Reduction in Pediatric Identi
fi
cation Band Errors:
A Quality Collaborative
abstract
BACKGROUND AND OBJECTIVE:Accurate and consistent placement of a patient identification (ID) band is used in health care to reduce errors associated with patient misidentification. Multiple safety organizations have devoted time and energy to improving patient ID, but no multi-center improvement collaboratives have shown scalability of previ-ously successful interventions. We hoped to reduce by half the pediatric patient ID band error rate, defined as absent, illegible, or inaccurate ID band, across a quality improvement learning collabora-tive of hospitals in 1 year.
METHODS: On the basis of a previously successful single-site intervention, we conducted a self-selected 6-site collaborative to reduce ID band errors in heterogeneous pediatric hospital settings. The collaborative had 3 phases: preparatory work and employee survey of current practice and barriers, data collection (ID band failure rate), and intervention driven by data and collaborative learning to accelerate change.
RESULTS:The collaborative audited 11 377 patients for ID band errors between September 2009 and September 2010. The ID band failure rate decreased from 17% to 4.1% (77% relative reduction). Interven-tions including education of frontline staff regarding correct ID bands as a safety strategy; a change to softer ID bands, including“luggage tag” type ID bands for some patients; and partnering with families and patients through education were applied at all institutions.
CONCLUSIONS:Over 13 months, a collaborative of pediatric institutions significantly reduced the ID band failure rate. This quality improvement learning collaborative demonstrates that safety improvements tested in a single institution can be disseminated to improve quality of care across large populations of children.Pediatrics2012;129:e1587–e1593 AUTHORS:Shannon Connor Phillips, MD, MPH,aMichele
Saysana, MD,bSarah Worley, MS,cand Paul D. Hain, MDd
aCleveland Clinic Children’s Hospital, Cleveland, Ohio;bRiley Hospital for Children, Indiana University School of Medicine, Indianapolis, Indiana;cDepartment of Quantitative Health Sciences, Cleveland Clinic, Cleveland, Ohio; anddMonroe Carell Jr Children’s Hospital at Vanderbilt, Nashville, Tennessee KEY WORDS
patient safety, quality of care
ABBREVIATIONS
ID—identification
MCJCHV—Monroe Carell Jr Children’s Hospital at Vanderbilt All authors participated in (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3)final approval of the version to be published.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1911 doi:10.1542/peds.2011-1911
Accepted for publication Jan 9, 2012
Address correspondence to Shannon Phillips, MD, MPH, Cleveland Clinic, 9500 Euclid Ave Desk M73, Cleveland, OH 44195. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
to the right person. Accurate and con-sistent placement of a hospital patient identification (ID) band is used in health care to reduce errors associated with patient misidentification. In fact, if the ID band is not placed on the patient but on equipment or supplies used to care for the patient, it has the opportunity to be separated from the patient, ren-dering it useless in correct patient ID and risking misidentification of another patient should the equipment be moved. At each point along a patient’s health care experience, accurate patient ID must occur to provide quality medical care and prevent medical error. A re-view of the literature identifies articles published about medication errors, wrong surgical site errors, and trans-fusion errors.1–5A root cause of many
of these errors is lack of proper patient ID.1–5 The Joint Commission reported
that 13% of surgical errors and 67% of transfusion errors were due to patient ID errors.6,7Between January 2000 and
March 2003, the Veterans Affairs Na-tional Center for Patient Safety reported that more than 100 root cause analyses involved patient ID errors.8Because of
reports such as these, improving pa-tient ID has been thefirst goal of the Joint Commission’s National Patient Safety Goals since 2003.9Although many
interventions to decrease medical error have focused on innovations in tech-nology such as barcode scanning, these require a critical element: a correct ID band on the patient.10
Few studies have evaluated ID band errors, defined as an absent, illegible, or inaccurate ID band. The College of American Pathologists Q-Tracks pro-gram noted a decrease in the ID band error rate when the ID bands were con-tinuously audited over a 2-year period.11
Greenly et al implemented educational initiatives and process improvements at a single hospital to ensure the accuracy
decreased to zero and was sustained for 15 months.12Hain et al demonstrated
that a multifaceted approach to quality improvement and sustainment can ef-fectively reduce the ID band error rate at an academic children’s hospital.13
Barriers unique to the pediatric pop-ulation, as documented in the study by Gray et al, suggest that both the process of care and culture are not highly re-liable.14 Additionally, little is known
about dissemination strategies among interorganizational networks of physi-cians representing unrelated insti-tutions.15 Experts in implementation
sciences have implored clinicians to report on their successful dissemina-tion and implementadissemina-tion strategies.16
However, studies have not been pub-lished using quality improvement learn-ing collaboratives to decrease patient ID band errors. We report on a quality improvement collaborative of pediat-ric hospitalists and their nursing and quality improvement colleagues who sought to apply the general improve-ment model developed and imple-mented by Hain and colleagues at the Monroe Carell Jr Children’s Hospital at Vanderbilt (MCJCHV) across 6 hospi-tals to reduce pediatric patient ID band error rates.
