ANNALS OF CLINICAL PSYCHIATRY 2012;24(4):255-260
RESEARCH ARTICLE
BACKGROUND: Borderline personality disorder (BPD) is a significant
psy-chiatric illness for which medication treatments are still being explored. The goal of this study was to assess divalproex extended release (ER) vs placebo for patients receiving dialectal behavior therapy (DBT).
METHODS: Patients with BPD received 4 weeks of “condensed DBT.” Those with Symptom Checklist-90 (SCL-90) scores >150 after this treatment were then randomly and blindly assigned to placebo or divalproex ER for 12 weeks. Repeated measures analysis of variance utilizing last observation carried forward was used to assess the results.
RESULTS: Seventeen participants completed the full assessment. Two patients had a significant decrease in SCL-90 in the first 4 weeks, leaving 15 patients for the medication phase of the trial. There were no signifi-cant differences between the participants assigned to divalproex ER com-pared with placebo. However, there was a significant improvement in both groups from baseline to endpoint (P = .001).
CONCLUSIONS: The response of 2 of 17 participants in the first 4 weeks prior
to medication may point to a practice strategy in approaching outpatients with BPD. Although the patients had a decrease in symptoms during the study, there was no advantage observed for divalproex ER and DBT over placebo and DBT.
KEYWORDS: borderline personality disorder, divalproex ER, dialectical
behavior therapy
Richelle Moen, PhD
Department of Psychiatry
University of Minnesota Medical School Minneapolis, MN, USA
Mary Freitag, PsyD
Integrative Psychological Services St. Paul, MN, USA
Michael Miller, PsyD Susanne Lee, PhD Ann Romine, BA, RN Sue Song, MA Adit Adityanjee, MD S. Charles Schulz, MD
Department of Psychiatry
University of Minnesota Medical School Minneapolis, MN, USA
Efficacy of extended-release divalproex
combined with “condensed” dialectical
behavior therapy for individuals with
borderline personality disorder
CORRESPONDENCE
S. Charles Schulz, MD Department of Psychiatry
University of Minnesota Medical School F282/2A West
2450 Riverside Avenue Minneapolis, MN 55454 USA
INTRODUCTION
Borderline personality disorder (BPD) is a common, chronic, and disabling disease that affects an estimated 1% to 2% of the general population1 and has an 8% to 10%
mortality rate.2 The prevalence of BPD found in outpatient
psychiatric clinics is 10%, although estimates suggest that as many as 20% of all psychiatric inpatient admissions meet full BPD criteria. BPD is twice as common in females vs males. Few patient groups require more mental health resources than BPD patients. BPD is known to be difficult to treat and treatment recommendations vary.3
BPD is characterized by instability in interpersonal relationships, self-image, and affect; high emotional reac-tivity with difficulty returning to baseline; chronic feelings of emptiness; dissociative experiences; and marked impul-sivity. Patients also experience impulsive risk-taking behav-ior, inappropriate/intense anger, self-injurious behavbehav-ior, multiple suicide attempts, and brief psychotic episodes.
Medication approaches to BPD have been tested in numerous studies over the last 25 years. Studies have examined a number of different compounds ranging from low doses of conventional4,5 and atypical
antipsy-chotic medications6-9 to selective serotonin reuptake
inhibitors.10,11 Based on observations that BPD patients
frequently have symptoms of impulsivity and/or aggres-sion or that they may be comorbid with mood disorders such as bipolar II disorder, a number of studies have investigated divalproex as a treatment for BPD.12,13
To date, Townsend et al14 reported reduction in
rat-ing scale scores, but not statistically significant differ-ences from placebo in the first controlled trial of dival-proex. Frankenburg and Zanarini12 examined divalproex
in BPD patients who also met criteria for bipolar II disor-der. They reported a significantly better outcome for the divalproex group on hostility scales. To refine the speci-ficity of patients who may have the best response to dival-proex, Hollander et al15 studied the outcome of cluster
B (impulsive and aggressive) behaviors in BPD patients, noting the superiority of divalproex in aggressive patients. Finally, to explore the potential of a new preparation of divalproex—1 with extended release (ER)—Simeon et al16
reported reduction in symptoms following administra-tion of divalproex ER in an open-label trial. Of note, the design of previous divalproex studies tended to focus attention on the impulsive-aggressive BPD patients.
