Veysi Akpolat
1, F, H. Murat Bilgin
2, A, B, D, E, M. Yusuf Celik
3, C,
Mahmut Erdemoglu
4, B, Birgul Isik
5, A, BAn Evaluation of Nitric Oxide, Folate,
Homocysteine Levels and Lipid Peroxidation
in Postmenopausal Osteoporosis
Ocena stężenia tlenku azotu, kwasu foliowego, homocysteiny
i peroksydacji lipidów w osteoporozie pomenopauzalnej
1 Department of Biophysics, Bone Mineral Densitometry Unit, Faculty of Medicine, Dicle University, Turkey 2 Department of Physiology, Faculty of Medicine, Dicle University, Turkey
3 Department of Biostatistics, Faculty of Medicine, Dicle University, Turkey
4 Department of Obstetrics and Gynecology, Faculty of Medicine, Dicle University, Turkey 5 Department of Biochemistry, Faculty of Medicine, Dicle University, Turkey
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Objectives.In the current study, the risk coefficients of nitric oxide (NO), folate, homocysteine levels and lipid peroxidation in postmenopausal osteoporotic women were determined.
Material and Methods. Bone mineral density was determined by dual-energy X-ray absorptiometry. The levels of serum lipid peroxidation products such as the thiobarbituric acid adduct of malondialdehyde (MDA) were measured spectrophotometrically. Plasma folate and homocysteine (Hcy) levels were measured by enzyme chemi-luminescence immunoassay. Plasma nitrite levels were measured with the Griess reaction
Results. The odds ratios and 95% Confidence Intervals (CI) of the variables MDA, folate, NO, body-mass index (BMI), menopause age and age were found significant. MDA, NO and folate variables were found statistically sig-nificant in the analysis of receiver operating charecteristic (ROCs). The areas under the curve (AUCs, 95% CI) of MDA, NO and folate were found to be statistically significant.
Conclusions. The current study indicates that NO, MDA and folate are risk variables for postmenopausal osteo-porosis (Adv Clin Exp Med 2013, 22, 3, 403–409).
Key words: nitric oxide, folate, malondialdehyde, homocysteine, osteoporosis.
Streszczenie
Cel pracy. W pracy oceniono czynniki ryzyka, takie jak stężenie tlenku azotu (NO), kwasu foliowego, homocyste-iny i peroksydację lipidów, w okresie pomenopauzalnym u kobiet chorych na osteoporozę.
Materiał i metody. Gęstość mineralną kości zmierzono za pomocą dwuwiązkowej absorpcjometrii rentgenowskiej. Stężenia produktów peroksydacji lipidów, takich jak addukt aldehydu malonowego (MDA) i kwasu tiobarbituro-wego, zmierzono spektrofotometrycznie. Stężenie kwasu foliowego i homocysteiny (Hcy) zmierzono za pomocą testu immunoenzymatycznego chemiluminescencji. Stężenie azotynów w osoczu zmierzono za pomocą reakcji Griessa.
Wyniki. Ilorazy szans i 95% przedziały ufności (CI) zmiennych MDA, kwas foliowy, NO, wskaźnik masy ciała (BMI), wiek menopauzy oraz wiek były znaczące. Stwierdzono, że zmienne MDA, NO i kwas foliowy są istotne statystycznie w analizie krzywej ROC. Obszary pod krzywą (AUC, 95% CI) MDA, NO i kwasu foliowego okazały się istotne statystycznie.
Adv Clin Exp Med 2013, 22, 3, 403–409 ISSN 1899–5276
ORIGINAl PAPERS
Osteoporosis, a major public health problem, is a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue [1, 2]. Several risk factors have been identified for osteoporosis such as age, low body mass index (BMI), current smoking, alcohol inta-ke and low bone mineral density (BMD). Defici-encies in folate lead to increased serum concentra-tions of homocysteine (Hcy), which is associated with bone disorders. Hcy accumulates collagen in bone and contributes to decrease in bone strength. As Tyagi et al. (2011) wrote: „The mechanism of Hcy induced bone loss and remodeling is unclear … Elevated levels of Hcy are associated with va-rious bone abnormalities, such as osteopenia and osteoporosis [3, 4]. The thiol groups in Hcy under-go auto-oxidation, thus triggering oxidative stress and causing the production of reactive oxygen species (ROS). Super oxide anion may react with nitric oxide to produce peroxynitrite with redu-ced NO bio-availability [5], which may impair the osteoblast–osteoclast balance with unpredictable consequences on bone remodeling” [3]. Folic acid (FA) is a naturally occurring dietary component that reduces the levels of Hcy by increasing the rate of recycling of Hcy to methionine [6]. It is known that Hcy-lowering therapy can favorably influen-ce the course of osteoporosis [7]. In addition, Hcy deficiencies are associated with increased levels of bone turnover markers [8].
