Agnieszka Matuszewska¹
, A–D, Jacek Szechiński²
, A, E, FEvaluation of Selected Bone Metabolism Markers
in Rheumatoid Arthritis Patients
Ocena wybranych markerów metabolizmu kostnego u chorych
na reumatoidalne zapalenie stawów
¹ Department of Pharmacology, Wroclaw Medical University, Poland
² Department and Clinic of Rheumatology and Internal Medicine, Wroclaw Medical University, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. Rheumatoid arthritis (RA) is a chronic systemic disease of connective tissue characterized by pro-gressive destructive arthritis associated with deformation and impairment of the function of the motor system. RA patients more often present secondary osteoporosis and increased risk of fractures. The aetiology of the process remains not fully understood. A significant role is played by proinflammatory cytokines being common mediators of both inflammatory processes and bone remodelling.
Objectives. The purpose of the study was to evaluate the effect of activity of the inflammation and of applied the-rapy on osteogenesis marker concentrations in RA patients.
Material and Methods. Thirty six female patients with RA, confirmed according to ACR criteria, aged from 35 to 77 years were qualified into the study. A control group included 45 healthy women aged between 34 and 78 years. Clinical evaluation (number of painful and swollen joints, DAS 28) and evaluation of RA laboratory activity (ESR, CRP, blood cell count) and levels of selected bone metabolism markers (osteocalcin, PICP) and serum interleukin 1 levels were performed to carry out the study. X-rays of hands and densitometric scanning of the femoral bone neck and spine were completed in order to assess the advancement of lesions in the bones.
Results. Osteocalcin and PICP levels were significantly lower in the RA groups compared to the control group (2.51 ± 0.22 pg/mL vs. 18.65 ± 12.84 pg/mL, p < 0.0001; 0.292 ± 0.047 pg/mL vs. 0.829 ± 0.263 pg/mL, p < 0.0001 respectively). A statistically significant difference was also observed between the levels of osteocalcin and PICP in both sub-groups of RA patients (DAS28 ≤ 5.1 and DAS28 > 5.1) and the control (osteocalcin 2.48 ± 0.23 pg/mL
vs. 18.65 ± 12.84 pg/mL, p < 0.0001; 2.52 ± 0.22 pg/mL vs. 18.65 ± 12.84 pg/mL, p < 0.0001 respectively and PICP 0.281 ± 0.053 pg/mL vs. 0.829 ± 0.263 pg/mL, p < 0.0001; 0.298 ± 0.044 pg/mL vs. 0.829 ± 0.263 pg/mL, p < 0.0001 respectively). No correlation was demonstrated between the levels of selected bone metabolism markers and the therapy with methotrexate or cyclosporine.
Conclusions. Analysis of the obtained results confirms the presence of disorders of bone metabolism in RA patients. A chronic inflammatory process favors the development of osteoporosis in RA patients. Reduced levels of bone metabolism markers (osteocalcin, PICP) in the study group, compared to the control, may indicate a reduced pace of osteogenesis in RA patients. No effect of therapy with methotrexate and cyclosporine on bone metabolism in that group of patients was found (Adv Clin Exp Med 2013, 22, 2, 193–202).
Key words: rheumatoid arthritis, osteoporosis, bone metabolism, osteocalcin, women.
Streszczenie
Wprowadzenie. Reumatoidalne zapalenie stawów (r.z.s.) jest przewlekłą układową chorobą tkanki łącznej, która charakteryzuje się postępującym destrukcyjnym zapaleniem stawów z deformacjami i upośledzeniem funkcji narzą-du ruchu. W tej grupie pacjentów częściej występuje osteoporoza wtórna i zwiększone ryzyko złamań. Patogeneza tego zjawiska nie została do końca wyjaśniona. Istotną rolę pełnią cytokiny prozapalne, które są wspólnymi media-torami procesów zapalenia i remodelingu kostnego.
Adv Clin Exp Med 2013, 22, 2, 193–202 ISSN 1899–5276
ORIgINAL PAPERS
Rheumatoid arthritis (RA) is an autoimmune, systemic disease of connective tissue. It is charac-terized by chronic synovitis accompanied by de-struction of cartilage and osseous changes [1]. RA is an important risk factor of osteoporosis and oc-currence of fractures [2, 3]. Many authors describe a significantly higher frequency of osteoporosis and fractures in patients with RA in comparison to a control group [4, 5]. The aetiology of progres-sive bone mass loss in RA patients is multi-facto-rial and remains obscure. Factors related to the pathological process – activity of RA and applied therapy – seem to be significant [6].
An active part in development of the inflamma-tion in RA patients is played by cytokines secreted by synoviocytes, macrophages, dendritic cells and endothelial cells. An important role is played by, among others, interleukin 1 (IL-1), interleukin 6 (IL-6) and tumor necrosis factor (TNFα). They are the same time mediators of the inflammatory pro-cess and bone remodeling [7, 8]. Previous studies also indicate a common basis for generalized bone mass loss and local damage of joints, observed in radiological examinations [9]. Many authors claim that active inflammation even in the early stage of RA influences bone mineral density [10, 11].