The collaborative goal was to reduce by half the pediatric patient ID band error rate across a quality improvement learning collaborative of hospitals in 1 year. Additionally, the goal was to demonstrate that learning across insti-tutions can effectively and efficiently drive quality improvement results.
METHODS
A self-selected 6-site learning collabora-tive, organized at the 2009 annual Pedi-atric Hospital Medicine meeting, formed with the intent to reproduce the ID band improvement initiative at MCJCHV. Two institutions served as collaborative
the data collection and analysis site (Cleveland Clinic) and the other serving as a consultant for quality improve-ment overall and specifically around the ID band improvement process (MCJCHV). Previous work demonstrated that focused attention to process, edu-cation, and accountability could drive ID band failure to low levels.13 Each
participating hospital received inter-nal review board approval or exemp-tion and signed a data use agreement allowing transparent sharing of data (Table 1). The participants represented freestanding children’s hospitals, child-ren’s hospitals within academic medical centers, and community hospitals with pediatric and neonatal inpatient care areas.
The collaborative had 3 phases: pre-paratory work and institution employee survey of current practice and barriers, data collection (ID band failure rate), and intervention driven by data and col-laborative learning to accelerate change.
Survey
To assist each hospital in understanding its preexisting assumptions around ID bands, a survey originally developed at MCJCHV was provided to each insti-tution to assess attitudes and barriers to correct patient ID band placement and maintenance local to the organi-zation (see Supplemental Information). Survey participation for individual em-ployees was voluntary and anonymous. No attempt was made to quantify or aggregate the results across organi-zations. However, organizations in-formally shared their results and sought guidance through the learning collaborative.
Interventions
through consensus among the mem-bers with consideration of baseline data and survey themes. Only those drivers felt to have the most significant impact were addressed by the collab-orative. During each call, hospitals shared their current data and lessons learned, posed problems, and sought the counsel of the collaborative for resolution. Hospitals used consistent staff and patient educational materials (see Supplemental Information), shared collaborative results with their respec-tive frontline staffs, and shared ID band alternatives for particularly vulnerable populations. The following interven-tions, from the MCJCHV initiative, were used by collaborative hospitals to im-pact improvement:
Run charts transparently reported failure data for each hospital and collaborative overall
ID bands were verified at nursing bedside handoff
Patients’and families’engagement in patient ID and the purpose of ID band
Hospital/unit education about why accurate patient ID bands matter
A sense of urgency was created by using storytelling, examples of wins and failures
Voluntary event reporting systems to catch errors or patients without bands in place
For some patient populations or hospitals, selection of new ID bands (softer) was critical to acceptance
With audit failures, the bedside RN was asked“why”and afix occurred immediately
Leadership engagement
The topic was discussed on safety walk-rounds
Data Collection
The population for the improvement project included patients admitted to pediatric medical-surgical, pediatric intensive care, and NICU. Some hospi-tals included patients in emergency/ ambulatory departments. ID band errors included absent bands (not present or present on patient care equipment), illegible bands, or inaccurate data on the bands. If a patient’s ID band had more than 1 error, the failure was only counted once. ID band failure rate was defined as the number of patients audited with ID band errors divided by all patients audited. Audits were completed on any patient physically present on the unit at the time the audit was scheduled. No attempt was made tofind patients who were off the unit at the time of the audit. If a parent was not at the bedside and the patient
TABLE 1 Participating Institutions
Collaborative Site Location Total Pediatric Beds
NICU Beds
PICU Beds Our Lady of the Lake Regional Medical Center Baton Rouge, LA 95 0 15 Cleveland Clinic Children’s Hospital Cleveland, OH 105 17 15 Children’s Hospital Colorado Aurora, CO 298 60 40 Riley Hospital for Children Indianapolis, IN 266 55 33 New York Hospital Queens New York, NY 39 14 5 Scottsdale Healthcare Scottsdale, AZ 52 20 0
To maintain confidentiality, the order of the hospitals in this table does not correspond to order of hospitals in the tables and
figures in the article.
