TALAR ARTICULAR CARTILAGE DEFORMITY FOLLOWING A WALKING BASED LOADING PROTOCOL
Alexandra Owen Glenn
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in the
Department of Exercise and Sport Science
Chapel Hill 2018
Approved by:
Advisor: Erik Wikstrom
Reader: Kyeongtak Song
CHAPTER 1: INTRODUCTION
Lateral ankle sprains are the most prevalent musculoskeletal injuries in physically active populations.1 Ankle ligament sprains are the most common injury in NCAA
sports.2 In the general population, ankle sprains are also the most common reason for
presenting to an Emergency Department with an estimated 2.1 per 1000 persons.3,4
Further the recurrence rates are high which subsequently leads to a large percentage of patients suffering from chronic ankle instability.1 This chronic instability leads to
decreased physical activity and quality of life as well as an increase in the rates of post-traumatic ankle osteoarthritis.5–12 Post-traumatic ankle osteoarthritis cases comprise the
majority of ankle joint osteoarthritis surgical cases.13 All of these create a tremendous
societal and financial burden. The mean societal costs for a joint sprain is $9.196 and the mean cost for ankle injuries was found to be $11,925 among high school athletes.14
Further, it must be recognized that less than 50% of patients with lateral ankle sprains may seek formal care which likely leads to an underestimation of true costs.15 This figure
also doesn’t include the costs of the possible surgeries for ankle instability or ankle fusion if osteoarthritis develops. Currently ankle fusions cost about $16,754 while an ankle replacement costs about $21,423.
Lateral ankle sprains occur due to a sudden rapid inversion and internal rotation loading of the foot and ankle complex irrespective of sagittal plane position.13 This one
injury can lead to general ankle instability and deficits in proprioception and
osteoarthritis and ultimately put patients in positions where there is no treatment to modify their disease besides surgery and symptomatic treatment.
Patients that have had ankle sprains and chronic ankle instability have
demonstrated degenerative changes to the talar cartilage in many studies. However, no study has analyzed the presence of symptoms pertaining to weakness, laxity, or pain prospectively while degenerative changes occur. Thus it is difficult to determine if lateral ankle sprains initiate degenerative changes. A recent study found higher T2 relaxation times in a group that had recently had an ankle sprain but had no symptoms (i.e. copers).5
This increased time indicates a loss of water content and collagen fiber which suggests that degeneration may occur quickly following an injury.13 It is then essential to gain
knowledge pertaining to normal cartilage function so that appropriate early interventions that could slow the development of PTOA can be developed.
Deficits in functional and sensorimotor control following an acute sprain could compress the joint and lead to degeneration and abnormal joint loading not present in uninjured controls. This abnormal joint loading can lead to an imbalance between degeneration and repair. Further, proprioceptive deficits are known to worsen after an injury and with age and may be linked to an increased risk of ankle osteoarthritis. Decreasing the possibility of another sprain and restoring motor control and
proprioception may help mitigate cartilage degeneration and decrease the likelihood of developing OA. Therefore, it would be beneficial to determine if worse cartilage health is associated with functional deficits that may be allowed to persist and accelerate
But before we can answer that question, we need to know more about how ankle cartilage deforms during normal daily activities. Ultrasonography imaging can be helpful in determining this as it has been found to be a valid tool for assessing cartilage thickness and can be used to monitor cartilage deformation post-acute loading in the knee.16–19 It is
much less costly than an MRI and can be done bedside. The purpose of this study is to quantify the amount of talar cartilage deformation following a standardized load.
CHAPTER II: REVIEW OF THE LITERATURE Introduction
The most prevalent musculoskeletal injury in physically active populations is a lateral ankle sprain.13 Reoccurrences of ankle injuries are common and often result in
chronic ankle stability (CAI). Hertel 20 proposed a model for CAI that incorporates
mechanical instability due to pathologic laxity after ankle-ligament injury and/or
functional instability due to occurrence of recurrent ankle instability and the sensation of joint instability due to contributions of proprioceptive and neuromuscular deficits.21,22
These proposed causal mechanisms are similar to those believed to cause the
development of ankle post-traumatic osteoarthritis (PTOA). Lateral ankle sprains are likely to develop into chronic ankle instability which increases the risk of developing early onset ankle joint PTOA.5–7,9,10 While research is not common, a link has been made
between lateral ankle sprains, CAI, and the development of ankle PTOA. Roughly fifty percent of patients with PTOA reported recurrent ankle sprains and/or CAI.23–25
nature.23–25 This may explain why patients with end-stage ankle OA tend to be younger
(average age of 53) than those with knee or hip OA. Similarly, ankle PTOA patients have a faster progression of functional loss with progression from injury to end stage OA taking 10-20 years.8 Patients with ankle OA have expressed profound physical limitations
comparable to those with end-stage kidney disease, congestive heart failure, and cervical pain and radiculopathy.8
Patients with ankle OA have no disease-modifying treatments and must resort to treatments that focus on treating symptoms and increasing functional stability.13 These
methods include treatments such as pain medication and physical therapy or surgery in more severe cases. Currently, at the ankle, these surgical options include arthroplasty or arthrodesis and ankle replacement. All of these treatment options create financial as well as time burdens for patients that must take off time from work due to flare-ups.