Bone is a living tissue, demonstrating metabol-ic activity. It undergoes constant remodeling that ensures maintenance of the structural integrity of the osseous system, repair of micro-damage and exchange of its components with body fluids [12, 13]. Regardless of the primary cause, osteoporosis is a result of a disturbed balance between the pro-cesses of resorption and formation of the osseous tissue [14]. The intensity of these processes may
be evaluated using markers of bone metabolism. These are protein structural fragments of bone, enzymes or proteins released into the circulation during the activity of osteoclasts and osteoblasts [15]. The level of bone metabolism markers indi-cates the resultant activity of all processes of re-sorption and osteogenesis present at a given mo-ment within the whole skeleton. Determination of these markers may facilitate fracture prognosis or evaluation of changes in bone mass during phar-macotherapy of osteoporosis [13].
Studies on the evaluation of bone marker lev-els in RA patients most often describe an increased resorption of the bone tissue [16]. Increased levels of some biochemical markers of bone resorption are associated with a more rapid progression of joint destruction in patients with early rheumatoid arthritis and local bone erosion [17]. The forma-tion process is unclear in RA patients. Levels of bone formation markers have been variously re-ported to be normal, elevated or reduced [18].
This study tries to provide an answer to the question if, and to what extent, the activity of RA affects the levels of selected osteogenic markers (osteocalcin, PICP).
Material and Methods
Characteristics of Study Groups
Thirty six women with RA diagnosed as per the ACR criteria of 1987, hospitalized at the Clinic of Rheumatology and Internal Diseases of the Ac-ademic Clinical Hospital in Wrocław, and in the Department of Internal Diseases andRheumatolo-Cel pracy. Ocena wpływu aktywności zapalenia i stosowanej terapii na stężenie markerów kościotworzenia u cho-rych na reumatoidalne zapalenie stawów.
Materiał i metody. Do badania zakwalifikowano 36 kobiet chorych na r.z.s. wg kryteriów ACR w wieku 35–77 lat. grupę kontrolną stanowiło 45 zdrowych kobiet w wieku 34–78 lat. W pracy oceniano kliniczną (liczba bolesnych i obrzękniętych stawów, DAS 28) i laboratoryjną aktywność r.z.s. (OB, CRP, morfologia), a także stężenie osteokal-cyny, PICP, interleukiny 1 w surowicy. Aby określić zaawansowanie zmian w układzie kostnym, wykonywano RTg rąk oraz badanie densytometryczne szyjki kości udowej i kręgosłupa.
Wyniki. Stężenie osteokalcyny i PICP było istotnie statystycznie mniejsze u chorych na r.z.s. niż w grupie kontrol-nej (odpowiednio 2.51 ± 0.22 pg/mL vs 18.65 ± 12.84 pg/mL, p < 0.0001; 0.292 ± 0.047 pg/mL vs 0.829 ± 0.263 pg/ mL, p < 0.0001). Zaobserwowano także różnicę istotną statystycznie między stężeniem osteokalcyny, PICP w obu podgrupach pacjentów z reumatoidalnym zapaleniem stawów (DAS28 ≤ 5.1 and DAS28 > 5.1) i grupą kontrolną (odpowiednio osteokalcyna 2.48 ± 0.23 pg/mL vs 18.65 ± 12.84 pg/mL, p < 0.0001; 2.52 ± 0.22 pg/mL vs 18.65 ± 12.84 pg/mL, p < 0.0001 i odpowiednio PICP 0.281 ± 0.053 pg/mL vs 0.829 ± 0.263 pg/mL, p < 0.0001; 0.298 ± 0.044 pg/mL vs 0.829 ± 0.263 pg/mL, p < 0.0001). Nie wykazano zależności między stężeniem wybranych markerów metabolizmu kostnego a stosowaniem metotreksatu, cyklosporyny.
Wnioski. Analiza uzyskanych wyników badań potwierdza istnienie zaburzeń metabolizmu kostnego u chorych na reumatoidalne zapalenie stawów. Przewlekły proces zapalny jest czynnikiem nasilającym występowanie osteoporo-zy u chorych na r.z.s. Zmniejszone stężenia markerów metabolizmu kostnego (osteokalcyny, PICP) w grupie bada-nej w porównaniu z grupą kontrolną mogą świadczyć o spowolnieniu procesu tworzenia tkanki kostbada-nej u chorych na reumatoidalne zapalenie stawów. Nie stwierdzono wpływu terapii metotreksatem i cyklosporyną na metabolizm tkanki kostnej w tej grupie pacjentów (Adv Clin Exp Med 2013, 22, 2, 193–202).
gy in the PKP Hospital in Wrocław, aged between 35 and 77 years (mean age 58.2; standard deviation s = 10.9, median value xmed = 56) were qualified for
the study. The characteristic of the patients with RA are presented in Table 1.
A control group included 45 healthy women aged between 34 and 78 (mean age 56.4; standard deviation s = 10.3; median value xmed = 58)
recruit-ed among blood donors, healthcare professionals and their families.
