ANTIBACTERIAL EFFECTS OF OZONE ON STREPTOCOCCUS MUTANS
Fernando Astorga
A thesis submitted to the Faculty of The University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master on Science in
the Department of Operative Dentistry of the School of Dentistry
Chapel Hill 2013
Approved by:
Luiz Pimenta, DDS, MS, PhD
Roland Arnold, PhD
Andre Ritter, DDS, MS, MBA
ABSTRACT
FERNANDO ASTORGA: Antibacterial effects of ozone on
Streptococcus mutans
(Under the direction of Luiz Pimenta)
Aims: To investigate the antibacterial effect s of ozone on Streptococcus mutans in vitro. Methods: A bacteria volume of 106 CFU/ml was inoculated on human and bovine dentin specimens and in Wilkins-Chalgren broth media (WC, Difco
Laboratories. Sparks) treated with two ozone sources ( Curozone X4®, Kavo; OL80A and
OL80W, Yanco Industries), at various concentrations (2, 20, 200, 2000 and 2100 ppm)
and exposure times (from 15 s ec to 4 min). Results: Curozone X4 had no effect on
bacteria recovery, while OL80A and OL80W showed a concentration -dependent
effect on S. mutans recover on a Trypticase™ Soy Agar with 5% Sheep Blood (Difco
Laboratories. Sparks). Concentrations of 200 and 2000 ppm showed no bacteria
recovery after treatment for 4 min, while 2 and 20 ppm showed significant
reduction of the recover ed bacteria. Conclusions: This study suggests that
Curozone X4® generator is not capable of delivering ozone to would effectively
disinfect a caries lesion.
To my mother Amarilis who taught me the pursuit of excellence in life,
wherever you are I hope you are proud
To my wife Liliana and my children Sebastian and Clementina, your love
and support made this dream come true
I love you all!
ACKNOWLEDGEMENTS
I want to thank the Lord and Jesus Christ my savior, for giving the
opportunity of coming here and follow his plan.
To my Thesis Committee members, Dr. Luiz Pimenta, Dr. Roland Arnold, Dr.
Andree Ritter and Dr. Kenneth Sexton, for accepting me as an advisee with my
limitations and stubbornness. I am grateful for your advice, patience, time, word of
encouragement, suggestions and guidance that made this thesis be completed.
Dr. Terry Donovan, Dr. Harald Heymann and Dr. Edward Swift, it has been
an honor to be your student.
The staff of the Department of Operative Dentistry, Shannon Tate, Dayna
McNaught, Jamie Desoto, Barbara Walton, Ginger Cole and Cynthia Lambert.
I want to thanks Mr. Eric Simmons for all your help and patience while
working with me in the lab and most of all I want to thank you for your friendship.
Kristi and Hiroko you have been the best classmates I ever had. I will never
forget these three years of sharing accomplishments, success, laugh and tears. You
will be in my heart forever. Also to the residents that made this experience even
more enjoyable Mario, Ayesha, Roopsie, Sumi, Alex, Silvia, Upoma, Vili and Clay.
The AEGD staff, Rosanna, Christy, Pam, Christina and Daryl.
All of you helped making UNC my home!
TABLE OF CONTENTS
Page
LIST OF TABLES………...viii
LIST OF FIGURES………. ....ix
LIST OF ABBREVIATONS…….………...x
1. INTRODUCTION……… ..…1
2. OBJECTIVES………….…….………..….…8
3. MATERIALS AND METHODS….………..…9
3.1 Bacteria species and culture. ……….……….……9
3.2 Ozone generators....……….……….………..9
3.3 Effect of ozone on human dental specimens..………..…..10
3.4Effect of ozone on bovine dental specimens………..….12
3.5Bactericidal activity as loss of recoverable CFU after exposure of S. mutans inoculated agar surfaces to defined atmospheres of ozone .……..….………...….15
3.6Influence of ozone exposure of S. mutans suspended in liquid in microtiter plate wells on bacterial viability.…………..………..….16
3.7Effect of ozone in S. mutans suspended in media in exposure times of 1, 2, 3 and 4 min……….18
3.8Effect of ozone in S. mutans suspended in media in concentrations of 106, 105, 104
and 103 for 1 min ………..………..………..….19
3.9Effect of ozone in S. mutans suspended in media and on agar under controlled conditions ……….…..…...21
4. RESULTS………...…..22
4.1 Effect ozone in S. mutans on human dental specimens………...…….……….22
4.2 Effect ozone in S. mutans on bovine dental specimens……….………22
4.3 Effect ozone in S. mutans suspended in media under controlled conditions ………..………..…23
4.4 Effect ozone in S. mutans suspended in media for 15, 30, 45 and 60 s……….………24
4.5 Effect ozone in S. mutans suspended in media for 1, 2, 3 and 4 min..……….….…24
4.6 Effect ozone in S. mutans suspended in media in concentrations of 106, 105, 104 and 103 ..……….…….24
4.7 Effect ozone in S. mutans in media and on agar……….……..25
5. DISCUSSION………..………..….………...26
6. CONCLUS IONS.……….…………..…….………..….35
7. TABLES……...………….……….………....36
8. FIGURES…….………….……….………..…..44
APPENDICES……..………….……….……… …....54
REFERENCES………..……….……….………...….55
LIST OF TABLES
Table
1. Indication of the ozone therapy in medicine……….………...29
2. Number of bacteria recovered after the different treatment
protocols applied with the Kavo Curozone X4® ozone generator
to human dentin specimens for 60 s (log10 CFU)……….………….……….30
3. Number of bacteria recovered after the different treatment
protocols applied with the Kavo Curozone X4® ozone generator
to bovine dentin specimens for 60 s (log10 CFU)…….…….……….………..31
4. Number of bacteria recovered and killing rates after exposing
S. mutans on agar (log10 CFU/ml) to ozone in the Modular Incubator Chamber at different concentrations for 4 min in
covered and uncovered Petri dishes..………....…..….32
5. Bacterial growth as optical density (mO.D. at λ610 nm)
attained following incubation at 37oC for 18 hr after the
different treatment protocols applied with the Kavo Curozone X4®
ozone generator on 10l of 106 CFU/ml of S. mutans………….….….…..…33
6. Bacterial growth as optical density (mO.D. λ610 nm)
attained following incubation at 37oC for 18 hr after the
different treatment protocols applied with the Kavo Curozone X4®
ozone generator on 10l of 106 CFU/ml of S. mutans…...34
7. Bacterial growth as optical density (mO.D. λ610 nm)
attained following incubation at 37oC for 18 hr after the
different treatment protocols applied with the Kavo Curozone X4®
ozone generator on 10l of a bacteria titration from
106 to 103 CFU/ml of S. mutans…………..……….…….35
8. Bacterial growth as optical density (mO.D. λ610 nm)
recovery in media and recovery (log10 CFU/ml) on agar
attained following incubation at 37oC for 18 hr after the
different treatment protocols applied with the ozone generator OL80W in the Modular Incubator Chamber
at 2000 ppm for 4 min………..36
LIST OF FIGURES
Figure
1. Curozone X4®………...………37
2. Curozone X4schematic functioning………..………...38
3. OL80A Ozone generator. ………...………..…41
4. Mouse Exposure Chamber …...………....42
5. OL80W Ozone generator. .………….……….….43
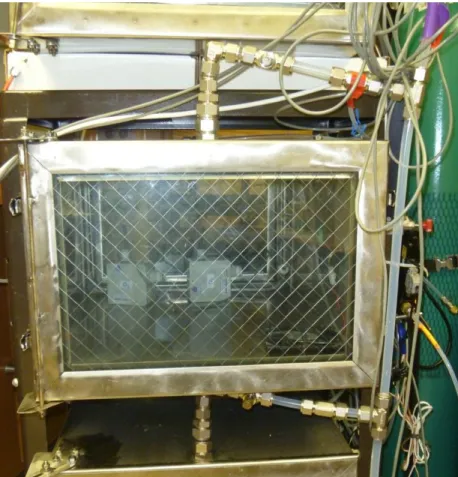
6. Modular Incubator Chamber …..…..……….………...44
7. Human root specimen………..….……...39
8. Bovine root specimen……….……..40
9. 96 well microtiter plate………...….……45
10. Experiment 10 sample distribution……….….…46
LIST OF ABBREVIATONS
S. mutans: Streptococcus mutans E. faecalis: Enterococcus faecalis S. sobrinus: Streptococcus sobrinus L. acidophilus: Lactobacillus acidophilus L. casei: Lactobacillus casei
A. naeslundii: Actinomyces naeslundii V. dispar: Veillonella dispar
F. nucleatum: Fusobacterium nucleatum S. oralis: Streptococcus oralis
C. albicans: Candida albicans S. aureus: Staphylococcus aureus E. coli: Escherichia coli
B. atrophaeus: Bacillus atrophaeus
mg/L: Milligrams per liter
mO.D.: Millioptical density
ppm: Parts per million
TSA: Trypticase soy agar
TSB: Trypticase soy broth
V. dispar: Veillonella dispar
l: Microliter
1. Introduction
Since the 1970’s there has been a significant reduction in dental caries in
industrialized countries for children and adolescents, due to environmental and educational
factors such as the increased use of fluoride in public water supplies, dentifrices and dental
products; improved oral hygiene and prophylaxis; dietary counseling; and increased access to
dental care.1 Nevertheless, dental caries is still a common disease, experienced by almost 80%
of children by the age of 18 and by almost 90% of adults.1
Dental caries is a multifactorial disease, characterized at the tooth level by a dynamic
imbalance of the demineralization/remineralization processes over time2. The mineral content
of the tooth is sensitive to increases in acidity. For enamel surfaces, when the pH drops below
5.5 demineralization proceeds faster than remineralization resulting in a net loss of mineral
structure. Carious lesions are caused by bacterial fermentation of dietary carbohydrates into
acids (principally lactic acid) within the dental biofilm. If the acid production and
accumulation exceeds the buffering capacity of the oral environment, demineralization
occurs eventually leading to cavitation.2
Dental biofilm is a key requirement for carious lesions to develop. Dental biofilm
results from adherence of oral microorganisms to and growth onto the tooth surface. When
is lowered, acids diffuse rapidly into the underlying enamel or dentin.3 The two most
important groups of bacteria that predominantly produce acids are the mutans streptococci
(Streptococcus mutans and Streptococcus sobrinus) and the lactobacilli.3 These acidogenic bacteria metabolize a variety of fermentable, dietary carbohydrates to lactic acid, the strongest
