleback-type ST-segment elevation was
significantly higher among the patients with lone AF than in the healthy control subjects. Although 20% of the patients with Brugada syndrome have AF,7,8,16 to the best of our
knowledge, there have been no prior studies examining the association between this specific ECG abnormality and AF in patients with no personal or family history of syncope, VT, or SCD.
Despite the similar ECG repolarization abnormalities, several findings indicate that the patients described here do not have the classic Brugada syndrome. (i) According to a recently published consensus report, only type 1 ST-segment elevation (i.e. the coved type) is diagnostic for Brugada syndrome.16 Here, all patients had either type 2 or type 3 (i.e. saddleback type) ECG, both at baseline and after drug challenge. (ii) In contrast to the patients with
Figure 1 Pedigree of a family with a high prevalence of lone AF and saddleback-type ST-segment elevation. Females are represented by circles and males by squares. Subjects with AF are designated by filled symbols. In addition to the proband (marked with an arrow), five other siblings and the father of the siblings (who also had lone AF) had saddleback-type ST-segment elevation and these subjects are marked with a star (asterisk) under the symbol.
Figure 2 Typical example of saddleback-type ST-segment elevation in a patient with lone AF in baseline ECG and during drug challenge. The precor-dial leads (V1–V6) of a subject who presented with a saddleback-type elevation of the J-point and the ST-segment at baseline ECG (A) and during drug challenge with flecainide (B) are also shown. Gain 10 mm/mV and paper speed 50 mm/s. See online supplementary material for a colour version of this figure.
Figure 3 Prevalence of saddleback-type ST-segment elevation in patients with lone AF and healthy control subjects. The prevalence of saddleback-type ST-segment elevation among patients with lone AF is depicted with the column on the left (10%, 95% CI: 6–15%), whereas the column on the right rep-resents the control population (0.4%, 95% CI: 0–0.9%).P,0.001 lone AF vs. control.
by guest on September 16, 2016
http://eurheartj.oxfordjournals.org/
the Brugada syndrome, none of our patients with lone AF had a personal or family history of syncope, life-threatening VT, and SCD, although Brugada syndrome patients with atrial arrhythmias have been reported to have a higher risk of VT than those without atrial arrhythmias.9 In our previous
study, we found 18 patients with saddleback-type ST-segment elevation among over 3000 healthy subjects.10 None of these subjects had a family history of syncope, VT, or SCD. Hence, despite the potential link between the elec-trophysiological features that cause the Brugada-type ECG pattern and lone AF, it is concluded that familiar AF described here is a disease entity distinct from the Brugada syndrome.
Familial clustering of lone AF among subjects with saddleback-type ST-segment elevation
The number of first-degree family members with AF was higher among the subjects with the saddleback-type ST-segment elevation. In particular, the subjects with the benign Brugada-type ECG pattern had a clear family history (i.e. AF in .30% of their first-degree relatives). There were no other differences in the clinical character-istics or arrhythmia history between the lone AF patients with and without saddleback ST-elevation. Thus, it is poss-ible that a hereditary ion channel dysfunction may be involved in the pathogenesis of AF in these patients. The occurrence of lone AF in.30% of the first-degree relatives of the patients, i.e. familiar clustering of AF, is consistent with an autosomal dominant mode of inheritance with a high penetrance.
Several population-based studies have recently described the familial aggregation of AF and a high risk of lone AF in individuals with parental AF.1 For example, Ellinor et al. reported that 38% of the patients with lone AF had a family history of this disorder. A very high risk of lone AF has also been observed in affected siblings, with risk ratios of up to 70-fold among the male siblings of affected patients.2–4 Brugada and coworkers described five Spanish
families in whom persistent AF was inherited as an
autosomal dominant trait with high penetrance. The arrhythmia was attributable to mutations in the region 10q22–24 of chromosome 10.19 More recently, another
locus for AF has been mapped to chromosome 6q14–16,20 and a four-generation family with hereditary AF caused by a gain-of-function mutation in the KCNQ1 gene encoding a subunit of the cardiac potassium channel IKs was described.21In contrast to the previous studies,1–4,19–21 fam-iliar clustering of AF, in our study, was associated with a dis-tinct ECG abnormality. It is anticipated that the ongoing genetic analyses will clarify our understanding of the gen-etics of lone AF.
Potential link between lone AF and saddleback-type ST-segment elevation
Our data indicate that there may be a link between the elec-trophysiological features that cause the saddleback-type ST-segment elevation and lone AF. The familial clustering of lone AF is consistent with an autosomal dominant mode of inheritance with high penetrance. This and the close relationship between saddleback-type ST-segment elevation and lone AF support the concept that the disorder is caused by a mutation in some of the ion channels, which play a role both in the pathogenesis of AF and in the early ventricular repolarization. The ECG pattern in our patients mimicked that seen in patients with the Brugada syndrome and the SCN5A mutations, but had a more benign clinical character-istics. Mutations in the SCN5A gene were excluded in the genetic analysis. The other potential candidates include mutation(s) or a polymorphism in the genes that encode or regulate the function of the ion channels, which are active during the depolarization and early repolarization of the myocardial cells (e.g.INa, Ito, andIKur). Abnormal function of these channels could not only explain the ECG pattern but also has been shown to play an important role in the pathogenesis of AF by modulating atrial conduction velocity and refractoriness.5Conduction slowing would also have a major effect on generating AF.5 Regional conduction
slowing in the atrial muscle could also provide a similar
Table 1 Clinical characteristics of the control subjects and the patients with lone AF Control subjects
(n¼541)
Patients with lone AF (n¼168)
Normal ECG (n¼151) Saddleback-type ST-elevation (n¼17)
Age (years) 50+6 50+8 49+9
Sex
Male 274 (51%) 116 (77%) 14 (82%)
Female 267 (49%) 35 (23%) 3 (18%)
AF history No Yes Yes
Age at AF onset (years) 41+10 37+10
Duration of AF history (years) 9+7 11+9
Number of symptomatic AF episodes 44+105 21+31
AF in at least one family member 55 (36%) 10 (59%) AF in.30% of family members 11 (7%) 4 (24%)a Echocardiographic findings LA diameter (mm) 39+5 40+5 41+5 Fractional shortening (%) 34+6 36+11 37+9 aP,0.05 vs. normal ECG. by guest on September 16, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from
heterogenous substrate to AF. In the future, detailed evalu-ation of the P-wave morphology with signal average ECG or other novel methods as well as further genetic and electro-physiological studies may offer explanation for the link between the lone AF and the saddleback ST-elevation.
In contrast, it is tempting to speculate that the ECG changes may not have been the cause of AF, but rather its consequence. It is well established that AF begets AF by inducing electrical and structural changes in the atria and ventricles.22 At the cellular level, electrical remodelling is linked to downregulation of several ionic currents (e.g.Ito,
IKur,ICa,L, andINa).23,24At first, this seems to be incompatible
with the ionic changes that initiate the saddleback-type ST-segment elevation.25,26 One possible explanation for this paradoxical phenomenon is that the contribution ofIto
andIKurto early myocardial repolarization becomes accentu-ated in remodelled tissues. In line with this idea, Blaauw
et al.27recently showed that, unlike the effects ofIKr
block-ers, the effect of a specificIKur/Itoblocker was enhanced in
the remodelled atria. Nevertheless, we found no correlation between the occurrence of saddleback-type ST-segment elevation and the duration of AF history or the total number of symptomatic AF episodes.
Limitations
Our data provide no direct evidence to identify the potential mutations underlying the ECG abnormality and lone AF. The genetic screening of the lone AF families and the benign Brugada-type ECG is ongoing. Therefore, we do not believe that one should speculate further on the genetic aetiology of this disorder. In comparison with many other countries, the genetic heritage in Finland is extremely homogeneous.28 Therefore, it would be interesting to test
whether our hypothesis is true also in other populations with different and less homogeneous genetic backgrounds. Finally, the potential effect of atrial remodelling on the ECG pattern of patients with lone AF needs to be evaluated in prospective trials.
Conclusion
Saddleback-type ST-segment elevation is significantly more frequent among patients with lone AF than healthy control subjects. The familial clustering of the disorder indicates that a hereditary ion channel dysfunction may be involved in the pathogenesis of ECG abnormalities and lone AF in these patients. Ongoing genetic screening of the families is expected to reveal more details of the molecular and genetic mechanisms of the disorder, which is characterized by lone AF and saddleback-type ST-segment elevation.
Supplementary Material
Supplementary material is available at European Heart
Journalonline.
Acknowledgements
We are grateful to Kai Lindgren, Antero Kesa¨niemi, and Heikki Kauma, who were a great help in this study by gathering the control data and part of the data of the study population. We would also like to thank Pirkko Huikuri, who helped us in the examination of the study subjects. We would like to thank the Medical Council of the Finnish Academy of Science, Helsinki, Finland, the Foundation for
Cardiovascular Research, Helsinki, Finland, and the Aarne Koskelo Foundation, Helsinki, Finland for the support to our study.
Conflict of interest: none declared.
References
1. Fox CS, Parise H, D’Agostino RB Sr, Lloyd-Jones DM, Vasan RS, Wang TJ, Levy D, Wolf PA, Benjamin EJ. Parental atrial fibrillation as a risk factor for atrial fibrillation in offspring.JAMA2004;291:2851–2855.
2. Patton KK, Zacks ES, Chang JY, Shea MA, Ruskin JN, Macrae CA, Ellinor PT. Clinical subtypes of lone atrial fibrillation. Pacing Clin Electrophysiol 2005;28:630–638.
3. Ellinor PT, Yoerger DM, Ruskin JN, MacRae CA. Familial aggregation in lone atrial fibrillation.Hum Genet2005;118:179–184.
4. Arnar DO, Thorvaldsson S, Manolio TA, Thorgeirsson G, Kristjansson K, Hakonarson H, Stefansson K. Familial aggregation of atrial fibrillation in Iceland.Eur Heart J2006;27:708–712.
5. Nattel S. New ideas about atrial fibrillation 50 years on. Nature 2002;415:219–226.
6. Brugada P, Brugada J. Right bundle-branch block, persistent ST-segment elevation and sudden cardiac death: a distinct clinical and electrocardio-graphic syndrome: a multicenter report.J Am Coll Cardiol 1992;20: 1391–1396.
7. Itoh H, Shimizu M, Ino H, Okeie K, Yamaguchi M, Fujino N, Mabuchi H, Hokuriku Brugada Study Group. Arrhythmias in patients with Brugada-type electrocardiographic findings.Jpn Circ J2001;65:483–486. 8. Eckardt L, Kirchhof P, Loh P, Schulze-Bahr E, Johna R, Wichter T,
Breithardt G, Haverkamp W, Borggrefe M. Brugada syndrome and supra-ventricular tachyarrhythmias: a novel association? J Cardiovasc
Electrophysiol2001;6:680–685.
9. Bordachar P, Reuter S, Garrigue S, Cai X, Hocini M, Jais P, Haissaguerre M, Clementy J. Incidence, clinical implications and prognosis of atrial arrhythmias in Brugada syndrome.Eur Heart J2004;10:879–884. 10. Junttila MJ, Raatikainen MJ, Karjalainen J, Kauma H, Kesaniemi YA,
Huikuri HV. Prevalence and prognosis of subjects with Brugada-type ECG pattern in a young and middle-aged Finnish population.Eur Heart J2004;10:874–878.
11. Miyasaka Y, Tsuji H, Yamada K, Tokunaga S, Saito D, Imuro Y, Matsumoto N, Iwasaka T. Prevalence and mortality of the Brugada-type electrocar-diogram in one city in Japan.J Am Coll Cardiol2001;38:771–774. 12. Matsuo K, Akahoshi M, Nakashima E, Suyama A, Seto S, Hayano M,
Yano K. The prevalence, incidence and value of the Brugada-type electrocardiogram: a population based study of four decades. J Am
Coll Cardiol2001;38:765–770.
13. Furuhashi M, Uno K, Tsuchihashi K, Nagahara D, Hyakukoku M, Ohtomo T, Satoh S, Nishimiya T, Shimamoto K. Prevalence of asymptomatic ST segment elevation in right precordial leads with right bundle branch block (Brugada-type ST shift) among the general Japanese population.
Heart2001;86:161–166.
14. Atarashi H, Ogawa S, Harumi K, Sugimoto T, Inoue H, Murayama M, Toyama J, Hayakawa H, Idiopathic Ventricular Fibrillation Investigators. Three-year follow-up of patients with right bundle branch block and ST segment elevation in the right precordial leads: Japanese Registry of Brugada Syndrome. Idiopathic Ventricular Fibrillation Investigators.
J Am Coll Cardiol2001;37:1916–1920.
15. Hermida JS, Lemoine JL, Aoun FB, Jarry G, Rey JL, Quiret JC. Prevalence of the Brugada syndrome in an apparently healthy population. Am J
Cardiol2000;86:91–94.
16. Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, Corrado D, Gussak I, LeMarec H, Nademanee K, Perez Riera AR, Shimizu W, Schulze-Bahr E, Tan H, Wilde A. Brugada Syndrome Report of the Second Consensus Conference. Endorsed by the Heart Rhythm Society and the European Heart Rhythm Association.Circulation2005;111:659–670. 17. Huikuri HV, Pikkujamsa SM, Airaksinen KE, Ikaheimo MJ, Rantala AO,
Kauma H, Lilja M, Kesaniemi YA. Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation 1996;94:122–125.
18. Chen Q, Kirsch GE, Zhang D, Brugada R, Brugada J, Brugada P, Potenza D, Moya A, Borggrefe M, Breithardt G, Ortiz-Lopez R, Wang Z, Antzelevitch C, O’Brien RE, Schulze-Bahr E, Keating MT, Towbin JA, Wang Q. Genetic basis and molecular mechanism for idiopathic ventricular fibrillation.
Nature1998;392:293–296.
19. Brugada R, Tapscott T, Czernuszewicz GZ, Marian AJ, Iglesias A, Mont L, Brugada J, Girona J, Domingo A, Bachinski LL, Roberts R. Identification
by guest on September 16, 2016
http://eurheartj.oxfordjournals.org/
of a genetic locus for familial atrial fibrillation. N Engl J Med 1997;336:905–911.
20. Ellinor PT, Shin JT, Moore RK, Yoerger DM, MacRae CA. Locus for atrial fibrillation maps to chromosome 6q14–16. Circulation 2003;107: 2880–2883.
21. Chen YH, Xu SJ, Bendahhou S, Wang XL, Wang Y, Xu WY, Jin HW, Sun H, Su XY, Zhuang QN, Yang YQ, Li YB, Liu Y, Xu HJ, Li XF, Ma N, Mou CP, Chen Z, Barhanin J, Huang W. KCNQ1 gain-of-function mutation in familial atrial fibrillation.Science2003;299:251–254.
22. Allessie MA. Atrial electrophysiologic remodeling: another vicious circle?
J Cardiovasc Electrophysiol1998;9:1378–1393.
23. Van Wagoner DR, Pond AL, McCarthy PM, Trimmer JS, Nerbonne JM. Outward Kþcurrent densities Kv1.5 expression are reduced in chronic human atrial fibrillation.Circ Res1997;80:772–781.
24. Bosch RF, Nattel S. Cellular electrophysiology of atrial fibrillation.
Cardiovasc Res2002;54:259–269.
25. Antzelevitch C. The Brugada syndrome: ionic basis and arrhythmia mechanisms.J Cardiovasc Electrophysiol2001;12:268–272.
26. Antzelevitch C, Brugada P, Brugada J, Brugada R. Brugada syndrome: from cell to bedside.Curr Probl Cardiol2005;30:9–54.
27. Blaauw Y, Gogelein H, Tieleman RG, van Hunnik A, Schotten U, Allessie MA. ‘Early’ class III drugs for the treatment of atrial fibrillation: efficacy and atrial selectivity of AVE0118 in remodeled atria of the goat.
Circulation2004;110:1717–1724.
28. Peltonen M, Jalanko A, Varilo T. Molecular genetics of the Finnish disease heritage.Hum Mol Genet1999;8:1913–1923.
by guest on September 16, 2016
http://eurheartj.oxfordjournals.org/