Iran J Reprod Med Vol. 10. No.2. pp: 155-160, March 2012 Short communication
Prolonged GnRH suppression period in controlled
ovarian hyperstimulation cycles: Impacts on IVF
outcomes?
Ozlem Gun Eryilmaz M.D., Esma Sarikaya M.D., Melike Doganay M.D., Leyla Mollamahmutoglu M.D., Nedim Cicek M.D.
Department of Obstetrics and Gynecology, Zekai Tahir Burak Women Education and Research
Hospital, Mithatpasa cad.
Hamamonu, Ankara, Turkey.
Corresponding Author:
Ozlem Gun Eryilmaz, Devlet Mah.
Subay Loj. No:19/11 Bakanlıklar, Ankara, Turkey.
Email: [email protected] Tel/ Fax: (+90) 312 3103100
Recieved: 27 March 2011 Revised: 20 July 2011 Accepted: 7 August 2011
Abstract
Background: Prolonged GnRH-a administration in IVF cycles may have some advantages related to the treatment outcomes.
Objective: In this study, we aimed to analyse the effect of prolonged gonadotropin releasing hormone agonist (GnRH-a) administration on controlled ovarian hyperstimulation outcomes of in vitro fertilization (IVF) patients.
Materials and Methods: In this retrospective study, 55 patients with a GnRH-a administration period more than 10 days were compared with 55 patients whose same period was ≤10 days with respect to the demographic characteristics, metaphase II (MII) oocyte ratio, grade I (GI) embryo ratio, blastocyst ratio, fertilization, implantation, and the clinical pregnancy rates.
Results: The mean hospital visit count of the prolonged GnRH-a patients was 2.6±0.4. As we expected, total GnRH-a doses used during hypophyseal down regulation were significantly different between the groups (p<0.0001). MII oocyte, G1 embryo and the blastocyst ratios were also significantly different between the groups (p<0.0001; p<0.01 and p<0.05). All the other parameters were insignificant. Conclusion: Prolonged GnRH-a administration during ovarian suppression in IVF patients may have positive impacts on the oocytes and the embryos, but this affect may not be observed in the overall pregnancy rates.
Key words: GnRH agonist, IVF outcome, Embryo quality.
Introduction
onadotropin releasing hormone
(GnRH) is the primary hypothalamic regulator of reproductive function. Synthetic GnRH causes a huge follicle stimulating hormone (FSH) and luteinizing hormone (LH) release from the pituitary gland and this agonistic activity was the reason why they were called as GnRH agonist (GnRH-a).
It has been used in in-vitro fertilization (IVF) programs since the 1980s, and the main
advantages were related with lesser
cancellation rate, prevention of premature LH surge (1), and higher oocyte recruitment in
poor responder patients (2).The optimal dose
and the duration of GnRH-a administration in hypophyseal suppression is not clear (3).
Jahnsens conducted a dose finding study and declared the needed dose to prevent LH surge was less than the doses needed for malignant diseases (4). Recent studies were
mostly concentrated on the optimal beginning time of the GnRH-a; follicular, early luteal, or late luteal (5) and the effects on the endometrial cells.
Loutradis compared the IVF outcomes of prolonged GnRH-a in a small group of patients whose administration period was less and more than 15 days, and found the favourable effects of GnRH-a prolongation on embryo cleavage speed and pregnancy rate (6). There is no other similar study in the literature related to the chronology. During controlled ovarian hyperstimulation (COH) programs, some patients reach the adequate hormonal profile of down regulation with E2 <50 pg/ml (7) in a few days like 7 to 10 days, and in some patients this time is more than 10 days.
In this study, we compared the IVF outcomes of the patients whose adequate ovarian suppression period was less than 10 days versus more than 10 days.
G
Materials and methods
This retrospective, single-institution, cross-sectional analysis was conducted between January-December 2009 in Zekai Tahir Burak Women’s Training and Research Hospital, IVF Department, Ankara, Turkey.
During this period, number of the patients who were treated with long agonist IVF protocol was 489, and among these, patients with a GnRH-a suppression period >10 days (Group A, n=55) were compared with the patients with a GnRH-a suppression period ≤10 days (Group B, n=55) with respect to age, body mass index (BMI), hospital visit count, preantral follicle count, duration and cause of
infertility, basal E2, FSH, and LH levels, total
doses and the duration of GnRH-a
administration during the hypophyseal down regulation period, duration of induction, total gonadotropin doses used, follicle count
>16mm, peak E2 level and endometrial
thickness on hCG day, number of aspirated oocytes, metaphase II (MII) oocyte ratio, grade I (GI) embryo ratio, blastocyst ratio, fertilization, implantation, and the clinical pregnancy rates.