naturally occurring acid produced by acidogenic bacteria during the caries process.3
Dental caries may have a significant impact on an individual’s life. The most common
consequences of untreated lesions are discomfort and pain.4 Restorative dental treatments can
now be provided pain free, apart from the pain of the local anesthetic injection. However, for
some people restorative treatments are associated with fear and anxiety, which may become
barriers to dental attendance as well as financial limitations.4 Treatment avoidance can
subsequently lead to further progression of caries lesions which, in turn, may cause more
distress and long-term complications4. Gross decay may lead to disturbances in eating and
sleeping patterns because of pain. Psychological distress can arise from the embarrassment
and self-consciousness of having missing or decayed teeth, especially in the anterior
dentition.4
According to the anatomical location of carious lesions, it is possible to differentiate
between coronal lesions, which may affect the pits and fissures or the smooth surfaces of a
tooth in enamel, and root lesions, which affect the exposed root surface in dentin.
The prevalence of root caries begins at about 30–40 years of age and tends to increase
thereafter. Adults are keeping their teeth longer however, increased retention of teeth means
that more adults are at risk for root caries. Gingival recession caused by aging puts root
surfaces especially at risk. Among dentate adults, the prevalence of root caries experience is
about 8 times higher among those aged 75+ years (55.9%) compared to those aged 18 to 24
years (6.9%).5
Ozone has been proposed as a therapeutic agent for dental caries.6-18 Ozone (O3) is a
triatomic molecule, consisting of three oxygen atoms with a molecular weight of 47.98 g/mol.
Ozone is a highly thermodynamically unstable compound that, dependent on system
conditions such as temperature and pressure, decomposes to pure oxygen with a short
half-life.19 Ground-level ozone is an air pollutant with harmful effects on the respiratory system.
Ozone in the upper atmosphere filters potentially damaging ultraviolet light from reaching the
Earth’s surface.19
The word ozone was first introduced by Schonbein in 1840. He subjected
oxygen to electrical discharges and noted “the odor of electrical matter”. Schonbein
concluded that odor was due to a gas which he named ozone, from the Greek Ozein, which
means smell.6
Ozone, in the gaseous or aqueous phase, has been shown to be a powerful
antimicrobial agent against bacteria, fungi, protozoa, and viruses.20 It is generally accepted
that the strong oxidizing potential of ozone initiates the destruction of cell walls and
cytoplasmic membranes of bacteria and fungi. 12, 21 During this process, ozone reacts with
glycoproteins, glycolipids, and select amino acids resulting in inhibition of the enzymatic
control systems of the cell. This inhibition results in a collapse in the permeability barrier
function of the membrane, permitting the ready diffusion of ozone and other toxic molecules
into the cell resulting in microbial death. 21 Ozone can attack many biomolecules, especially
the cysteine, methionine, and histidine amino acid residues of proteins. By oxidizing critical
biomolecules associated with the etiology of dental caries, ozone can have disruptive effects
on the cariogenic processes of bacteria.21 For example, ozone is capable of decarboxylation of
pyruvic acid to the weaker acetic acid. It has been shown that remineralization of incipient
carious lesions can be encouraged when the production of acetic acid, or other high pKa acids
found in resting biofilm, buffers plaque fluid.21
The water industry has used ozone to kill microorganisms for many years.22 One of the
most common uses of ozone is treating drinking water for disinfection; oxidation of natural
organic matter; degradation of hazardous micropollutants; algae inactivation; improvement of
color, taste, and odor of water.23
Ozone has also been tested in medicine to decontaminate hospital side rooms, rooms
contaminated with methicillin-resistant S. aureus and in auto-hemotherapy.23 Ozone has been
used in the medical field for over 150 years to disinfect and treat infections, wounds and
multiple diseases (Table 1).24 Some of the contraindications for the ozone therapy are acute
alcohol intoxication, recent myocardial infarction, hemorrhage from any organ, pregnancy,
hyperthyroidism, thrombocytopenia and ozone allergy.19
The first use of ozone in dentistry is attributed to Dr. E. Fisch who used ozonated
water in his practice;21 and Dr. Erwin Payr used it in surgery and reported his results at the
59th Congress of the German Surgical Society in Berlin (1935).21 In dental surgery, ozonated
water was used to promote hemostasis, enhance local oxygen supply, and inhibit bacterial
proliferation.21 Theoretically, ozone in either gas or ozonated water forms, can reduce the
bacterial count in biofilm as well as in active carious lesions, and therefore it may temporarily
arrest the progression of caries, resulting in prevention of or delaying the need for tooth
restorations.21 In the dental field, ozone has been advocated for treatment in endodontics,
ozonated oils as medicaments, root and cavitated caries and for its potential application in
reducing bacterial counts in dental unit water delivery systems.15 Cesar et al. (2012) tested
the effectiveness of ozonated water for disinfection of the surfaces of dental diamond burs
that were contaminated with Eschericia coli, Staphylococcus aureus, Candida albicans, or the
spores of Bacillus atrophaeus. They found that ozonated water effectively reduced the
number of CFU/mL in an exposure of 10 or 30 min at a concentration of 10 mg/L for all
microorganisms.25
There is evidence that ozone can effectively kill microorganisms on surfaces26, 27 but
the evidence that ozone effectively kills microorganism in biofilm is contradictory. There are
reports that ozone is effective in short-time exposures (10 seconds),11, 13 while other studies
have shown its effectiveness in short20 and longer exposures (over 60 seconds).28 There are
also other authors who claim that ozone applied as gas has no effect on biofilm.22, 29, 30 Many
authors claim ozone has an anticariogenic effect not only in vitro11, 13, 14, 20 but also in vivo, and clinically by reducing the number of cariogenic bacteria in the oral cavity reversing the
caries process in existing lesions.7, 10-12 Saini (2011) advocates the use of ozone as an
anticariogenic agent.31 It has been suggested that the application of ozone, as an adjunct
therapy in association with a remineralizing agent, could arrest or reverse carious lesions,
providing an alternative to restorative treatment.7, 8, 10, 11 Using ozone to reduce the bacterial
count in active carious lesions might temporarily modify the biofilm allowing the arrestment
of caries lesions11. This could prevent or delay the need for restorative procedures. The
clinical protocol for application of ozone is purportedly fast and easy. It has been proposed
that the application of 10 to 60 seconds of ozone could reduce the number of most of the
microorganisms in leathery (active) root caries lesions.4 These studies report that ozone acts
rapidly and at lower concentrations than those required for chlorine, and has no side-effects
such as taste and odor which are characteristic of other disinfectant agents.4 Once the
ecological niche of the acid-producing microorganisms has been reduced or eradicated, the
area is treated with a remineralizing solution. It has been suggested that for clinical treatment
the ozone exposure be repeated at 3 and 6 months after the initial application.12
Knight et al. in 2008 found that the infusion of ozone into non-carious dentin
prevented biofilm formation in vitro from S. mutans and L. acidophilus over a four-week
period. It has been hypothesized that ozone treatment might alter the surface wettability of
dentin through reaction with organic constituents leading to a delay in bacterial colonization.14
In contrast several publications report negative results both in vitro22, 29, 30, 32 and in
clinical trials.33 Two systematic4, 21 and one Cochrane review34 agree in “given the high risk of
bias in the available studies and lack of consistency between different outcome measures,
there is no reliable evidence that application of ozone gas to the surface of carious teeth stops
or reverses the caries process. There is a fundamental need for more evidence of appropriate
rigor and quality before the use of ozone can be accepted into mainstream primary dental care
or can be considered a viable alternative to current methods for the management and
treatment of dental caries”.34
The publication by Brazzelli et al. concluded that the current
evidence base for ozone is insufficient to say that ozone is a cost-effective addition to the
management and treatment of occlusal and root caries4. Before expensive and
time-consuming independent randomized clinical trials are performed, well-controlled in vitro
proof of concept study showing that ozone kills cariogenic bacteria are needed.