Nwachukwu et al performed a cost-analysis for those with ankle osteoarthritis based on the cost of ankle fusion and ankle replacement in 2012 and found that given the indirect and direct costs of ankle OA, the best option for patients is an ankle replacement
($21,423).26 Despite these large financial and physical burdens associated with ankle OA,
there is little known pertaining to the underlying causes of this disease or how it can be slowed or prevented.
Pathophysiology of Ankle Osteoarthritis
patients, often seen as osteochondral lesions and/or intraarticular pathologies soon after the initial incident.8 In fact, 87% of patients who had a history of recurrent ankle sprains
for at least 10 years had evidence of arthritic changes.27 Similarly, 21-95% of patients
with CAI have demonstrated degenerative changes.9,10,28–37 Sammarco and DiRaimondo’s
study found only 21% of patients with CAI demonstrating degenerative changes less than 2 years after the initial injury.32 A study by Takao et al similarly found only 50% of his
patients to have degenerative changes an average of seven months post ankle injury and only 29% were found to have osteochondral lesions.34 However, studies by Komenda and
Ferkel31 and Ferkel and Chams29 found 91% of patients to have degenerative changes
close to two years post injury but only 25% to have osteochondral lesions. The above studies were based on populations that needed ankle surgery to treat their symptoms of CAI, not patients diagnosed with ankle joint OA. Thus the percentages may be higher if one were to look solely at patients diagnosed with ankle joint OA. However, this is difficult to determine given the lack of studies in which cartilage imaging is performed for those sustaining a lateral ankle sprain or CAI to date. Very few studies analyze the development of symptoms with documented changes. However, a paper by Van Ochten et al36 found that relative to the contralateral limb of patients with a lateral ankle sprain,
significant evidence of radiographic changes in the injured ankle was found. This study suggests that though there may not be self-reported dysfunction of PTOA following an ankle sprain, the lateral ankle sprain initiates the degenerative changes. This brings up the question if altered biomechanics play a role in the degeneration of talar cartilage.
symptoms of CAI found that these groups had higher T2 relaxation times compared to those in the study that were uninjured.5 This increased relaxation time points to a
alteration of water content and collagen fiber integrity.13 With the average age of
participants in this study approximately 25 and their initial ankle sprain occurring within 5 years prior to testing, the results suggest that ankle degeneration occurs over a very short time frame after the initial sprain. Research is needed to determine if early
degenerative changes are precursors for the development of end stage ankle OA later in life, as it may not develop for twenty-five to thirty years after injury.8 It would be
beneficial to determine how early degeneration and end-stage ankle OA relate and if there are any possible interventions that may be helpful to disrupt this timeline.
The difficulty pertaining to ankle PTOA is there is no known underlying etiology for its degenerative changes. A study by Taga et al10 found that an acute lateral ankle
sprain may be enough to cause an osteochondral lesion as they found 89% of the acutely sprained ankle patients with a mean age of nineteen to have one. This suggests the claim that half of those that have developed PTOA developed it after only one traumatic ankle sprain.6,25 Further the copers in the Golditz et al5 study also support this claim. Finally,
Lee et al12 examined patients that had all developed osteochondral lesions and found
further evidence that a single ankle sprain is enough to cause this degenerative change. Thus the assumption can be made that if a single ankle sprain may cause osteochondral lesions then recurrent ankle sprains will exacerbate contact stress adaptations11 and
advance degenerative changes.
in neuromuscular control.38 It has been found that individuals with a history of ankle
sprains have a greater number of alterations of dynamic postural control due to
fatigue.39,40 Retrospective assessments have found that many functional and sensorimotor
deficits persist in the months following an ankle sprain.41,42 These deficits in balance and
movement control following an injury may compress the joint (i.e. alter normal loading patterns) and lead to degenerative changes that eventually lead to ankle PTOA.