Patients, who were at the primary infertility age, 20-38 years, were included. Patients with FSH>13 Mıu/ml were excluded from the study. In no instance was donor sperm or oocyte used for ICSI since it is forbidden by law in Turkey. This study was approved by the local Ethics Committee.
Study design
Leuprolide acetate (Lucrin, Abbott,
Istanbul) was started in the mid lutel phase of
the cycle at a dose of 0.5mg/day
subcutaneously (SC). Menstrual bleeding was the sign of the adequate ovarian suppression during GnRH-a administration which was
confirmed with the serum levels of E2<50
pg/mL and LH<5 IU/mL without any ovarian mass (7). The comparison group had confirmed the suppression in the period of 10
days, and this was assessed via the beginning of the menstrual bleeding with the suppressed hormonal levels or it was stated with only the adequate hormonal results in the patients
without menstrual bleeding which was
measured at the 10th day.
If the ovarian suppression was not achieved, GnRH-a dose was increased, and the patient was called back in 6 to 7 days later
for repeat E2 and LH measurements.
Increasing the dose and the duration of the GnRH-a had continued in a period of about 3 weeks, and they set up the study group. After achievement of the adequate hypophyseal suppression recombinant FSH stimulation was initiated and at that time, the dose of leuprolide acetate was decreased to 0.25 mg/day. Further recombinant FSH doses were determined according to the standard criterion
for follicular maturation assessed by
ultrasound and serum E2 measurements.
250 µg recombinant hCG (r-hCG)
(Ovitrelle, Merck Serono, Italy) was
administered when at least three follicles had reached a diameter of 18 mm. Transvaginal-guided oocyte retrieval was done under general anesthesia 36 hours after the hCG injection. The morphological grading of the oocytes was done according to oocyte-cumulus complex, and embryo transfer was
done between the 2nd to 5th days.
Statistical analysis
The data was analysed with SPSS 11.0 package program. The observed power
computed using α=0.05 was 0.80 for the
present study. Independent sample’s t-test, Mann-Whitney U test, and Pearson-chi square test were used for the analysis. p<0.05 was accepted as significant.
Results
Demographic variables of the patients are summarized in table I. Infertility reasons were grouped as unexplained, endometriosis, male,
GnRH prolongation & IVF outcomes.
tubal, and ovulatory factors. Age, infertility reasons and the durations were insignificant between the groups. The mean hospital visit count of the prolonged GnRH-a patients was 2.6±0.4. The minimum and the maximum durations of the cycles in the patients of prolonged GnRH-a group were 22 and 39 days; respectively. Hormonal profile and the IVF outcomes are shown in table II.
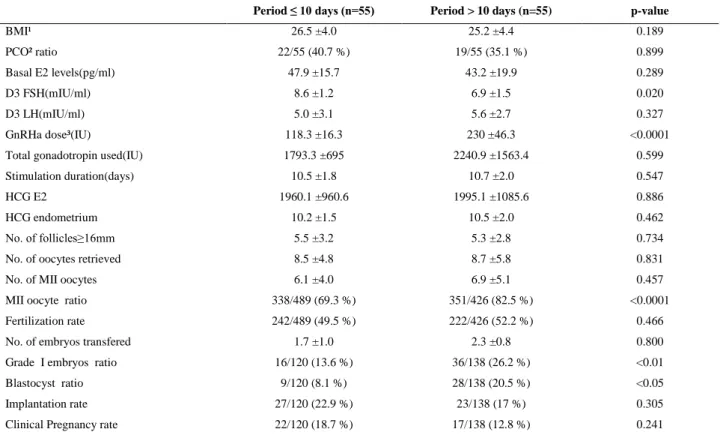
As we expected total GnRH-a doses used during hypophyseal down regulation were
significantly different between the groups (p<0.0001). MII oocyte ratio of the patients with GnRH-a suppression period less than 10 days was significantly different from the patients whose suppression period was more than 10 days (p<0.0001).
Grade I embryo and the blastocyst ratios were significantly more in the patients of GnRHa suppression >10 days (p<0.01 and p<0.05 respectively), but clinical pregnancy rates were similar.
Table I. Demographic data of the patients of GnRH-a administration period ≤10 days and >10 days.
Period ≤ 10 days (n=55) Period > 10 days (n=55) p-value
Age (years) 28.9 ± 4 29.3 ± 3.8 0.675
Infertility duration (years) 8.1 ± 4.3 8.5 ± 3.4 0.282
Infertility causes
Unexplained 21/55 (39.2 %) 20/55 (37.0 %) 0.841
Ovulatory 10/55 (18.5 %) 12/55 (22.2 %) 0.841
Endometriosis 7/55 (13.1 %) 6/55 (11.2 %) 0.764
Male 14/55 (25.5 %) 17/55 (29.6 %) 0.823
Tubal 3/55 (3.7 %) 0/55 (0.0 %) 0.241
Hospital visit count 1.0 ± 0.0 2.6 ± 0.4 0.0001
Values are expressed as mean±SD. NS: Not significant.