Hems et al. in 2005 showed the inability of gas ozone to effectively kill E. faecalis
after a 240 s exposure; stating that “gaseous ozone had no significant antibacterial effect on
the biofilms. This was predictable considering that the effectiveness of ozone is highest in
solution and given the previous results with biofilms, gaseous ozone would not be expected to
exert any great antibacterial effect”. They state that “Ozone is a selective oxidant and affects
only certain compounds but when it dissolves in water, it becomes highly unstable and rapidly
decomposes through a complex series of chain reactions”.22 Consequently, there is a
fundamental need for more evidence that ozone can be accepted into mainstream primary
dental care and be considered a viable alternative as adjunctive treatment of dental caries.
2. Objectives
1. To develop a mechanical model that simulates a “lesion” in dentin as a surface for
reproducible recovery of inoculated bacteria to test efficacy of ozone delivery to target
bacteria in a relevant environment.
2. To treat that lesion model with ozone to simulate clinical conditions.
3. To determine the conditions and circumstances where ozone can have a killing effect
on S. mutans (concentration, exposure time, bacteria on surface or in media)
4. To investigate if ozone can be effectively delivered to a caries lesion to kill S. mutans.
5. To determine if S. mutans can be killed by ozone where the concentrations are
validated.
3. Materials and methods
3.1 Bacterial species and culture
The bacterial species used in this study was Streptococcus mutans strain ATCC 10449
(serotype c).
A stock culture of the bacteria was transferred to Wilkins-Chalgren broth media (WC,
Difco Laboratories. Sparks) and then incubated at 37°C in aerobic (ambient) atmosphere.
After 24 hours, an aliquot of this culture was inoculated to a fresh W-C tube, to an
approximate concentration of 108 colony forming units (CFU) /ml using McFarland standards
(equivalent to ~108 CFU/ml).
3.2 Ozone generators
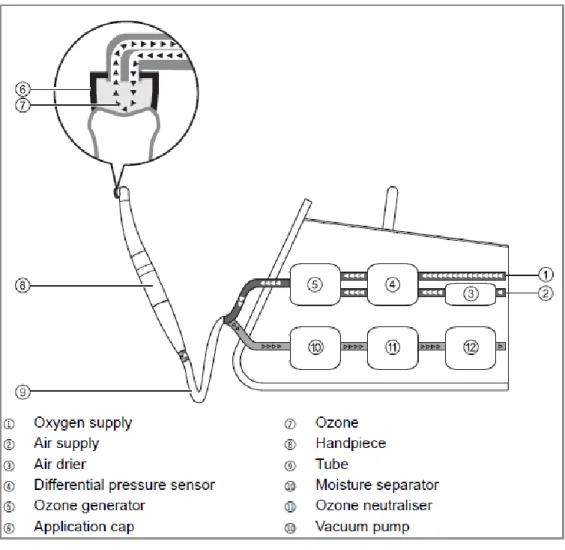
The ozone generator used for this study was the Curozone X4® (Kavo, Biberach/Riß,
Germany) generator (Fig. 1). The device is designed to generate ozone either using
atmospheric oxygen or with supplemental oxygen delivered with an attached oxygen tank to
yield higher ozone concentration. According to the manufacturer the generated ozone
concentration is 2100 ppm, ±10%, delivering 65µmol ozone/min. The exposure time can be
set from 5 to 60 sec. The ozone is delivered through a hand-piece fitted with disposable
silicone tips of variable sizes as appropriate to the treatment surface, designed to seal the
surface, otherwise the device stops working. After the exposure time there is a two sec
vacuum/ scrubbing cycle to eliminate any remaining ozone in the system thus preventing
escape of ozone to the ambient atmosphere (Fig. 2).
The ozone generator OL80A (Ozone Services, Yanco Industries, Burton, BC). (Fig.
3), was used to expose the bacteria in the Mouse Exposure Chamber (ESE Design Center,
Department of Environmental Sciences and Engineering, Gillings School of Global Public
Health. University of North Carolina at Chapel Hill) (Fig. 4) to atmospheres of either 2 or 20
ppm of ozone. The OL80W (Fig. 5, located at the Environmental Sciences and Engineering
Laboratory located at Gillings School of Global Public Health at the University of North
Carolina at Chapel Hill) was used to expose the bacteria in the Modular Incubator Chamber
(Billups-Rothenberg, Inc. Del Mar, CA) (Fig. 6) to atmospheres of either 200 or 2000 ppm of
ozone.
3.3 Effect of ozone on human dental specimens.
Thirty-six extracted human third molars were used as dental specimens. The teeth
were debrided and examined to ensure that they were free of defects (caries, fractures,
cracks). The crowns were separated from the roots using an Isomet diamond saw (Buehler
Ltd., Lake Bluff, IL) under running water to obtain 6 x 4 mm slabs. The specimens were
ground mechanically (Ecomet 3, Buehler Ltd.) under running water using a 600-grit silicon
carbide (SiC) paper to obtain flat dentin surface (Fig. 7). Single preparations were made on
the specimens with a #2 bur at high speed with water refrigeration to create a cavity of 1 mm2
that would harbor bacteria; they were then sterilized with steam autoclave. The specimens
were then inoculated with serial ten-fold dilutions of the bacteria culture 108 to 106 CFU/ml
and incubated at 37°C for 24 hours. The specimens were exposed to ozone generated by the
Curozone X4® which produces concentrations up to 2100 ppm, according to the manufacture.
This was accomplished using the Curozone handpiece fitted with 3 mm silicone tips. This
completely surrounded the “inoculated lesion”, creating a sealed ozone atmosphere at the
treatment site. Fresh tips were used with each treatment to prevent cross-contamination. The
treatment timing was begun automatically by the instrument once the desired ozone
atmosphere was achieved.
