H
epatitis C virus (HCV) is an enveloped, single-stranded ribonucleic acid (RNA) virus of the flaviviridae family, which is classi-fied into six major genotypes and more than 100 subtypes. Genotype prevalence can vary based on region. In North America, genotype 1 is the most common, whereas genotypes 4 to 6 are rare. The genotype is important with respect toresponse to therapy. Genotype 1 has a poorer response as compared to genotypes 2 and 3. HCV continually mutates to form a variety of quasispecies and, in a single infected person, the viral genome can differ by 1% to 2%. This genetic heterogeneity allows the virus to evade immunity.
Long-Term Management of
Hepatitis C Virus Infection
Hepatitis C virus is now the main cause of chronic liver disease in North
America and, as such, family physicians must be prepared to identify it at
first glance.
By Alnoor S. Ramji, MD, and Eric M. Yoshida, MD, MHSc, FRCPC
Presented at the 36th Annual Postgraduate Review In Family Medicine, University of
British Columbia, March 2001.
Dr. Ramji is gastroenterology fellow, University of British Columbia, Vancouver.
Dr. Yoshida is assistant professor of medicine, University of British Columbia, and medical director, liver transplant program, British Columbia Transplant Society, Vancouver. His areas of medical interest include hepatology and gastroenterology.
Prevalence
HCV is now the main cause of chronic liver dis-ease in North America. It is responsible for 40% of all cases, and is the most common indication for liver transplantation.
Natural History Of HCV Infection
The exact natural history of HCV is still not completely understood, as previous tive studies differ from more recent retrospec-tive-prospective studies in terms of likelihood of progression to cirrhosis. It also is clear that the natural history differs depending on the popula-tion studied (i.e., it is more benign in children). The clinically important endpoint of HCV infec-tion is progression to cirrhosis and risk of hepa-tocellular carcinoma (HCC) (Figure 1).
Acute HCV infection
Most patients are asymptomatic or have non-specific prodromic symptoms of fatigue, malaise and anorexia. About 30% of patients will have jaundice. HCV-RNA is detectable within one to three weeks of infection and the HCV antibody may not develop for several weeks or months.1
Chronic HCV
After six months, approximately 20% of HCV patients will shed the virus, while the remainder will have chronic hepatitis and develop fibrosis of varying severity. The lifetime risk of an infected person to progress to cirrhosis often is cited as 25%. The progression to cirrhosis can take 10 to 20 years and can be strongly influ-enced by host factors, such as alcohol
consump-Summary
Long-Term Management of Hepatitis C Virus Infection
• About 170 million people, or 5% of the world population, are chronically infected with hepatitis C virus (HCV), with the North American prevalence rate being 1.8%.
• The clinically important end point of HCV infection is progression to cirrhosis and risk of hepatocellular carcinoma (HCC).
• HCV is primarily transmitted via percutaneous or mucous membrane exposure to blood.
• Until the development of decompensated cirrhosis, HCV patients are either asymptomatic or have nonspecific symptoms.
• Initial screening includes testing for antibodies to HCV. Patients testing positive for HCV antibodies should have a confirmatory test done.
• The most significant factor known to affect the progression of liver injury is associated alcohol consumption.
• The objective of treatment is to prevent cirrhosis and HCC. The current choice of therapy is combination interferon (subcutaneously three times a week) and ribavirin.
• Modified therapies include pegylated interferons, with the addition of a polyethylene glycol molecule to the interferon.
• Predictive factors for HCC development include infection with genotype 1b, alcohol use, older age and co-infection with hepatitis B virus.
tion. The overall lifetime risk of developing HCC is 1% to 5%, but this is strongly affected by the pres-ence or abspres-ence of cirrhosis. HCC is rare in patients without cirrhosis, but the infected person’s annual risk of HCC after developing cirrhosis is between 1% to 3%.1-5
Transmission
HCV is primarily transmitted via percutaneous or mucous membrane exposure to blood. With the advent of blood-donor screening, the current groups at highest risk are intravenous drug users (Table 1). Previously, blood transfusion accounted for a large proportion of transmission, with up to 25% of cases. The current risk via blood transfusion is estimated to be 0.01% to 0.001% per unit transfused.1
Transmission via practices that cause contact with small amounts of blood also are of concern. These practices include tattooing, acupuncture, body piercing and commercial shaving; there is even a recent report of transmission via fist-fights. The true magnitude of risk via these activities, however, is not well studied.