During the remodelling cycle, bone is conti-nuously resorbed by osteoclasts and new bone is formed by osteoblasts; this is regulated by local factors such as nitric oxide (NO) [9]. NO is a free radical, synthesized from l-arginine by NO synt-hases. It has been shown that NO has significant modulatory effects on bone metabolism [10, 11]. It is produced constitutively by osteoblasts [12] and
stimulates their proliferation in vitro [13].
Malondialdehyde (MDA), the end product of lipid peroxidation, plays an important role in the process of bone loss and is a measure of osteoclas-tic activity [14, 15].
Hcy is a thiol-containing amino acid that forms in the process of methionine metabolism. The remethylation pathway that exists for the deg-radation of Hcy uses folate as a cofactor. Recently, Hcy levels and plasma folate concentrations have been shown to be associated with fracture risk or lower BMD [16, 17].
BMD measurement is widely used for detect-ing osteoporosis, and dual-energy X-ray
absorb-siometry (DXA) is a non-invasive method that provides precise BMD assessment [1]. It is likely that BMD is lower in postmenopausal than in pre-menopausal subjects [18].
In the current study, the risk coefficients of ni-tric oxide, folate, homocysteine levels and lipid per-oxidation in postmenopausal osteoporotic women were studied by using the logistic regression meth-od. Receiver Operating Charecteristic (ROCs) and areas under the curves (AUCs) also were used to de-termine the discriminitive ability of the variables.
Material and Methods
The Subjects
Postmenopausal women aged 45–65 years (n = 126) who were admitted to the out-patient clin- ic of gynecology department of faculty of
medici-ne of Dicle University in betweenApril–October
2008 were enrolled in this study. Exclusion criteria were alcohol consumption, tobacco use, postme-nopausal hormone replacement therapy, systemic diseases, such as diabetes mellitus and renal failu-re. All of the subjects had experienced natural me-nopause; menopause was defined as 1 year with no menstrual bleeding. Routine biochemical analyses (including glucose, urea, creatine, liver function tests, free calcium, and phosphorus) and complete blood count of the subjects were assessed as nor-mal. None of the subjects took any medications likely to affect BMD or calcium metabolism du-ring the study. Baseline characteristics including age, age at menopause, weight, height and body mass index (BMI) were recorded for each subject. A self-administered questionnaire was used to collect information about the subjects’ history as hormone use, smoking status, caffeine consump-tion, regular alcohol intake, and daily use of milk or milk products. The study was explained to each subject, and written informed consent was read and signed by all the participant, in accordence with the Declaration of Helsinki.
Anthropometric Measurements
The participants’ weight was measured to the nearest 0.1 kg, and their height was measured to the nearest 0.1 cm with a wall-mounted stadio-meter (Seca Model 786, Vagel & Halke, Hamburg, Germany) with the subjects wearing light clothingWnioski. Wyniki badania wskazują, że NO, MDA i kwas foliowy są czynnikami ryzyka osteoporozy pomenopau-zalnej (Adv Clin Exp Med 2013, 22, 3, 403–409).
and no shoes. Their BMIs (in kg/m2) were then
calculated as weight (kg) divided by the square of the height (m2).