The specimens were randomly divided in three groups: (n=12)
1. Low ozone group: Exposed to ozone generated using ambient air for 60 seconds.
2. High ozone group: Exposed to ozone generated using pure oxygen for 60 seconds.
3. Control group: Exposed to ambient air for 60 seconds.
After the exposure to air or ozone, dentin shavings were collected from the
circumferential cavity walls to a 1.4 mm depth into 1 ml sterile bacterial transport media
containing glass beads to facilitate dispersion of the bacteria clumps with vortexing, by using
sterilized #4 carbide burs at low speed (NSK Ultimate 450K, Nakanishi Inc. Japan). A new
sterile bur was used for each specimen to prevent over heating of dentinal walls and cross-
contamination.
Serial ten-fold dilutions of the vortexed transport media were used to determine the
bacteria counts from the dentin shavings obtained. The diluted solutions were spiral plated
(Spiral Systems Inc., Cincinnati, OH) on Trypticase™ Soy Agar with 5% Sheep Blood.
(Becton, Dickinson and Company. Sparks, MD). After 24 hours of incubation at 37°C, the
resulting colonies were counted using a ProtoCol automatic plate counter (Spiral Systems
Inc., Cincinnati, OH) and Protocol software. Data were calculated as CFU/ml of the original
transport medium. To normalize the CFU/ml, descriptive statistics (means and standard
deviations) were performed on log transformed data.
3.4 Effect of ozone on bovine dental specimens
Thirty six extracted bovine teeth were used. The teeth were debrided and examined to
ensure that they were free of defects (caries, fractures, cracks). The crowns were separated
from the roots using an Isomet diamond saw (Buehler Ltd., Lake Bluff, IL) under running
water to obtain 10 x 6 mm slabs. The specimens were ground mechanically (Ecomet 3,
Buehler Ltd.) under running water using a 600-grit SiC paper to obtain a flat dentin surface,
(Fig. 8). Single preparations of 1.4 mm2 were made on the specimens with a #4 bur at high
speed with water refrigeration to create a cavity that would harbor bacteria. They were then
sterilized with steam autoclave. The specimens were then inoculated with ten fold dilutions of
the bacteria culture 108 to 106CFU/ml and incubated at 37°C for 24 hours.
The results of Experiment 1 show that the recovered log10 CFU obtained from low
ozone, high ozone and control groups did not differ significantly among the three groups
results. It was therefore decided to compare the results of the two test groups: high ozone and
low ozone delivered using handpiece of the Curozone X4® fitted with 3 mm silicon tips as
described above for the human teeth.
The specimens were randomly divided in two groups: (n=18)
1. Low ozone control group: Exposed to ozone generated using ambient air for 60
seconds.
2. High ozone: Exposed to ozone generated using pure oxygen for 60 seconds.
After the exposure to ozone generated from ambient air or using pure oxygen, dentin
shavings were collected from the circumferential cavity walls of diameter to 1.8 mm depth
into 1 ml sterile bacterial transport media containing glass beads to facilitate dispersion of the
bacteria clumps with vortexing, sterilized #6 carbide burs at low speed. A new sterile bur was
used to prevent over-heating of dentinal walls and cross-contamination.
Serial ten-fold dilutions of the vortexed transport media were used to determine the
bacteria counts from the dentin shavings obtained. The solution was spiral plated on
Trypticase™ Soy Agar with 5% Sheep Blood (WC, Difco Laboratories. Sparks). After 24
hours of incubation at 37°C, the resulting colonies were counted using a ProtoCol automatic
plate counter and Protocol software as described above.
3.5 Bactericidal activity as loss of recoverable CFU after exposure of S. mutans inoculated agar surfaces to defined atmospheres of ozone
After showing the inability of the Curozone X4 to effectively inhibit S. mutans on
human and bovine roots at purported levels of ozone of 2100 ppm for 1 min, it was decided to
determine if the target strain of bacterium (S. mutans ATCC 10449) is, in fact, susceptible to
ozone. To optimize delivery to the target, the bacteria were spread on a Trypticase™ Soy
Agar with 5% Sheep Blood surface to allow uniform delivery of ozone in a contained
atmosphere. These inoculated plate surfaces were treated by directly exposing the uncover
plates to specific ozone atmospheres. Determination of the effective killing dose of ozone was
accomplished by varying the exposure atmosphere to include 2, 20, 200 and 2000 ppm of
ozone for 4 min under laboratory conditions using a different ozone generator. In addition, the
2 and 20 ppm groups were tested with the Petri dish covers in place to determine if the cover
would be a physical barrier to ozone access to the inoculated surface.
The experiments were performed under defined conditions at the Environmental
Sciences and Engineering Laboratory located in the Gillings School of Global Public Health
at the University of North Carolina at Chapel Hill.
To determine the bactericidal activity of ozone, an overnight culture (early
exponential) of S. mutans was adjusted to a suspension of 106 CFU/ml and 49.2 l was spiral
plated to replicates of seven SBA plates. Six plates were treated by varied exposures to
atmospheres of ozone and one was left untreated as control. The 2000 and 200 ppm ozone
atmosphere groups were exposed using the OL80A ozone generator into the Modular
Incubator Chamber. The 2 and 20 ppm ozone atmosphere groups were exposed either with or
without the Petri dish cover in place using the OL80W ozone generator into the Mouse
Exposure Chamber. The larger size of this chamber permitted the simultaneous treatment of
multiple plates in a single plane.
The distribution of the groups was as follows:
1. Uncovered replicate plate exposed to 2000 ppm of ozone for 4 min
2. Uncovered replicate plate exposed to 200 ppm of ozone for 4 min
3. Uncovered replicate plate exposed to 20 ppm of ozone for 4 min
4. Replicate plate exposed to 20 ppm of ozone for 4 min with the Petri dish cover in
place to determine if the cover would be a physical barrier to ozone
5. Uncovered replicate plate exposed to 2 ppm of ozone for 4 min
6. Replicate plate exposed to 2 ppm of ozone for 4 min with the Petri dish cover in
place to determine if the cover would be a physical barrier to ozone
7. Untreated replicate plate as a control for determining recoverable CFU.
Following treatments the replicate plates were incubated in an anaerobic chamber
(10% H2 – 5% CO2 – 85% N2) at 37°C for 18 hours to permit development of the CFU. After
this period the resulting CFU were counted using a ProtoCol automatic plate counter. The log
transformed data were treated as described above. The experiments exposing uncovered plates
to the various atmospheres were repeated on three independent occasions. Treatment of
covered plates with 2 and 20 ppm ozone atmosphere was only done once.
3.6 Influence of ozone exposure of S. mutans suspended in liquid in microtiter plate wells on bacterial viability.
Our previous experiments with S. mutans in the artificial cavity preparations in either
human or bovine dentin slabs determined that exposure to ozone delivered directly with the
hand piece did not result in demonstrable reduction in viability of the bacteria target even at
the highest concentration (2,100 ppm) for up to 60 sec. Longer treatments were technically
challenging with the small dentin slabs and there relatively irregular surfaces. It was also
possible that the failure to kill was due to the competitive inactivation of the ozone by the
dentin. The aqueous environment of the suspended bacteria in the “cavity” could also have
limited accessibility of the ozone to the target bacteria. In the next set of experiments, a more
uniform approach for testing the effects of ozone atmospheres on the viability of S. mutans in
an aqueous environment was sought. It was determined that the 3 mm silicone tip fit formed a
tight seal with the well of a 96-well microtiter plate. This permitted the creation of individual
ozone atmospheres in the micro-format of each well. A liquid volume containing the target
bacteria could be uniformly delivered to the bottom of each well and exposed to a define
ozone atmosphere. After exposure the treated bacteria could be resuspended in culture
medium and incubated to permit growth. Total killing of the bacteria would result in a failure
to grow (no change in optical density). Logarithmic killing of the bacteria would result in
delays in attaining discernible growth and consequent reductions in attained optical densities
when compared to untreated controls. The effectiveness of Curozone X4® on bacteria
suspended in liquid was therefore tested by comparing the post-treatment growth as optical
density (mO.D.at λ610 nm) 18 to 24h after exposure to 15, 30, 45 and 60 seconds of ozone
with that of untreated controls.