The risk of HCV via sexual transmission is thought to be low, with prevalence rates of 0% to 2.7% in stable couples where one partner is anti-HCV-positive. Patients with high-risk sexual behaviors (more than 50 lifetime sexual part-ners) have an increased risk, with prevalence rates of 4% to 8%.1,6
Health-care workers who have a percutaneous exposure to blood from an anti-HCV-positive
Figure 1. Natural history of HCV infection.
Adapted from: Seeff LB: Symposium: Update on viral hepatitis. American Association of Liver Disease, 2000. 100 patients
20 patients 80 patients
24 patients 32 patients 24 patients
36 patients 20 patients
100 patients
20 patients 80 patients
24 patients 32 patients 24 patients
36 patients 20 patients
20% recovery 80% recovery
40% variable progression 30% stable
chronic hepatitis
30% severe progression
Antiviral treatment Treatment
failure 65%
Sustained response 35%
patient have a 1.8% (0% to 10%) risk of sero-conversion.1,6
The risk of perinatal HCV transmission is low. Rates of HCV infection in infants of moth-ers with chronic HCV is 5%. The risk of trans-mission is proportional to maternal viremia.1
Clinical Manifestations Of Chronic
HCV Infection
Until the development of decompensated cirrho-sis, HCV patients are either asymptomatic or have nonspecific symptoms. The most common symptom is fatigue, but others may include anorexia, nausea, arthralgia, abdominal discom-fort and weight loss. Other organ systems may be affected (Table 2).
Diagnosis
Initial screening includes testing for antibodies to HCV. The third generation of enzyme-linked
immunosorbent assay (ELISA) tests are avail-able, with a sensitivity of 99% and a specificity of 99.3%. False-negative results can occur in the immunocompromised population and early in the course of infection before antibodies develop (Table 3).
Patients testing positive for HCV antibodies should have a confirmatory test done. Recombinant immunoblot assay (RIBA), analo-gous to the Western blot technique, was previ-ously used, but this test has been replaced. Instead, commercial assays for HCV-RNA by polymerase chain reaction (PCR) testing are now used, with both quantitative and qualitative tests, as well as genotyping.
Liver biopsy helps to establish co-existing liver pathologies, as well as severity, progres-sion and possible prognoses of disease. Liver biopsy can help guide therapy by determining the degree of inflammation and fibrosis, which
Table 1
Candidates For Routine Testing • People who ever injected illegal drugs. • People who had previous blood product
transfusions or organ recipients (prior to 1991). • Intranasal cocaine users.
• People with certain medical conditions: - long-term hemodialysis
- persistent elevation of alanine aminotransferase (ALT)
• Those who exhibit high-risk sexual behavior (> 50 sex partners).
• People who are exposed to blood products through their work (e.g., needlestick injuries). • Children born to HCV-positive mothers.
Table 2
Extrahepatic-Associated
Manifestations Of Chronic HCV
Hematologic • Essential mixed
cryoglobulinemia
• Non-Hodgkin’s lymphoma
Renal • Membranoproliferative
glomerulonephritis
Autoimmune • Autoimmune thyroiditis
• Sjögren’s syndrome
• Idiopathic thrombocytopathic purpura
Dermatologic • Porphyria cutanea tarda
• Lichen planus
• Leukocytoclastic vasculitis
may not be well-predicted by liver enzymes. Since the end point of therapy is sustained HCV-RNA undetectability, not all patients require biopsy prior to therapy.
Predictive Factors For Progression
To Liver Disease
There are certain factors known to affect the pro-gression of liver injury. The most significant fac-tor is associated alcohol consumption. Patients with HCV infection and alcohol consumption of greater than 50 g daily have a mean progression to cirrhosis of 13 years. In patients with only HCV infection, the mean interval to progression is 42 years.2,3,7-9
Other factors for increased progression of liver disease include:
• Over the age of 40 when exposed; • Male gender;
• Longer duration of infection; • HCV genotype 1; and
• Co-infection with other hepatotrophic viruses or human immunodeficiency virus (HIV).
