Disclaimer: The Rapid Response Service is an information service for those involved in planning and providing health care in Canada. Rapid responses are based on a limited literature search and are not comprehensive, systematic reviews. The intent is to provide a list of sources and a summary of the best evidence on the topic that CADTH could identify using all reasonable efforts within the time allowed. Rapid responses should be considered along with other types of information and health care considerations. The information included in this response is not intended to replace professional medical advice, nor should it be construed as a recommendation for or against the use of a particular health technology. Readers are also cautioned that a lack of good quality evidence does not necessarily mean a lack of effectiveness particularly in the case of new and emerging health technologies, for which little information can be found, but which may in future prove to be effective. While CADTH has taken care in the preparation of the report to ensure that its contents are accurate, complete and up to date, CADTH does not make any guarantee to that effect. CADTH is not liable for any loss or damages resulting from use of the information in the report.
Copyright: This report contains CADTH copyright material. It may be copied and used for non-commercial purposes, provided that attribution is given to CADTH.
TITLE: Day Programming for Post-Traumatic Stress Disorder: A Review of the Clinical Effectiveness, Cost-Effectiveness and Guidelines
DATE: 26 March 2012
CONTEXT AND POLICY ISSUES
Post-traumatic stress disorder (PTSD) is the recurring and intrusive recollection of an
overwhelming traumatic event.1 Individuals with PTSD relive the traumatic event in a variety of ways (e.g. memories, flashbacks, dreams), avoid stimuli associated with the event (e.g. places, people, thoughts, feelings, dissociation), and experience symptoms of increased arousal (e.g. difficulty sleeping, irritability, decreased concentration, hypervigilance).1,2 A recently published Canadian study based on a nationally representative sample of 3006 adults reported that the prevalence rates of lifetime PTSD range from 9.2% to 13.4% depending on the diagnostic criteria used, that major depressive disorder occurs concurrently in up to three-quarters of PTSD patients, and that substance and alcohol abuse are common in this population.3 The treatment of PTSD includes psychotherapy (e.g. exposure psychotherapy, supportive psychotherapy) and drug therapy.1 As with other mental health conditions, the provision of therapy for PTSD may occur in different settings (e.g. hospital or community) and in varying program intensities (e.g. inpatient/overnight, outpatient, day programs).4-6
Day programs for mental health conditions provide therapeutic support to individuals for several hours per day while they remain in the community, and may be administered through a hospital or a community-based clinic. In general, day programs may offer certain advantages over inpatient care including a less restrictive setting for patients, lower costs, and possibly similar outcomes.5 In comparison to outpatient care which typically has shorter session durations (e.g. one-hour psychotherapy) and may have fewer sessions over the same period of time, day programs may be more effective.6 However, these findings may differ by mental health condition.
The present review was conducted to assess the evidence for the relative clinical effectiveness and cost-effectiveness of day programming, specifically in PTSD. A search for evidence-based guidelines on the use of day programming in PTSD was also conducted with the aim of
RESEARCH QUESTIONS
1. What is the clinical effectiveness of day programming for post-traumatic stress disorder? 2. What is the cost effectiveness of day programming for post-traumatic stress disorder? 3. What are the evidence-based guidelines regarding the use of day programming for
post-traumatic stress disorder? KEY MESSAGE
A small number of studies of limited quality suggest that day programs may be effective in reducing PTSD symptoms and other psychiatric comorbidities, however the extent to which they are more or less effective than inpatient or residential and outpatient PTSD treatment programs is unclear. Cost-effectiveness evaluations of day programs and guidelines for their use were not identified. Randomized trials of day programs and their comparators are needed to address the question of their relative effectiveness in PTSD.
METHODS
Literature search strategy
A limited literature search was conducted on key resources including PubMed, PsycINFO, The Cochrane Library (2012, Issue 2), University of York Centre for Reviews and Dissemination (CRD) databases, Canadian and abbreviated list of major international health technology agencies, as well as a focused Internet search. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2002 and February 27, 2012.
Article Selection
Titles and abstracts of the retrieved citations were screened by one reviewer, and full-text publications of selected citations were examined and further screened for final inclusion based on the selection criteria provided in Table 1.