A 96-well microtiter plate (Fig.9) was used to receive ten microliter (l) of 106
CFU/ml of bacteria to be treated with ozone through the Curozone X4®unit using a 3 mm
silicone tip in high and low ozone modes. The controls consisted of two groups of 200l of
media without bacteria, one group was treated for 1 min and the other was left untreated. The
positive control was 10l of the bacteria culture that was not treated.
Each bacteria and control group, with the exception of the untreated media group, was
divided in 2 groups of 4 wells each. One received the low ozone treatment and the other high
ozone treatment.
The group distribution was as follows:
1. Media untreated. 200l.
2. Media treated for 1 min. 200l.
3. Bacteria untreated. 10l of 106 CFU/ml.
4. Bacteria treated for 15 sec. 10l of 106 CFU/ml..
5. Bacteria treated for 30 sec. 10l of 106 CFU/ml.
6. Bacteria treated for 45 sec. 10l of 106 CFU/ml.
7. Bacteria treated for 60 sec. 10l of 106 CFU/ml.
After treatment, the 10l aliquots of bacteria were resuspended in 200l of fresh W-C
medium broth and incubated in an anaerobic chamber at 37oC. The optical densities (λ610
nm) of the quadruplicate samples were determined after 18 hours by using a Vmax kinetic
microplate reader and companion SoftMax Pro 3.1 software (Molecular Devices, Sunnyvale
CA). Data were expressed as mOD and means and standard deviations determined on
replicate wells. Each experiment was independently repeated at least three times.
3.7 Effect of ozone in S. mutans suspended in media in exposures times of 1, 2, 3 and 4 min
This experiment was designed to determine ozone effectiveness on bacteria in media
after different exposures times ranging from 1 to 4 min.
A 96 well microtiter plate was used to receive ten microliter (l) of 106 CFU/ml of
bacteria to be treated with ozone through the Curozone X4® unit using a 3 mm silicone tip in
high and low ozone modes in exposures time of 1, 2, 3 and 4 min. The controls consisted of
two groups of 200 l of medium without bacteria, one group was treated for 1 min and the
other was left untreated. The positive control was 10l of the bacteria culture that was not
treated.
Each bacteria and control group, with the exception of the untreated media group, was
divided in 2 groups of 4 wells. One received the low ozone treatment and the other high ozone
treatment.
The group distribution was as follows:
1. Media untreated. 200l
2. Media treated for 1 min. 200l
3. Bacteria untreated 10l of 106 CFU/ml.
4. Bacteria treated for 1 min. 10l of 106 CFU/ml.
5. Bacteria treated for 2 min. 10l of 106 CFU/ml.
6. Bacteria treated for 3 min. 10l of 106 CFU/ml.
7. Bacteria treated for 4 min. 10l of 106 CFU/ml.
After treatment, the 10l aliquots of bacteria were resuspended in 200l of fresh W-C
medium broth and incubated in an anaerobic chamber at 37oC. The optical densities (λ610
nm) of the quadruplicate samples were determined after 18 hours by using a Vmax kinetic
microplate reader and companion SoftMax Pro 3.1 software (Molecular Devices, Sunnyvale
CA).
3.8 Effect of ozone in S. mutans suspended in media in concentrations of 106, 105, 104 and 103 for 1 min
This experiment was designed to determine ozone effectiveness on titrated bacteria in
concentration of 106,105,104 and 103 CFU/ml in media for 1 min.
This experiment was designed to determine ozone effectiveness on titrated bacteria in
concentration of 106,105,104 and 103 CFU/ml in media for 1 min. A 96 well microtiter plate
was used to receive ten microliter (l) of 106 CFU/ml of bacteria to be treated with ozone
through the Curozone X4®unit using a 3 mm silicone tip in high and low ozone modes. The
controls consisted in two groups of 200 l of media without bacteria, one group was treated
for 1 min and the other was left untreated. The positive control was 10l of the bacteria
culture that was not treated.
Each bacteria and control group, with the exception of the untreated media group, was
divided in two groups of four wells. One received the low ozone treatment and the other high
ozone treatment.
The group distribution was as follows:
1. Media untreated. 200l
2. Media treated. 200l
3. Bacteria untreated 10l of 106 CFU/ml.
4. Bacteria treated for 1 min. 10l of 106 CFU/ml.
5. Bacteria treated for 1 min. 10l of 105 CFU/ml.
6. Bacteria treated for 1 min. 10l of 104 CFU/ml.
7. Bacteria treated for 1 min. 10l of 103 CFU/ml.
After treatment, the 10l aliquots of bacteria were resuspended in 200l of fresh W-C
medium and incubated in an anaerobic chamber at 37oC. The optical densities (λ610 nm) of
the quadruplicate samples were determined after 18 hours by using a Vmax kinetic microplate
reader and companion SoftMax Pro 3.1 software (Molecular Devices, Sunnyvale CA).
3.9 Effect of ozone in S. mutans suspended in media and on agar under controlled conditions
The ozone generator OL80W was used to expose the bacteria in the Modular
Incubator Chamber at Environmental Sciences and Engineering Laboratory located at Gillings
School of Global Public Health at the University of North Carolina at Chapel Hill.
This experiment was designed to test the effectiveness of exposing S. mutans in media
and on a surface to ozone gas, at the same time for four min in an atmosphere of 2000 ppm
ozone. To accomplish this objective two groups were designed:
Media Group: A total of 15 wells of a 96 well microtiter plate were inoculated with
10l of 103 CFU/ml. Five wells were inoculated with 200l of media serving as controls.
(Fig.10). Two sets were prepared one was treated and the other left untreated as control.
Agar Group: For this group two agar plates with 49.2l from a culture 106 CFU were
spiral plated on Trypticase™ Soy Agar with 5% Sheep Blood. One was treated with ozone
and the other left untreated as control.
After being exposed to ozone at 2000 ppm for four min, the 10l suspension of the
treated bacteria in the media group was brought to a volume of 210l with fresh W-C medium
and incubated in an anaerobic chamber at 37oC. The optical densities (λ610 nm) of the
quadruplicate samples were determined after 18 hours by using a Vmax kinetic microplate
reader and companion SoftMax Pro 3.1 software (Molecular Devices, Sunnyvale CA).
4. Results
4.1 Effect ozone in S. mutans on human dental specimens
Results are presented in Table 2. The The mean recoverable CFU/ml obtained from
low ozone (5.25 ± 0.87), high ozone (5.47 ± 0.92) and control (5.58 ± 0.67) groups did not
differ significantly among the three groups. (Kruskal-Wallis test, p=0.58).
During the experiment it was noticed the handling difficulties of the Curozone X4®,
keeping the seal of the silicone tip turn to be problematic, changings in pressure and holding
angle of the hand-piece lead to seal loss, also the irregularities of the tooth surface made the
dentin shaving proccess challenging. Due to this inconvenient it was decided to utilize bovine
teeth to minimize the mechanical problems found with human teeth.
4.2 Effect ozone in S. mutans on bovine dental specimens
Results are reported in Table 3. There was no statistically significant difference
between the mean of recovered log10 CFU obtained from low ozone control (5.37 ± 0.71) and
high ozone (5.32 ± 0.82) (Wilcoxon test, p=0.53).
Having a larger tooth surface did not prevent the mechanical problems explained in
Curozone X4® is not delivering ozone to the lesion site in a concentration that is sufficient to
kill or that the test bacterial strain is inherently resistant to ozone. A different approach is
proposed, to test the antibacterial effect of ozone under control conditions at the
Environmental Sciences and Engineering Laboratory located at Gillings School of Global
Public Health at the University of North Carolina at Chapel Hill.