Scope of Tests
Evaluation of the clinical and laboratory activ-ity of the disease and determination of the levels of selected bone metabolism markers in RA patients were performed.
The DAS28 index, commonly used in clinical practice and in studies of the efficacy of a therapy activity, was used for evaluation of rheumatoid ar-thritis intensity. The index involves both edema-tous joints (physical examination by a physician – objective evaluation), intensity of pain of joints during the last week (patient’s subjective evalua-tion) and a laboratory parameter of activity of the disease – ESR (objective evaluation). A high
activ-ity of RA is reflected by a DAS28 score over 5.1. This value was adopted as a limiting one (accord-ing to EULAR guidelines).
Markers of osteogenesis were assayed – osteo-calcin (hOST EASIA Kit KAP 1381, BioSource, normal range: 5–25 ng/mL), PICP (Procollagen Type I C-Peptide EIA Kit, Takara Bio Inc, normal range: 0.01–0.64 pg/mL) and interleukin 1 (Quan-tikine Human IL-1β Immunoassay, R&D Systems Inc, Minneapolis, MN, USA, normal range: up to 3.9 pg/mL).
Imaging techniques were used to evaluate changes occurring in the osseous system: X-ray and densitometric scanning (DXA) of the proxi-mal epiphysis of the femur and lumbar spine. Ra-diological examination of hands was performed, because of the occurrence of changes characteris-tic for RA in that area, and to evaluate the stage of progression of the disease (acc. to the Steinbrocker classification).
The study obtained permission from the Bio-ethical Commission operating by the Wroclaw Medical University in Wrocław. The majority of the tests were financed from funds granted by the Committee of Scientific Research (N 402 048 32/1494; gR – 672/2007).
Table 1. Characteristic of the 36 patients with RA
Tabela 1. Charakterystyka 36 pacjentów z r.z.s. Demographic (Czynniki demograficzne) Female (Kobiety) [%]
Age – years (Wiek – lata)
Post-menopausal (Odsetek kobiet po menopauzie) [%] Body mass index (Wskaźnik masy ciała) [kg/m²]
100 58.2 (35–77) 77.8 25.8 (18–35) Disease (Choroba)
Rheumatoid arthritis duration – years (Czas trwania reumatoidalnego zapalenia stawów – lata) Rheumatoid factor-positive (Dodatni czynnik reumatoidalny) [%]
Disease activity score comprising 28 joints (Wskaźnik aktywności choroby DAS28) Visual analogue score (Wizualna skala analogowa bólu) [mm]
Steinbrocker functional class – % in class IV (Zaawansowanie zmian kostnych wg Stein- brockera – % w klasie IV)
Standardized BMD hip (Standaryzowane BMD biodra) [g/cm²] Standardized BMD spine (Standaryzowane BMD kręgosłupa) [g/cm²] 10-year risk fracture FRAX (10-letnie ryzyko złamań FRAX) [%]
13.3 (1–35) 86.1 5.8 (2.6–8.4) 60.9 (10–100) 41.7
827.3 (444.5–1334.4) 957.9 (614.0–1323.9) 21.8 (8–61)
Laboratory investigation (Badania laboratoryjne)
Erythrocyte sedimentation rate (Odczyn Biernackiego) [mm/h] C-reactive protein (Białko C-reaktywne) [mg/dL]
Leucocyte (Leukocyty) [tys./mm³] Hemoglobin (Hemoglobina) [g/dL] Thrombocyte (Płytki krwi) [tys./mm³]
Calcium in serum (Wapń całkowity we krwi) [mg/dL]
42 (7–112) 20.2 (3.0–80.7) 8.5 (4.2–16.4) 12.0 (8.9–14.5) 283 (82–500) 9.4 (8.4–11.2) Medication (Leki)
Methotrexate use present (Odsetek chorych obecnie stosujących metotreksat) [%] Cyclosporine use present (Odsetek chorych obecnie stosujących cyklosporynę) [%] Steroid use present (Odsetek chorych obecnie stosujących steroidoterapię) [%] Duration of steroid use – years (Czas trwania steroidoterapii – lata)
Statistical Analysis
The results are presented as mean ± standard deviation. Normality of distribution was verified using a Shapiro-Wilk normality test. If normal dis-tribution was proved, a comparison of the groups was performed with a parametric Student t-test. If the distribution of markers was significantly dif-ferent from normal distribution, a non-paramet-ric Mann-Whitney U test was used for compari-son. The results were treated as significant if the p value was less than 0.05. The statistical analysis was performed with STATISTICA 9 AXFP104-B401313AR-K, Wroclaw Medical University, Po-land.
