is “¿ready―to be set off and may serve to discharge accumulated tension—stored from the constant internal and external stimuli acting on the newborn infant. This ability of the neonate to ( 1) delay a response, (2) store tension and (3) discharge it effec tively later in mass activity is impressive evidence of a barrier present in the imma ture central nervous system, which helps to maintain homeostasis.10'@ Thus the cry of the newborn infant is an important part of effective neurophysiologic function in the early days.
Crying begins to be differentiated soon after birth as a response to physiologic needs—such as hunger, temperature change and discomfort. As these demands are met a conditioning element is added, and the cry becomes more and more purposeful. The infant “¿expects―a response from the environment and cries for the mothering that relieves his condition.
A different kind of crying arises soon after the baby arrives at home. This crying is seen during discrete periods of the day, seems cyclic in its regular occurrence, is heightened by environmental tension, but is not eliminated by the obvious methods of relief offered by “¿normal―mothers.
Since the normal crying of the infant may be compounded by environmental ten sion,6 this “¿paroxysmalfussing― can easily become the precursor for many cases of “¿infantilecolic.― Crying in the infant rep resents a failure in mothering to most new, young parents. Their efforts to compensate for this failure may create unnecessary stimuli for the newborn, and the resulting tension is added to his innate reasons for crying. An ever-increasing cycle in the du ration and intensity of the crying may result in the picture of 24-hour “¿colic.―
In pediatric practice early prophylaxis in C RYING in the new infant at home may
become such a problem to parents and pediatrician that it seems important to evaluate its occurrence in “¿normal―infants. It is apparent to all physicians concerned with newborn infants that many infants cry regularly for a part of each day. A regu lar “¿paroxysmalfussing― is described by Wessel et al.1 as occurring in 87% of the babies in a follow-up during the Yale Rooming-in project. These regular crying periods need not be associated with any of the underlying pathology suggested by the literature, viz., congenital hypertoni city, allergy, gross immaturity of the intesti nal tract, or abnormal tension in the en vironment.26 The cyclic regularity of this crying, the fact that it cannot be eliminated by environmental influences, and its com mon occurrence in healthy, happy babies suggests that a certain amount may be “¿normal―for infants in our culture. One wonders whether this normal crying may even serve an important developmental purpose.
THEORY OF CRYING
Crying has physiologic and neurophysio logic usefulness in the early days of neona tal adjustment. Babies survive with the help of their first cry.7'8 This serves as an effec tive force in the re-organization of extra uterine cardiorespiratory function. Various stimuli—internal and external—maintain and improve this function. Stimuli institute startling, which is followed by crying. Cry ing improves pulmonary capacity in the first few days and thus serves a valuable phy siologic purpose.9
Often the stimuli that institute the “¿startle-cry―cycle are mild and seem out of proportion to the resulting response in the baby. It becomes apparent that this cycle
ADDRESS:51 BrattleStreet,Cambridge, Massachusetts.
PEDIATRICS, April 1962 579
CRYING IN INFANCY
the area of parental anxiety may be the most effective method for avoiding colic. The repeated assurance that a certain amount of crying is common and even necessary to a normal infant in the first few months may dispel some of the anxiety
in earnest young parents and eliminate un
necessary tension in the newborn infant.
This study attempts to estimate the in cidence of crying in a group of “¿normal― newborn infants in our culture in whom no apparent pathologic factors were pre sent. The distribution of their fussy periods, the apparent meaning of this activity to them, and its relationship to other behavior in the newborn infant—such as sleeping, feeding and extra-nutritional sucking—is estimated.
METHOD OF STUDY
Eighty mothers seen in private practice in Cambridge, Massachusettes, were asked to keep daily records of crying in their in fants for the first 12 weeks. The daily re cord (Fig. 1) was based on Gesell's 24-hour charts.12
This was not a random sample. The mothers were chosen because they pre
sented a “¿normal―positive approach to mothering their new babies. Fifty-two of these mothers, who had other children, had been previously known to us, and they seemed to be relaxed, competent mothers. It seemed likely that environmental tension
would be at a minimum and couldbe ac
counted for from previous knowledge of them. Twenty-eight mothers were primi paras and were chosen during the newborn
period,withoutpriorcontact.They also
presented no apparent evidence of unusual tension in our early contacts with them.