4.3 Effect ozone in S. mutans suspended in media under controlled conditions
Results are reported in Table 4.The plates exposed to 2000 and 200 ppm had no
recoverable colony forming units (total inhibition). The 20 ppm group that was left uncovered
showed 99.99% bacteria inhibition (1.59 log10 CFU/ml recovered), while the covered group
showed 99% bacteria inhibition (3.55log10 CFU/ml recovered). The 2 ppm group that was left
uncovered showed 99.99% bacteria inhibition (2.81 log10 CFU/ml recovered), while the
covered groups showed 91.41% bacteria inhibition (4.58 log10 CFU/ml recovered). The
untreated control group showed a bacteria value of 5.64 log10 CFU/ml. Logarithmic
reduction in recoverable CFU greater than 1 compared to control was considered significant.
These results show the antibacterial effect of ozone on S. mutans while spread on a
surface, during the test another agar plate was spot assay with 10l of a titration of S. mutans,
L. acidophilus and E. faecalis from 109 to 103 and exposed to ozone at 2000 ppm for 4 min, resulting in complete killing of the bacteria. This experiment was made in collaboration with
Dr. Marcos Ximenes.
A new experiment for the Curozone X4® is designed. The tooth model could bring
limitations in the recovery of the treated bacteria which can diffuse through the dentin tubules
and become unreachable to ozone; in this approach a 96 microtiter well was used to avoid the
bacteria recover process with the tooth model.
4.4 Effect ozone in S. mutans suspended in media for 15, 30, 45 and 60 s
Results are reported on Table 5. No killing was observed. Bacteria counts are not
different among the high ozone and low ozone groups (Wilcoxon rank sum test, p=0.42).
Being unable to reduce the bacteria recover in different exposure times a new
experiment was run increasing the time for 1, 2, 3 and 4 min.
4.5 Effect ozone in S. mutans suspended in media for 1, 2, 3 and 4 min
Results are reported on Table 6. No killing was observed. Bacteria counts are not
different among the high ozone and low ozone groups but they are significantly different
compared to media control groups (Wilcoxon rank sum test, p=0.53).
Being unable to reduce the bacteria recover in exposures up to 4 min, a new
experiment was designed titrating the bacteria concentration one log from 106 to 103.
4.6 Effect ozone in S. mutans suspended in media in concentrations of 106, 105, 104 and 103
Results are reported on Table 7. No killing was observed. Bacteria counts are not
different among the high ozone and low ozone groups but they are significantly different
compared to media control groups (Wilcoxon rank sum test, p=0.56).
These results demonstrate the inability of the Curozone X4® to effectively reduce the
CFU/ml of bacteria on suspension. A new experiment testing the ozone effect under control
conditions was run exposing bacteria in a microtiter plate and a spiral plate and the same time
to 2000 ppm for 4 min.
4.7 Effect ozone in S. mutans in media and on agar
Results are shown on Table 8. The bacteria density of the treated (424 mO.D. λ610
nm) and untreated group (432 mO.D. λ610 nm) showed no bacteria killing.
For the agar group, the plate that was treated with ozone gas showed 100% bacteria
inhibition, the untreated control group showed 5.63 log10 CFU/ml. Bacteria counts are
different among the 3 mutually exclusive groups of non-treated, ozone treated, treated media.
(Wilcoxon. p<.0001).
5. Discussion
The association between plaque levels of S. mutans and caries is well described35-38 .
Bowden et al (1990) found the strongest association when plaque was removed from single
occlusal fissures. Seventy-one percent of the carious fissures had S. mutans accounting for
more than 10% of the viable flora, whereas 70% of the fissures that were caries free had no
detectable S. mutans. Sixty-five percent of the pooled plaque samples from the children with
rampant caries had S. mutans accounting for more than 10% of the viable flora, whereas 40%
of the pooled samples from children that were caries free had no detectable S. mutans35.
Therefore methods to eliminate or inhibit S. mutans in the oral cavity must be the main
objective in caries prevention. Ozone is considered a strong oxidizer of the cell walls and
cytoplasmatic membranes of bacteria and is considered a potent bactericidal, antiviral, and
antifungal agent39. It is important to point out that this statement is based on the use of ozone
in blood not gassing ozone to a microfilm.39, 40 This is a common finding in the literature,
extrapolating the use and effect of systemic ozone dissolving it in the bloodstream, to the
dental field.18, 39 These articles explain the indications and mechanism of action of ozone
dissolved in blood but there is no reference to the effect in the oral cavity. Therefore the real
ability of ozone to kill cariogenic bacteria is yet to be determined.
grow to form biofilms. Biofilms have been defined as matrix embedded microbial
populations, adherent to each other and/or to surfaces or interfaces.2, 41, 42 This is especially
true in the oral cavity which is permanently in wet conditions. One property of biofilms is the
protection from host defenses, desiccation etc. by production of extracellular polymers to
form a functional matrix2 this is a key factor understanding the effect of antimicrobial agents,
they have to be able to reach the bacteria through the biofilm. There is evidence that bacteria
living in biofilms as dental plaque on tooth surfaces are generally more resistant to
antimicrobial agents than bacteria in batch culture normally used for “in vitro” susceptibility
testing43. The bacteria culture used in this study was grown in a sucrose free media; therefore
the bacteria could not secrete a glucan layer that would allow creating a protective biosphere.
The antibacterial effect of ozonated water and ozone bubbled in liquid has been
extensively published. 20, 23, 39, 40, 44 There are numerous publications that claim an antibacterial
effect ozone in vivo7, 12 and in vitro8, 9, 11, 13, 14, 16, 17, 20 but several authors have reported the inability of gas ozone to reduce the number of bacteria as a result of treatment 4, 22, 29, 30, 32, 33
which are in accordance with the results obtained in this investigation when using the
Curozone X4®on both root surfaces and microtiter plates and the ozone generator OL80A on
the microtiter plate. Reviewing the literature that supports the use of ozone in dentistry it was
found that not all the cited “in vitro” studies tested ozone in the same conditions.11, 13, 14, 20
Baysan et al. (2000) tested the effect of ozone gas and ozonated water on S. mutans and S.
sobrinus, the bacteria was collected from primary carious lesions on freshly extracted teeth;
they concluded that ozone gas application for a period of 10 s was capable of reducing the
numbers of S. mutans and S. sobrinus on saliva-coated glass beads “in vitro”. The article by
Nagayoshi et al. (2005) on S. mutans tested the effect of ozone on dental plaque samples from
human subjects showing that S. mutans was killed immediately when exposed to ozone water;
however there was no exposure to ozone gas in this study. Johansson et al. (2009) showed
99.9% killing of S. mutans in saliva after being exposed to ozone gas for 60 s. It is important
to point out that the ozone generator used in this investigation KaVo HealozoneTM 2130C
(Curozone; KaVo Biberach/Riss, Germany) was modified to bubble the bacteria culture. The
device was not used as proposed by the clinical protocol in the oral cavity.
In contrast, there are other “in vitro” studies showing the inability of ozone gas to
effectively reduce the bacteria number 22, 29, 30, 32, 45 Hems et al. (2005) compared the effect of
sodium hypochlorite (NaOCl ) and ozone gas generated by Purezone (Ipswich, UK). They
concluded that “Ozone had an antibacterial effect on planktonic E. faecalis cells and those
suspended in fluid, but little effect when embedded in biofilms. The antibacterial efficacy of
ozone was not comparable with that of NaOCl under the test conditions used”. In 2007 Muller
et al. published an article where ozone gas, photodynamic therapy, chlorhexidine in 0.2 and
2% and NaOCl in 0.5 and 5% were applied to A. naeslundii, V. dispar, F. nucleatum, S.