Therapy For Chronic HCV
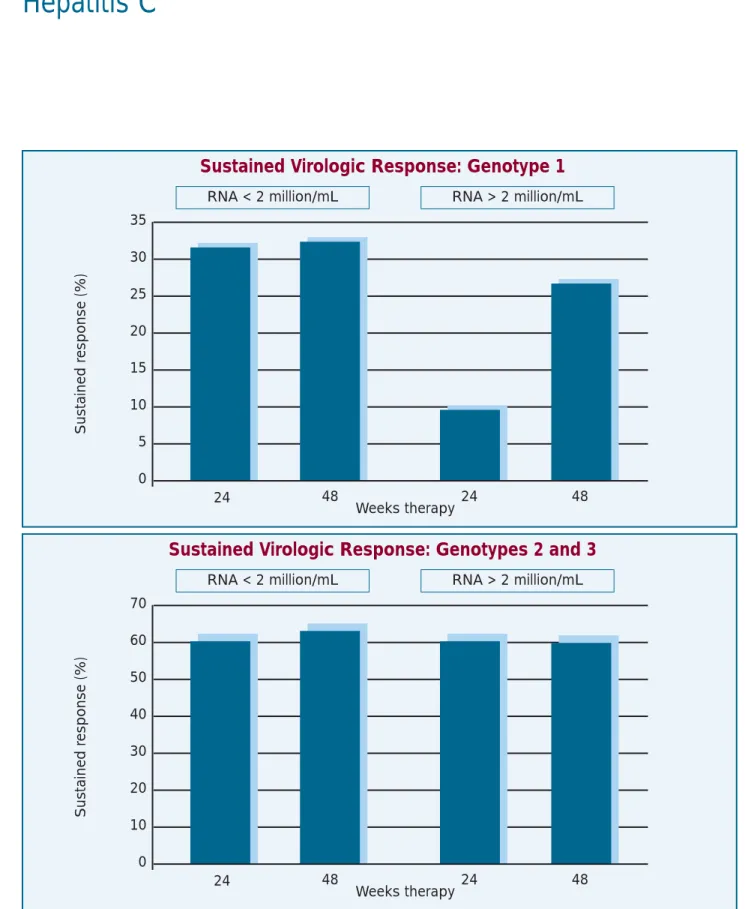
The objective of treatment is to prevent cirrhosis and HCC. The current choice of therapy is com-bination interferon (subcutaneously three times weekly) and ribavirin, with an overall 40% sus-tained rate: 30% in genotype 1 and 60% to 70% in genotypes 2 and 3 (Figure 2). Previously, monotherapy with interferon-alfa for 12 to 18 months produced a virologic response in 10% to 15% of patients, and is currently not recom-mended. Treatment requires therapy for between 24 weeks (genotypes 2 and 3) and 48 weeks (genotype 1 if HCV-RNA-negative after 24 weeks).10-14It should be noted there may be
sig-nificant side effects.
Patients should meet certain criteria for thera-py. These include medical aspects of the disease, as well as its associated social considerations. The decision to treat must evaluate overall health, age, likelihood of response and compli-ance issues. On at least two occasions separated by three months, patients should have confirmed HCV infection with detectable serum HCV-PCR and elevated alanine aminotransferase (ALT)
Table 3
Laboratory Tests For HCV Infection
Test Utility Clinical significance
Anti-HCV Indicates past or Cannot differentiate between acute/chronic infection. Useful present infection as a screening test only, not to follow patients.
HCV-RNA: Detects HCV-RNA in Confirmatory test of HCV infection. Useful to monitor success Qualitative serum of therapy. Positive earlier than antibodies after acute
infection.
HCV-RNA: Concentration of HCV- May be predictive of success of antiviral therapy. Large Qualitative RNA in serum. variability between different assays.
Genotype Differentiation on type May be predictive of success of antiviral therapy. Genotype 1 is of HCV, 6 genotypes the most prevalent and least responsive to antiviral therapy.
Figure 2. Virologic responses of combination therapy with ribavirin and interferon for genotypes 1 versus2 and 3. Sustained virologic response rates stratified by genotype and viral loads in patients treated with interferon plus ribavirin. Only patients with genotype 1 and viral load above 2 million copies/mL had a greater response rate to interferon plus rib-avirin therapy for 48 weeks versus24 weeks.
Adapted from: Seeff LB: Symposium: Update on viral hepatitis. American Association of Liver Disease, 2000.
35 30 25 20 15 10 5 0
Sustained r
esponse (%)
Sustained Virologic Response: Genotype 1
RNA < 2 million/mL RNA > 2 million/mL
24 48 24 48
Weeks therapy
70 60 50 40 30 20 10 0
Sustained r
esponse (%)
Sustained Virologic Response: Genotypes 2 and 3
RNA < 2 million/mL RNA > 2 million/mL
24 48 24 48
values greater than 1.5 times the upper limit of normal. These people should not have decom-pensated liver disease and need to abstain from drugs and alcohol, as well as comply with the treatment schedule.
Patients can have normal ALT levels with detectable HCV-RNA levels. These patients often have milder histology patterns, with slow-er and possibly non-progressive natural histo-ries. Treatment of this group generally is not rec-ommended.
Contraindications to interferon therapy include:
• Major psychiatric disease (especially depres-sion and bipolar disease);
• Autoimmune disease; • Pregnancy;
• Uncontrolled diabetes,
• Epilepsy or hypertension; and • Unstable coronary artery disease.
Contraindications to ribavirin include: • Hemolysis;
• Anemia with hemoglobin less than 110 g/L; • Coronary artery disease;
• Cerebrovascular disease; • Renal insufficiency; and
• Inability to practise contraception.
Predictors Of
Response To Therapy
Increased sustained response is reported with younger patients (under age 40), female gender, lower viral load (less than 3.5 million copies/mL), lack of alcohol use, lack of co-exis-tent liver disease and mild histologic changes. Genotypes 2 and 3 have the most favorable response rates. Patients with genotype 1 are less likely to respond, but with treatment of up to 48 weeks, response was improved and sustained. The effect of viral load upon treatment in geno-type 1 appeared to be predictive of response,
with lower titers having a more favorable out-come. Further, patients with higher viral loads responded better to prolonged therapy at 48 weeks. Although given multiple assays for HCV titer and a large variation within the same indi-vidual, these values should be used with cau-tion.12-15
Patients with stage 0 or 1 fibrosis have improved response rates over those with stage 3 or 4 fibrosis. Race may be a predictive factor of treatment response. African Americans appear to have a poorer response than Caucasians when controlled for genotype and compliance.16
Treatment Follow-up
Treatment responses during therapy and at short-term follow-up are generally maintained. If patients have normal liver tests, but detectable HCV-RNA, they tend to relapse after therapy. Clearance of serum HCV-RNA at 24 weeks post-treatment is considered a successful response, with a durability of approximately 90%. In gen-eral, patients will have normal liver tests and some improvement in liver histology.12,13
Side Effects
Of Combination Therapy
Side effects of combination therapy are experi-enced by most patients, and are usually manage-able. The most common side effects of interferon are flu-like symptoms, fatigue, arthralgia, myal-gia and weight loss. Ribavirin can cause cough, pruritis, insomnia, anorexia and hemolytic ane-mia. Because of common adverse effects, it is important to discuss these side effects in detail with patients, as well as to offer accessibility to health-care professionals and support groups.
Monitoring While
On Combination Therapy
Initially, patients on combination therapy should visit their physician on a biweekly basis, pro-gressing to monthly visits. Table 4 provides an approach to laboratory tests, though testing pro-grams should be individualized.15
Treatment In Special Groups
Chronic HCV infection and normal liver tests
Persistently normal ALT values occur in about 25% of patients with detectable HCV-RNA. Histologically, these patients are reported to have minimal inflammation and slowly progres-sive fibrosis. They also are less likely to develop cirrhosis. Occasionally, treatment strategies have failed to produce virologic responses and may even induce increased inflammation. There is no clear consensus as to the management of these patients.
Chronic HCV infection and cirrhosis
Even on combination therapy, only 20% of patients have sustained virologic responses.15
Acute HCV
A documented exposure and positive HCV-RNA by PCR is required for treatment. Therapy with interferon alfa three times weekly for three months showed a sustained response in 41% of patients versus 4% in controls.
Newer Therapies
Modified therapies include pegylated interfer-ons, with the addition of a polyethylene glycol molecule to interferon. This has a longer half-life, allowing once-a-week administration. Early data indicate improved virologic responses com-pared to interferon monotherapy, with response rates of 38% in non-cirrhotics. Preliminary data of pegylated interferon in combination with rib-avirin suggest a sustained virologic response of
Table 4
Monitoring Of Patients On Combination Interferon And Ribavirin Therapy
Laboratory Test Baseline Week 1 * Monthly Week 24
CBC X X X
HCV-RNA X X
ALT/AST X X X
Creatinine X
Thyrotropin X
Pregnancy X X
*These tests should be done weekly, for the first three weeks
CBC = complete blood count; HCV = hepatitis C virus; RNA = ribonucleic acid; ALT = alanine aminotransferase; AST = aspartate aminotransferase
over 50% overall and over 70% for genotypes 2 and 3, as well as fewer side effects.1,17
The development of a vaccine has proven challenging due to HCV’s ability to mutate, as well as its avoidance of immune surveillance. Milk thistle is a commonly used alternative ther-apy. There is no data to suggest any improvement in liver histology. In small studies, no significant unfavorable outcomes have been reported.