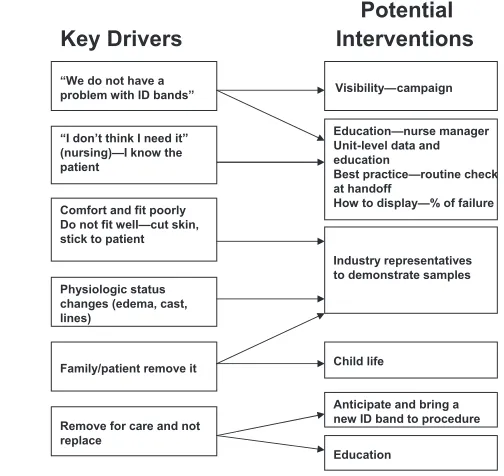
FIGURE 1
Collaborative key driver diagram.
fiers, the auditor used a hospital cen-sus list to find eligible patients and verified the patient’s bed assignment with the medical record. If both were congruent, the medical record was used as the source of truth against which the ID band was verified. For identified failures, the auditor sought clarifying information from the family or nurse about why the band was not present on the patient. Each“failure” was an opportunity to provide just-in-time education to the staff, family, and patient about the importance of ID bands to safe care.
A baseline prevalence measurement was taken at each hospital between September 2009 and April 2010 fol-lowed by prevalence audits as often as 4 times monthly through September 2010. Those audits included night, day, and weekend assessments. Each of the hospitals contributed data fora minimum of 6 and a maximum of 13 months, and all participated for thefinal 5 months (from May to September 2010). Prevalence audits for each hospital were completed by the local nursing units, the hospital quality staff, or a combination of both. Data were submitted monthly on a stan-dardized spreadsheet to a single site for aggregation and analysis. The data collection sheet was modified after the
first few months to allow discrete data collections for the reason for ID band failure. The reasons list came from the initial work at MCJCHV with small revisions from our initial collaborative audits.
Because the goal was to reduce errors for the collaborative as a whole, data were collected and all analyses per-formed at the patient level. The primary analyses combined all patient audits in a single cohort, ignoring the effect of hospital (the“combined rate”). The trend in failure rate over time was assessed by using the Cochran-Armitage Trend Test,
as month 1 and numbering each sub-sequent month of submitted data in order. The difference in failure rate from baseline to end of study was assessed by comparing failure rates among patients audited during each hospital’sfirst and last month of study participation, regardless of the num-ber of months each hospital partici-pated in the study, by using thex2test. A secondary repeated-measures anal-ysis adjusting for intrahospital corre-lation was performed by using logistic regression with generalized estimating equations. All tests were 2-tailed and performed at a significance level of .05. SAS 9.2 software (SAS Institute, Cary, NC) was used for analysis and R soft-ware 2.11.1 (The R Foundation for Sta-tistical Computing, Vienna, Austria) was used for graphics.
RESULTS
Survey
Through collaborative meetings, mis-beliefs and practices among the staff of the collaborative hospitals were dis-cussed, including placement of ID bands on isolette or intravenous tubing of neonatal patients, the belief that checking the band at each intervention with the patient was not a needed strategy to reduce error, and the im-pression that“I know my patient,”so an ID band is not required. Staff reported that ID bands cut into skin, so the bands were removed for comfort. Hospitals shared their locally identified barriers at collaborative meetings and brain-stormed potential actions collectively.
Collaborative Initiatives
The iterative work of the collaborative resulted in the following interventions applied at all institutions: education of frontline clinical employees and sup-port staff such as dietary and child life specialists regarding the importance of
with the clinical care areas; a change to softer ID bands, including“luggage tag” type ID bands for some NICU patients; and partnering with families and patients through education.
ID Band Observations
ID band audits were conducted on 11 377 patients between September 2009 and September 2010. Baseline patient ID band failure rates by hospital ranged between 4.9% and 52% with mean of 22% and a combined rate of 17% (140 failures in 795 audits) (Fig 2). Included in these failures were several hospitals where the practice for preterm or very ill patients was to place the ID band on the isolette/bed or IV tubing attached to the patient. Final month patient ID band failure rates by hospital ranged be-tween 0% and 11% with mean of 4.0% and a combined rate of 4.1% (50 failures in 1129 audits) (Table 2).