sobrinus, S. oralis and C. albicans biofilms on bovine teeth. The HealOzone 2130C device generator was used. They found that “only the 5% sodium hypochlorite solution was able to
totally eliminate the microorganisms in the biofilm. The observed reduction of viable counts
by vacuum-ozone application and PDT was less than one log10 step. Under the conditions of
the study, gasiform ozone and PDT had a minimal effect on the viability of microorganisms
organized in a cariogenic biofilm”. Polydorou et al. (2012) tested the HealOzone 2130C
device by inoculating S. mutans and L. cassei in artificially made cavities in caries-free third
molars and then treat them for 60 s with ozone. The cavities were filled with composite. After
4 and 8 weeks, the bacteria number was determined. The conclusion brought is the exposure
of ozone through the “HealOzone 2130C device for 60 s can provide some antibacterial
treatment against S. mutans even after 8 weeks. However, an elimination of the
microorganisms seems not to be possible. L. cassei was more resistant to ozone. Although
ozone exerts a significant antibacterial effect against S. mutans, it is probably not enough as
the only antibacterial method, during the fillings therapy”.30 The article published by Estrela
et al (2007) tested the effect of ozonated water, gaseous ozone (PXZ3507; Eaglesat
Tecnologia em Sistemas Ltda., Sao Jose dos Campos, SP, Brazil), sodium hypochlorite
(2.5%) and chlorhexidine (2%) on E. faecalis inoculated in human roots. They concluded that
“The irrigation of infected human root canals with ozonated water, NaOCl, chlorhexidine and
the application of gaseous ozone for 20 min was not sufficient to inactivate E. faecalis”. Iman
et al. (2008) tested the effect of 5.25% sodium hypochlorite (NaOCl), 2% chlorhexidine
(CHX) and ozonated water on E. faecalis and C. albicans biofilms. They found that NaOCl
succeeded in complete degradation of the biofilm. This effect was less with CHX and even
less with ozonated water. Their conclusion is that the antimicrobial effectiveness of 5.25%
NaOCl was reinforced, whereas that of ozonated water was questionable.
Previous studies with positive results have been presented in Europe but there are
several studies that question the effectiveness of ozone as an anticariogenic agent. A
Cochrane Database of Systematic Reviews 34 on three clinical studies reported that the
analyses of all the studies were conducted at the level of the lesion, which is not independent
of the person, for this reason pooling of data was not appropriate or attempted. Few secondary
outcomes were reported, but one trial reported an absence of adverse events. Also, masking of
participants was absent (as no placebo was provided), and there are doubts about the
randomization. Therefore, the Cochrane study concluded that given the high risk of bias in the
available studies and lack of consistency between different outcome measures, there is no
reliable evidence that application of ozone gas to the carious lesion stops or reverses the
process30,46.
Several investigations show that different killing methods have demonstrated dose
effectiveness.29, 47 Gomes et al. (2001) compared sodium hypochlorite (NaOCl) (0.5%, 1%,
2.5%, 4% and 5.25%) and chlorhexidine (CHX) liquid and gel at (0.2%, 1% and 2%). it was
concluded that all irrigants were effective in killing E. faecalis, but at different times. CHX in
the liquid form at all concentrations tested (0.2%, 1% and 2%) and NaOCl (5.25%) were the
most effective irrigants. However, the time required by 0.2% CHX liquid and 2% CHX gel to
promote negative cultures was only 30 s and 1 min, respectively in contrast NaOCL 5.25%
required less than 30 s to produce 100% inhibition growth. 47Their conclusion was that all
irrigating solutions had antibacterial activity but it effectiveness was depended on its
concentration. The results in the present study show that ozone is not dose dependent, there
was no effective bacteria killing either after an exposure of 15 seconds or 4 minutes in the two
different experimental designs. In the root experiments, the results were similar among the
low and high ozone modes compared to the control while exposing 7l of 106 CFU/ml for up
to 60 sec; the microtiter experiment show similar result where effective killing could not be
achieved in exposition that were form 15 to 4 min and the results were not different from the
control.
The present in vitro study could not demonstrate any reduction in the number of S.
mutans after being treated with gasiforme ozone using the Kavo Curozone X4® generator in exposures that went from 15 sec to 4 min; the results were similar on roots as well as in
microtiter plates. It is interesting to mention that while using the Curozone X4® it was found
that the pressure required to keep the seal of the silicone tip to the surface being treated was
minimal, when increasing the pressure, the device stopped working making this procedure
very sensitive and not easy to perform even on the bench in the laboratory, so we presume
that clinically would be even more difficult to obtain good sealing and consequently easy
application. Even though some publications suggest that “It is recommended to deliver ozone
be under pressure into a lesion by pressing the delivery tube onto the carious surface so that it
can penetrate the lesion”.15, 17
It was also noticed that after the ozone exposures some biofilms
were desiccated and some other were wet; but the bacteria recovery did not show any
difference compared to the control, this finding is in accordance with the study published by
Hems et al. (2005). It has been published that “ozone will react immediately with the
reductants in culture media, and the authors did not bubble the ozone into the biofilm”.15, 16
During the present investigation the bubbling effect was not seen when the ozone was applied
to bacteria in media. Actually while using the Curozone X4®when pressure was applied the
device immediately stopped the ozone delivery.
The ozone concentrations tested were 2 and 20 using the ozone generator OL80A in
the Mouse Exposure Chamber; for the 200 and 2000 ppm the ozone generator OL80W in the
Modular Incubator Chamber for exposure time of 4 min. It is important to mention that the
samples were exposed longer that the mentioned times, the chamber took around 20 min to
reach the concentration levels and then the 4 min were counted, therefore the exposure time to
ozone was longer but it is important to emphasize that the effect on bacteria in the microtiter
plate was still negative. The inability of ozone gas to diffuse in liquid has been proposed by
different authors.22, 48 In 1976 Hoigné and Bader stated that “Ozone is a selective oxidant and
affects only certain compounds but when it dissolves in water, it becomes highly unstable and
rapidly decomposes through a complex series of chain reactions”. It has also been stated that
the stability of ozone in water is low and the ozone dissipates very quickly at room
temperature.49
Separate experiments in collaboration with Dr. Marcos Ximenes were conducted at the
same time as the spiral plated assays described above. Instead of spiral plating 49.2ml
volumes, 10l volumes of S. mutans, Lactobacillus acidophilus and Enterococcus faecalis in
concentration ranging from 108 to 103 CFU/ml were delivered as drops on the agar surface
prior to exposure to atmospheres of 2, 20, 200 and 2000 ppm of ozone for 4 min. This
simulated the volumes in the microtiter plate wells. As with the spiral plate studies with S.
mutans, the results obtained showed 100% killing at 2000 and 200 ppm and logarithmic reductions in 20 and 2 ppm atmospheres with all three test species. In addition an experiment
exposing 10l of 106 CFU/ml of S. mutans on the bottom of an agar free Petri dish to 2000
ppm of ozone for 4 min, showed 100% killing (Unpublished data). This may suggest that
ozone gas does not equilibrate with the atmospheric air into a small space such as a well in a
microtiter plate as a result it is no capable to have an antimicrobial effect. The results obtained
in the experiment conducted by Dr. Marcos Ximenes show that ozone can effectively kill
bacteria when it has access to the microorganism and while being on a surface in low volume
of liquid (unpublished data) and probably ozone is ineffective in larger liquid amounts.22, 48
These results may explain why the Curozone X4 could not kill bacteria, the ozone generated
by the instrument was not able to adequately displace the air either in the artificial lesion
preparation in the dentin slab or in the microtiter plate to achieve bactericidal concentrations
of ozone in the target bacterial suspension.
The negative results of this and other in vitro investigations along with the fact that
bacteria living in biofilms as dental plaque on tooth surfaces are generally more resistant to
antimicrobial agents than bacteria in batch culture normally used for in vitro susceptibility
testing43; raise questions about the antimicrobial capacity of the Curozone X4 for clinical use.
In a communication received by the manufacture it was assured that the device used for this
investigation had been tested by the quality control department of the company and was
properly working before being sent to us. (See appendix A).
The results of the present study suggest that ozone in controlled conditions is not
capable to effectively reduce the bacteria number inoculated in media in long exposures when
placed in a microtiter plate. In contrast ozone was able to reduce the bacteria number when it
had adequate access to the bacteria (Petri dish (100 mm diameter) vs. microtiter well (6 mm
diameter) vs. the ~ 1 mm diameter simulated lesion in the dentin slab. The latter result
confirms the finding of previous studies that ozone gas is effective in killing S. mutans.25, 27
6. Conclusions
Without the obvious limitations that exist in a clinical environment, it can be
concluded that the Curozone X4® generator is not capable to effectively reduce the number of
S. mutans in exposure times up to 4 min.
When the bacteria exposure is in an open surface, ozone at 2000 ppm for 4 min can
completely kill S. mutans. Concentrations of ozone as low as 2 ppm result in biologically
significant (exponential) killing of S. mutans.