Post-trauma, excessive and abnormal joint loading may lead to an imbalance between degeneration and repair of articular cartilage.43 Healing and bone remodeling
increases subchondral bone stiffness which decreases the ability to dissipate force and results in cartilage absorbing higher stress44 which may also contribute to the
development of OA.
Proprioceptive deficits (or deficits in the perception of the body segment position) may lead to individuals being unable to appropriately protect their joints from impulsive loading during ambulation. Studies have shown that proprioceptive acuity diminishes with age in the lower extremity45–47 but more so in patients with OA at a similar age.48
Thus, these deficits in proprioception may be pathophysiologically related to the onset or progression of OA. Further, deficits in neuromuscular control may cause patients to have higher loading rates of their joints.13 Ergo the worse the neuromuscular control, the higher
the joint may be loaded which may also be a possible predisposing factor to ankle OA. This information puts an emphasis on restoring correct biomechanics and motor control following an ankle sprain. There is a higher likelihood of recurrent injury following a single ankle sprain possibly due to deficits in neuromuscular control.13
biomechanics would likely mitigate cartilage degeneration and decrease the likelihood of developing ankle OA. Golditz et al49 found mediolateral time to stabilization was
correlated to increased relaxation time which suggests that that ankle OA may be associated with functional deficits. While there are currently no known possible interventions to lessen or slow the degeneration of cartilage, it would be beneficial to determine if worse cartilage health is associated with functional deficits that may be allowed to persist and accelerate deterioration of ankle health and function.
Cartilage Imaging
OA is primarily recognizable through the degradation of articular cartilage, which causes a decrease in cartilage thickness.50 OA is typically diagnosed through analysis of
joint space via radiography to determine if there is a narrowing of this space.51 However
this can be affected by the position of the ankle while the joint space is analyzed. While radiography is the current gold standard for imaging to diagnosis established
osteoarthritis due to its low cost and ease of access, it does not give a meaningful look at the cartilage because it cannot be viewed. This lack of ability to image is not helpful in diagnosing the early stages of PTOA and does not provide any pathophysiological information for physicians to use.
The current most detailed method of diagnosis and analyzing cartilage is through magnetic resonance imaging (MRI) as it is able to visualize structures not imaged by radiography.52–54 While this method allows clinicians to evaluate the ankle as a whole unit
types of MRI that have been utilized in imaging ankle cartilage. The first, T1-weighted imaging is useful for detection of proteoglycan density, which is the make-up of articular cartilage such as talar cartilage.56 This is useful in the early stages of deformation because
the diminishing of proteoglycan density allows for the cartilage to swell. Whereas the second, T2-weighted, is better at detecting water content which may be increased in those with deformation of articular cartilage.56 This influx of water due to the cartilage swelling
is picked up by this test.
Similar to radiography, ultrasonography (US) imaging provides imaging at a low cost. However, this imaging is real-time and multi-planar which may make it a more functional assessment of OA and its associated features without exposure to radiation or the necessity of contrast administration.16 It is also portable so that it can be easily used in
a clinical setting. Recent studies have found US to be a valid tool for assessing cartilage thickness in the knee as compared to cadaver measurements17 and MRI.18,19 Studies
pertaining to knee OA evaluated femoral cartilage deformation (i.e. change in thickness) before and after loading when walking and running and observed a 6.7% decrease in cartilage thickness post walking within 5 minutes of movement.57 This demonstrates how
US can be utilized to monitor cartilage deformation post acute loading. However, such information regarding the normal deformation patterns, post-loading, at the ankle joint has not been generated.
In this observational study, talar articular cartilage was measured prior to and following treadmill walking in twenty healthy, physically active individuals. Participants reported for a screening intervention session. Participants were educated on the
procedures of the study and signed an IRB approved informed consent during screening. For the control session, cartilage was measured pre- and post-walking 5000 steps. All participants were required to have no history of acute or chronic lower extremity musculoskeletal injury, or lower extremity surgery. A convenience sample of healthy individuals between the ages of 18 and 30 years of age who self-reported participating in physical activity for at least 20 minutes 3 days per week were enrolled.