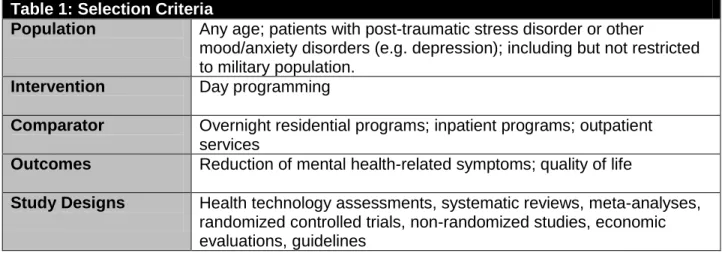
Table 1: Selection Criteria
Population Any age; patients with post-traumatic stress disorder or other
mood/anxiety disorders (e.g. depression); including but not restricted to military population.
Intervention Day programming
Comparator Overnight residential programs; inpatient programs; outpatient services
Outcomes Reduction of mental health-related symptoms; quality of life
Study Designs Health technology assessments, systematic reviews, meta-analyses, randomized controlled trials, non-randomized studies, economic evaluations, guidelines
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria in Table 1, or if they were published prior to January 2002.
Critical Appraisal of Individual Studies
The quality of the included randomized controlled trial and non-randomized studies was assessed using the Downs and Black7 checklist. Numeric scores were not calculated; instead the strengths and limitations of each study were described. No systematic reviews, economic evaluations, or evidence-based guidelines were identified for critical appraisal.
SUMMARY OF EVIDENCE Quantity of Research Available
A total of 224 citations were identified through the literature search, and an additional five reports were identified in the grey literature. Screening of the abstracts resulted in the selection of 25 potentially relevant reports (20 from the literature search, and 5 from the grey literature) for full-text review.
One randomized controlled trial,8 three non-randomized controlled studies,9-11 and one
uncontrolled study12 were included in the review. No health technology assessments, systematic reviews and meta-analyses, economic evaluations or guidelines providing recommendations specific to day programming were identified. Details of the study selection process are provided in the PRISMA flowchart in Appendix 1.
Summary of Study Characteristics Study design
Five studies are included in this review; one randomized controlled trial,8 three prospective non-randomized controlled studies9-11 and one prospective uncontrolled study.12 A detailed summary of the characteristics of the included studies is provided in Table A1 in Appendix 2.
Populations
Populations included patients with diagnosed PTSD. The randomized controlled trial8 included homeless individuals with concurrent cocaine addiction. Three studies included patients with combat-related PTSD10-12 and one study9 included traumatized asylum seekers and refugees. Interventions and comparators
The randomized controlled trial8 compared abstinence-contingent housing and vocational training both with and without behavioral day treatment. One non-randomized controlled study study10 compared five group-based programs of varying intensity (i.e. inpatient, residential, day program (2 programs), and weekly outpatient). A second non-randomized controlled study11 compared day hospital treatment with inpatient followed by outpatient care. A third non-randomized controlled study9 compared three trauma focus-group day treatment programs of
varying intensity with a supportive psychotherapy group and a waiting list control group. Finally, one study12 looked at the impact of a three-week day program and did not have a comparator. Outcomes
The main outcomes in the reviewed studies included PTSD symptom reduction,8-12 reduction in PTSD symptom severity,8 reduction in psychopathology9-12 (e.g. anxiety, depression,
psychoticism), reduction in substance use,10,11 anger,11 change in coping,8 general health11 and general quality of life.11
Summary of Critical Appraisal
The randomized study by Lester et al.8 did not appear to be originally designed to answer the research question, and the majority of the included patients did not have a diagnosis of current PTSD. Some baseline differences in patient characteristics were noted. The authors did not adjust for concurrent drug therapy, and a power calculation for adequate sample size was not reported. Because of the nature of the interventions, blinding is difficult if not unfeasible. All three non-randomized controlled studies9-11 were prospective and clearly described their outcomes. Treatment assignment may have been systematically biased in two reports.9,10 Baseline patient characteristics were not reported in all three reports however two studies10,11 reported baseline outcome values. Potential confounding was not accounted for in any of the three studies, particularly the potential impact of concurrent drug therapy, and sample sizes were unequally distributed in two of the studies, primarily due to biased allocation.9,10 The uncontrolled study12 had no comparator, the potential impact of concurrent drug therapy on the main outcomes was not considered, and the extent to which symptom reduction would have sustained beyond three weeks is unknown.
A detailed summary of individual study strengths and limitations is provided in Table A2 of Appendix 3.
Summary of Findings
The main findings and authors’ conclusion of the reviewed studies are given in Table A3 of Appendix 4.
What is the clinical effectiveness of day programming for post-traumatic stress disorder? Reduction in PTSD symptoms
A sub-analysis of an RCT8 compared the impact of two programs of abstinence-contingent housing and vocational training, with and without day programing, on PTSD symptoms as measured by the Post-Traumatic Diagnosis Scale (PDS) in homeless people with cocaine dependence and coexisting mental disorder. A multiple regression analysis on 90 of the 118 participating patients reported non-significant reductions in PTSD symptoms (B=-2.13, SE B=1.15, t-statistic=-1.85) and severity (B=-3.13, SE B=2.19, t-statistic=-1.43) with day program at 6 months. Significant predictors of symptoms and their severity at 6 months were baseline symptoms and coping measures including baseline negative avoidance, baseline positive distraction, and change in negative avoidance. The extent to which a change in coping skills could be attributed to the day treatment program was not clear in the reporting of the results.
Among the limitations of this study was that only 15% of patients met the DSM-IV criteria for current PTSD.
Three non-randomized controlled studies9-11 compared day programs with other interventions. A study from the Netherlands by Drozdek et al.9 compared three trauma-focus group treatment day programs of varying intensity (at one year) with weekly psychotherapy (at one year), and being on a six-month waiting list with medication, in asylum seekers and refugees. Significant reductions in PTSD symptoms as measured by the Harvard Trauma Questionnaire (HTQ) were seen in each of the day program groups, while no differences were seen in weekly
psychotherapy and waiting list groups. An Australian study of 4339 military personnel by Forbes et al.10 compared the impact of five programs of varying intensity [inpatient-outpatient for 12 weeks (high); residential for 12 weeks (high); metropolitan day hospital for 2-3 days/week and decreasing intensity after 4-6 weeks for up to twelve weeks (moderate); regional day hospital of the same intensity as the metropolitan day hospital (moderate); and weekly cognitive behavioral sessions for up to six months (low)]. PTSD symptoms were assessed at six and at 12 months using the PTSD Checklist (PCL). The authors reported significantly improved and comparable outcomes in PTSD symptoms across the five programs. Further analyses based on categories of severity of PTSD symptoms suggested that outcomes might be maximized by matching level of PTSD severity with program intensity. A second Australian study (Creamer et al.) of 202 male Vietnam veterans compared day programs with an inpatient-outpatient model, and measured PTSD symptoms using the PCL at nine months.11 The authors described the content of both programs as being the same. Results showed significant improvement in PTSD symptoms in both treatment groups over time for up to 9 months, however there were no significant between-group differences.
A single non-comparative study (Lande et al.) of a structured day-long three-week program in 39 military personnel reported a statistically significant reduction in PTSD symptoms as measured by the PCL at three weeks.12
Reduction in other mental health related symptoms
All three non-randomized controlled studies reported on changes in other mental health related symptoms.9-11 Drozdek et al.9 reported statistically significant reductions in anxiety, depression, and psychoticism in two of the more intensive of three day programs, and no significant
reduction of these symptoms in the weekly psychotherapy program or the 6-month waiting list with drug therapy. As was the case with PTSD symptoms, Forbes et al.10 reported comparable outcomes for depression, anxiety, and alcohol use in the five programs of varying treatment intensity that were studied. Creamer et al.11 found significant improvement in comorbidity (depression, anxiety, alcohol use) in both inpatient-outpatient and day programs over nine months, however there were no between-group differences. The non-comparative observational study by Lande et al.12 reported a statistically significant reduction in depression scores after a three-week day program.
Impact on quality of life
The study by Creamer et al.11 assessed health-related quality of life using the 12-item Short-Form Questionnaire (SF-12) and reported no significant differences between inpatient-outpatient and day programs in either the physical or mental component of the measure.
Limitations
The quantity and quality of evidence for the effectiveness of day programs in PTSD is limited. The variation in program content and treatment intensities and durations among interventions classified as day programs poses some challenges in the assessment of its effectiveness as a category versus other treatment programs. PTSD may also be treated with medication however the extent to which the patients in most of the reviewed studies were treated with concurrent medication, how medication use may have differed by treatment group, and the extent to which the observed effects in any program can be attributed to medication is unknown. One study9 noted in its discussion that the majority of its patients were prescribed psychotropic medications, however this medication was not strictly controlled. The reviewed studies used different
diagnostic criteria for PTSD (e.g. DSM-IV, CAPS), which would impact the types of patients included in the studies, as prevalence rates for PTSD have been shown to differ by diagnostic criteria used.3 The outcome measures used to evaluate PTSD symptoms varied across studies (e.g. PCL, HTQ, PCL), and may have had differing properties (e.g. responsiveness to change). The extent to which the day programs described in the reviewed studies are representative of the care available in Canadian settings is unclear. Studies assessing the cost-effectiveness of day programs compared with other treatment programs in PTSD were not identified, nor were guidelines for the use of day programs versus other treatment programs in this condition. CONCLUSIONS AND IMPLICATIONS FOR DECISION OR POLICY MAKING
The studies reviewed for this report suggest that day programs may be effective in reducing PTSD symptoms and other psychiatric comorbidities, however these studies all have noted methodological limitations. The extent to which day programs are more or less effective than inpatient or residential and outpatient PTSD treatment programs is unclear. Randomized studies of day programs and their comparators are needed to properly address this question, with relative program content and duration and intensity of therapy being important considerations.
PREPARED BY:
Canadian Agency for Drugs and Technologies in Health Tel: 1-866-898-8439
REFERENCES
1. Merck. The Merck Manual for Health Care Professionals [Internet]. Whitehouse Station (NJ): Merck; 2011. Stress disorders: acute stress disorder; 2007 [cited 2012 Mar 23]. Available from:
http://www.merckmanuals.com/professional/psychiatric_disorders/anxiety_disorders/stress _disorders.html?qt=stress
2. Diagnostic and statistical manual of mental disorders. 4th ed. text rev. Washington (DC): American Psychiatric Association; 2000.
3. Van Ameringen M, Mancini C, Patterson B. The impact of changing diagnostic criteria in posttraumatic stress disorder in a Canadian epidemiologic sample. J Clin Psychiatry. 2011 Aug;72(8):1034-41.
4. National Center for PTSD [Internet]. Washington (DC): U.S. Department of Veterans Affairs; 2012 Mar 19. PTSD treatment programs in the U.S. Department of Veterans Affairs; 2007 Jan 1 [cited 2012 Mar 13]. Available from:
http://www.ptsd.va.gov/public/pages/va-ptsd-treatment-programs.asp
5. Health Systems Research Unit, Clarke Institute of Psychiatry. Review of best practices in mental health reform [Internet]. Ottawa: Federal/Provincial/Territorial Advisory Network on Mental Health; 1997. [cited 2012 Mar 13]. Available from: http://www.phac-aspc.gc.ca/mh-sm/pubs/bp_review/pdf/e_bp-rev.pdf
6. Marshall M, Crowther R, Almaraz-Serrano A, Creed F, Sledge W, Kluiter H, et al. Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care. Health Technol Assess [Internet]. 2001 [cited 2012 Mar 13];5(21):1-75. Available from: http://www.hta.ac.uk/fullmono/mon521.pdf
7. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health [Internet]. 1998 Jun [cited 2012 Mar 23];52(6):377-84. Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1756728/pdf/v052p00377.pdf
8. Lester KM, Milby JB, Schumacher JE, Vuchinich R, Person S, Clay OJ. Impact of behavioral contingency management intervention on coping behaviors and PTSD
symptom reduction in cocaine-addicted homeless. J Trauma Stress. 2007 Aug;20(4):565-75.