Screening For HCC
Predictive factors for HCC development include infection with genotype 1b, alcohol use, older age groups and co-infection with hepatitis B virus (HBV). The risk of HCC is increased par-ticularly in the context of cirrhosis. Screening of patients should be done in cirrhotics with alpha-fetoprotein and an ultrasound every six months.
Liver Transplantation
HCV accounts for approximately 25% of liver transplants. Patients should be referred to a transplant setting earlier, rather than later. Patients with compensated cirrhosis should be referred at the first indication of decompensation (i.e., ascites, variceal bleed, encephalopathy), upon the development of malnutrition or upon a progressive decline in liver synthetic function.
Post-transplantation HCV recurs almost uni-versally. The natural history and role of combi-nation treatment for post-transplant HCV is unclear.
References
1. Cheney CP, Chopra S, Graham C: Hepatitis C. Infect Dis Clin North Am 2000; 14:633-67.
2. Poynard T, Bedossa M, Opolon P: Natural history of fibrosis progression in patients with chronic hepatitis C. Lancet 1997; 349:825-32.
3. Seeff LB, Miller RN, Rabkin CS, et al: 45-year follow-up of hepatitis C virus infection in healthy young adults. Ann Intern Med 2000; 132:105-11.
4. Tong MJ, El-Farra NS, Raikes AR, et al: Clinical out-comes after transfusion associated hepatitis C. N Engl J Med 1995; 332:1463-6.
5. Yano M, Kumada H, Kage M, et al: The long-term patho-logical evolution of chronic hepatitis C. Hepatology 1996; 23:1334-40.
6. Lauer GM, Walker BD: Hepatitis C virus infection. N Engl J Med 2001; 345(1):41-52.
7. Moyer LA, Mast EE, Alter MJ: Hepatitis C: Part I. Routine serologic testing and diagnosis. Am Fam Physician 1999; 59(1):79-88, 91-2.
8. Corrao G, Arico S: Independent and combined action of hepatitis C virus and alcohol on the risk of symptomatic liver cirrhosis. Hepatology 1998; 27:914-9.
9. Niederau C, Lange S, Heintges T, et al: Prognosis of chronic hepatitis C: Results of a large prospective cohort study. Hepatology 1998; 28:1687-95.
10. Chamello L, Cavalletto L, Bernardinello E, et al: The effect of interferon alfa and ribavirin combination thera-py in patients with chronic hepatitis C. J Hepatology 1995; 23:8-12.
11. Lai MY, Kao JH, Yang DM, et al: Long-term efficacy of ribavirin plus interferon-alfa in the treatment of chronic hepatitis C. Gastroenterology 1996; 111:1307-12. 12. McHutchsion JG, Gordon SC, Schiff ER, et al: Interferon
alfa-2b alone or in combination with ribavirin as initial treatment for chronic hepatitis C. N Engl J Med 1998; 339:1485-92.
13. Poynard T, Marcellin P, Lee SS, et al: Randomized trial of interferon alfa-2b plus ribavirin for 48 weeks or for 24 weeks versus interferon alfa-2b plus placebo for 48 weeks for treatment of chronic infection with hepatitis C virus. Lancet 1998; 352:1426-32.
14. Reichard O, Norkrans G, Fryden A, et al: Randomized, double-blind, placebo controlled trial of interferon alfa-2b with and without ribavirin for chronic hepatitis C. Lancet 1998; 351:83-7.
15. Shad JA, McHutchison JG: Current and future therapies of hepatitis C. Clin Liver Dis 2001; 5:335-60.
16. Reddy KR, Hoofnagle JH, Tong MJ, et al: Racial differ-ences in response to therapy with interferon in chronic hepatitis C. Hepatology 1999; 30:787-93.
17. Seeff LB: Symposium: Update on viral hepatitis. American Association of Liver Disease, 2000.