Procedures
Upon arrival to the Sports Medicine Research Laboratory and Human
Performance Center at the University of North Carolina-Chapel Hill for data collection, participants rested on a padded table in a long-sit position with knees in full extension and ankles relaxed for 45 minutes to unload the cartilage, permit fluid rebound, and minimize effects of preceding activity.13 US images of the talar cartilage for both limbs
were obtained prior to and following treadmill walking. All post-loading images were captured within 5 minutes to minimize fluid rebound of the cartilage. The dominant limb of participants, defined as the leg a participant would choose to kick a ball with, were used for statistical analyses.
Ultrasonographic Assessment of the Talar Articular Cartilage
transversely in line with the distal portion of the medial and lateral malleoli (Figure I). Three images were recorded for each patient during the pre and post loading sessions.
Figure I. Probe Placement.
Treadmill Walking Protocol
After the US images were obtained, an investigator transported the patient from the treatment table to the treadmill via a wheelchair. The participants then walked at a comfortable self-selected pace for 5000 steps on a treadmill (4Front, WOODWAY, Waukesha, WI). Participants were instructed to walk at a self-selected speed described as “comfortably walking over a sidewalk.” Force Sensitive Resistor (FSR) Sensors (Trigno, DelSys Inc., Natick, MA) were placed on the plantar surfaces of the calcaneus and head of the first metatarsal to identify steps and phases of the gait cycle. Custom LabVIEW code was then used to calculate the number of steps per minute to estimate the time necessary to attain 5,000 steps.
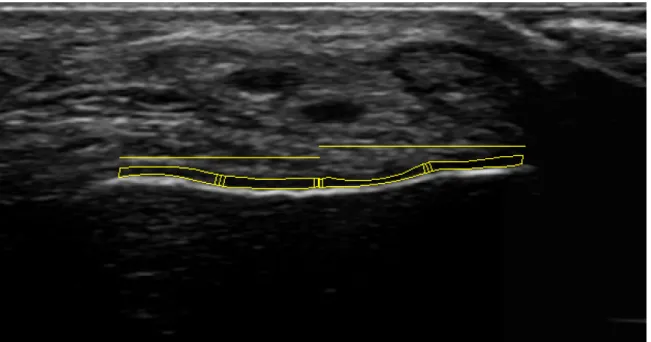
Ultrasound images were processed using ImageJ software (National Institutes of Health, Bethesda, MD). To determine cartilage thickness, perpendicular lines in ImageJ were drawn (in millimeters) from hyper-echoic edge of the tibia to hyper-echoic edge of the talus at a midpoint and lateral and medial portion dependent on the upslope of the lateral and medial shoulders. Cartilage area was also recorded by outlining the entire cartilage via segmentation (i.e. polygon function) to calculate the average thickness across the entire joint surface. Values were obtained for each image at each time point (pre and post walking) and averaged from three images for statistical analysis.
Statistical Analysis
Statistical analysis was performed using SPSS. A two-by-two repeated measure ANOVA (Time x Limb) was used to assess the changes from pre to post-loading between the dominant and non-dominant limb. An alpha level of 0.05 was used for all analyses.
Figure III. Example of Talar Cartilage Ultrasound Image Analysis. CHAPTER IV: RESULTS
Table I. Demographics of the participants.
Sample Size Age Height (cm) Weight (kg) Walking Speed (mph)
20 21.85 (±2.04) 170.83 (±8.94) 71.12 (±11.46) 3.06 (±0.26)
*Indicates a significant difference p<0.05 CHAPTER V: DISCUSSION
The purpose of this study was to quantify the amount of talar cartilage
deformation and magnitude of echo intensity change following a standardized loading protocol using treadmill walking. The main findings indicate that the loading protocol did not cause a notable deformation of the talar cartilage or change in echo intensity Table II. Means and standard deviations of talar cartilage thickness and echo intensity measures for each limb, before and after the walking protocol.
Dominant Pre Dominant Post Non-DominantPre Non-DominantPost Lateral side: single
point thickness
(mm) 0.050±0.015 0.048±0.014 0.050±0.017 0.049±0.016 Medial side: single
point thickness (mm)
0.048±0.017 0.049±0.017 0.045±0.017 0.046±0.022
Lateral side: average
thickness (mm) 0.050±0.015 0.048±0.014 0.050±0.017 0.049±0.016 Medial side: average
thickness (mm) 0.051±0.027 0.049±0.017 0.045±0.017 0.045±0.022 Lateral side: Echo
Intensity (AU) 16.560±7.651 16.904±5.687 15.949±5.264 16.972±4.942 Medial side: Echo
Intensity (AU) 19.041±7.301 18.642±7.335 21.058±6.733 20.7936±7.582 Table III. Means and standard deviations of talar cartilage thickness and echo intensity measures collapse across limbs, before and after the walking protocol.