The demanding effort involved in main taining daily charts for 12 weeks must have been a selective factor. The willingness to co-operate in this type of study denoted a certain intellectual curiosity and/or an in tensity of physician-mother relationship. This may have been a factor that affected the amount of crying in these babies. Since pediatric advice was given freely to all of these mothers, this type of parent may have
been ableto utilizehelp more effectively
and toreducethetotalcryingtime.
Sixteen of these babies were fed with an
evaporatedmilk and Karo formula.Sixty
four were breast fed for all or part of the
Dot.
LI I
123 6
8TtEY 07 I@AE cR@iio
I! I I 1 II I I I@ I@ , t 7 8 9 10 1.112 1 2 3
boo P.$.
__I I II I I I I II
@ 6 7 8
@ 10 11 12 1 2 3
boo P.M.
I I I I M.d—crying
@@ 4 9 10 II -12 5fl5-'S.11r4
Midnight ynlov-sio.pjng
S@@.suckin.g or —¿ other setloity
__________________________________2Z.!@.!-he1dorrocked
I I I I I W-oot.r fs.dlng
6 5 6 7 8 9 10 11 12 B-br..st Midnight 7-foruai.
-1 2 3 6
AM. 5 1 7 0 9 10 1.1boon12 P.M.1 2 3
6 , 6 7@8 9 10.11
Midnight
1236 ,6 7891011121 23
AM. boon P.M. lot.episod.:..sdor ..ch
6 967 8 910 11 12
Midnight
1. suddos or grsdusl 2. OUst due to?
@-1-i 1@[@1 @f:@:•.tc.
8 9 10 11 12 @. rk psok with MIdnight 6. whet r.iised
crying sod for
hoe losog?
(Us•rewerse side of
shoot if n.c.s..ry)
7. lorry lrensltos, M.D.
51 lr.tti. Str..t Csshrd@ 38 boss.
(@I II
65 67
12 3 6 5 t 7 0 9 iOii@ 6 0 .5
0.0. loon P.M.
IIIIIIIII !1I I
.7891011121 23
AM. boon P.M.
±1 1
10 11 12
Midnight
1 2 @@67 8 9 10 11 12 1 2 3
@ 9 6 7 8 9 10 11 12
AM. boos P.M. Midnight
ARTICLES period. For these 64, supplementary form ula was encouraged when indicated. None had any apparent intolerance to food, and all gained well. Allergic families were ex cluded from the study.
Fifty-one babies were male; 29 were female. The babies were evaluated in the newborn nursery to rule out “¿hypertonic ity,―“¿hypotonicity,―or abnormalities of the central nervous system. A routine pedia tric examination as well as a behavioral neurologic examination (methods of Gra ham13 and Taylor-Jones's) were given three times in the first week to each infant. They were re-checked at least twice in the first 12 weeks, and all were followed for at least 12 months thereafter in order to sub stantiate early developmental impressions of normalcy. None of these babies deviated markedly from a so-called “¿average―in psychomotor development.
PEDIATRICADVICE
From a pediatric standpoint, contact was maintained with these mothers by phone at their discretion and according to their needs. New mothers were urged to call at a routine morning call hour as frequently as they deemed necessary, and at least weekly in the first few weeks. The more experienced mothers had a similar oppor tunity but used it less often.
Feeding advice was kept as non-directive as possible. The mothers were initially ad vised to begin with a demand schedule and to use this in stress periods. In general, however, a more reliable but flexible 3-to-4-hour schedule was instituted. Breast-feed ing mothers were urged to offer a formula once a day when it seemed helpful in main taining breast-milk supply. Solids were added after 8 to 10 weeks when the baby seemed unsatisfied with milk feedings.
During the crying periods, mothers were urged to eliminate obvious reasons for cry ing—i.e., to feed them (breast, formula, and, later, solids), to bubble them, to offer lactose periodically (at least hourly) to facilitate mobilization of stomach gas, to change them when wet or dirty, to offer
them more sucking ( either by lactose, fingers or pacifier15), to play with them, to change their position periodically, to place them on their stomachs, to prop them in supine in a 30° position with head up, to rock them,b6 and even to swaddle them. They were not advised as to how much time they should spend in socializing with their babies, but they were urged to do so in these periods. However, it was pointed out that their own tension communicated itself to the infants in bad periods, and that a restrained routine was more effective when this seemed to be likely. They were advised to pick up their babies every 20 to 30 minutes during crying periods, calm them, offer them lactose and bubble them, in order to minimize cyclic hyperactivity and to counteract air swallowing from cry ing. Feedings were not to be offered sooner than 2% to 3 hours in these upset periods.
MOTHERS' DESCRIPTIONOF CRYING PERIODS
4
3
UPPER QUARTILE MEDIAN 2
LOWER QUARTILE
FIG. 2. Summary of the total crying time of the 80 infants studied.
23'@4 5 6 7 R
@ 10 1112
ACE IN WEEk'S
In Figure 3 a spread of fussing is re corded throughout the day, with major concentration from 6 to 11 p.m. This is the period when the father is at home, the
mother is physicallymore exhausted, and
other siblingsare making more demands.
Other humps occur in the early morning
(4 to 7 am.) and latermorning (9 to 11
am.).
At six weeks of age (Fig. 4) the concen
tration of crying is more marked at the end
of the day, with a small hump in the early
morning. The period from 3 to 12 p.m. is
now seen as the intervalin which the long
periods of crying and fussing occur in over half the infants. This would seem to em phasize the environmental influence on the timing of these “¿fussy―periods. Many par ents consciously attempted to manipulate the timing of these periods so that they
occurred at a time when the rest of the
family could tolerate the crying.
At 10 weeks of age (Fig. 5) the infants
were quieting down to a marked extent,
and there were two intervals, 6 to 12 a.m.
and 5 to 11 p.m., when the much-reduced
crying occurred.
#@URSOFFU@S/MC PER24 NR@
5
to let him wait for his feedings, he cried
and fussed more frequentlyduring the day,
but his prolonged crying period was short ened, and she felt that he worked some of it out during these other times. These periods were always longer and more in
tense whenever anyone in the household
was upset.
RESULTS
A summary of the recorded number of hours' crying and fussing in the first 12 weeks for these 80 babies is given in Fig ure 2.
In the second week (the first week at home) there was a median of 1 3/4 hours, with a spread of % hour, in the upper quar tile, and 20 minutes in the lower quartile. There was a gradual increase to a peak median of 2 3/4 hours at 6 weeks, with a decrease in quantity of crying thereafter. This 6 weeks' peak in the surrounding quar tiles was parallel, as was the following de crease. Data for the more extreme cases are summarized in Figures 6 and 7.
ARTICLES
FIG. 3. Time of day of fussing of infants at 3 weeks of age.
NUMBER OF BABIES
hIVES I
II
345671910 II @I234567S9I0 II 12
AM. PM
S
A.M PM
ASSOCIATED ACTIVITY
In summarizing the total amount of cry ing in the two extreme groups, the heavy and the light fussers, it became apparent
36
32
2S
24
20
I6@
12
S
HOURS
that their other activity differed markedly also. In particular, their extra-nutritional sucking activity deviated markedly from the averages for ages reported previously.17
MIMBER OFBABIES
40
12
NUMBER OF BABIES
40
36
32
25
24
20
16
12
S
4
HOURS 12
FIG. 5. Time of day of fussing of infants at 10 weeks of age.
3 4567910 11 12123456719 101112
A.M PM
‘¿Thetotal amount of sucking in these two
groups seemed to bear a reliable inverse
relationship to the total amount of crying.
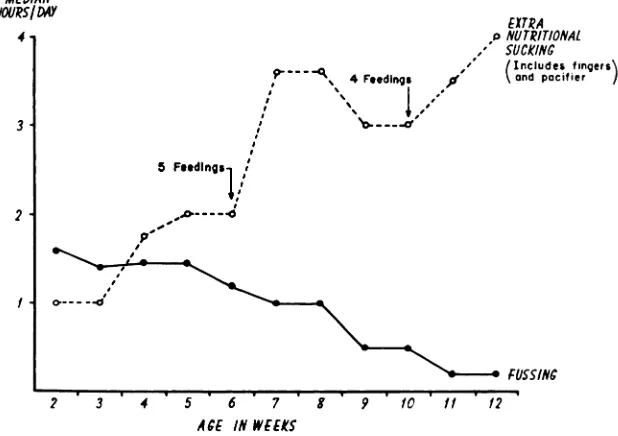
In Figures 6 and 7 the total crying is sum marized, along with the extra-nutritional sucking (i.e., on fingers and pacifier, not directly associated with feedings), as well as with other developmental trends, to
show their relationship to crying time in
these two extreme groups.
@slothers commented that their infants
seemed to substitute finger sucking for fussing at certain times and that a pacifier could reduce the total amount of crying (cf. Levine and BelP@). On observation, this pertained to moderate crying only, and
EXTRA
o NUTRITIONAL
SUCK/NC
,“ (Includes fingers
0
\and
pacifier
MEDIAN HOURS/DAY
4
3
2
- \ 4 F.edlngs
/
@
1@--―
2'3'4'5'6'7'S'9'10'II'12 FUSS/NC
ACE IN WEEKS
ARTICLES
motor accomplishments, seemed somewhat slower in this group of babies than in the heavier fussers.
The average crying time for six heavy fussers is shown in Figure 7. The crying time was 1 hour more than the average at 3 weeks, despite attempts to substitute other environmental outlets. The increase to 4 hours of fussing a day at 6 weeks, which lasted until 8 weeks, remained well above the averages for the total group given in Figure 2. Some of the environmental influ ences that may have played a role are given in the next section.
Coincident with the decrease in crying, which started by 8 weeks, was an increase in other activity, such as sucking, cooing, watching hands, turning over, etc. Extra nutritional sucking was below average for the first 7 weeks, but by 10 weeks had in creased to 2% hours a day. The average for this age group was 2 hours.'7 Whether these new activities represent an improve ment in the neuromuscular organization and in the ability of the infant to satisfy his needs in other ways than by crying, or whether there is a decrease in the gross tension accumulated and less need for such a total kind of discharge as crying, is not answerable by this data. The cumulative time spent in these two types of oral ac
tivity (crying and sucking) increases over
the 12-week period and does not suggest
a decrease in total activity output. That
the over-all organization of the babies in this group may be proceeding rapidly in other ways is suggested by the fact that night feedings were given up by these babies 1% weeks before the quieter babies (Fig. 6).
The amount of total oral activity in these fussier babies, as evidenced by the sum of crying plus sucking, is reliably different and averages one hour more than the total in the quieter babies. This suggests a more vigorous congenital activity type, or one that is more sensitive to accumulated ten sion in the former group. In a study as superficial as this one, however, the early influence of environmental stimuli on the innate characteristics of the individual new sucking would not become a substitute for
more intense fussing. This observation seemed pertinent to the inverse correlation that seemed to exist between the total amount of crying in these infants and their ability to discharge this energy in other activity ( such as sucking) in the early weeks (Fig. 6).
The group of 12 less fussy babies cried an average amount ( 1% hours) during the first week at home but showed a steady decrease in crying thereafter. At 6 weeks, when the average trend was still rising, this group cried less than before and re mained well below average throughout the
12-week period. Because the environmental
influences appeared similar on the surface to the major group, we wondered whether there was an innate difference within these babies in their ability to assimilate stimuli and/or handle accumulated tension, which need not discharge itself as crying. As this study was not set up as an attempt to evalu ate early individual differences in innate equipment, we have had to be content with conjectures based on gross behavior in the divergent groups.
These less fussy babies sucked on their fingers and pacifiers for 1 hour a day for the first 3 weeks. This is only slightly above the average for all babies at this age. But then their sucking time began to increase, and after 6 weeks there was a rapid in crease in time spent in extra-nutritional sucking activity (33@hours versus an aver age of 2 hoursls). This marked increase is coincident with a corresponding rapid in crease in crying time at 6 weeks in the heavy fussers (Fig. 7). The increase in sucking time in the light fussers made us wonder whether this indicated that (1) their ability to effect voluntary hand to mouth organization had improved, so that
it was possible for them and a gratifying
4 FeedIngs
.LookInQ at hands,
mobile turning over
EXTRA (Includes
NUTRITIONAL @fIngersand SUCK/NC
@ @pocLfier
FUSS/NC ,0-- .-.
@1 tCooIng
,0
o----.o._
4
3
2
I
2 3 4 5 6 7 1 9 10 II 12
ACE IN WEEKS
FIG. 7. Summary of total crying time of six heavy fussers.
born infant cannot be accurately evaluated.
More detailed observation of the early in fluence of environment on the crying of
innately different newborn types must be
reserved for future study.
“¿COLIC―
The crying of the heavy fussers seemed to be consistent with the description of daily irritable crying of 3-month colic given
by 18 Their crying periods increased
in duration and intensity until the sixth week; then a plateau existed at 4 hours for
2 weeks, before diminishing. They were not
markedly affected by any of these previ
ously described maneuvers ( e.g., change of
feedings, pacifier or antispasmodics).
Four of the six infants were the first
children, one was a second, the other a
third child. The environmental tension
which resulted from their initial crying was
a large additive factor in all of these cases, according to parents' reports.
A typical report from this group of babies
is as follows : The young mother had be
lieved the hospital nurses' reports that her
baby was quiet in the nursery, and she was
surprised at the amount of crying he did
when they arrived home. She immediately felt guilty and responsible for this “¿change―
in his behavior. She was breastfeeding him,
blamed herself for lack of milk, and tilen for “¿badmilk.―Her husband was also upset
by the infant's crying, alternated between
worrying about the possibility that some
thing was wrong with the baby and being
irritated with him for upsetting their home life. The grandmother, who had come to
help, felt helpless and concerned about her
daughter's exilausted condition. Her ideas
and criticisms thus added to everyone's
mounting tension. The young mother did
“¿everything she knew to do―when the in
fant cried. She rapidly ran the gamut of
picking him up, holding and rocking him,
walking around with him, patting him fun
ously, feeding him every hour, etc. Her ten
sion and hostility to tins situation mounted
with her fatigue and realization of helpless
ness to change it. The baby's crying, which
had begun at rather reliably cyclic inter vals, began to invade all periods, especially
at night. The mother began to lose her milk
with this strain, began to be less effective in
handling the baby, was depressed and fright ened by her negative feelings about the
baby, and wished for someone wllo would
take over. Tile father, who had other, pro
fessional demands on him, was frightened
by the situation and tried to stay away from
Ct al.,6 who found that most “¿colic―oc
curred in relation to environmental ten sions. The evening for every baby in this group was the peak period of tension in the family as a whole. The student-father was at home trying to study. The other sib lings were at their most demanding. To the naturally fatigued mother, the baby's cry ing was at this time the most difficult to stand so that her unconscious resentment must have been transmitted to the infant. By 6 weeks the parents had found that fussing during the hours from 6 to 11 p.m. aborted most of the night fussing. Hence they made a conscious effort to encourage the earlier time. This added a conditioning element to the timing and cyclic nature of these fussy periods.
This study cannot answer the question of whether such cycles of fussing are innate in the neonate or whether they are brought out at regular intervals by environmental influences. But it does suggest that the neo nate is acutely sensitive to the tensions of those around him and may be influenced by them to express his own tension at particu lar intervals during the day.
There was a gradual increase in daily crying needs for 6 weeks. As other ways of discharging tension and of reaching out to the environment became available, there was a constant gradual reduction in the quantity of daily crying. Many parents re ported that their infants seemed to replace these crying periods with sociable inter action with them, or with other activities such as rolling over, watching their hands or other objects, etc. The babies who cried little from the first seemed to be able early to substitute autonomous behavior, such as sucking. But these babies also seemed to need less total oral activity, as there was a reliable difference in the sum of sucking and crying in these two groups, after the second week.
Ribble19 believed that there should be a one-to-one relationship between a baby's protest, an appropriate environmental re sponse, and successful tension discharge on the part of the infant. When this does not seem possible with reasonable effort on the home during the fussy periods. The grand
mother felt unsure of herself and was not able to take over effectively in these crying periods when the mother needed the most help. It became obvious to them all that their tensions transmitted themselves to the infant and increased his own reasons for crying. They seemed unable, however, to take outside advice about remedying the situation. It became obvious to us, on the other hand, that a rather drastic change in the environment was necessary to decrease the crying resulting from the external ten sion surrounding the infant.
In four of these cases maternal grand mothers were present and seemed to be adding to the environmental tension. The parents were urged to change this situation, and more consistent phone supervision was instituted in an attempt to replace the grandmother's positive support. Three of the babies responded with dramatic im provement. In two other cases a nurse was urged to relieve parental fatigue and ten sion—with marked improvement in the babies' crying. In the sixth case, a weekly visit with focus on the mother and her feel ings was instituted, with good results.
By the sixth week, the crying was no longer increasing in any of these babies. By the ninth week it had begun to decrease in intensity and duration. Constant reassur ance that this crying was not in itself detri mental to the baby, as well as the knowl edge that it was self-limited, helped these parents.
COMMENT
In these 80 cases, the mothers described regular crying periods as an important part of the daily activity cycle. The periods were called “¿exerciseperiods― or a time for “¿lettingoff steam.― When these periods were not prolonged by unmet needs or added environmental tension, they tended to be limited in duration.
part of the parent, it is reassuring and even anxiety-reducing to be able to offer conscientious mothers the knowledge that babies may cry for regular periods for their own reasons—such as exercise, tension dis charge, efforts to maintain homeostatis, etc. In these 80 babies there were only 12 who fussed less than 1% hours daily throughout the newborn period. Most of them needed more than 2 hours in the third, fourth and fifth weeks, 2% hours in the sixth week, and 2 hours in the seventh and eighth weeks. Because these babies may reflect the pattern of well-mothered normal babies in our culture, this may be offered as evidence that their crying is not necessarily a reflec tion of environmental neglect.
Obviously this advice cannot be offered until other possible reasons for the infant's crying are well ruled out. An unnecessary amount of crying in an infant must always be the cue for a recognition of environmen tal defects by the pediatrician. In the cases of the six heavy fussers, environmental ma nipulation and attention to environmental tensions brought noticeable results in de creasing the total quantity of crying in the neonate. The innate trend in the newborn toward a better organization must have been a major factor also, but even in these upset babies, total crying began to decrease after 8 weeks, rather than after 10 or 12, when “¿colic―has been reported to be self terminated.1'3'5'8
SUMMARY
Eighty mothers of normal newborn in fants kept daily records of their infants' fussing for the first 12 weeks. Twenty-eight babies were the firstborn in the family. An attempt was made to eliminate excessive environmental tension as an additive factor. Babies with underlying pathology were eliminated also. There was an average of 2% hours' crying in the first 7 weeks, with less each week thereafter. The time of day of its occurrence is summarized. Typical non-fussers sucked their fingers for longer periods each day. Babies who cried an unusual amount responded to manipulation
of environmental tension. The possible in nate reasons for crying in the infant are summarized. The hypothesis is made that a certain amount of crying is necessary. The reassuring aspect of this incidence of crying in “¿normal,―emotionally secure, well-fed infants can be stressed by pediatricians for earnest parents who become anxious about a normal amount of unsatisfiable crying in their own neonate.
REFERENCES
1. Wessel, M. A., et a!.: Paroxysmalfussing in
infancy. PEDIATRICS,14:421, 1954.
2. Aldrich, C. A., et al.: The crying of newly born
babies: III. The early period at home. J.
Pediat., 27:428, 1945.
3. Escalona, S.: Feeding disturbances in very
young children. Amer. J. Orthopsychiat., 15:
76, 1945.
4. Lippman, H. S.: Restlessness in infants.
J.A.M.A., 91:1848, 1928.
5. Spock, B.: Etiological factors in the hyper
trophic stenosis and infantile colic.
Psychosom. Med., 6:162, 1944.
6. Stewart, A., et a!.: Excessive infant crying
(colic) in relation to parent behavior. Amer.
J. Psychiat., 110:687, 1954.
7. Greenacre, P.: Predisposition to anxiety.
Psychoanal. Quart., 10:66, 610, 1941.
8. Ihlingsworth, R. S.: Crying in infants and chil dren. Brit. Med. J., 1:75, 1955.
9. Long, E. C., and Hull, W. E.: Respiratory vol
ume flow in the crying newborn infant.
PEDIATRICS, 27:373, 1961.
10. Benedek, T. B.: Adaptation to reality in early infancy. Psychoanal. Quart., 7:200, 1938.
11. Dewey, E.: Behavior Development in Infants.
New York, Columbia, 1935, pp. 70 if.
12. Gesell, A., and hg, F. L.: Infant and Child
in the Culture of Today. New York, Harper, 1943, pp. 52 if.
13. Graham, F. K.: Behavioral differences between
normal and traumatized newborns. Psychol.
Monogr., 79:20, 1956.
14. Taylor-Jones, L.: Study of behavior in the
newborn. Amer. J. Med. Sci., 174:357, 1927.
15. Levine, M. I., and Bell, A. I.: Treatment of
colic in infants by the use of a pacifier. J. Pediat., 37:750, 1950.
16. Zahorsky, J.: The discard of the cradle. J.
Pediat.,4:660, 1934.
17. Brazelton, T. B.: Sucking in infancy. PEDI
ATRICS,17:400, 1956.
18. Spock, B.: Baby and Child Care. New York,
Duel, Sloan & Pearce, 1945, pp. 111-115. 19. Ribble, M.: The Rights of Infants. New York,
1962;29;579
Pediatrics
T. Berry Brazelton
CRYING IN INFANCY
Services
Updated Information &
http://pediatrics.aappublications.org/content/29/4/579
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
1962;29;579
Pediatrics
T. Berry Brazelton
CRYING IN INFANCY
http://pediatrics.aappublications.org/content/29/4/579
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.