Both divalproex and divalproex ER have shown significant potential for patients with BPD. Some of the
recent review articles have critically assessed the efficacy data for both divalproex and divalproex ER.17-19 However,
next steps would be informative if they addressed issues of psychosocial treatment and placebo response.20,21 For
example, Schulz et al22 noted a significant reduction in
scores of BPD patients assigned to risperidone that was equal to the placebo response, thus indicating the impor-tance of understanding psychosocial circumsimpor-tances of patients in medication trials.
Psychotherapeutic strategies are important for treat-ing personality disorders. Dialectical behavior therapy (DBT) has been proven to be effective in BPD treatment in controlled studies.23,24 Medication and psychosocial
com-binations have only recently begun to be explored with this population. In a 12-week, combined placebo-controlled trial of fluoxetine plus DBT vs placebo plus DBT, Simpson et al25 found no significant differences in outcome
mea-sures between the 2 groups. On the other hand, Soler et al21 found significant advantages for DBT plus
olanzap-ine compared with DBT plus placebo in decreasing both depressive symptoms and impulsivity/aggressive behav-iors in BPD patients. Linehan et al20 found a more rapid
reduction of irritability and aggression with DBT plus olanzapine than with DBT plus placebo, and both groups exhibited large and consistent reductions in aggression, depression, irritability, and self-injury.
Therefore, a double-blind, placebo-controlled pilot trial was designed to address the usefulness of divalproex ER in BPD patients in the context of short-term DBT treatment. In order to address the frequently observed rapid response of some patients during the initial phase of the clinical trial, all participants received “condensed” DBT for 4 weeks, and only those with significant symptoms were randomly assigned to blinded divalproex ER or placebo while continu-ing DBT. Therefore, the study addressed the issue of rapid response of patients at study entry as well as usefulness of divalproex ER in BPD patients undergoing DBT treatment.
METHODS
Participants
Recruitment of women and men age 21 to 55 who were disturbed by moodiness, distrustfulness, impulsivity, and painful and difficult relationships was accomplished primarily through newspaper and radio advertisements in the Minneapolis area. Local psychiatric clinics and men-tal health centers also were notified of the study, although
no clinical referrals were made. Participants were initially screened by telephone questionnaire using the 9 DSM-IV criteria for diagnosis of BPD.3 Potential participants were
excluded if they had a current or past history of bipolar disorder, schizophrenia, or major depression with psy-chotic features; were currently prescribed any psychotro-pic medication; or were acutely suicidal (ie, had a clear-cut and pressing intent to commit suicide in the near future). Although current diagnosis of major depression was an exclusion criterion, a history of major depression was allowed provided it had been 12 weeks since the last major depressive episode. No current alcohol or illicit substance dependency; a seizure disorder and/or anticonvulsant medications; or pregnancy were allowed. Women of child-bearing potential were given a pregnancy test at the begin-ning of the study. Women who were pregnant, breast- feeding, planning to become pregnant, or not using a reli-able form of contraception also were excluded.
After the initial phone screen, patients were invited to participate in a face-to-face assessment screening inter-view. At that time, written informed consent, which was approved by the University of Minnesota institutional review board, was obtained. The following semi-structured diagnostic interview and symptom screening instruments were administered to each participant: 1) the Structured Clinical Interview for DSM-IV Axis I Disorders26; 2) the
Structured Clinical Interview for DSM-IV Axis II Disorder (SCID-II)27 (along with past clinical records to screen for
other mental illnesses); and 3) the Symptom Checklist-90 (SCL-90).28 In order to be included in the study, all patients
had to have a score of >150 on the SCL-90 indicating a high severity of symptoms, and meet ≥5 criteria on the SCID-II. In order to participate in the study, each potential research patient had to be medication free for 2 to 4 weeks. A 4-week medication-free period was required for patients on long-acting depot medications.
Study design
In order to achieve the stated goals of the study, a 16-week, randomized, double-blind, placebo-controlled trial was designed. This controlled clinical trial consisted of a selection phase lasting 4 weeks and an experimen-tal phase lasting 12 weeks. All participants were given the psychosocial intervention of “condensed-DBT” for 4 weeks and then reassessed. The SCL-90 was given for the second time on week 4. Those scoring >150 were con-sidered nonresponders of “condensed-DBT” and were randomized to the double-blind (active drug vs placebo)
phase. These nonresponders to the condensed-DBT were randomly and blindly assigned to receive continued “condensed-DBT” plus either divalproex ER or placebo on a 2:1 ratio. All participants continued 12 more weeks of the “condensed-DBT” (total 16-week program).