Pre Post
when both limbs were averaged. This information does not support our hypothesis as we expected a significant deformation following the loading protocol.
Cartilage Thickness
Recent studies have found ultrasonography to be a valid tool for assessing cartilage thickness in the knee as compared to cadaver measurements and MRI.17,18,19
Further, studies have noted that knee femoral cartilage thickness decreases after a standardized walking protocol.57 While this demonstrates that ultrasound can be utilized
to monitor cartilage deformation post acute loading, there are several anatomical and biomechanical differences between the femoral and talar cartilage that may explain why talar cartilage did not deform to the same extent as femoral cartilage. Cartilage from the ankle joint is significantly more cellular and synthesizes more proteoglycans and collagens as compared to the knee.56 Additionally, the size, shape, and function differs
greatly between the two joints. The knee consists of two crests to hold the condyles of the femur as it moves in a hinge motion. The talar joint functions more as a gliding joint when performing the hinge motion with the talus moving to allow foot movement up and down and the tarsal bones help with an inversion and eversion movement. Because of the increased complexity of bones absorbing weight and shock in the foot as compared to the knee, talar cartilage may not absorb as much as knee cartilage does in the same amount of time or distance walking.
Currently, magnetic resonance imaging allows for detailed diagnosis and analysis of cartilage degeneration given the inability of radiography to visualize cartilage
understand talar cartilage composition but the lack of deformation observed may suggest that US is not a sensitive enough measure given the size of the talar cartilage (1-1.5mm thickness). Thus, future studies are needed to examine cartilage deformation in those with a history of ankle trauma (i.e. those with an increased risk of developing post-traumatic osteoarthritis) and in a variety of population following more dynamic loading protocols (e.g. running, hopping).
It is also possible that significant deformation may not occur in young healthy adults following a walking protocol. When walking, anterior calf muscles undergo an eccentric contraction as compared to a concentric contraction when running or sprinting.58 Further, muscle function of the posterior calf mainly occurs during the
midstance phase, whereas these muscles are predominately active in the late swing phase when running or sprinting.58 Finally, dorsiflexion at the ankle joint is decreased with
walking as compared to running or sprinting.58 Given how these patterns change at
different speeds, they may play a role in how the talar cartilage is stressed. It is also possible that walking for a longer time could continue to increase stress and/or
deformation of the talar cartilage and result in more uniform and/or obvious deformation changes. Therefore, talar cartilage deformation should also be assessed when running and during other tasks such as jump landing to determine the task most likely to elicit talar cartilage loading.
Echo Intensity
walking protocol would suggest that water has been pushed out of the cartilage, leaving a more homogeneous tissue of proteoglycans. While significant changes were not detected, a subtle decline in echo intensity was observed on the lateral side which corresponded to a subtle change in lateral side thickness. Interestingly, an increased echo intensity (not significant) was noted on the medial side following the loading protocol. Cartilage is a viscoelastic material and while speculative, it is possible that the lateral side of the ankle was loaded more during the walking protocol and “pushed” water into the medial aspect of the talar cartilage. While we would anticipate a subtle thickness increase on the medial side as well, this was not observed. However, is should be noted that only a small view of the cartilage was taken and thickness changes may have occurred in an anterior-posterior direction. This should be the focus of future research.
the speed of the gait of the individuals may need to be evaluated as a co-variate in future research. The lack of clear and consistent anatomical landmarks makes it difficult to ensure that single point thickness measures are taken at the same location across participants and time points. This can be seen when viewing Figure III, as there is an obvious lack of clarity on definitive edges and landmarks. Images are also in two
dimensions, despite the ankle obviously functioning in three dimensions. More thorough imaging from different angles may provide more data in future studies. Finally, the possible role of differences of foot structure was not evaluated in this study but may play a role in the amount or type of deformation that presents following a load.
Conclusion
In conclusion, no significant difference in echo intensity or cartilage deformation was observed following a standardized walking protocol. The results from this initial investigation using healthy participants highlights the need for further research in this area in order to enhance clinician friendly tools capable of describing early degenerative changes to the talar cartilage in those with a history of ankle joint trauma.