Results
Comparative Evaluation of
Levels of Bone Metabolism
Markers in RA Patients and in
the Control Group
Osteocalcin and PICP levels were significantly lower in the RA groups compared to the control group (2.51 ± 0.22 pg/mL vs. 18.65 ± 12.84 pg/mL, p < 0.0001; 0.292 ± 0.047 pg/mL vs. 0.829 ± 0.263 pg/mL, p < 0.0001). Moreover, a higher concentra-tion of interleukin 1 in the serum of RA patients was found, compared to the values determined in
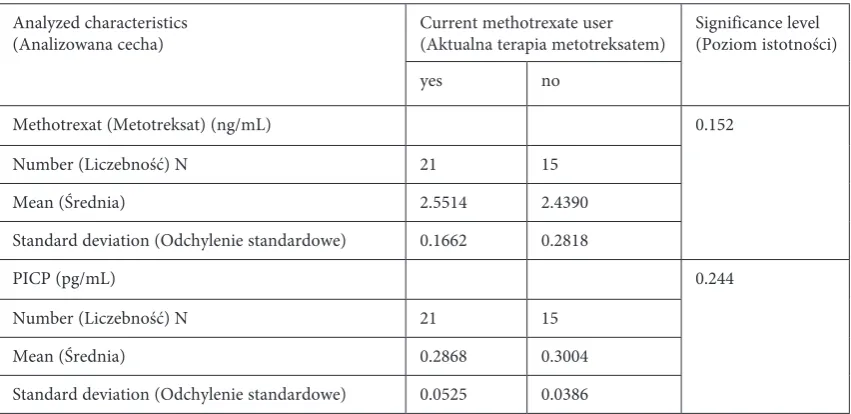
Table 2. Analysis of levels of individual markers of bone metabolism in relation to use of methotrexate therapy
Tabela 2. Analiza stężeń wybranych markerów obrotu kostnego w zależności od stosowania w terapii metotreksatu
Analyzed characteristics
(Analizowana cecha) Current methotrexate user(Aktualna terapia metotreksatem) Significance level(Poziom istotności)
yes no
Methotrexat (Metotreksat) (ng/mL) 0.152
Number (Liczebność) N 21 15
Mean (Średnia) 2.5514 2.4390
Standard deviation (Odchylenie standardowe) 0.1662 0.2818
PICP (pg/mL) 0.244
Number (Liczebność) N 21 15
Mean (Średnia) 0.2868 0.3004
Standard deviation (Odchylenie standardowe) 0.0525 0.0386
Table 3. Analysis of levels of individual markers of bone metabolism in relation to use of cyclosporine therapy
Tabela 3. Analiza stężeń wybranych markerów obrotu kostnego w zależności od stosowania w terapii cyklosporyny
Analyzed characteristics
(Analizowana cecha) Current cyclosporine user(Aktualna terapia cyklosporyną) Significance level(Poziom istotności)
yes no
Osteocalcin (Osteokalcyna) (ng/mL) 0.731
Number (Liczebność) N 9 27
Mean (Średnia) 2.521778 2.498778
Standard deviation (Odchylenie standardowe) 0.114413 0.253167
PICP (pg/mL) 0.869
Number (Liczebność) N 9 27
Mean (Średnia) 0.2907 0.2931
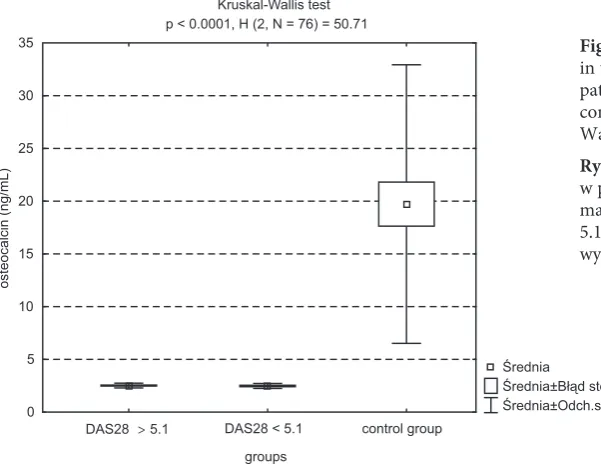
Kruskal-Wallis test p < 0.0001, H (2, N = 76) = 50.71
Średnia Średnia±Błąd std Średnia±Odch.std DAS28 > 5.1 DAS28 < 5.1 control group
groups 0
5 10 15 20 25 30 35
osteocalcin (ng/mL
)
Fig. 1. Mean osteocalcin level in control and study groups
Ryc. 1. Średnie stężenie osteokalcyny w grupach kon-trolnej i badanej
Fig. 2. Mean of PICP level in control and study groups
Ryc. 2. Średnie stężenie PICP w grupach kontrolnej i badanej
Fig. 3. Mean IL-1β level in control and study groups
Ryc. 3. Średnie stężenie IL-1β w grupach kontrolnej i badanej
Fig. 4. Comparison of osteocalcin levels in the subgroup of rheumatoid arthritis patients: DAS28 > 5.1, DAS28 ≤ 5.1 and control group and the result of Kruskal-Wallis test
Ryc. 4. Porównanie stężenia osteokalcyny w podgrupach kobiet chorych na reu-matoidalne zapalenie stawów: DAS28 > 5.1, DAS28 < 5.1 i grupie kontrolnej oraz wynik testu Kruskala-Wallisa
0,00 5,00 10,00 15,00 20,00 25,00
control group
17.92 RA group2.5
osteocalcin mg/m
L
0,00 0,10 0,20 0,30 0,40 0,50 0,60 0,70 0,80 0,90
control group
0.83 RA group0.29
PICP
pg/m
L
0,00 0,50 1,00 1,50 2,00 2,50 3,00
control group
0.83 RA group2.6
IL-1β pg/mL
the control group (2.60 ± 0.63 pg/mL vs. 0.83 ± 0.57 pg/mL, p < 0.0001).