The collaborative saw a 77% relative reduction in ID band failures over the 13 months of the initiative (Cochran-Armitage Trend Test,P,.001). At the initiation of the collaborative, the NICUs were the most likely location for ID band failure owing to skin issues and accepted practice of allowing the band to be placed on intravenous tubing at-tached to the patient or taped to the isolette. By the end, NICU failures were greatly improved but still most com-mon (7% of the 167 NICU audits in the
audits were significantly more common in the last month of evaluation than at baseline and therefore cannot be ana-lyzed as independent factors. Because an ID band failure was defined as any defect in the ID band, the number of bands with multiple defects was not collected.
DISCUSSION
We report on a learning collaborative that resulted in a 77% relative reduction in ID band errors across 6 hospitals where pediatric care is delivered. Al-though quality improvement learning collaboratives have previously been reported in the literature,17experts have
questioned the enthusiasm for collab-oratives that disseminate unproven
quality improvement strategies.18
In-deed, calls have gone out to the quality community to publish successes in quality improvement learning collabo-ratives to build an evidence base that supports this method.19 A recent
re-view of the impact of quality improve-ment collaboratives found positive overall effects on quality but stressed the need for creation of new knowledge regarding the effectiveness and suc-cess factors in future collaboratives.20
The authors are fortunate to report on a collaborative that satisfies those published concerns. Our project takes its basic methods from already suc-cessful and published improvement work.13 We report that a quality
im-provement learning collaborative is
able to disseminate those methods with local modifications but equivalent success.
This quality improvement learning col-laborative demonstrated that ID band processes of care were not highly re-liable for hospitalized pediatric patients at several types of institutions. Although different types of institutions partici-pated, many of our challenges were similar, which lent itself well to a col-laborative approach to improvement. This collaborative was successful at meeting the goal of reducing patient ID band errors by half within 1 year.
Monthly collaborative conference calls gave each hospital the opportunity to present its current challenges and successes. These calls also held the members of the collaborative ac-countable for data submission and in-formation sharing. Each institution had its own methodology for staff education about patient ID bands and patient safety. One institution incorporated this initiative in a patient safety blog. An-other institution used the concepts of just culture to teach staff about patient safety and the importance of patient ID FIGURE 2
ID Band Failure Rate by Month by Hospital and Combined.
TABLE 2 ID Band Failure Rates in First and Last Month by Hospital
Hospital Failure Rate (First Month), %
95% CI (First Month)
Failure Rate (Last Month), %
95% CI (Last Month) 1 15.3 (8.6–25.5) 1.9 (0.7–4.6) 2 23.1 (10.7–42.4) 11.2 (6.7–18.0) 3 9.7 (6.5–14.3) 3.4 (1.7–6.4) 4 25.5 (17.7–35.2) 1.8 (0.5–4.7) 5 52.0 (43.3–60.7) 0.0 (0.0–9.8) 6 4.9 (2.8–8.5) 5.7 (3.6–8.9)
Number of failures is not included to conceal sites. CI, confidence interval.
bands on patients.21At individual
hos-pitals, sharing stories of patient ID band errors and patient impact helped staff understand the importance of patient ID.
For all the institutions, collaboration among nurses, physicians, and quality professionals ensured that the collab-orative was a priority. Collabcollab-orative member sites shared data with all caregivers, from leadership to frontline staff at their institutions. Sharing with
hospital employees helped engage all levels and appeared to strengthen the desire to change and the will to sustain gains made. Frequent auditing of the ID band error rate for each institution was instrumental in driving improvement and sustainability. Many hospitals in the collaborative continue to audit patient ID bands beyond the collaborative. Ad-ditionally, 1 site uses these audits as part of a manager incentive program.
Many of the collaborative participants were faced with the same challenge; 1 size and type of ID band did not work for all pediatric patients. This realization led some of the hospitals to develop prototype bands for patients when there are difficulties with skin integrity and keeping the band in place, as in the NICU. Hospitals reached out to vendors to help develop different bands for these patients, and not all incurred additional cost.
Another key intervention was the devel-opment of patient and family educational handouts. Beginning with a patient edu-cation poster developed at MCJCHV, the collaborative members edited the text incorporating our collective initial obser-vations (see Supplemental Information).
These were then modified as needed to meet local facility standards for publishing. The final product was de-signed to be given to families or hung on the wall in the patient’s room to educate patients and families about the im-portance of the patient ID band and why it should remain on the patient at all times.