REFERENCES
physically active. Med Sci Sport Exerc. 2001;33(5):778-782. doi:10.1097/00005768-200105000-00016.
2. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42(2):311-319. doi:10.1111/j.1600-0838.2006.00528.x.
3. Waterman CBR, Owens MBD, Davey CS, Zacchilli CMA, Belmont LCPJ. The Epidemiology of Ankle Sprains in the United States. J Bone Jt Surgery-American Vol. 2010;92(13):2279-2284. doi:10.2106/JBJS.I.01537.
4. Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012;470(1):284-290. doi:10.1007/s11999-011-1982-z.
5. Golditz T, Steib S, Pfeifer K, et al. Functional ankle instability as a risk factor for osteoarthritis: Using T2-mapping to analyze early cartilage degeneration in the ankle joint of young athletes. Osteoarthr Cartil. 2014;22(10):1377-1385. doi:10.1016/j.joca.2014.04.029.
6. Valderrabano V, Horisberger M, Russell I, Dougall H, Hintermann B. Etiology of ankle osteoarthritis. Clin Orthop Relat Res. 2009;467(7):1800-1806.
doi:10.1007/s11999-008-0543-6.
7. Valderrabano V, Pagenstert G, Horisberger M, Knupp M, Hintermann B. Sports and Recreation Activity of Ankle Arthritis Patients before and after Total Ankle Replacement. Am J Sports Med. 2006;34(6):993-999.
doi:10.1177/0363546505284189.
8. Valderrabano V, Hintermann B, Horisberger M, Fung TS. Ligamentous Posttraumatic Ankle Osteoarthritis. Am J Sports Med. 2006;34(4):612-620. doi:10.1177/0363546505281813.
9. Hirose K, Murakami G, Minowa T, Kura H, Yamashita T. Lateral ligament injury of the ankle and associated articular cartilage degeneration in the talocrural joint: Anatomic study using elderly cadavers. J Orthop Sci. 2004;9(1):37-43.
doi:10.1007/s00776-003-0732-9.
10. Taga I, Shino K, Inoue M, Nakata K, Maeda A. Articular Cartilage Lesions in Ankles with Lateral Ligament Injury. An arthroscopic study. Am J Sports Med. 1993;21(1):120-127. doi:10.1177/036354659302100120.
11. Bischof JE, Spritzer CE, Caputo AM, et al. In vivo cartilage contact strains in patients with lateral ankle instability. J Biomech. 2010;43(13):2561-2566. doi:10.1016/j.jbiomech.2010.05.013.
12. Lee M, Kwon JW, Choi WJ, Lee JW. Comparison of Outcomes for Osteochondral Lesions of the Talus With and Without Chronic Lateral Ankle Instability. Foot
Ankle Int. 2015;36(9):1050-1057. doi:10.1177/1071100715581477.
13. Gribble PA, Bleakley CM, Caulfield BM, et al. 2016 consensus statement of the International Ankle Consortium: prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sport Med. 2016;50:1493-1495. doi:10.1136/bjsports-2016-096188.
15. McKay GD, Goldie P a, Payne WR, Oakes BW. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med. 2001;35(2):103-108.
doi:10.1136/bjsm.35.2.103.
16. Roemer FW, Kwoh CK, Hannon MJ, et al. Risk factors for magnetic resonance imaging-detected patellofemoral and tibiofemoral cartilage loss during a six-month period: The Joints on Glucosamine study. Arthritis Rheum. 2012;64(6):1888-1898. doi:10.1002/art.34353.
17. Keen HI, Conaghan PG. Ultrasonography in Osteoarthritis. Radiol Clin North Am. 2009;47(4):581-594. doi:10.1016/j.rcl.2009.04.007.
18. Naredo E, Acebes C, Moller I, et al. Ultrasound validity in the measurement of knee cartilage thickness. Ann Rheum Dis. 2009;68(8):1322-1327.
doi:10.1136/ard.2008.090738.
19. Ostergaard M, Court-Payen M, Gideon P, et al. Ultrasonography in arthritis of the knee. A comparison with MR imaging. Acta Radiol. 1995;36(1):19-26.
20. Hertel J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J Athl Train. 2002;37(4):364-375.
doi:10.1017/CBO9781107415324.004.
21. Freeman M. Instability of the foot after injuries to the lateral ligament of the ankle.
J Bone Jt Surg Br Ed. 1965;47(4):669-677.