Evaluation of Levels of Bone
Metabolism Markers in Relation
to RA Activity Measured
with DAS28
dif-ferences were observed between both subgroups. The results are presented in Figs. 4 and 5.
The sub-groups of women presenting different indexes of activity of the disease (group I: DAS28 ≤ 5.1, group II: DAS28 > 5.1) demonstrated sta-tistically significant differences in relation to the following:
– the ratio of patients with positive RF – latex (66.7% vs. 95.8%, p = 0.020),
– the average time of therapy with glucocor-ticosteroids (7.8 ± 5.3 years vs. 4.3 ± 3.5 years, p = 0.046).
No significant difference between the other analyzed characteristics (e.g. age, number of post-menopausal women, years after menopause, dura-tion of RA, advancement of RA acc. to X-ray
scan-ning, 10-year risk of fracture) analyzed in relation to the DAS28 value was found.
Evaluation of Levels of Bone
Metabolism Markers in Relation
to the Therapy of RA
No statistically significant relationship was found between the level of osteocalcin and PICP and the use of methotrexate or cyclosporine (Ta-bles 2 and 3). Analysis of the a.m. markers of bone metabolism showed no statistically significant dif-ferences between the users and non-users of ste-roid therapy. However, a higher PICP level was found in women treated with glucocorticosteroids
Kruskal-Wallis test p <0.0001, H (2, N = 76) = 56.37
Mediana 25%-75% Min-Maks
DAS28 > 5.1 DAS28 < 5.1 control group
groups 0,0
0,2 0,4 0,6 0,8 1,0 1,2 1,4 1,6
PICP
(pg/mL
)
U Mann-Whitney test p = 0.034, Z = -2.112
Mediana 25%-75% Min-Maks
up to 10 years more than 10 years
RA duration -2
0 2 4 6 8 10 12 14 16 18 20
duration of glucocorticosteroids treatment
Fig. 5. Comparison of PICP levels in the subgroup of rheumatoid arthritis patients: DAS28 > 5.1, DAS28 < 5.1 and control group and the result of Kruskal-Wallis test
Ryc. 5. Porównanie stężenia PICP w podgrupach kobiet chorych na reuma-toidalne zapalenie stawów: DAS28 > 5.1, DAS28 < 5.1 i grupie kontrolnej oraz wynik testu Kruskala-Wallisa
Fig. 6. Comparison of duration of glu-cocorticosteroids treatment in the sub-groups with various duration of RA and the result of U Mann-Whitney test
(gKS) for over 12 months compared to women treated for a shorter period of time. No correlation was observed between the accumulated gCS dose and the level of PICP and osteocalcin.
Evaluation of Levels of Bone
Metabolism Markers in Relation
to Duration of RA
No statistically significant differences were ob-served between the subgroups with various dura-tion of the disease (group I – up to 10 years, group II – 11 years and longer) in relation to age, num-ber of post-menopausal women, numnum-ber of low-energy fractures, number of patients with a
sero-positive form of RA and the dose of currently-used steroid therapy.
Statistically significant differences between the subgroups of women with various durations of RA (group I – up to 10 years, group II – 11 years and lon-ger) were observed for the following characteristics:
– duration of gKS treatment (Fig. 6), (3.7 ± 2.8 years vs. 7.2 ± 5.1 years, p = 0.034),
– standardized BMD in DXA of the neck of the femur (Fig. 7), (914.9 ± 194.9 vs. 659.1 ± 247.3, p = 0.007),
– duration of postmenopausal period (Fig. 8), (5.5 ± 7.1 years vs. 15.7 ± 7.8 years, p = 0.025).
Moreover, a difference was observed in the number of patients in the compared subgroups in relation to the stage of advancement of the disease
U Mann-Whitney test p = 0.007, Z = 2.674
Mediana 25%-75% Min-Maks
up to 10 years more than 10 years
RA duration 400
500 600 700 800 900 1000 1100 1200 1300 1400
standardised BMD in DX
A
of the neck of the femu
r
U Mann-Whitney test p = 0.025, Z = 2.234
Mediana 25%-75% Min-Maks
more than 10 years up to 10 years
RA duration -5
0 5 10 15 20 25 30 35
duration of postmenopausal period
Fig. 7. Comparison of standardised BMD in DXA of the neck of the femur in the subgroups with various duration of RA and the result of U Mann-Whitney test
Ryc. 7. Porównanie standaryzowanej BMD w DXA szyjki kości udowej w podgrupach różniących się czasem trwania choroby oraz wynik testu
U Manna-Whitneya
Fig. 8. Comparison of duration of post-menopausal period in the subgroups women with various duration of RA and the result of U Mann-Whitney test
as revealed by an X-ray. In women suffering from RA for up to 10 years, the 2nd stage of advancement
acc. to the Steinbrocker classification predominat-ed, and in women suffering from RA for 11 years or longer – the 4th stage (p = 0.011).