Table II. Cycle characteristics of the patients of GnRH-a administration period ≤ 10 days and > 10 days.
Period ≤ 10 days (n=55) Period > 10 days (n=55) p-value
BMI¹ 26.5 ±4.0 25.2 ±4.4 0.189
PCO² ratio 22/55 (40.7 %) 19/55 (35.1 %) 0.899
Basal E2 levels(pg/ml) 47.9 ±15.7 43.2 ±19.9 0.289
D3 FSH(mIU/ml) 8.6 ±1.2 6.9 ±1.5 0.020
D3 LH(mIU/ml) 5.0 ±3.1 5.6 ±2.7 0.327
GnRHa dose³(IU) 118.3 ±16.3 230 ±46.3 <0.0001
Total gonadotropin used(IU) 1793.3 ±695 2240.9 ±1563.4 0.599
Stimulation duration(days) 10.5 ±1.8 10.7 ±2.0 0.547
HCG E2 1960.1 ±960.6 1995.1 ±1085.6 0.886
HCG endometrium 10.2 ±1.5 10.5 ±2.0 0.462
No. of follicles≥16mm 5.5 ±3.2 5.3 ±2.8 0.734
No. of oocytes retrieved 8.5 ±4.8 8.7 ±5.8 0.831
No. of MII oocytes 6.1 ±4.0 6.9 ±5.1 0.457
MII oocyte ratio 338/489 (69.3 %) 351/426 (82.5 %) <0.0001
Fertilization rate 242/489 (49.5 %) 222/426 (52.2 %) 0.466
No. of embryos transfered 1.7 ±1.0 2.3 ±0.8 0.800
Grade I embryos ratio 16/120 (13.6 %) 36/138 (26.2 %) <0.01
Blastocyst ratio 9/120 (8.1 %) 28/138 (20.5 %) <0.05
Implantation rate 27/120 (22.9 %) 23/138 (17 %) 0.305
Clinical Pregnancy rate 22/120 (18.7 %) 17/138 (12.8 %) 0.241
Values are expressed as mean ± SD. NS: Not significant. ¹Body mass index; ²Polycystic ovary; ³Dose during suppression period.
Discussion
GnRH-a treatment is used for hypophyseal down regulation in long protocols of IVF
treatments and adequate hypophyseal
suppression was achieved when E2 and LH
levels were less than 50 pg/mL and 5 IU/mL respectively. Hormonal levels of ovarian suppression were reached in almost three weeks of administration (3). In this study, COH outcome differences were analysed with the acceptance of the 10days as the point of act.
GnRH-a prolongation for adequate ovarian suppression needed much more GnRH-a
doses. Loutradis et al (6) had found a
favorable status of GnRH-a prolongation in embryo cleavage speed and pregnancy rates. In his study, the compared durations were less and more than 15 days. In our study, 10 day was the period of patient selection, and
the results of prolonged suppression
supported Loutradis’s study. Patients with a prolonged suppression duration more than 10 days had more qualified embryos with a
significantly more G1, and blastocyst
formation ratio.
GnRH-a effect on endometrial cells was studied many times and the results were
variable. Meresman et al had concluded the
apoptotic effect of GnRH-a on the
endometrium (8). In this study, the more doses of GnRH-a usage was not related with
any kind of endometrial disturbance.
Endometrial measurements of the patients
with prolonged GnRH-a usage was
comparable with the others on
ultrasonographic appearances.
This conclusion was supported with our results, that the endometrial thickness on the hCG day was comparable between the groups. Endometrial matrix proteins and their
inhibitors was studied by Chou et al who
found that GnRH can modulate the cyclic remodelling events before implantation (9). The promoter effect of GnRH-a on embryo development and implantation was also reported (10, 11).
Kawamura et al documented the
antiapoptotic effect on mouse blastocysts which was parallel with our results with a significantly more blastocyst formation in prolonged GnRH-a used IVF cycles (10). In a
recent study by Klemmt et al, the effect on
embryo invasion was analysed, and no negative impact was found (12). In our study, GnRH-a prolongation with higher doses did improve the oocyte and the embryo, but not the implantation and the clinical pregnancy rates.
This may be because of the apoptotic effect of the prolonged GnRH administration on the endometrium that the implantation was not improved even with a qualified embryo. This apoptotic effect was not shown in the
gross thickness measurements of the
endometrium, but undetectable biochemicals
that may be released into the
microenvironment could negatively impact the implantation process itself. GnRH-a may be successful in the role of the ovarian suppression, and in the ovarian improvement with qualified oocytes, but it may cause some negative effects on the endometrium that implantation rates may not be affected in the same positive manner.