The DBT skills training that was done in this study was based on the model of DBT for Adolescents, a “condensed” version of the skills, as modified by Alec Miller and Jill Rathus. This version allowed the participants to receive all 4 modules of skills in a 12-week period of time rather than the usual 26 weeks for adults.29 Slight modifications of
wording were needed to focus on “adult behaviors” vs ado-lescent and their parents’ references. Participants received the entire package of DBT, including all modes and func-tions of DBT, with weekly individual therapy sessions (45 to 50 minutes) incorporating the use of diary cards and behavioral chain analysis; skills training group (90 min-utes); and telephone coaching calls (as-needed basis). The contract and commitment to this DBT program was the 16 weeks (not the 6 months of group or 1 year of individual therapy as prescribed by the formal DBT model of ther-apy). All therapists were intensively trained in DBT and participated in a mandatory weekly consultation group.
After the screening and enrollment into the study, par-ticipants were assessed on the Hamilton Depression Rating Scale,30 the Borderline Evaluation of Severity over Time
(BEST),31 and the Barratt Impulsivity Scale (BIS).28,32 The
BEST is a measure designed specifically to assess patients with BPD. It allows the patient to rate the degree of impair-ment or interference from each of the 9 BPD criteria over the past week; each item is rated on a 5-point scale, and scores can range from 12 to 72. The BIS is a 20-item self-report measure with subscales measuring trait impulsivity. All participants received a physical examination, ECG, and laboratory testing (chemistry and hematology includ-ing comprehensive metabolic panel [renal and hepatic], complete blood count, thyroid-stimulating hormone, and urinalysis) to ascertain health status. Any medical illness thought to interfere with the study was cause for exclusion. Laboratory testing was performed at the same time as the divalproex ER blood level—at weeks 3, 6, 11, and 13 weeks after starting the study drug. The time of the last divalproex ER dose was documented, and divalproex ER levels were drawn approximately 24 hours after the last dose to assess relevant trough levels. All raters were kept blind of the serum divalproex level results. Only one study physician (A.A.), who did not participate in the ratings, was privy to the results of serum divalproex levels.
To study the possibility of medication side effects, all physical and psychiatric symptoms were recorded. Patients’ weight and height were measured at entry to double-blind study (to calculate body mass index) and at completion of the trial.
Divalproex ER dosing. Blood samples were
obtained to measure blood concentration of divalproex ER at weeks 4, 8, and 16. A study physician then adjusted the dose to maintain the medication at the therapeutic range. The study physician changed the dosing the study medicine and placebo at pre-determined dose-escala-tion steps so as not to reveal medicadose-escala-tion assignment.
Data analysis
Statistical analysis of data was conducted using SPSS v.16 (Chicago, IL, USA). Chi-square analyses and one-way analysis of variance (ANOVA) were used to com-pare demographic characteristics between the 2 groups. Repeated measures ANOVA using last observation carried forward (LOCF) data was used to test group differences in rate of change over time on the SCL-90 total score, the BIS-Motor Score, and the BEST total score. Non-parametric test (Kruskal-Wallis test) was applied to explore group differ-ences in the SCL-90 total score, the BIS-Motor Score, and the BEST total score at each timepoint. Non-parametric test was used for the exploratory analysis due to small sample size and high variability in scores. All statistical tests were 2-tailed with a significance of .05.
RESULTS
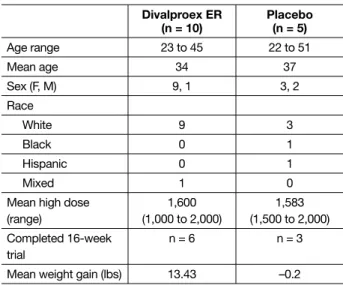
Twenty-nine participants completed the telephone inter-view after volunteering to be in the study and signed informed consent for the diagnostic and symptom rating assessment for study entry. Nine were “screen failures.” Of the 20 participants who were eligible to continue in the trial, 3 withdrew during the 4-week period of DBT before randomization in the medication trial, leaving 17 patients to go forward with the trial. Two of the participants’ SCL-90 scores were too low to meet criteria for randomization, but continued DBT. Fifteen participants were randomized to either divalproex ER or placebo (TABLE 1). In the divalproex
ER group, 6 out of 10 patients completed the study and 3 out of 5 assigned to placebo remained in the study until completion. Assessment of participation in the condensed DBT section of the study revealed that only 1 individual missed >2 of the 16 sessions.