22. Hertel J. Functional Instability Following Lateral Ankle Sprain. Sport Med. 2000;29(5):361-371. doi:10.2165/00007256-200029050-00005.
23. Saltzman CL. Impact of Comorbidities on the Measurement of Health in Patients with Ankle Osteoarthritis. J Bone Jt Surg. 2006;88(11):2366.
doi:10.2106/JBJS.F.00295.
24. Brown TD, Johnston RC, Saltzman CL, Marsh JL, Buckwalter JA. Posttraumatic Osteoarthritis: A First Estimate of Incidence, Prevalence, and Burden of Disease. J
Orthop Trauma. 2006;20(10):739-744. doi:10.1097/01.bot.0000246468.80635.ef.
25. Saltzman CL, Salamon ML, Blanchard GM, et al. Epidemiology of ankle arthritis: report of a consecutive series of 639 patients from a tertiary orthopaedic center.
Iowa Orthop J. 2005;25:44-46.
http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=1888779&tool=pmcentrez&rendertype=abstract.
26. Nwachukwu BU, McLawhorn AS, Simon MS, et al. Management of End-Stage Ankle Arthritis: Cost-Utility Analysis Using Direct and Indirect Costs. J Bone Jt
Surg Am. 2015;97(14):1159-1172. doi:10.2106/JBJS.N.01215.
27. Harrington KD. Degenerative arthritis of the ankle secondary to long-standing lateral ligament instability. J Bone Joint Surg Am. 1979;61(3):354-361. http://www.ncbi.nlm.nih.gov/pubmed/429402.
28. Hintermann B, Boss A, Schafer D. Arthroscopic findings in patients with chronic ankle instability. Am J Sport Med. 2002;30(3):402-409.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?
cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12016082.
29. Ferkel RD, Chams RN. Chronic Lateral Instability: Arthroscopic Findings and Long-Term Results. Foot Ankle Int. 2007;28(1):24-31.
doi:10.3113/FAI.2007.0005.
Med. 1996;15(4):799-804. http://www.ncbi.nlm.nih.gov/pubmed/8891409. 31. Komenda GA, Ferkel RD. Arthroscopic Findings Associated with the Unstable
Ankle. Foot Ankle Int. 1999;20(11):708-713. doi:10.1177/107110079902001106. 32. Sammarco GJ, DiRaimondo C V. Surgical treatment of lateral ankle instability
syndrome. Am J Sports Med. 1995;16(5):501-511. http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=2989041&tool=pmcentrez&rendertype=abstract.
33. Sugimoto K, Takakura Y, Okahashi K, Samoto N, Kawate K, Iwai M. Chondral Injuries of the Ankle with Recurrent Lateral Instability: An Arthroscopic Study. J
Bone Jt Surgery-American Vol. 2009;91(1):99-106. doi:10.2106/JBJS.G.00087.
34. Takao M, Uchio Y, Naito K, Fukazawa I, Ochi M. Arthroscopic Assessment for Intra-articular Disorders in Residual Ankle Disability after Sprain. Am J Sports Med. 2005;33(5):686-692. doi:10.1177/0363546504270566.
35. van Dijk CN, Bossuyt PM, Marti RK. Medial ankle pain after lateral ligament rupture. J Bone Joint Surg Br. 1996;78(4):562-567.
36. Van Ochten JM, Mos MCE, Van Putte-Katier N, et al. Structural abnormalities and persistent complaints after an ankle sprain are not associated: An observational case control study in primary care. Br J Gen Pract. 2014;64(626):e545-e553. doi:10.3399/bjgp14X681349.
37. Van Putte-Katier N, Van Ochten JM, Van Middelkoop M, Bierma-Zeinstra SMA, Oei EHG. Magnetic resonance imaging abnormalities after lateral ankle trauma in injured and contralateral ankles. Eur J Radiol. 2015;84(12):2586-2592.
doi:10.1016/j.ejrad.2015.09.028.
38. Steib S, Zech A, Hentschke C, Pfeifer K. Fatigue-induced alterations of static and dynamic postural control in athletes with a history of ankle sprain. J Athl Train. 2013;48(2):203-208. doi:10.4085/1062-6050-48.1.08.
39. Gribble PA, Hertel J, Denegar CR. Chronic ankle instability and fatigue create proximal joint alterations during performance of the star excursion balance test. Int
J Sports Med. 2007;28(3):236-242. doi:10.1055/s-2006-924289.