Discussion
Osteoporosis is a significant complication of rheumatoid arthritis, having an additional nega-tive effect on patients’ quality of life. Progressive bone mass reduction is a result of numerous fac-tors. Some of them are known, and their effect is confirmed. They are old age, gender, postmeno-pausal period of life, unbalanced diet or tobacco smoking. However, there are still doubts whether osteoporosis depends on the activity of RA, its du-ration and applied therapy.
Studies completed by numerous authors have demonstrated a significantly higher prevalence of osteoporosis in the group of RA patients compared to healthy controls [4, 5]. A statistically significant relationship was found between the development of osteoporosis and the time of advancement of the disease [19, 20]. Also in this study, a more frequent osteoporosis prevalence was observed in patients with a long-lasting RA.
According to many authors, the activity of RA is the main factor deciding the level of intensity of generalized osteoporosis in that pathology [21]. Excessive production of proinflammatory cytok-ines, including IL-1, TNF-alpha and IL-6, plays an important role in the stimulation of the catabolic processes of the osseous tissue, leading to its de-struction [22]. Their increased levels compared to the control group were found in RA patients [23]. This observation is also confirmed by the results of this study. In RA patients, increased CRP level and ESR value were associated with an intensified loss of BMD in hand bones [24]. Franck et al. [5] dem-onstrated significantly lower BMD values of the femoral bone neck in patients with elevated CRP (CRP > 5 mg/L). However, Hafez et al. [25] ob-served an increased DAS28 index in patients with early RA meeting the densitometric criteria of os-teoporosis compared to patients with a regular mineral density of bones or osteopenia, although the difference was not statistically significant.
Secondary osteoporosis develops in RA pa-tients as a result of a disturbed homeostasis of bone metabolism. Numerous authors point out the intensification of the process of resorption of osseous tissue [5, 26]. The process of the formation of osseous tissue has not been precisely understood yet. There are only a few studies focusing on that phenomenon. Wisłowska et al. [20] did not find
a correlation between the intensification of RA ac-tivity measured by the DAS28 index and the level of a marker of osteogenesis: procollagen type I N-terminal propeptide (PINP). This study also failed to observe a relationship between the DAS28 in-dex and levels of osteocalcin and PICP. However, in both subgroups of patients (DAS28 ≤ 5.1 and DAS28 > 5.1), statistically significantly lower levels of osteocalcin and PICP were found compared to the control group (p < 0.0001). Dequeker [10] sug-gested that the activity of RA may only be reflected by periarticular osteoporosis, and only during the early stage of the disease, because only there and then does the condition depend solely on the active phase of inflammation. That opinion seems to ex-plain the results presented here, as patients suffer-ing from RA for multiple years had been included. Despite the fact that momentary activity did not correlate with the markers of bone metabolism, repeated episodes of exacerbation affected ad-vancement of the disease and associated bone loss. Decreased levels of the bone metabolism markers osteocalcin and PICP in the study group compared to the control group may reflect inhibition of the formation of osseous tissue in RA patients.
Literature data indicates that the administration of cyclosporine may affect osteoblasts and osteoclasts, leading to a prevalence of the processes of resorption over osteogenesis, and therefore to more pronounced bone mass loss [31]. Previous clinical research indi-cating an unfavorable effect of cyclosporine on bone mineral density and risk of fractures were based on large doses of the drug used in transplantology [32]. It is believed nowadays that a dose of 5 mg/kg/day or less of cyclosporine used in RA has no unfavorable effects on bone metabolism [33]. This observation is confirmed by the results of this study. No statistically significant correlation was observed between the level of osteocalcin and PICP and the use of cyclosporine at a dose of 2–3.5 mg/kg/day. Also Mazzantini et al. [34], comparing patients treated with CsA and pa-tients receiving no treatment with the drug noted that the mean values of the T-score in densitomet-ric scanning of the neck of the femur or spine were comparable. The ratio of patients with osteoporosis was also not different in those groups. However, ana-lyzing the duration of the therapy, a lower mineral density of bones was observed in patients treated with cyclosporine for over 24 months, than in those treated for shorter period of time.
glucocorticosteroids (gCS) exert a confirmed effect on the osseous tissue. There are numerous pa-pers describing the intensification of the process of resorption and progressive bone mass loss, as well as the development of osteoporosis as a complication of long-term steroid therapy. On the other hand, however, an important role in the optimal con-trol of the inflammatory process in RA patients is
stressed. Some authors indicate that along with the use of DMARDs for the achievement of remission, a short-term therapy with low doses of glucocorti-costeroids may be also favorable [35]. Korczowska et al. [36] found no statistical differences between the level of osteocalcin in RA patients and in the control group, with higher concentration of pro-collagen type I C-terminal propeptide in the group of RA patients. Following a 12-month follow-up, the authors demonstrated, however, a statistically significant reduction of osteogenic markers in RA patients who had glucocorticosteroids introduced for the first time. Also Engwall et al. [37] observed a reduced level of the marker of osteogenesis (pro-collagen type I N-terminal propeptide) in patients with early RA treated with prednisone. The results of this study indicate no relationship between the use of gCS and the level of osteocalcin and PICP. This observation may be a result of the fact that the highest remodeling takes place during the first 6–12 months of steroid therapy [38], and a result of the selection of the study group – a significant majority of qualified women used steroids for periods longer than 12 months years.