9. Drozdek B, Bolwerk N. Evaluation of group therapy with traumatized asylum seekers and refugees--The Den Bosch Model. Traumatology [Internet]. 2010 [cited 2012 Mar
2];16(4):117-27. Available from: http://tmt.sagepub.com/content/16/4/117.full.pdf+html
10. Forbes D, Lewis V, Parslow R, Hawthorne G, Creamer M. Naturalistic comparison of models of programmatic interventions for combat-related post-traumatic stress disorder. Aust N Z J Psychiatry. 2008 Dec;42(12):1051-9.
11. Creamer M, Forbes D, Biddle D, Elliott P. Inpatient versus day hospital treatment for chronic, combat-related posttraumatic stress disorder: a naturalistic comparison. J Nerv Ment Dis. 2002 Mar;190(3):183-9.
12. Lande RG, Williams LB, Francis JL, Gragnani C, Morin ML. Characteristics and
effectiveness of an intensive military outpatient treatment program for PTSD. J Aggression Maltreat Trauma. 2011;20(5):530-8.
APPENDIX 1: Selection of Included Studies
204 citations excluded
20 potentially relevant articles retrieved for scrutiny (full text, if
available)
25 potentially relevant reports
5 reports included in review 224 citations identified from electronic literature search and
screened
5 potentially relevant reports identified from
grey literature
20 reports excluded: -irrelevant population (1) -irrelevant intervention (12) -other (wrong study design, guidance not provided)(7)
APPENDIX 2: Summary of Study Characteristics
Table A1: Characteristics of Included Studies
First author, Publication year, Country Study design, Length of follow-up Patient characteristics, Sample size (n)
Intervention Comparator(s) Main study
outcomes
Randomized Controlled Trial Lester8 2007, United States RCT, 6 months 90* homeless persons (gender not stated) with cocaine dependence and coexisting mental disorder not requiring immediate hospitalization. Patients with diagnosis of PTSD (15% of participants) was based on SCID for DSM-IV Abstinence-contingent housing (6 months), plus abstinence-contingent vocational training (6 months), plus behavioral day treatment (4 hours per day, 4 days per week for 1-2 months, individual and group therapy) with aftercare (3-6 months) Abstinence-contingent housing (6 months), plus abstinence-contingent vocational training (6 months) PDS (assesses DSM-IV post-traumatic stress disorder symptoms and severity in past 30 days), and 28-item COPE scale
Non-randomized Controlled Studies Drozdek9 2010, Netherlands Prospective, 6 months and/or one year (depending on program)
88 male and female asylum seekers and refugees diagnosed with PTSD based on DSM-IV, not previously treated for PTSD Three trauma-focus group treatment day programs of varying intensity (3 non-verbal therapy+2 psychotherapy sessions in 3 days/week; 3+2 sessions in 2 days/week; 2+2 sessions in 2 days per week), each following the Den-Bosch Phase-Oriented trauma treatment approach Psychotherapy one time per week, or 6-month waiting list with medication HTQ to evaluate post-traumatic damage; HSCL-25 and SCL-90 Psychoticism Scale to assess co-morbid psychiatric symptoms Forbes10 2008, Australia Prospective, 12 weeks to 6 months treatment (depending on program), 4339 male veterans diagnosed with PTSD based on CAPS. Concurrent conditions included substance abuse 2 day hospital programs (1 was regional) for 2-3 days per week for 4 to 6 weeks, followed Inpatient-outpatient program (12 weeks), residential program (12 PCL as a measure of PTSD;HADS for assessment of concurrent
Table A1: Characteristics of Included Studies First author, Publication year, Country Study design, Length of follow-up Patient characteristics, Sample size (n)
Intervention Comparator(s) Main study
outcomes outcomes measured at 6 months after program intake (36%), depression (39%), and anxiety disorder (11%). by less intensive phase for up to 12 weeks weeks), once-weekly outpatient program (6 months) anxiety and depression; AUDIT for assessment of alcohol use Creamer11 2002, Australia Prospective, 3 and 9 months 202 male Vietnam veterans diagnosed with PTSD based on CAPS. Average age: 51.2 (inpatient) and 52.3 (day program) years. Day program (details of program not provided, however content of treatment and comparator programs was the same) Inpatient-outpatient model PCL as a measure of PTSD; AUDIT for assessment of alcohol use; HADS for assessment of concurrent anxiety and depression; General Health Questionnaire (28-item version), and the SF-12 Health Survey to assess quality of life, anger (assessed using American VA evaluation protocols) Uncontrolled Study Lande12 2011, United States Prospective, 3 weeks
39 male and female military personnel aged 21 to 30 with PTSD diagnosis based on SCID and CAPS Structured day-long program that included individual counseling, group therapy, medication management, trauma recovery and crisis management skills focus groups, anger management focus groups No comparator PCL as a measure of PTSD; Zung Self-Rating Depression Scale
*This study was a subset of a larger study. 118 patients were used in the analysis of the COPE scale and 90 patients were used in the analysis of the PDS
AUDIT: Alcohol Use Disorders Identification Test; CAPS: Clinician-Administered PTSD Scale; COPE: Coping Orientations to Problems Experienced; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Version IV; HADS: Hospital Anxiety and Depression Scale; HSLC-25: Hopkins Symptoms Checklist; HTQ: Harvard Trauma Questionnaire; PCL: PTSD Checklist; PDS: Post-traumatic Diagnosis Scale; PTSD: Post-traumatic stress disorder; RCT: Randomized controlled trial; SCID: Structured Clinical Interview; VA: Veterans’ Affairs
APPENDIX 3: Summary of Critical Appraisal
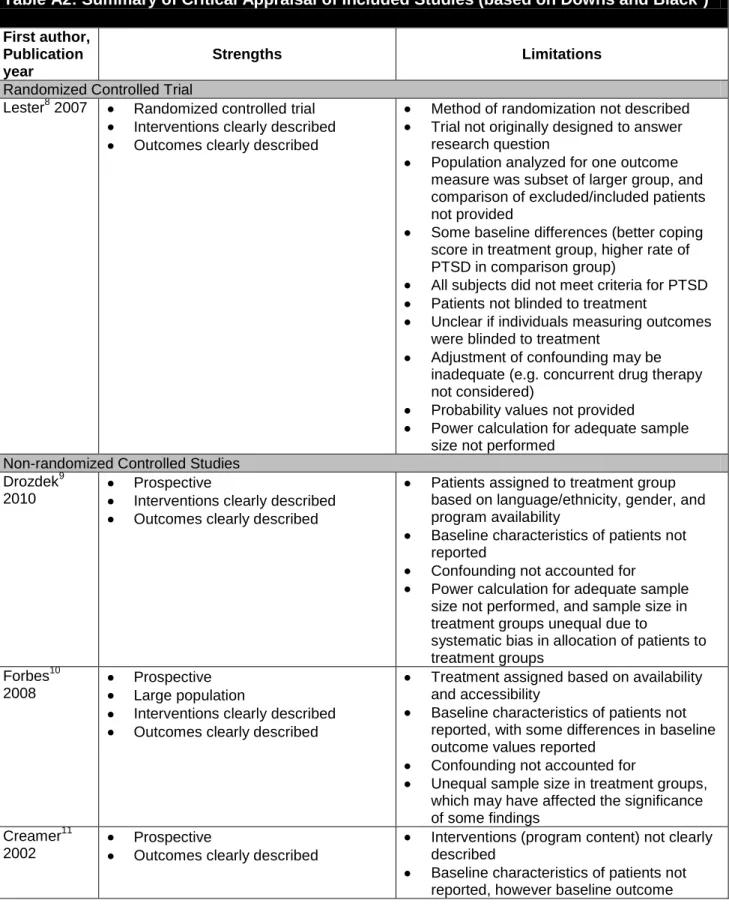
Table A2: Summary of Critical Appraisal of Included Studies (based on Downs and Black7)
First author, Publication year
Strengths Limitations
Randomized Controlled Trial
Lester8 2007 Randomized controlled trial Interventions clearly described Outcomes clearly described
Method of randomization not described Trial not originally designed to answer research question
Population analyzed for one outcome measure was subset of larger group, and comparison of excluded/included patients not provided
Some baseline differences (better coping score in treatment group, higher rate of PTSD in comparison group)
All subjects did not meet criteria for PTSD Patients not blinded to treatment
Unclear if individuals measuring outcomes were blinded to treatment
Adjustment of confounding may be inadequate (e.g. concurrent drug therapy not considered)
Probability values not provided
Power calculation for adequate sample size not performed
Non-randomized Controlled Studies Drozdek9
2010
Prospective
Interventions clearly described Outcomes clearly described
Patients assigned to treatment group based on language/ethnicity, gender, and program availability
Baseline characteristics of patients not reported
Confounding not accounted for
Power calculation for adequate sample size not performed, and sample size in treatment groups unequal due to
systematic bias in allocation of patients to treatment groups
Forbes10 2008
Prospective Large population
Interventions clearly described Outcomes clearly described
Treatment assigned based on availability and accessibility
Baseline characteristics of patients not reported, with some differences in baseline outcome values reported
Confounding not accounted for
Unequal sample size in treatment groups, which may have affected the significance of some findings
Creamer11 2002
Prospective
Outcomes clearly described
Interventions (program content) not clearly described
Baseline characteristics of patients not reported, however baseline outcome
values were comparable Confounding not accounted for
Power calculation for adequate sample size not performed
Uncontrolled Study Lande12
2011
Prospective
Intervention clearly described Outcomes clearly described Baseline characteristics of patients reported
No comparator
Potential impact of drug therapy not addressed
Relatively short duration of follow-up PSTD: Post-traumatic Stress Disorder
APPENDIX 4: Summary of Study Findings
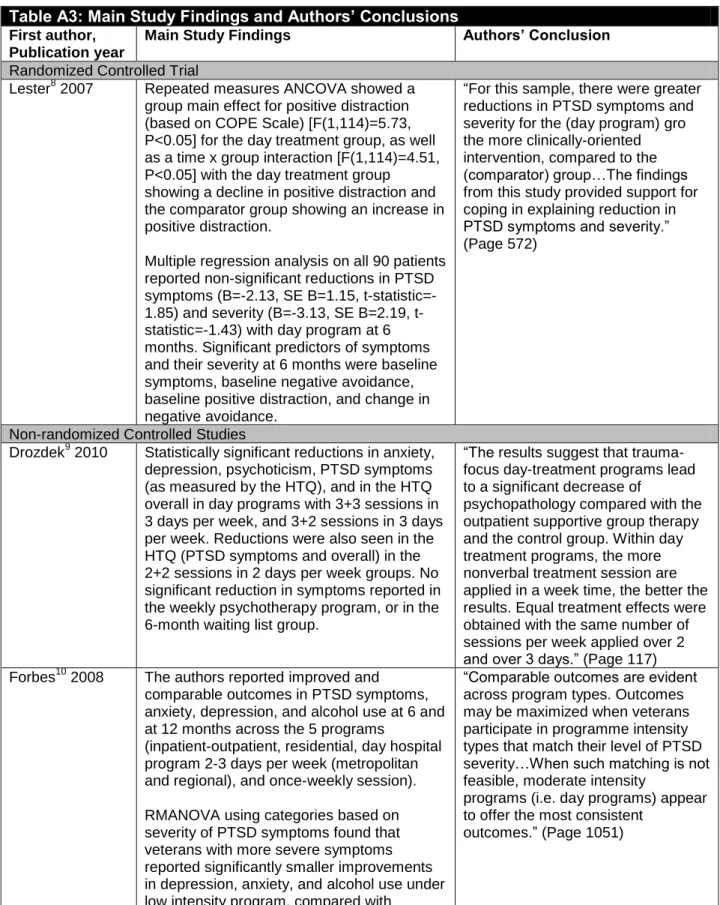
Table A3: Main Study Findings and Authors’ Conclusions
First author, Publication year
Main Study Findings Authors’ Conclusion
Randomized Controlled Trial
Lester8 2007 Repeated measures ANCOVA showed a
group main effect for positive distraction (based on COPE Scale) [F(1,114)=5.73, P<0.05] for the day treatment group, as well as a time x group interaction [F(1,114)=4.51, P<0.05] with the day treatment group showing a decline in positive distraction and the comparator group showing an increase in positive distraction.