It is known that age more than 35 years was a poor prognostic factor for IVF success (13), but this poor expectation was not seen in the prolonged GnRH-a suppression period. The insignificant age correlation showed that older patients did not have a risk of suppression failure in long agonist protocols. Increased BMI also was not a predictive criterion for prolonged GnRH-a administration need. Patients with larger fatty mass in their
GnRH prolongation & IVF outcomes.
bodies did not have an unfavorable hormonal status during hypophyseal down regulation.
Their gonadotropin initiation time was comparable with the lean patients. Adequate ovarian suppression in 10 days did not show any specificity from the ovarian reserve point of view. Ovaries with a high number of follicle count, like in polycystic appeared ovaries were not different from the other lower follicle counted ovaries in GnRH-a suppression duration and doses. An ovary containing lots of prenatal follicles did not needed higher GnRH-a doses, and the expectation of a
prolonged suppression period was not
reliable. The increased hospital visit count in patients of prolonged suppression period was the only negative side. Prolongation caused almost three times more hospital attendance in these patients.
In summary, prolonged GnRH-a
administration during ovarian suppression may have positive impacts on the oocytes and the embryos. But this effect was not observed
in the overall pregnancy rates. Long
suppression period with more hospital visits may tire the patients, but it may be a chance to achieve more qualified oocytes and embryos.
References
1. Muasher SJ, Abdallah RT, Hubayter ZR. Optimal stimulation protocols for in vitro fertilization. Fertil
Steril 2006; 86: 267-273.
2. Serafini P, Stone B, Kerin J, Batzofin J, Quinn P, Mars R. An alternate approach to controlled ovarian hyper-stimulation in ‘poor responders’: pretreatment with a gonadotropin releasing hormone analog. Fertil
Steril 1988; 49: 90-95.
3. Huirne AFJ, Schats R. The use of GnRH agonists. In: Gardner KD, Weissman A, Howles CM, Shoham Z. Textbook of assisted reproductive technologies. 3rd Ed. UK; Informa Healthcare; 2009: 529-538.
4. Janssens RM, Lambalk CB, Vermeiden JP, Schats R, Bernards JM, Rekers-Mombarg LT, et al. Dose
finding study of triptorelin acetate for prevention of a premature LH surge in IVF: a
prospective, randomised, double-blind, placebo-controlled study. Hum Reprod 2000; 15: 2333-2340.
5. Kondaveeti-Gordon U, Harrison RF, Barry-Kinsella C, Gordon AC, Drudy L, Cottell E. A randomized prospective study of early follicular or midluteal initiation of long protocol gonadotropin-releasing hormone in an in vitro fertilization program. Fertil
Steril 1996; 66: 582-586.
6. Loutradis D, Kallianidis K, Sakellaropoulos G, Dokos J, Siskos K. Outcome of ovarian response after suppression with a gonadotropin releasing hormone agonist in different chronological periods prior to gonadotropin stimulation for in vitro fertilization.
Gynecol Obstet Invest 1991; 32: 68-71.
7. Daya S. Gonadotropin-releasing hormone agonist protocols for pituitary desensitization in in-vitro fertilization and gamete intrafallopian transfer cycles (Cochrane review). In: The Cochrane Library, Issue 1. Oxford; Update Software; 2000.
8. Meresman GF, Bilotas MA, Lombardi E, Tesone M, Sueldo C, Branao RI. Effect of GnRH analogues on apoptosis and release of interleukin-I beta and vascular endothelial growth factor in endometrial cell cultures from patients with endometriosis. Hum
Reprod 2003; 18: 1767-1771.
9. Chou CS, Tai CJ, MacCalman CD, Leung PC. Dose dependant effects of gonadotropin releasing hormone on matrix metattoproteinase (MMS) -2 and MMP-9 and tissue spesfic inhibitor of matalloproteinase-I massenger ribonucleic acid levels in human decidual stromal cells in vitro. J Clin
Endocrinol Metab 2003; 88: 680-688.
10. Kawamura K, Fukuda J, Kumagai J, Shimizu Y, Kodama H, Nakamura A, et al. Gonadotropin releasing hormone I analogue acts on an antiptotic factor in Mouse blastocysts. Endocrinology
2005; 146: 4105-4116.
11. Torres Mde M, Donadio N, Donadio NF, Brandao AC, Heck B. Comparison of embryo implantation in Wistar rats that underwent ovarian stimulation using exogenous gonadotropins assiciated with cetrorelix acetate and leuprolide acetate.
Fertil Steril 2005; 84: 1235-1240.
12. Klemmt PAB, Liu F, Carver JG, Jones C, Brosi D, Adamson C. Effect of gonadotropin releasing hormone analogues on human endometrial stromal cells and embryo invasion in vitro. Hum Reprod
2009; 24: 2187-2192.
13. Korula G, Mohan S Kamath. Fertility and age. J Hum Reprod Sci 2010; 3: 121-123.