TABLE 2 summarizes the means and standard
devia-tions on the SCL-90 total score; BIS-Motor Score; and the BEST parts A+B (Negative Thoughts, Feelings, and Behaviors) score. According to the repeated measures ANOVA on the group difference in outcomes measured over time, there was no significant Time × Group inter-action (slope) as assessed by the SCL-90 total score [F(8,56) = 1.09; P = .38] or BIS-Motor Score [F(6,39) = 0.21;
P = .97]. Although no significant group differences were found in the slopes, there was a significant time effect on the SCL-90 overall score, which indicated that the 2 groups showed improvement over time [F(4,56) = 5.36;
P < .001]. The statistically significant improvement of all the participants in the study are consistent with the cur-rent findings of BPD patients having better outcomes33
(TABLE 2).
Because of small sample size and high variability in scores, we applied nonparametric tests (Kruskal-Wallis Test) to compare the 2 groups at each timepoint. There was no significant group difference in the SCL-90 overall score (screening χ2[2] = 4.42, P = .11; randomization χ2[2]
= 5.25, P = .07; week 4 χ2[2] = 4.44, P = .11; week 8 χ2[2] =
3.98, P = .14; week 12 χ2[2] 3.70, P = .16) or the BIS-Motor
Score (randomization χ2[2] = 1.87, P = .39; week 4 χ2[2] =
1.72, P = .42; week 8 χ2[2] = 1.90, P = .39; week 12 χ2[2] =
2.65, P = .27).
Several side effects were reported during the study. Patients receiving divalproex ER during the study noted weight gain, sedation, confusion, increased appetite, yawn-ing, vivid dreams, tremor, edema, and tinnitus. Patients on
TABLE 1
Demographic characteristics of divalproex ER, placebo, and non-randomized groups
Divalproex ER (n = 10) Placebo(n = 5) Age range 23 to 45 22 to 51 Mean age 34 37 Sex (F, M) 9, 1 3, 2 Race White 9 3 Black 0 1 Hispanic 0 1 Mixed 1 0
Mean high dose (range) 1,600 (1,000 to 2,000) 1,583 (1,500 to 2,000) Completed 16-week trial n = 6 n = 3
Mean weight gain (lbs) 13.43 –0.2
placebo also reported weight gain (although mean mea-sures of weight declined), insomnia, and headache.
Reasons for early withdrawal for the 4 divalproex ER participants were: increased liver enzymes, stopped attending and did not return calls, assessed as potential risk to others, and did not like group therapy. For the pla-cebo group, the reasons for early withdrawal were com-plaint of no change and a statement of stopping for per-sonal reasons.
DISCUSSION
Our primary goal with this study was to examine the safety and efficacy of divalproex ER while addressing the impact of the “placebo” effect and controlled psychoso-cial intervention. One of the most interesting findings within this study was the effectiveness of the 4-week “run-in” of condensed DBT, which allowed us to separate out potential placebo, and/or “early responders” who benefited from treatment without medications. Almost 12% (2 of 17) of our study patients improved with therapy alone. Our research design is unique in how it mirrors psychology practice (therapists and psychologists) in that the patient’s response to therapy determines the need for a referral for medication.
All patients improved over time, even though there were no significant differences between the 2 random-ized groups. These findings were consistent with earlier findings by Simpson et al,25 who reported that combined
DBT plus fluoxetine did not have an advantage over DBT plus placebo. On the other hand, our results are unlike recent studies by Linehan et al20 and Soler et al,21 in which
DBT plus olanzapine was found to be significantly supe-rior to DBT plus placebo for improving mood/anxiety symptoms and impulsive behavior.
Although the patients assigned to divalproex ER had a reduction in symptoms over the course of the study, similar to results seen in earlier studies, the change was not greater than that observed in the placebo group.
Limitations of the study
This study has several methodologic limitations. First, although intended as a pilot study of a new medication, the small sample size limited our statistical power to investigate significant treatment group differences as well as our ability to generalize from our sample. Regarding the issue of whether a larger sample could have led to a
significant difference between groups, it is of note that the placebo group had numerically greater response. In addition, only 6 patients in the divalproex ER- and 3 patients in the placebo-treated group completed the entire 12-week medication trial (a 60% completion rate). Because of the LOCF analysis, data of all participants were included in the report of the statistical outcome.
Because BPD is not a homogeneous population, stud-ies are needed to increase our understanding of subcate-gories of BPD patients, such as those who may benefit from briefer vs longer interventions or those with symptoms that may be more responsive to divalproex ER.15 For
exam-ple, a recent meta-analysis by Ingenhoven et al34 showed a
targeted effect of divalproex for aggression and agitation. This patient group was not selected for specific subtypes of behaviors. It should be noted that there was no difference between divalproex ER and placebo on the BIS.
Moreover, no life-event measure or scale was used to ascertain presence or absence and putative severity of a recent life crisis in the lives of study patients. The
self-TABLE 2
Means and standard deviations on SCL-90 total score, BIS-Motor Score, and BEST Parts A+B (Negative Thoughts, Feelings, and Behaviors) score Divalproex ER Placebo M SD M SD SCL-90 Total Score Baseline 156.1 33.6 193.8 41.0 Randomization 168.5 22.7 171.0 16.3 Week 4 148.6 61.5 137.2 74.5 Week 8 142.4 60.0 129.6 70.2 Week 12 137 60.9 114.2 79.8 BIS-Motor Score Randomization 26.1 8.1 20.6 6.5 Week 4 26.1 7.6 20.8 6.5 Week 8 26.4 10.2 19.6 6.7 Week 12 23.9 10.3 18.2 6.4
BEST A+B Score
Randomization 33.7 8.9 41.3 5.1
Week 4 31.3 6.8 37.3 8.8
Week 8 31.1 7.7 31 11.2
Week 12 28.7 7.1 30 11.4
BEST: Borderline Evaluation of Severity over Time; BIS: Barratt Impulsivity Scale; ER: extended release; M: mean; SCL-90: Symptoms Checklist-90; SD: standard deviation.
referred research volunteers may have sought clinical help through the study participation following a life crisis leading to their recruitment in the study. Also, there may be some concern about the mean age of the research par-ticipants (mid-30s) and the need to study less persistently ill patients.
Lastly, it should be noted that the psychosocial treat-ment “condensed” DBT was chosen to match the length of time of the trial. However, this treatment has not been validated for adult patients with DBT. Therefore, a repli-cation of this approach is warranted.
CONCLUSIONS
In summary, divalproex has shown efficacy in some studies12-15 and the ER formulation was tested in this
pilot trial. In addition, other issues of concern in BPD trials were incorporated into the study, including the treatment with “condensed” DBT during the medica-tion trial and the exclusion of the rapidly responding patients prior to randomization. ■
DISCLOSURES: Dr. Schulz receives grant or research
sup-port from AstraZeneca, Myriad RBM, and Otsuka and is a consultant to Eli Lilly and Company and Genetech. Drs. Moen, Freitag, Miller, Lee, and Adityanjee and Ms. Romine and Ms. Song report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
ACKNOWLEDGEMENTS: This study was sponsored by a
research grant from Abbott Pharmaceuticals to the prin-cipal investigator, S. Charles Schulz, MD.
1. Torgersen S, Kringlen E, Cramer V. The prevalence of personality disorders in a community sample. Arch Gen Psychiatry. 2001;58:590-596.
2. Pompili M, Girardi P, Ruberto A, et al. Suicide in borderline personality disorder: a meta-analysis. Nord J Psychiatry. 2005;59:319-324.
3. Practice guideline for the treatment of patients with borderline personality disorder. American Psychiatric Association. Am J Psychiatry. 2001;158(10 suppl):1-52. 4. Goldberg SC, Schulz SC, Schulz PM, et al. Borderline and schizotypal personality disorders treated with low-dose thiothixene vs placebo. Arch Gen Psychiatry. 1986; 43:680-686.
5. Soloff PH, George A, Nathan RS, et al. Progress in pharmacotherapy of borderline disorders. A double-blind study of amitriptyline, haloperidol, and placebo. Arch Gen Psychiatry. 1986;43:691-697.
6. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with border-line personality disorder: a double-blind, placebo-con-trolled study. Am J Psychiatry. 2006;163:833-838. 7. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personal-ity disorder and comorbid dysthymia. Biol Psychiatry. 1999;46:1429-1435.
8. Schulz SC, Zanarini MC, Bateman A, et al. Olanzapine for the treatment of borderline personality disorder: vari-able dose 12-week randomised double-blind placebo-controlled study. Br J Psychiatry. 2008;193:485-492. 9. Adityanjee, Romine A, Brown E, et al. Quetiapine in patients with borderline personality disorder: an open-label trial. Ann Clin Psychiatry. 2008;20:219-226. 10. Coccaro EF, Kavoussi RJ. Fluoxetine and impulsive aggressive behavior in personality-disordered subjects. Arch Gen Psychiatry. 1997;54:1081-1088.