Summing up the results of the above study, the presence of a disturbance in bone metabolism in RA patients has to be confirmed. A chronic inflammatory process is a factor intensifying the development of osteoporosis in RA patients. Re-duced levels of bone metabolism markers (osteo-calcin, PICP) in the study group compared to the control may reflect a reduced intensity of the pro-cess of osteogenesis in RA patients.
References
[1] Scott DL, Wolfe F, Huizinga TWJ: Rheumatoid arthritis. Lancet 2010, 376, 1094–1108.
[2] Broy SB, Tanner SB and on behalf of the FRAX Position Development Conference Member: Official Positions for FRAX Clinical Regarding Rheumatoid Arthritis. J Clin Densitom 2011, 14, 3, 184–189.
[3] Kim SY, Schneeweiss S, Liu J, Daniel GW, Chang CL, Garneau K, Solomon DH: Risk of osteoporotic fracture in a large population-based cohort of patients with rheumatoid arthritis. Arthritis Res Ther 2010, 12, 154–164.
[4] Macovei L, Ancuta C, Belibou C, Chirieac R: Bone mineral density in patients with rheumatoid arthritis. Rev Med Chir Soc Med Nat Iasi 2011, 115, 3, 723–730.
[5] Franck H, Gottwalt J: Peripheral bone density in patients with rheumatoid arthritis. Clin Rheumatol 2009, 28, 1141–1145.
[6] Lacativa PG, Farias ML: Osteoporosis and inflammation. Arq Bras Endocrinol Metab 2010, 54, 2, 123–132.
[7] Oelzner P, Hein G: Inflammation and bone metabolism in rheumatoid arthritis. Pathogenetic viewpoints and therapeutic possibilities. Med Klin 1997, 92, 10, 607–614.
[8] Shiozawa S, Kuroki Y: Osteoporosis in rheumatoid arthritis: a molecular biological aspect of connective tissue gene activation. Tohoku J Exp Med 1994, 173, 1, 189–198.
[9] Solomon DH, Finkelstein JS, Shadick N, LeBoff MS, Winalski CS, Stedman M, Glass R, Brookhart MA, Weinblatt ME, Gravallese EM: The relationship between focal erosions and generalized osteoporosis in postme-nopauzal women with rheumatoid arthritis. Arthritis Rheum 2009, 60, 1624–1631.
[10] Urbanek R, Tłustochowicz W, Patoła J, Głodzik J: Częstość występowania osteoporozy u chorych na reumato-idalne zapalenie stawów. Prz Lek 2000, 57, 2, 103–107.
[11] Ferraccioli G, Casatta L, Bartoli E: Increase of bone mineral density and anabolic variables in patients with rheu-matoid arthritis resistant to methotrexate after cyclosporin A therapy. J Rheumatol 1996, 23, 1539–1542.
[12] Raisz LG: Pathogenesis of osteoporosis: concepts, conflicts and prospects. J Clin Invest 2005, 115, 3318–3324.
[14] Kmieć Z, Sokołowska I: Rola cytokin z rodziny czynnika martwicy nowotworu w przebiegu reumatoidalnego zapalenia stawów – nowe możliwości terapii. Pol Mer Lek 2007, XXII, 130, 300–304.
[15] Datta HK, Ng WF, Walker JA, Tuck SP, Varanasi SS: The cell biology of bone metabolism. J Clin Pathol 2008, 61, 5, 577–587.
[16] Geusens P, Lems WF: Osteoimmunology and osteoporosis. Arthritis Res Ther 2011, 13, 5, 242.
[17] Garnero P, Delmas PD: Noninvasive techniques for assessing skeletal changes in inflammatory arthritis: bone biomarkers. Curr Opin Rheumatol 2004, 16, 4, 428–434.
[18] Singer FR, Eyre DR: Using biochemical markers of bone turnover in clinical practice. Cleve Clin J Med 2008, 75, 10, 739–750.
[19] Forsblad-d’Elia H, Carlsten H: Bone mineral density by digital X-ray radiogrammetry is strongly decreased and associated with joint destruction in long-standing. Rheumatoid Arthritis: a cross-sectional study. BMC Musculoskelet Disord 2011, 12, 242–250.
[20] Wisłowska M, Jakubicz D, Stępień K, Cicha M: Serum concentrations of formation (PINP) and resorption (Ctx) bone turnover markers in rheumatoid arthritis. Rheumatol Int 2009, 29, 1403–1409.