DXA Scanning
Bone mineral density was determined by du-al-energy X-ray absorptiometry (DXA, Discovery QDR 4500A series, Hologic, Waltham, MA, USA, Software 12.3.3 version). Spinal and femoral sites were measured in slow mode and supine
positi-on. BMD (g/cm2) was calculated from the bone
mineral content (BMC) and bone area (BA). All measurements and analyses were performed by the same experienced investigator. The NHANES III spine and hip reference population for young women (age range 20–40 years) was used. T-Sco-res were calculated by using a standard formula: [T-score = BMD of participant mean–mean BMD of reference population/SD of BMD of reference population]. The diagnostic criteria were derived from World Health Organization criteria for post-menopausal women. Osteoporosis is diagnosed if the bone density at any site has a T-score less than or equal to –2.5. Normal bone density is a T-score greater than –1.0 [19]. The subjects were divided into two groups according to their T-scores: nor-mal and osteoporotic postmenopausal women.
Blood Samples
Fasting venous blood samples of the subjects were collected and centrifuged at 3500 rpm for 10 min at room temperature. The samples were stored at −70°C until analysis.
The levels of serum lipid peroxidation pro-ducts such as the thiobarbituric acid adduct of malondialdehyde (TBA-MDA) were measured spectrophotometrically by a modification of the method described by Buege and Aust [20]. The spectrophotometric measurements were done with Shimadzu UV-1208 spectrophotometer (Ja-pan). The concentrations of lipid peroxidation products were calculated as MDA concentration using the extinction coefficient for the MDA– thi-obarbituric acid complex of 1.56×105 l/mol cm at 535 nm.
Plasma tHcy was measured using commerci-ally available kits on an autoanalyzer (Immulite 2500, USA) by enzyme chemiluminescent immu-noassay. Plasma folate was analyzed using com-mercially available kits on an autoanalyzer (Roche E 170, USA), also by enzyme chemiluminescent immunoassay.
Plasma nitrite levels were measured with the Griess reaction [21]. As described in a previous
article [22],reduction of nitrate to nitrite was
ac-complished by catalytic reaction using cadmium. The nitrite produced was determined by diazoti-sation of sulfanilamide and coupling to naphthy-lethylene diamine. Absorbance of this complex was measured at 545 nm. A standard curve was
established with a set of serial dilutions (10–8–10–
3 mol/l) of sodium nitrite. A linear regression was
performed using the peak area from the nitrite standard. The resulting equation was then used to calculate the sample concentrations. The results were expressed as µmoles per liter plasma.
Statistical Analysis
The mean and standard deviation (x– ± SD) for
continuous variables were calculated. The norma-lity of the variables was analyzed by the Kolmo-gorov-Smirnov test. The means of variables for the groups of postmenopausal women with and without osteoporosis were tested using Student’s
t-test for independent groups.
Binary logistic regression analysis was used to determine the risk factors in osteoporotic postme-nopausal women according to total hip T-scores. The subjects’ age, menopause age, folate levels, ho-mocysteine levels, NO levels, BMI and MDA were included when the backward stepwise logistic reg-ression analysis was performed. The variables we-re considewe-red statistically significant for the model at p < 0.05. ROC curves and areas under the curves were assessed for age, menopause age, folate, NO, BMI and MDA that were found to be significant in the logistic regression model. The ROC curve was applied for folate, NO, and MDA that had high AUCs values. Odds ratios were calculated by the logistic regression method. Two-sided p-values were considered statistically significant at p < 0.05. The statistical analyses were carried out using the statistical packages for SPSS 15.0 for Windows (SPSS, Inc., Chicago, Il, USA).
Results
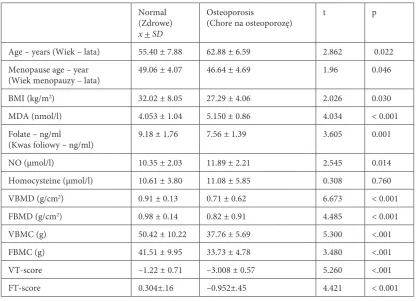
There were significant differences between the two groups, in age, menopause age, BMI, MDA, folate, NO (P < 0.05). The osteoporotic markers were presented in Table 1. Differences in femur BMD (FBMD), vertebra BMD (VBMD), vertebra BMC (VBMC), femur BMC (FBMC) and vertebra T-score (VT-score) were also found to be statisti-cally significant (p < 0.001).
women with osteoporosis. The odds ratios and 95% confidence intervals (CI) of those variables (MDA, folate, NO, BMI, menapouse age and age) were found to be significant and were as follows: 1.682 (1.06–2.66), 1.373 (1.01 –1.87), 1.575 (1.29 – 1.93), 1.925 (1.57 – 2.35), 1.526 (1.28 – 1.82) and 1.261 (1.07 – 1.49), respectively. The ratio of cor-rect classification was 0.9675 (Table 2).
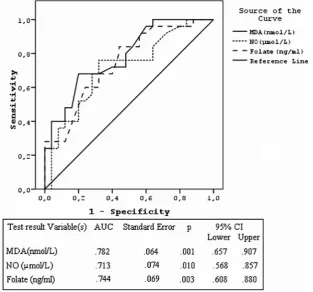
The variables found significant in the analy-sis of logistic regression were then analysed using ROCs. The ROC curves are presented in Figure 1. MDA, NO and folate were the variables that were found to be significant in the analysis of ROCs. The AUCs (95%CI) values of MDA, NO and fo-late were found to be significant, as follows: 0.782 (0.657 – 0.907), 0.713 (0.568 – 0.857) and 0.744 (0.608 – 0.880), respectively.
Discussion
In the current study, the variables which con-stituted risk for osteoporosis in post menopausal women were determined by using logistic regres-sion and receiver operating characteristic (ROCs) with the areas under the curves (AUCs). The sta-tistical analyses for NO, folate and MDA revealed statistically significant results for postmenopausal osteoporotic women.
As Armour et al. wrote: “Nitric oxide (NO) is a pleiotropic signaling molecule that has potent
effects on osteoblast and osteoclast activity in
vi-tro” [23]. Previous studies conducted on both
ani-mal and human models have shown that NO is an important regulator on bone cell function [9, 11, 24]. Hao et al. noted that “NO has biphasic effects on osteoclastic bone resorption, and low concen-trations of NO augment interleukin-1-induced
Table 1. Characteristics and the results of comparison between normal and osteoporotic postmenopausal women
Tabela 1. Charakterystyka i porównanie wyników kobiet po menopauzie zdrowych i chorych na osteoporozę
Normal (Zdrowe) x + SD
Osteoporosis
(Chore na osteoporozę) t p
Age – years (Wiek – lata) 55.40 ± 7.88 62.88 ± 6.59 2.862 0.022
Menopause age – year
(Wiek menopauzy – lata) 49.06 ± 4.07 46.64 ± 4.69 1.96 0.046
BMI (kg/m2) 32.02 ± 8.05 27.29 ± 4.06 2.026 0.030
MDA (nmol/l) 4.053 ± 1.04 5.150 ± 0.86 4.034 < 0.001
Folate – ng/ml
(Kwas foliowy – ng/ml) 9.18 ± 1.76 7.56 ± 1.39 3.605 0.001
NO (µmol/l) 10.35 ± 2.03 11.89 ± 2.21 2.545 0.014
Homocysteine (µmol/l) 10.61 ± 3.80 11.08 ± 5.85 0.308 0.760
VBMD (g/cm2) 0.91 ± 0.13 0.71 ± 0.62 6.673 < 0.001
FBMD (g/cm2) 0.98 ± 0.14 0.82 ± 0.91 4.485 < 0.001
VBMC (g) 50.42 ± 10.22 37.76 ± 5.69 5.300 <.001
FBMC (g) 41.51 ± 9.95 33.73 ± 4.78 3.480 <.001
VT-score –1.22 ± 0.71 –3.008 ± 0.57 5.260 <.001
FT-score 0.304±.16 –0.952±.45 4.421 < 0.001
BMI: body-mass index. MDA: malondialdehyde. BMD: bone mineral density. BMC: bone mineral content.
FT-VT-score: femur - vertebra T-score. BMI – wskaźnik masy ciała.
MDA – malonaldehyd. BMD – mineralna gęstość kości. BMC – mineralna zawartość kości.
bone resorption” [25]. However, as Van’t Hoff et al. pointed out, “High concentrations of NO in-hibit osteoclast formation and activity” [11].
Increasing levels of MDA (in plasma and er-ythrocyte) have been shown to be a result of lipid peroxidation in osteoporotic females compared with a non-porotic control group [14, 15]. Son-takke and Tare [26] found elevated levels of MDA in a group of postmenopausal osteoporotic indivi-duals compared to healthy controls, indicating the potential role of lipid peroxidation in bone meta-bolism. However, Maggio et al. [27] has reported
similar MDA levels in aged osteoporotic women compared to non-porotic controls.
In highly stressed conditions like increased os-teoclastic activity, NO can react with oxygen-deri-ved free radicals such as superoxide anions to form highly reactive molecules. The production of such toxic moieties may contribute to the tissue damage by inducing lipid peroxidation [14, 15]. This may explain the increased NO and MDA levels in os-teoporotic women.
Ravaglia et al. [28] found that low serum folate is responsible for the risk of osteoporotic fracture,
indi-Table 2. The results of logistic regression and odds ratios
Tabela 2. Wyniki regresji logistycznej oraz ilorazy szans
Variables (Zmienne) b SE Wald OR (95% CI) p
MDA 0.522 0.234 4.97 1.682 (1.06–2.66) 0.027
Folate (Kwas foliowy) 0.322 0.156 4.26 1.373 (1.01–1.87) 0.021
NO (Tlenek azotu) 0.457 0.101 20.47 1.575 (1.29–1.93) < 0.001
BMI 0.655 0.102 41.24 1.925 (1.57–2.35) < 0.001
Menopause age
(Wiek menopauzy) 0.423 0.093 22.09 1.526 (1.28–1.82) < 0.001
Age (Wiek) 0.232 0.085 7.449 1.261 (1.07–1.49) < 0.001
Correct classification (Poprawna klasyfikacja): 96.75%
Fig. 1. ROC curves, AUC values and standard error, p value and 95% CI of AUC of MDA, NO and folate
cating the role of folate in BMD. Cagnacci et al [29] observed a significant relation between folate and BMD in the lumbar spine, as plasma folate levels we-re decwe-reased in the osteoporotic group as compawe-red with the non osteoporotic controls. This coincides with a study of 271 postmenopausal Iranian women by Golbahar et al., in which BMD exhibited a positi-ve correlation with serum folate [30].
In the current study, the risk ratios of NO, MDA and folate in postmenopausal women with osteo-porosis were found to be significant (1.575, 1.682 and 1.373, respectively). These risk ratios show the real amount of NO, MDA and folate in osteoporot-ic women. The present study has established that these important risk variables have the discrimina-tive ability to identify women with or without os-teoporosis. In fact, the discriminative ability (AUCs values) of MDA, NO, and folate were found to be 0.78, 0.71 and 0.74, respectively, in the results of the ROCs. These distinct outcomes show the risk of os-teoporosis in postmenopausal women in detail.
Recent data suggest that homocysteine (Hcy) and folate affect bone metabolism in humans [17]. Yılmaz et al. showed that serum Hcy levels were significantly higher in postmenopausal osteopo-rotic women than their non-osteopoosteopo-rotic
counter-parts [31]. Similarly, the increased risk of osteo-porosis in case of high homocysteine blood levels was emphasized by leboff et al. [32]. However, several investigations reported no associations, or only weak or inversed associations between Hcy and bone mineral density (BMD) [29, 30, 33]; the current study showed no relation between Hcy and BMD. In the current study the mean age of postmenopausal women was 62.9 ± 6.6 years, whereas in the study of Van Meurs et al. [34], the subjects were over 70 years of age. As Herrmann et al. pointed out: „However, [the lack of interac-tion between Hcy and BMD] is not surprising, since BMD mainly reflects bone mineralization and provides only an integral measure of bone metabolism” [35].
In addition, the current study found that age, menopause age and BMI were also significant pre-dictors of BMD in postmenopausal women. The negative association of BMD with age and posi-tive association with BMI have already been docu-mented [36, 37].
The authors concluded that NO, MDA and fo-late are risk variables and the detailed risk ratios of these factors on the postmenopausal osteoporotic women have also been presented.
References
[1] Manolagas SC: Birth and death of bone cells: basic regulatory mechanisms and implications for the pathogenesis and treatment of osteoporosis. Endocr Rev 2000, 21, 115–137.
[2] Christodoulou C, Cooper C: What is osteoporosis? Postgrad Med J 2003, 79, 133–138.
[3] Tyagi N, Kandel M, Munjal C, Qipshidze N, Vacek JC, Pushpakumar SB et al.: Homocysteine mediated decrease in bone blood flow and remodeling: role of folic acid. J Orthop Res 2011, 29(10), 1511–1516.
[4] Alley RA, Chen EL, Beyer TD, Prinz RA: Does homocysteine contribute to bone disease in hyperparathyroidism? Am J Surg2008, 195,374–377.
[5] Banfi G, Iorio EL, Corsi MM:Oxidative stress, free radicals and bone remodeling. Clin Chem lab Med2008, 46, 1550–1555.
[6] Woo KS, Chook P, Lolin YI,Sanderson JE, Metreweli C, CelermajerDS:Folic acid improves arterial endothelial function in adults with hyperhomocystinemia. J Am Coll Cardiol1999, 34, 2002–2006.
[7] Herrmann M, Taban-Shomal O, Muller S, Gunter L, Hübner U, Böhm Met al.:Hyperhomocysteinemia – The biochemical link between a weak heart and brittle bones?Clin lab2006, 52, 137–147.
[8] Dhonukshe-Rutten RA, Pluijm SM, de Groot LC, Lips P, Smit JH, van Staveren WA:Homocysteine and vita-min B12 status relate to bone turnover markers, broadband ultrasound attenuation, and fractures in healthy elderly people. J Bone Miner Res2005, 20,921–929.
[9] Van’t Hof RJ, Ralston SH: Nitric oxide and bone. Immunology 2001, 103, 255–261.
[10] Caballero-Alias AM, Loveridge N, Lyon A, Das-Gupta V, Pitsillides A, Reeve J: NOS isoforms in adult human osteocytes: multiple pathways of NO regulation? Calcif Tissue Int 2004, 75, 78–84.
[11] Van’t Hof RJ, Armour KJ, Smith LM Armour KE, Wei XQ, Liew FY et al.: Requirement of the inducible nitric oxide synthase pathway for Il-1 induced osteoclastic bone resorption. Proc Natl Acad Sci USA 2000, 97(14), 7993–7998.
[12] Calabrese EJ: Nitric oxide: Biphasic dose responses. Crit Rev Toxicol 2001, 31, 489–501.
[13] RianchoJA, Zarrabeitia MT, Fernandez Luna JL, Gonzalez Macias J: Mechanisms controlling nitric oxide syn-thesis in osteoblasts. Mol Cell Endocrinol 1995, 107, 87–92.
[14] Ozgocmen S, Kaya H, Fadillioglu E, Aydogan R, Yilmaz Z: Role of antioxidant systems, lipid peroxidation, and nitric oxide in postmenopausal osteoporosis. Mol Cell Biochem 2007, 295, 45–52.
[15] Korachich GB, Mishra OP: lipid peroxidation in rat brain cortical slices as measured by TBA test. J Neurochem 1980, 35, 1449–1452.
[17] Villadsen MM, Bunger MH, Carstens M, Stenkjaer L, Langdahl BL: Methylene tetrahydrofolate reductase (MTHFR) C677T polymorphism is associated with osteoporotic vertebral fractures, but is a weak predictor of BMD. Osteoporos Int 2005, 16, 411–416.
[18] Perry HM 3rd, Bernard M, Horowitz M, Miller DK, Fleming S, Baker MZ et al.: The effect of aging on bone mineral metabolism and bone mass in Native American women. J Am Geriatr Soc 1998, 46(11), 1418–1422.
[19] The WHO Study Group: Assessment of fracture risk and its application to screening for postmenopausal osteopo-rosis. Osteoporos Int 1994, 4, 368–381.
[20] Buege JA, Aust SD: Microsomal lipid peroxidation. Methods Enzymol 1978, 52, 301–310.
[21] Cortas NK, Wakid NW: Determination of inorganic nitrate in serum and urine by a kinetic cadmium-reduction method. Clin Chem1990, 36(8), 1440–1443.