11. Markovitz PJ, Calabrese JR, Schulz SC, et al. Fluoxetine in the treatment of borderline and schizotypal personality disorders. Am J Psychiatry. 1991;148:1064-1067. 12. Frankenburg FR, Zanarini MC. Divalproex sodium treatment of women with borderline personality disor-der and bipolar II disordisor-der: a double-blind placebo-con-trolled pilot study. J Clin Psychiatry. 2002;63:442-446. 13. Hollander E, Allen A, Lopez RP, et al. A prelimi-nary double-blind, placebo-controlled trial of
dival-proex sodium in borderline personality disorder. J Clin Psychiatry. 2001;62:199-203.
14. Townsend MH, Cambre KM, Barbee JG. Treatment of borderline personality disorder with mood instabil-ity with divalproex sodium: series of ten cases. J Clin Psychopharmacol. 2001;21:249-251.
15. Hollander E, Swann AC, Coccaro EF, et al. Impact of trait impulsivity and state aggression on divalproex ver-sus placebo response in borderline personality disorder. Am J Psychiatry. 2005;162:621-624.
16. Simeon D, Baker B, Chaplin W, et al. An open-label trial of divalproex extended-release in the treat-ment of borderline personality disorder. CNS Spectr. 2007;12:439-443.
17. Bellino S, Paradiso E, Bogetto F. Efficacy and toler-ability of pharmacotherapies for borderline personality disorder. CNS Drugs. 2008;22:671-692.
18. Herpertz SC, Zanarini M, Schulz CS, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of personality disor-ders. World J Biol Psychiatry. 2007;8:212-244. 19. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane system-atic review of randomised trials. Br J Psychiatry. 2010; 196:4-12.
20. Linehan MM, McDavid JD, Brown MZ, et al. Olanzapine plus dialectical behavior therapy for women with high irritability who meet criteria for borderline personality disorder: a double-blind, placebo-con-trolled pilot study. J Clin Psychiatry. 2008;69:999-1005. 21. Soler J, Pascual JC, Campins J, et al. Double-blind, placebo-controlled study of dialectical behavior therapy plus olanzapine for borderline personality disorder. Am J Psychiatry. 2005;162:1221-1224.
22. Schulz SC, Camlin KL, Berry SA, et al. A double-blind, placebo-controlled study of risperidone for borderline personality disorder: a preliminary report. Presented at: 37th ACNP Annual Meeting; December, 14-18, 1998; San Juan, PR.
23. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63:757-766.
24. Robins CJ, Chapman AL. Dialectical behavior ther-apy: current status, recent developments, and future directions. J Pers Disord. 2004;18:73-89.
25. Simpson EB, Yen S, Costello E, et al. Combined dia-lectical behavior therapy and fluoxetine in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65:379-385.
26. First MB, Spitzer RL, Gibbon M, et al. Structured Clinical Interview for DSM-IV-TR Axis I Disorders. New York, NY: New York State Psychiatric Institute, Biometrics Research Department; 2001.
27. First MB, Spitzer RL, Gibbon M, et al. The Structured Clinical Interview for DSM-III-R Personality Disorders (SCID-II). Part II: multi-site test-retest reliability study. J Pers Disord. 1995;9:92-104.
28. Derogatis RL. The SCL-R-90 manual I: scoring, administration and procedures for the SCL-90. Baltimore, MD: Clinical Psychometric Research; 1977.
29. Miller AL, Rathus JH, Linehan MM, et al. Dialectical behavior therapy adapted for suicidal adolescents. Journal of Practical Psychiatry and Behavioral Health. 1997;3:78.
30. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56-62.
31. Pfohl B, Blum N, St John D, et al. Reliability and validity of the Borderline Evaluation of Severity Over Time (BEST): a self-rated scale to measure severity and change in persons with borderline personality disorder. J Pers Disord. 2009;23:281-293.
32. Barratt E, Patton JH. Impulsivity: cognitive, behav-ioral and psychophysiological correlates. In: Zuckerman M, ed. The biological basis of sensation seeking, impul-sivity, and anxiety. Hillsdale, NJ: Lawrence Earlbaum Associates; 1983:77-122.
33. Gunderson JG, Stout RL, McGlashan TH, et al. Ten-year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study. Arch Gen Psychiatry. 2011;68:827-837.
34. Ingenhoven T, Lafay P, Rinne T, et al. Effectiveness of pharmacotherapy for severe personality disorders: meta-analyses of randomized controlled trials. J Clin Psychiatry. 2010;71:14-25.