Multiple regression analysis on all 90 patients reported non-significant reductions in PTSD symptoms (B=-2.13, SE B=1.15, statistic=-1.85) and severity (B=-3.13, SE B=2.19, t-statistic=-1.43) with day program at 6 months. Significant predictors of symptoms and their severity at 6 months were baseline symptoms, baseline negative avoidance, baseline positive distraction, and change in negative avoidance.
“For this sample, there were greater reductions in PTSD symptoms and severity for the (day program) gro the more clinically-oriented intervention, compared to the (comparator) group…The findings from this study provided support for coping in explaining reduction in PTSD symptoms and severity.” (Page 572)
Non-randomized Controlled Studies
Drozdek9 2010 Statistically significant reductions in anxiety, depression, psychoticism, PTSD symptoms (as measured by the HTQ), and in the HTQ overall in day programs with 3+3 sessions in 3 days per week, and 3+2 sessions in 3 days per week. Reductions were also seen in the HTQ (PTSD symptoms and overall) in the 2+2 sessions in 2 days per week groups. No significant reduction in symptoms reported in the weekly psychotherapy program, or in the 6-month waiting list group.
“The results suggest that trauma-focus day-treatment programs lead to a significant decrease of
psychopathology compared with the outpatient supportive group therapy and the control group. Within day treatment programs, the more nonverbal treatment session are applied in a week time, the better the results. Equal treatment effects were obtained with the same number of sessions per week applied over 2 and over 3 days.” (Page 117) Forbes10 2008 The authors reported improved and
comparable outcomes in PTSD symptoms, anxiety, depression, and alcohol use at 6 and at 12 months across the 5 programs
(inpatient-outpatient, residential, day hospital program 2-3 days per week (metropolitan and regional), and once-weekly session). RMANOVA using categories based on severity of PTSD symptoms found that veterans with more severe symptoms reported significantly smaller improvements in depression, anxiety, and alcohol use under low intensity program, compared with
“Comparable outcomes are evident across program types. Outcomes may be maximized when veterans participate in programme intensity types that match their level of PTSD severity…When such matching is not feasible, moderate intensity
programs (i.e. day programs) appear to offer the most consistent
veterans treated with moderate-to-high intensity programs. There was also a trend for those with the lowest severity to benefit less from high-intensity programs compared with low-intensity programs.
Creamer11 2002 Result from ANOVA suggested that both treatment models (inpatient-outpatient and day program) produced significant
improvement in core PTSD symptoms and comorbidity over time for up to 9 months, however there was no main effect for group on any outcome, suggesting that both treatment models produced similar patterns of treatment response over time.
“Group by time effects were not significant, which suggests that inpatient-outpatient programs are not more efficacious than less expensive day hospital alternatives. In line with current mental health policy
directions, the current study lends broad support to the
recommendation that treatment services for veterans with posttraumatic stress disorder be delivered in the least restrictive environment.” (Page 183) Uncontrolled Study
Lande12 2011 A significant reduction in PTSD and depression scores over time was reported (mean±standard deviation): PCL: Baseline: 64.92±10.00 Week 3: 57.76±14.88 t(37)=3.68, P=<0.001 Zung: Baseline: 71.04±9.20 Week 3: 64±13.69 t(34)=3.38, P=<0.001
“Results showed a statistically significant reduction in depression and PTSD symptoms after participants completed 3 weeks of intensive outpatient therapy.” (Page 530)
ANCOVA: analysis of covariance; ANOVA: Analysis of Variance; B: beta; COPE: Coping Orientations to Problems Experienced ; HTQ: Harvard Trauma Questionnaire; PCL: PTSD Checklist; PTSD: post-traumatic stress disorder; RMANOVA: repeated measures analysis of variance; SE B: Standard error of beta; t: t-statistic