40. Gribble PA, Hertel J, Denegar CR, Buckley WE. The effects of fatigue and chronic ankle instability on dynamic postural control. J Athl Train.
2004;39(4):321-329. doi:10.3844/pisp.2010.22.26.
41. Hertel J. Sensorimotor Deficits with Ankle Sprains and Chronic Ankle Instability.
Clin Sports Med. 2008;27(3):353-370. doi:10.1016/j.csm.2008.03.006.
42. McKeon PO, Hertel J. Systematic review of postural control and lateral ankle instability, Part I: Can deficits be detected with instrumented testing? J Athl Train. 2008;43(3):293-304. doi:10.4085/1062-6050-43.3.293.
43. Maly MR. Abnormal and cumulative loading in knee osteoarthritis. Curr Opin
Rheumatol. 2008;20(5):547-552. doi:10.1097/BOR.0b013e328307f58c.
44. Barrett DS, Cobb AG, Bentley G. Joint proprioception in normal, osteoarthritic and replaced knees. J Bone Joint Surg Br. 1991;73(1):53-56. doi:10.4172/2157-7595.1000119.
45. Hurley M V., Scott DL, Rees J, Newham DJ. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Ann Rheum Dis. 1997;56:641-648. doi:10.1136/ard.56.11.641.
knee proprioception. Arthritis Rheum. 1997;40(12):2260-2265. doi:10.1002/art.1780401223.
47. Lephart SM, Fu FH. Proprioception and neuromuscular control in joint stability.
Phys Rehabil Inj Athl. 2000:xxiv, 439 . doi:10.1016/B978-1-4377-2411-0.00024-1.
48. Collins JJ, Whittle MW. Impulsive forces during walking and their clinical implications. Clin Biomech. 1989;4(3):179-187.
doi:10.1016/0268-0033(89)90023-5.
49. Golditz T, Welsch GH, Pachowsky M, Hennig FF, Pfeifer K, Steib S. A
multimodal approach to ankle instability: Interrelations between subjective and objective assessments of ankle status in athletes. J Orthop Res. 2016;34(3):525-532. doi:10.1002/jor.23039.
50. Benedetti MG, Bonato P, Catani F, et al. Myoelectric activation pattern during gait in total knee replacement: Relationship with kinematics, kinetics, and clinical outcome. IEEE Trans Rehabil Eng. 1999;7(2):140-149. doi:10.1109/86.769404. 51. Eckstein F, Collins JE, Nevitt MC, et al. Brief Report: Cartilage Thickness Change
as an Imaging Biomarker of Knee Osteoarthritis Progression: Data From the Foundation for the National Institutes of Health Osteoarthritis Biomarkers Consortium. Arthritis Rheumatol (Hoboken, NJ). 2015;67(12):3184-3189. doi:10.1002/art.39324.
52. Eckstein F, Wirth W, Nevitt MC. Recent advances in osteoarthritis imaging—the Osteoarthritis Initiative. Nat Rev Rheumatol. 2012;8(10):622-630.
doi:10.1038/nrrheum.2012.113.
53. Guermazi A, Niu J, Hayashi D, et al. Prevalence of abnormalities in knees detected by MRI in adults without knee osteoarthritis: population based observational study (Framingham Osteoarthritis Study). BMJ. 2012;345(aug29 1):e5339-e5339. doi:10.1136/bmj.e5339.
54. Englund M, Roemer FW, Hayashi D, Crema MD, Guermazi A. Meniscus pathology, osteoarthritis and the treatment controversy. Nat Rev Rheumatol. 2012;8(7):412-419. doi:10.1038/nrrheum.2012.69.
55. Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012;64(6):1697-1707.
doi:10.1002/art.34453.
56. Filippi M, Charil A, Rovaris M, Absinta M, Rocca MA. Insights from magnetic resonance imaging. Handb Clin Neurol. 2014;122:115-149. doi:10.1016/B978-0-444-52001-2.00006-6.
57. Harkey MS, Blackburn JT, Davis H, Sierra-Arévalo L, Nissman D, Pietrosimone B. Ultrasonographic assessment of medial femoral cartilage deformation acutely following walking and running. Osteoarthr Cartil. 2017;25(6):907-913.
doi:10.1016/j.joca.2016.12.026.
58. Mann RA, Hagy J. Biomechanics of walking, running, and sprinting. The
American Journal of Sports Medicine. 1980;8(5):345-350. doi: