The Healthcare Costs of Sarcopenia in the United States
Ian Janssen, PhD,
wDonald S. Shepard, PhD,
§Peter T. Katzmarzyk, PhD,
wzand
Ronenn Roubenoff, MD, MHS
OBJECTIVES: To estimate the healthcare costs of sarco-penia in the United States and to examine the effect that a reduced sarcopenia prevalence would have on healthcare expenditures.
DESIGN: Cross-sectional surveys.
SETTING: Nationally representative surveys using data from the U.S. Census, Third National Health and Nutrition Examination Survey, and National Medical Care and Utilization Expenditure Survey.
PARTICIPANTS: Representative samples of U.S. adults aged 60 and older.
MEASUREMENTS: The healthcare costs of sarcopenia were estimated based on the effect of sarcopenia on increasing physical disability risk in older persons. In the first step, the healthcare cost of disability in older Americans was estimated from national surveys. In the second step, the proportion of the disability cost due to sarcopenia (population-attributable risk) was calculated to determine the healthcare costs of sarcopenia. These calculations relied upon previously published relative risk values for disability in sarcopenic individuals and sarcope-nia prevalence rates in the older population.
RESULTS: The estimated direct healthcare cost attribut-able to sarcopenia in the United States in 2000 was $18.5 billion ($10.8 billion in men, $7.7 billion in women), which represented about 1.5% of total healthcare expenditures for that year. A sensitivity analysis indicated that the costs could be as low as $11.8 billion and as high as $26.2 billion. The excess healthcare expenditures were $860 for every
sarcopenic man and $933 for every sarcopenic woman. A 10% reduction in sarcopenia prevalence would result in savings of $1.1 billion (dollars adjusted to 2000 rate) per year in U.S. healthcare costs.
CONCLUSION: Sarcopenia imposes a significant but modifiable economic burden on government-reimbursed healthcare services in the United States. Because the number of older Americans is increasing, the economic costs of sarcopenia will escalate unless effective public health campaigns aimed at reducing the occurrence of sarcopenia are implemented.J Am Geriatr Soc 52:80–85, 2004. Key words: skeletal muscle; sarcopenia; disability; health-care costs
T
he aging process is associated with sarcopenia (loss of skeletal muscle mass)1–3 and an increase in theprevalence of physical disability.4 Sarcopenia5–8 and
dis-ability9–11are highly prevalent in older Americans. Recent
estimates indicate that approximately 45% of the older U.S. population is sarcopenic7and that approximately 20% of
the older U.S. population is functionally disabled.10 Not
surprisingly, sarcopenia is related to physical disability in older men and women.5–8At the individual level, disability
leads to reduced quality of life; at the societal level, it leads to an increase in healthcare expenditures. In older persons, physical disability is associated with an increased risk of nursing home placement,12 home healthcare13and
hospi-tal14use, and healthcare expenditures.4,15
Given the high prevalence of sarcopenia and disability in older persons, the strong effect sarcopenia has on disability, and the increased healthcare expenditures in disabled persons, the economic burden of sarcopenia is presumed to be great. Nevertheless, even though the economic costs of illnesses play an important role in health policy,16there is a worldwide absence of reports that seek to
quantify the effect of sarcopenia on the use of health services. Thus, the primary objective of this study was to estimate the healthcare costs of sarcopenia in the United States. Because sarcopenia is a potentially avoidable and reversible condition, a secondary objective was to examine the effect that reduced sarcopenia prevalence would have on healthcare expenditures.
Research supported by the U.S. Department of Agriculture under Agreement 58-1950-9-001 and Contract 53-K06-1. I. Dr. Janssen is supported by a Canadian Institutes of Health Research Postdoctoral Fellowship. Any opinions or recommendations expressed in this publication are those of the authors and do not necessarily reflect the view of the U.S. Department of Agriculture.
Address correspondence to Ian Janssen, PhD, Department of Community Health and Epidemiology, Abramsky Hall, Queen’s University, Kingston, Ontario, Canada, K7L 3N6. E-mail: [email protected]
From theNutrition, Exercise Physiology, and Sarcopenia Laboratory, Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University, Boston, Massachusetts;wDepartment of Community Health and Epidemiology andzSchool of Physical and Health Education, Queen’s University, Kingston, Ontario, Canada;§Schneider Institute for Health Policy, Heller School for Social Policy and Management, Brandeis University, Waltham, Massachusetts.
JAGS 52:80–85, 2004
METHODS
The only condition that is known to be related to sarcopenia and that is associated with significant healthcare costs is physical disability (e.g., requiring help with personal care needs, such as bathing and dressing, or requiring help with routine needs, such as performing household chores and getting around). Thus, the healthcare costs associated with sarcopenia were estimated based on the effect of sarcopenia on increasing the risk of physical disability in older persons. To estimate the proportion of senescence-related disability that could theoretically be prevented in the United States if sarcopenia were eliminated, population-attributable risk (PAR) was calculated. PAR is an estimate of the effects of an individual risk factor on a given disease or conditionFthe proportion of the disease or condition due to the risk factor in question. The PAR for disability was calculated as
ðPðRR1ÞÞ=ð1þPðRR1ÞÞ
where P is the prevalence of sarcopenia in the population and RR is the relative risk of disability in a sarcopenic individual. The prevalence of sarcopenia in the United States and the RR of disability in sarcopenic individuals has previously been calculated using data from the Third National Health and Nutrition Examination Survey (NHANES III).7NHANES III is a nationally representative
cross-sectional survey that was conducted from 1988 through 1994.17 According to the results from NHANES
III, the prevalence of older (Z60) men at increased risk for
disability because of moderate (skeletal muscle index (SMI)58.75–10.74 kg/m2) and severe (SMIr8.74kg/m2)
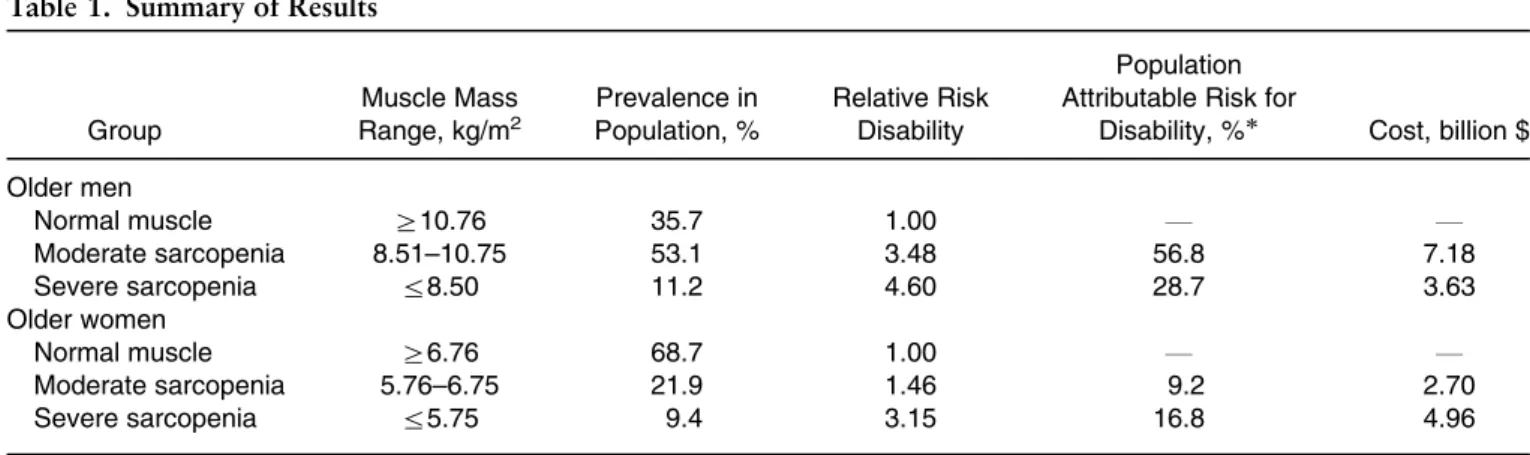
sarcopenia are 53.1% and 11.2%, respectively (Table 1). The corresponding RRs for disability in men with moderate and severe sarcopenia are 3.48 and 4.60, respectively. The prevalences of older women at increased risk for disability in NHANES III because of moderate (SMI55.75–6.74 kg/ m2) and severe (SMIr5.74 kg/m2) sarcopenia are 21.9%
and 9.4%, respectively. The corresponding RRs for disability in women with moderate and severe sarcopenia are 1.46 and 3.15, respectively.7Within each sex, the PAR
was calculated separately for moderate and severe sarco-penia, and the total PAR was determined by adding the PAR for the two levels of sarcopenia.18
Economic Costs of Sarcopenia
To estimate the economic burden of disability in older Americans, data from two national surveys, NHANES III17
and the National Medical Care Utilization and Expendi-tures Survey (NMCUES) were used.19 One study4
pre-viously calculated medical expenditures according to disability classification in older adults (Z65) using the
NMCUES data set. Using the NHANES III data set, it was determined that the prevalence of disability in older adults is 17.2%,17 which is similar to the disability prevalence
rates (B20%) for older Americans that was recently published.10
The definition of physical disability was slightly different in the NMCUES and NHANES III studies. In the NMCUES survey, disability was defined as the number of chronic conditions limiting work or keeping house,4
whereas in the NHANES III survey, disability was defined as requiring help with personal care (eating, bathing, dressing) or routine needs (performing household chores, doing necessary business, shopping).17 The RR for
dis-ability in sarcopenic individuals and prevalences of sarcopenia (see previous paragraph and Table 1) were calculated based on the NHANES III definition of disability. Because information from the NHANES III and NMCUES surveys had to be combined to estimate the cost of disability in older Americans, a consistent score for disability in the two studies was determined. First, temporal changes in the prevalence of disability from when NMCUES was conducted (1980) to when NHANES III was conducted (1988–94) were adjusted for. To do so, data from a study11 that reported a 12.6% reduction in the
prevalence of age-related disability (activities and instru-mental activities of daily living) in the United States over a similar time frame (1982–95) were used. It was then determined that a disability prevalence of 19.4% (17.2% adjusted to 1980 value) in the older adults in NHANES III corresponded to a disability score (number of chronic conditions) of 1.57 or greater in the older adults in NMCUES. This was determined by regressing the disability score against the number of subjects with each disability score in NMCUES. Taking into consideration the distribu-tion of subjects along the disability spectrum in the NMCUES survey, it was determined that the average disabled person in NHANES III would have a disability
Table 1. Summary of Results
Group Muscle Mass Range, kg/m2 Prevalence in Population, % Relative Risk Disability Population Attributable Risk for
Disability, % Cost, billion $ Older men Normal muscle Z10.76 35.7 1.00 F F Moderate sarcopenia 8.51–10.75 53.1 3.48 56.8 7.18 Severe sarcopenia r8.50 11.2 4.60 28.7 3.63 Older women Normal muscle Z6.76 68.7 1.00 F F Moderate sarcopenia 5.76–6.75 21.9 1.46 9.2 2.70 Severe sarcopenia r5.75 9.4 3.15 16.8 4.96 [prevalence (RR1)]/[11prevalence (RR1)].
score of 1.67 in NMCUES. By regressing the disability score against healthcare expenditures, it was calculated that the theoretical excess medical expenditures (e.g., medical expenditures above that of a person with no disabling conditions) for an older person in NMCUES with a disability score of 1.67 was $6,395 per year. This value, which was calculated based on data obtained for indivi-duals aged 65 and older, was adjusted to represent all individuals aged 60 and older, based on the percentage (25.4%) of the American population aged 60 and older who fit within the 60 to 64 age bracket in 200020and the medical
costs associated with disability in persons aged 60 to 64. The medical expenditures associated with a disability score of 1.67 for persons aged 60 to 64 in the NMCUES survey was determined by regressing age (Z45) against healthcare
expenditures. Based on this information, the excess healthcare expenditure in the average disabled American aged 60 and older was estimated at $6,212 per year. All 1980 values have been converted to 2000 values using the medical component of the consumer price index.21 The
value of $6,212 per year is comparable with that previously published in another study.15 In a sample of 843 older
(Z72) adults from Connecticut, that study determined that
disabled individuals accounted for $6,628 more per year (adjusted to 2000 dollars) in healthcare spending than nondisabled individuals.
The number of older Americans with disability was multiplied by $6,212 to estimate the yearly healthcare cost of disability in older Americans. Using the NHANES III data set, it was determined that 10.4% of older (Z60) men
and 18.1% of older women are disabled.17In 2000, there
were 19,546,252 American men and 26,250,948 American women aged 60 and older.20Taken together, these results
indicate that 2,032,810 older American men and 4,751,422 older American women were disabled in 2000. Thus, given that each individual with disability had an excess healthcare expenditure of $6,212/y, the estimated healthcare costs associated with disability in 2000 were $12.6 billion in older men and $29.5 billion in older women. The healthcare cost of sarcopenia was subsequently determined within each sex by multiplying the PAR by the economic cost of disability.
To determine the influence of variations in the PAR and disability costs on the sarcopenia healthcare costs, a two-way sensitivity analysis similar to that previously used was performed to determine the healthcare costs of obesity22
and physical inactivity.23PAR and disability healthcare cost
were simultaneous varied by720%.
Savings from Reduction in Sarcopenia
Because it would be unrealistic to expect an individual with severe sarcopenia to move all the way to the normal muscle category, the 10% reduced sarcopenia prevalence rates were calculated based on the assumption that those moving out of the severe sarcopenia category moved into the moderate sarcopenia category and not into the normal muscle category. Healthcare savings associated with a 10% reduction or improvement in the prevalence of sarcopenia were estimated by recalculating the PARs, assuming the prevalence of severe sarcopenia in older men to be 10.1% (11.2%1.12%), the prevalence of moderate sarcopenia
in older men to be 48.9% (53.1%5.31%11.12%), the prevalence of severe sarcopenia in older women to be 8.5% (9.4%0.94%), and the prevalence of moderate sarcope-nia in older women to be 20.6% (21.9%2.19%
10.94%). The savings were then calculated by taking the difference between the costs derived using the actual and theoretical (e.g., 10% reduced) sarcopenia prevalence rates.
RESULTS
The PAR for disability in older men due to sarcopenia (moderate1severe) was 85.6% (Table 1). The PAR for disability due to sarcopenia (moderate1severe) in older women was 26.0%. This suggests that, if sarcopenia were completely eliminated, 85.6% of the disability cases in older men and 26.0% of the disability cases in older women would be eliminated.
The estimated direct healthcare cost attributable to sarcopenia in the United States in 2000 was $18.5 billion ($10.8 billion in men, $7.7 billion in women). The sensitivity analysis indicated that the healthcare costs attributable to sarcopenia might be as low as $11.8 billion and as high as $26.2 billion. The distribution of the healthcare costs by degree of sarcopenia (moderate or severe) and sex are shown in Table 1. The excess healthcare expenditures were $860 for every sarcopenic man and $933 for every sarcopenic woman. Because the national health-care expenditure for 2000 was $1,299 billion,24sarcopenia
represented about 1.5% of total healthcare expenditures in the United States.
Recalculating the healthcare costs with a 10% reduc-tion in the prevalence of sarcopenia yielded a cost of $17.4 billion. Thus, a 10% reduction in sarcopenia prevalence would result in savings of $1.1 billion (2000 dollars) per year in U.S. healthcare costs. Almost half (46.6%) of this savings would occur if 10% of the population with severe sarcopenia moved into the moderate sarcopenia category; the remaining 54.4% of the savings would occur if 10% of the population with moderate sarcopenia moved into the normal muscle category.
DISCUSSION
The economic burden of sarcopenia in the United States was estimated using prevalence-based cost-of-illness methods and data from national surveys. The results indicate that $18.5 billion ($10.8 billion in men, $7.7 billion in women), or about 1.5% of total direct healthcare costs in the United States in 2000, were attributable to sarcopenia. Reducing the prevalence of sarcopenia by 10% would result in savings of $1.1 billion per year in U.S. healthcare costs. These findings confirm that sarcopenia is a significant public health problem, and one that imposes a significant burden on the U.S. economy.
In a public health context, the finding that sarcopenia accounted for $18.5 billion in direct healthcare costs in 2000 is important. To put this in perspective, it has been estimated that the yearly economic costs of osteoporotic fractures in the United States is $16.3 billion (adjusted to 2000 dollars).25Given the extent of the economic burden
numerous public health campaigns aimed at reducing the occurrence of this disease. However, although sarcopenia accounts for a similar percentage of healthcare costs as osteoporosis, no public health campaigns are directly aimed at reducing the prevalence of sarcopenia.
These estimates suggest that, if the prevalence of moderate and severe sarcopenia were reduced by 10%, it would result in savings of $1.1 billion per year in U.S. healthcare costs. Thus, even a modest reduction in the prevalence of sarcopenia in older persons would bring about marked healthcare savings when compiled over a number of years. These costs reflect the loss of skeletal muscle mass that occurs with advancing age and could theoretically be avoided if individuals maintained a healthy skeletal muscle mass throughout the lifespan. The authors recommend that older men strive to maintain a skeletal muscle mass relative to body height above 10.75 kg/m2and
that older women strive to maintain a skeletal muscle mass relative to body height above 6.75 kg/m2. Muscle values
below these cutpoints are associated with increased risk of disability.7
An initial treatment that may reduce the normal progression of sarcopenia in older persons is to ensure that they are eating enough protein. Approximately 35% of the older population eats less than the current recommended dietary intake (RDI) for protein (0.8 g of proteinkg–1
day–1), and about 15% eat less than 75% of this amount.26
One study reported that eating about half of the RDI for protein over a 9-week period led to significant reductions in lean body mass in elderly women, whereas elderly women who consumed the RDI for protein maintained lean body mass.27However, it is not known whether modest
reduc-tions in dietary protein (e.g., 10–15% below RDI) contribute to sarcopenia or whether increasing protein intake levels to 100% of the RDI would result in an increase in muscle mass in sarcopenic individuals.
Physical activity also holds great promise as a strategy for preventing and treating sarcopenia. Physically active older persons, particularly those who perform regular resistance exercise, have larger muscles than their sedentary counterparts.28,29Furthermore, it is well documented that
strength training can increase muscle mass and strength in previously sedentary elderly men and women, independent of disease status and functional ability.30–33For example, a
group of researchers31 observed a 9% increase in muscle
size after only 8 weeks of resistance training in the frail elderly. Because the age-related reduction in skeletal muscle begins in the fifth decade of life,2,3persons older than this
should be encouraged to perform resistance exercise to help alleviate the normal reduction in muscle mass that occurs with advancing age. The American College of Sports Medicine recommends that older adults perform one to three sets of 10 to 15 repetitions for each of the major muscle groups (B8 exercises) three times per week.32This
can be accomplished in anywhere from 1 to 3 hours per week.
Although the cost-effectiveness of resistance exercise as a treatment for sarcopenia is unclear, the hypertrophic effects of resistance training occur quickly,30–33and most
exercise interventions are relatively inexpensive. Lifestyle exercise programs (home-based exercise and lifestyle counseling) cost about $200 per person per year, not
including the cost of exercise equipment, and structured exercise programs (gym-based exercise and exercise coun-seling) cost about $600 per person per year.34 By
comparison, the analysis in this study revealed that sarcopenic individuals incurred about an extra $900 per year in healthcare expenditures. Thus, at the individual level, the healthcare costs of sarcopenia are greater than those of exercise participation, but additional research is needed to determine the cost-effectiveness of exercise interventions. A complete cost-benefit analyses would require valuing all economic inputs and outcomes to determine whether a net benefit of exercise is realized. Other inputs would include, for example, personal time and expenses (e.g., purchasing athletic clothing). Other out-comes would include, for example, the influence that exercise has on decreasing the healthcare costs of other diseases including cardiovascular disease, type II diabetes mellitus, osteoporosis, and cancer.23,35
From a population perspective, it would take a considerable amount of time from the point at which money was invested in sarcopenia prevention and treatment to the point at which significant healthcare savings would be recognized. This lag can be explained by the fact that few older Americans perform resistance exercise on a regular basis (e.g., once per week or more).17,36Thus, campaigns
aimed at increasing the public’s awareness of incorporating resistance training as part of a well-rounded physical activity program would have to be developed and implemented before healthcare savings would occur. In addition, the feasibility of alternative programs such as dietary interventions and community-based exercise pro-grams should be explored. The low-resistance training participation rates suggest that current resistance training practices (e.g., home-based and gym-based programs) are not effective in older persons.
It is important to note that not everyone with sarcopenia is physically disabled, but depending on sex and the degree of sarcopenia (moderate or severe), the risk of disability is 1.5 to 4.6 times higher in older persons with sarcopenia than in older persons with normal muscle.7
Furthermore, the findings of this study indicate that the proportion of disability (PAR) due to sarcopenia was 85.6% in older men and 26.0% in older women. There are two possible explanations for why sarcopenia had a greater effect on disability in men than women. The first is that the prevalence of sarcopenia is greater in men than women (64.2% vs 31.3%).7The second is that the other
factors that contribute to disability (e.g., chronic disease) have a greater effect in women than men, consistent with the knowledge that the prevalence of disability is higher in women.6,9,10,11
The healthcare cost estimates only took into considera-tion the direct costs of sarcopenia, including hospital, outpatient, and home healthcare expenditures. No attempt was made to include the indirect costs of sarcopenia such as lost productivity. Furthermore, in addition to disability, sarcopenia may also have an effect on osteoporosis,37
obesity,38 and type II diabetes mellitus39,40 and their
associated healthcare costs. However, a lack of epidemio-logical studies documenting a relationship between sarco-penia and these diseases caused us to choose a more conservative approach for the current analysis. Finally, in
addition to economic costs, it is reasonable to assume that sarcopenic individuals have worse quality of life than do nonsarcopenic older persons and that sarcopenic indivi-duals and their families and friends encounter additional psychosocial problems.
The major limitation of this study was that the RRs for sarcopenia that were used to determine the PARs for disability were derived from cross-sectional analysis. The authors are unaware of prospective findings demonstrating a cause-and-effect relationship between sarcopenia and disability. However, muscular strength, which is in large measure determined by muscle mass,41 is predictive of
disability in longitudinal studies.42,43 Thus, a causal
relationship between sarcopenia and disability seems likely. Nonetheless, it is also probable that chronic disease of old age may lead to disability, which in turn would contribute to muscle wasting.
A second limitation of the analysis was that the stage of disability for each subject was not taken into consideration. Although there is no commonly accepted system for grading disability, healthcare costs increase with greater degrees of disability.4It was also not possible to examine the effect of
age on the relationship between disability and healthcare costs. It is possible that the cost of disability is higher in the oldest old (e.g.,Z85) than in the young old (e.g., 60–70).
However, to complete such an analysis would require estimates of the incidence of sarcopenia and disability and information on the costs of disability at each age for each sex. Another limitation was that the disability costs were derived from the NMCUES survey, which was conducted in 1980. The 1980 amounts were inflated to 2000 values using the medical component of the consumer price index, and it was therefore assumed that the relative contribution of disability to health expenditures did not change dramati-cally between 1980 and 2000.
In summary, it has been demonstrated that sarcopenia imposes a significant economic burden on government-reimbursed healthcare services in the United States. Because the number of older Americans is increasing, the economic costs of sarcopenia will escalate unless effective public health campaigns aimed at reducing the occurrence of sarcopenia are implemented. These are important observa-tions given that economic costs of illnesses play an important role in health policy decision-making.16
REFERENCES
1. Frontera WR, Hughes VA, Fielding RA et al. Aging of skeletal muscle: A 12-yr longitudinal study. J Appl Physiol 2000;88:1321–1326.
2. Janssen I, Heymsfield SB, Wang ZM et al. Skeletal muscle mass and distri-bution in 468 men and women aged 18–88 y. J Appl Physiol 2000;89:81–88. 3. Kehayias JJ, Fiatarone MA, Zhuang H et al. Total body potassium and body
fat: Relevance to aging. Am J Clin Nutr 1997;66:904–910.
4. Rice DP, LaPlante MP. Medical expenditures for disability and disabling comorbidity. Am J Public Health 1992;82:739–741.
5. Baumgartner RN, Koehler KM, Gallagher D et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998;147:755–763. 6. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass
(sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc 2002;50:889–896.
7. Janssen I, Baumgartner RN, Ross R et al. Skeletal muscle cutpoints associated with elevated disability risk in older men and women. Am J Epidemiol in press. 8. Melton LJ 3rd, Khosla S, Crowson CS et al. Epidemiology of sarcopenia. J Am
Geriatr Soc 2000;48:625–630.
9. Ostchega Y, Harris TB, Hirsch R et al. The prevalence of functional limitations and disability in older persons in the U.S. data from the National Health and Nutrition Examination Survey III. J Am Geriatr Soc 2000;48:1132–1135. 10. Manton KG, Gu X. Changes in the prevalence of chronic disability in the
United States black and nonblack population above age 65 from 1982 to 1999. Proc Natl Acad Sci U S A 2001;98:6354–6359.
11. Manton KG, Corder L, Stallard E. Chronic disability trends in elderly United States populations, 1982–94. Proc Natl Acad Sci U S A 1997;94:2593–2598. 12. Wolinsky FD, Callahan CM, Fitzgerald JF et al. The risk of nursing home placement and subsequent death among older adults. J Gerontol 1992;47: S173–S182.
13. Branch LG, Wetle TT, Scherr PA et al. A prospective study of incident comprehensive medical home care use among the elderly. Am J Public Health 1988;78:255–259.
14. Ferrucci L, Guralnik JM, Pahor M et al. Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled. JAMA 1997;277:728–734.
15. Fried TR, Bradley EH, Williams CS et al. Functional disability and health care expenditures for older persons. Arch Intern Med 2001;161:2602–2607. 16. Rice DP, Hodgson TA, Kopstein AN. The economic costs of illness: A
replication and update. Health Care Financ Rev 1985;7:61–80.
17. U.S. Department of Health and Human Services, National Center for Health Statistics. NHANES III Reference Manuals and Reports (CD-ROM). Hyattsville, MD: Centers for Disease Control and Prevention, 1996. 18. Powell KE, Blair SN. The public health burdens of sedentary living habits:
Theoretical but realistic estimates. Med Sci Sports Exerc 1994;26:851–856. 19. Bonham GS Procedures and Questionnaires of the National Medical Care
Utilization and Expenditure Survey. Washington, DC: U.S. Government Printing Office, 1983.
20. U.S. Census Bureau. U.S. Summary 2000FCensus 2002 Profile. Washington, DC: U.S. Census Bureau, 2002.
21. U.S. Department of Labor, Bureau of Labor Statistics. CPI Detailed Report. Washington, DC: Labor Department, Labor Statistics Bureau, Office of Prices and Working Conditions, 2002.