[21] Rell-Bakalarska M: Osteoporoza w reumatoidalnym zapaleniu stawów. Post Nauk Med 2008, XXI, 6, 381–388.
[22] Korczowska I, Olewicz-Gawlik A, Trefler J, Hrycaj P, Łącki K: Does low-dose and short-term glucocorticoids treatment increase the risk of osteoporosis in rheumatoid arthritis female patients? Clin Rheum 2008, 27, 565–572.
[23] Kokebie R, Aggarwal R, Lidder S, Hakimiyan AA, Rueger DC, Block JA, Chubinskaya S: The role of synovial fluid markers of catabolism and anabolism in osteoarthritis, rheumatoid arthritis and asymptomatic organ donors. Arthritis Res Ther 2011, 13, R50, 2–10.
[24] Boyesen P, Hoff M, Odegard S, Haugeberg G, Syversen SW, Gaarder PI, Okkenhaug C, Kvien TK: Antibodies to cyclic citrullinated protein and erythrocyte sedimentation rate predict hand bone loss in patients with rheuma-toid arthritis of short duration: a longitudinal study. Arthritis Res Ther 2009, 11, 4, R103.
[25] Hafez EA, Mansour HW, Hamza, Moftah SG, Younes TB, Ismail MA: Bone mineral density in patients with recent-onset rheumatoid arthritis. Clin Med Insights Arthritis Musculoskelet Disord 2011, 4, 87–94.
[26] Braun T, Zwerina J: Positive regulators of osteoclastogenesis and bone resorption in rheumatoid arthritis. Arthritis Res Ther 2011, 13, 235–246.
[27] Kucharz EJ: Reumatoidalne zapalenie stawów. Antczak A, Myśliwiec M, Pruszczyk P: Wielka Interna. Puszczewicz M (red): Reumatologia. Med Tribune Pol 2011, 75–88.
[28] Fan C, Georgiou KR, King TJ, Xian CJ: Methotrexate toxicity in growing long bones of young rats: a model for studying cancer chemotherapy-induced bone growth defects in children. J Biomed Biotechnol 2011, 903097.
[29] Stava CJ, Jimenez C, Hu MI, Vassilopoulou-Sellin R: Skeletal sequelae of cancer and cancer treatment. J Cancer Surviv 2009, 3, 75–88.
[30] Torikai E, Kageyama Y, Takahashi M, Nagano A: The effect of methotrexate on bone metabolism markers in patients with rheumatoid arthritis. Mod Rheumatol 2006, 16, 350–354.
[31] Rell-Bakalarska M: Przyczyny osteoporozy wtórnej. Choroby układu ruchu. Osteoporoza wtórna osób dorosłych. Przedlacki J, Rell-Bakalarska M. Warszawa 2007, 47–60.
[32] Launius BK, Brown PA, Cush EM, Mancini MC: Osteoporosis. The dynamic relationship between magnesium and bone mineral density in the heart transplant patient. Crit Care Nurs Q 2004, 27, 1, 96–100.
[33] Di Munno O, Delle Sedie A, Rossini M, Adami S: Disease-modifying. antirheumatic drugs and bone mass in rheumatoid arthritis. Clin Exp Rheum 2005, 23, 137–144.
[34] Mazzantini M, Di Munno O, Sinigaglia L, Bianchi G, Rossini M, Mela Q, Del Puente A, Frediani B, Cantatore F, Adami S: for the study group on bone mass in rheumatoid arthritis of the Italian society for rheumatology: Effect of cyclosporine A on bone density in female rheumatoid arthritis patients: results from a multicenter, cross-sectional study. Clin Exp Rheumatol 2007, 25, 5, 709–715.
[35] Roux C: Osteoporosis in inflammatory joint diseases. Osteoporosis Int 2011, 22, 2, 421–433.
[36] Korczowska I, Łącki JK, Leszczyński P, Mackiewicz SH: Metabolizm tkanki kostnej u chorych na reumatoidalne zapalenie stawów leczonych glikokortykosteroidami. Pol Arch Med Wew 2000, 104, 2, 455–465.
[37] Engvall IL, Svensson B, Tengstrand B, Brismar K, Hafström I, Better Anti-Rheumatic FarmacO Therapy Study group: Impact of low-dose prednisolone on bone synthesis and resorption in early rheumatoid arthritis: experi-ences from a two-year randomized study. Arthritis Res Ther 2008, 10, R128.
[38] Adachi JD, Olsztyński Wp, Hanley DA, Hodsman AB, Kendler DL, Siminoski KG, Brown J, Cowden EA, Goltzman D, Ioannidis G, Josse RG, Ste-Marie LG, Tenenhouse AM, Davison KS, Blocka KL, Pollock AP, Sibley J: Management of corticosteroid-induced osteoporosis. Semin Arthritis Rheum 2000, 29, 4, 228–251.
Address for correspondence:
Agnieszka MatuszewskaDepartment of Pharmacology Wroclaw Medical University J. Mikulicza-Radeckiego 2 50-345 Wrocław
Poland
Tel.: +48 71 784 14 38
E-mail: [email protected]
Conflict of interest: None declared