[22] Bilgin HM, Tumer C, Diken H, Kelle M, Sermet A: Role of ghrelin in the regulation of gastric acid secretion involving nitrergic mechanisms in rats. Physiol Res 2008, 57(4), 563–568.
[23] Armour KE, Armour KJ, Gallagher ME, Gödecke A, Helfrich MH, Reid DM, Ralston SH: Defective bone for-mation and anabolic response to exogenous estrogen in mice with targeted disruption of endothelial nitric oxide synthase. Endocrinology 2001, 142(2), 760–766.
[24] Aguirre J, Buttery L, O’Shaughnessy M, Afzal F, Fernandez de Marticorena I, Hukkanen M et al.: Endothelial nitric oxide synthase gene-deficient mice demonstrate marked retardation in postnatal bone formation, reduced bone volume, and defects in osteoblast maturation and activity. Am J Pathol 2001, 158, 247–257.
[25] Hao YJ, Tang Y, Chen FB, Pei FX: Different Doses of Nitric Oxide Donor Prevent Osteoporosis in Ovariectomized Rats. Clin Orthop Relat Res 2005, 435, 226–231.
[26] Sontakke AN, Tare RS: A duality in the roles of reactive oxygen species with respect to bone metabolism. Clin Chim Acta 2002, 318, 145–148.
[27] Maggio D, Barabani M, Pierandrei M, Polidori MC, Catani M, Mecocci P et al.: Marked decrease in plasma antioxidants in aged osteoporotic women: results of a cross-sectional study. J Clin Endocrinol Metab 2003, 88(4), 1523–1527.
[28] Ravaglia G, Forti P, Maioli F,Servadei L, Martelli M, Brunetti N et al.: Folate, but not homocysteine, predicts the risk of fracture in elderly persons. J Gerontol A Biol Sci Med Sci 2005, 60, 1458–1462.
[29] Cagnacci A, Baldassari F, Rivolta G, Arangino S, Volpe A: Relation of homocysteine, folate, and vitamin B12 to bone mineral density of postmenopausal women. Bone 2003, 33(6), 956–959.
[30] Golbahar J, Hamidi A, Aminzadeh MA, Omrani GR: Association of plasma folate, plasma total homocysteine, but not methylenetetrahydrofolate reductase C667T polymorphism, with bone mineral density in postmenopausal Iranian women: a cross-sectional study. Bone 2004, 35, 760–765.
[31] Yılmaz N, Eren E: Homocysteine oxidative stress and relation to bone mineral density in postmenopausal osteo-porosis. Aging Clin Exp Res 2009, 21, 353–357.
[32] Leboff MS, Narweker R, Lacroix A, Wu L, Jackson R, Lee J et al.: Homocysteine levels and risk of hip fracture in postmenopausal women. J Clin Endocrinol Metab 2009, 94(4), 1207–1213.
[33] Sato Y, Honda Y, Iwamoto J, Kanoko T, Satoh K: Effect of folate and mecobalamin on hip fractures in patients with stroke: a randomized controlled trial. J Am Med Assoc 2005, 293, 1082–1088.
[34] Van Meurs JB, Dhonukshe-Rutten RA, Pluijm SM, et al.: Homocysteine levels and the risk of osteoporotic frac-ture. N Engl J Med 2004, 350, 2033–2041.
[35] Herrmann W, Herrmann M:Is hyperhomocysteinemia a risk factor for osteoporosis? Expert Rev Endocrinol Metab 2008, 3(3), 309–313.
[36] Lenchik L, Kiebzak GM, Blunt BA: What is the role of serial bone mineral density measurements in patient man-agement? J Clin Densitom 2002, 5, 29–38.
[37] Rasmussen LB, Ovesen L, Bülow I, Knudsen N, Laurberg P, Perrild H: Folate intake, lifestyle factors, and homo-cysteine concentrations in younger and older women. Am J Clin Nutr 2000, 72, 1156–1163.
Address for correspondence:
Veysi Akpolat
Department of Biophysics Faculty of Medicine Dicle University 21280 Diyarbakir Turkey
Tel.: +90 533 6691111 E-mail: [email protected] Conflict of interest: None declared Received: 5.07.2012