22. Birmingham CL, Muller JL, Palepu A et al. The cost of obesity in Canada. Can Med Assoc J 1999;160:483–488.
23. Katzmarzyk PT, Gledhill N, Shephard RJ. The economic burden of physical inactivity in Canada. Can Med Assoc J 2000;163:1435–1440.
24. Levit K, Smith C, Cowan C et al. Trends in U.S. health care spending, 2001. Health Aff (Millwood) 2003;22:154–164.
25. Ray NF, Chan JK, Thamer M et al. Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995. Report from the National Osteoporosis Foundation. J Bone Miner Res 1997;12:24–35.
26. Roubenoff R, Hughes VA. Sarcopenia. Current concepts. J Gerontol A Biol Sci Med Sci 2000;55A:M716–M724.
27. Castaneda C, Charnley JM, Evans WJ et al. Elderly women accommodate to a low-protein diet with losses of body cell mass, muscle function, and immune response. Am J Clin Nutr 1995;62:30–39.
28. Melichna J, Zauner CW, Havlickova L et al. Morphologic differences in skeletal muscle with age in normally active human males and their well-trained counterparts. Hum Biol 1990;62:205–220.
29. Klitgaard H, Mantoni M, Schiaffino S et al. Function, morphology and protein expression of ageing skeletal muscle: A cross-sectional study of elderly men with different training backgrounds. Acta Physiol Scand 1990;140:41–54. 30. Hurley BF, Redmond RA, Pratley RE et al. Effects of strength training on
muscle hypertrophy and muscle cell disruption in older men. Int J Sports Med 1995;16:378–384.
31. Fiatarone MA, Marks EC, Ryan ND et al. High-intensity strength training in nonagenarians. JAMA 1990;263:3029–3034.
32. American College of Sports Medicine Position Stand. The recommended quality and quality of exercise for developing and maintaining cardiorespira-tory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc 1998;30:975–991.
33. Frontera WR, Meredith CN, O’Reilly KP et al. Strength conditioning in older men. Skeletal muscle hypertrophy and improved function. J Appl Physiol 1988;64:1038–1044.
34. Sevick MA, Dunn AL, Morrow MS et al. Cost-effectiveness of lifestyle and structured exercise interventions in sedentary adults. Results of Project ACTIVE. Am J Prev Med 2000;19:1–8.
35. Colditz GA. Economic costs of obesity and inactivity. Med Sci Sports Exerc 1999;31:S663–S667.
36. Adams PF, Benson V. Current estimates from the National Health Interview Survey. Vital Health Stat 10 1990;October:1–221.
37. Gillette-Guyonnet S, Nourhashemi F, Lauque S et al. Body composition and osteoporosis in elderly women. Gerontology 2000;46:189–193.
38. Baumgartner RN. Body composition in healthy aging. Ann N Y Acad Sci 2000;904:437–448.
39. Castaneda C, Bermudez OI, Tucker KL. Protein nutritional status and function are associated with type 2 diabetes in Hispanic elders. Am J Clin Nutr 2000;72:89–95.
40. Gougeon R, Pencharz PB, Sigal RJ. Effect of glycemic control on the kinetics of whole-body protein metabolism in obese subjects with non-insulin-dependent diabetes mellitus during iso- and hypoenergetic feeding. Am J Clin Nutr 1997;65:861–870.
41. Newman AB, Haggerty CL, Goodpaster B et al. Strength and muscle quality in a well-functioning cohort of older adults: The Health, Aging and Body Composition Study. J Am Geriatr Soc 2003;51:323–330.
42. Rantanen T, Guralnik JM, Foley D et al. Midlife hand grip strength as a predictor of old age disability. JAMA 1999;281:558–560.
43. Rantanen T, Guralnik JM, Ferrucci L et al. Coimpairments as predictors of severe walking disability in older women. J Am Geriatr Soc 2001;49:21–27.