This study suggests that Curozone X4® generator is not capable of delivering ozone in
7. Tables
Table 1. Indication of the ozone therapy in medicine.19
Indications Mechanisms
External ulcers and skin lesions Disinfection, wound cleansing and improved
wound healing
Arterial circulatory disorders Activation of red blood cell metabolism
with an improvement of oxygen release Activation of reactive oxygen species and radical scavengers
Immunodeficiency and
immunodysbalance: Activation of immunocompetent cells with
Chronic forms of release of cytokins such as interferons and
hepatitis B and C interleukins.
Supportive therapy in cancer patients
Supportive therapy in Modulation of the immune system
rheumatoid arthritis Increase of antioxydative capacity
by activation of biological antioxidants
Inflammatory condition such as: Antiinflammatory effect
Knee arthrosis Activation of antioxidative enzymes as radical
Gonarthrosis scavengers
Traumatic knee disorders Activation of immunocompetent
Table 2. Number of bacteria recovered after the different treatment protocols applied with the Kavo Curozone X4® ozone generator to human dentin specimens for 60 s (log10 CFU)
Treatment protocol (n=36) log10 CFU (Mean ± SD)
Low ozone1 5.25 ± 0.87
High ozone2 5.47 ± 0.92
Control 3 5.58 ± 0.67
(Kruskal-Wallis test, p=0.58)
1. Exposed to ozone in ambient air for 60 seconds. n=12
2. Exposed to ozone in oxygen using the attachedtank for 60 seconds. n=12 3. Exposed to ambient air for 60 seconds. n=12
Table 3. Number of bacteria recovered after the different treatment protocols applied with the Kavo Curozone X4® ozone generator to bovine dentin specimens for 60 s (log10 CFU)
Treatment protocol (n=36) log10 CFU
Low ozone control1 5.37 ± 0.71
High ozone2 5.32 ± 0.82
(Wilcoxon rank sum test, p=0.53)
1. Exposed to ozone in ambient air for 60 seconds. n=18
2. Exposed to ozone in oxygen using the attachedtank for 60 seconds. n=18
Table 4. Number of bacteria recovered and killing rates after exposing S. mutans on agar (log10 CFU/ml) to ozone in the Modular Incubator Chamber at different concentrations for 4 min in covered and uncovered Petri dishes.
After 24
hours Control 2 ppm
2 ppm
cover on 20 ppm
20 ppm
cover on 200 ppm 2000 ppm mean 5.64 2.81 4.58 1.59 3.55 0 0
log10
reduction 2.83 1.06 4.05 2.09 5.64 5.64
logarithmic reduction in recoverable CFU greater than 1 compared to control was considered significant.
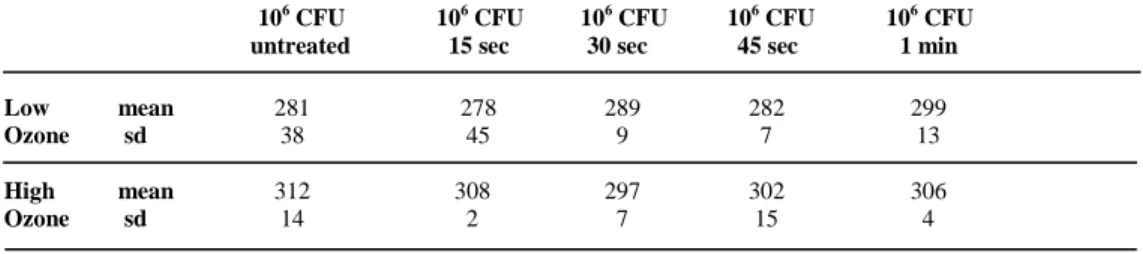
Table 5. Bacterial growth as optical density (mO.D. at λ610 nm) attained following incubation at 37oC for 18 hr after the different treatment protocols applied with the Kavo Curozone X4® ozone generator on 10l of 106 CFU/ml of S. mutans
106 CFU 106 CFU 106 CFU 106 CFU 106 CFU untreated 15 sec 30 sec 45 sec 1 min
Low mean 281 278 289 282 299
Ozone sd 38 45 9 7 13
High mean 312 308 297 302 306
Ozone sd 14 2 7 15 4 (Wilcoxon rank sum test, p=0.42)
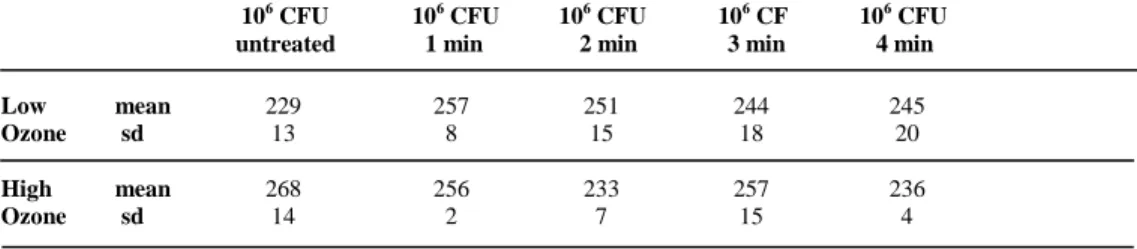
Table 6. Bacterial growth as optical density (mO.D. λ610 nm) attained following incubation at 37oC for 18 hr after the different treatment protocols applied with the Kavo Curozone X4® ozone generator on 10l of 106 CFU/ml of S. mutans
106 CFU 106 CFU 106 CFU 106 CF 106 CFU untreated 1 min 2 min 3 min 4 min
Low mean 229 257 251 244 245
Ozone sd 13 8 15 18 20
High mean 268 256 233 257 236
Ozone sd 14 2 7 15 4 (Wilcoxon rank sum test, p=0.53)
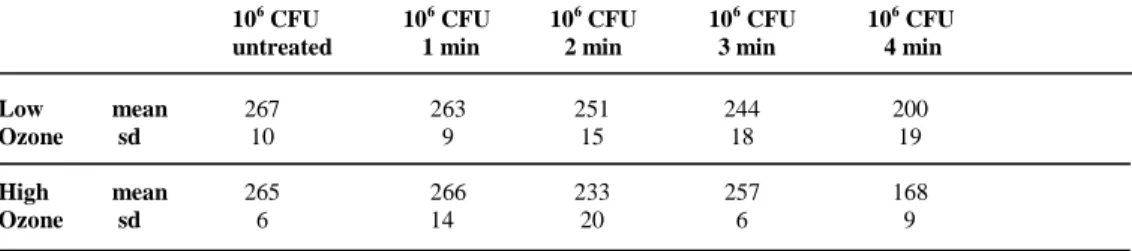
Table 7. Bacterial growth as optical density (mO.D. λ610 nm) attained following incubation at 37oC for 18 hr after the different treatment protocols applied with the Kavo Curozone X4® ozone generator on 10l of a bacteria titration from 106 to 103 CFU/ml of S. mutans
106 CFU 106 CFU 106 CFU 106 CFU 106 CFU untreated 1 min 2 min 3 min 4 min
Low mean 267 263 251 244 200
Ozone sd 10 9 15 18 19
High mean 265 266 233 257 168
Ozone sd 6 14 20 6 9 (Wilcoxon rank sum test, p=0.56)
Table 8. Bacterial growth as optical density (mO.D. λ610 nm) recovery in media and recovery (log10 CFU/ml) on agar attained following incubation at 37oC for 18 hr after the different treatment protocols applied with the ozone generator
OL80W in the Modular Incubator Chamber at 2000 ppm for 4 min
At 24 hours
Non treated bacteria in
media1
Ozone treated bacteria in
media1
Non treated bacteria in
agar2
Ozone treated bacteria in
agar2
mean 432 424 5.63 0
SD 108 158
(Wilcoxon. p<.0001). 1. mO.D. at λ610 nm 2. log10 CFU/ml