There are several limitations to this study. Although definitions for all data elements were clearly stated, we did leave some room for local processes. Each hospital needed to have its own standard process to confirm ID band accuracy. Because the hospitals in-volved were geographically diverse, we did not ensure interrater reliability. Additionally, we encouraged units to self-monitor, in addition to “external” audits, because this creates local champions for improvement. We were not able to track patient misidentifi ca-tion errors, nor did we evaluate wrong patient, wrong procedure/medication events. Hospitals voluntarily partici-pating in the collaborative likely have caregivers with greater interest and resources to devote to patient safety research than an average hospital and
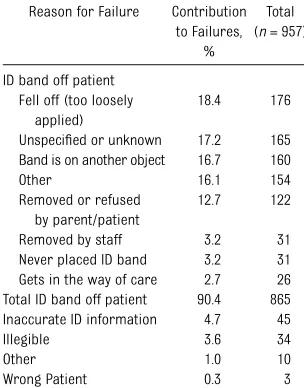
TABLE 3 Reasons for ID Band Failure Overall
Reason for Failure Contribution to Failures,
%
Total (n= 957) ID band off patient
Fell off (too loosely applied)
18.4 176 Unspecified or unknown 17.2 165 Band is on another object 16.7 160 Other 16.1 154 Removed or refused
by parent/patient
may have seen greater improvement than can be expected in a large-scale initiative.
This collaborative provides a frame-work for any hospital to assess and address the gaps in performance in ID band placement. The steps include the following: audit current ID band per-formance to define the problem, survey perceptions of staff, and apply tar-geted interventions to drive improve-ment. Future work regarding ID bands should evaluate the association be-tween accurate patient ID bands and
ID-related errors. One collaborative site noted more than 50 near misses around patient ID each month. Fur-thermore, the culture that allows caregivers to assume that the hospi-talized patient is already correctly banded needs to be explored. Lastly, future work regarding quality improve-ment collaboratives should include publication of proven collaborative strategies and the generation of new knowledge regarding which types of collaborations are best able to create improvement.
ACKNOWLEDGMENTS
We recognize the significant work of each of the hospitals in the collabora-tive. Specifically, Meredith Lahl and LaShonda Davis at Cleveland Clinic Children’s Hospital; Dr John Pope at Scottsdale Healthcare; Dr Steve Narang and Tracie Majors at Our Lady of the Lake Regional Medical Center; Dr Laurie Gordon at New York Hospital Queens; Dr Dan Hyman and Mariel Laire at Child-ren’s Hospital of Colorado; and Christin Dawson and Denise Young at Riley Hos-pital for Children.
REFERENCES
1. Leape LL, Bates DW, Cullen DJ, et al; ADE Prevention Study Group. Systems analysis of adverse drug events.JAMA. 1995;274(1):35–43
2. Zohar E, Noga Y, Davidson E, Kantor M, Fredman B. Perioperative patient safety: correct patient, correct surgery, correct side—a multifaceted, cross-organizational, interventional study. Anesth Analg. 2007; 105(2):443–447
3. Garnerin P, Arès M, Huchet A, Clergue F. Verifying patient identity and site of sur-gery: improving compliance with protocol by audit and feedback. Qual Saf Health Care. 2008;17(6):454–458
4. Renner SW, Howanitz PJ, Bachner P. Wrist-band identification error reporting in 712 hospitals. A College of American Patholo-gists’ Q-Probes study of quality issues in transfusion practice.Arch Pathol Lab Med. 1993;117(6):573–577
5. Murphy MF, Casbard AC, Ballard S, et al; BEST Research Collaborative. Prevention of bedside errors in transfusion medicine (PROBE-TM) study: a cluster-randomized, matched-paired clinical areas trial of a simple intervention to reduce errors in the pretransfusion bedside check.Transfusion. 2007;47(5):771–780
6. Beyea SC. Patient identification—a crucial aspect of patient safety.AORN J. 2003;78(3): 478–, 481–482
7. Cleopas A, Kolly V, Bovier PA, Garnerin P, Perneger TV. Acceptability of identification
bracelets for hospital inpatients.Qual Saf Health Care. 2004;13(5):344–348
8. Mannos D. NCPS patient misidentification study: a summary of root cause analyses. VA NCPS Topics in Patient Safety. Washington, DC: US Department of Veterans Affairs, June–July 2003. Available at: www.va.gov/ ncps/TIPS/Docs/TIPS_Jul03.doc. Accessed December 15, 2010
9. The Joint Commission. 2011 National patient safety goals. Available at: www.jointcommission. org/assets/1/6/2011_NPSGs_HAP.pdf. Accessed December 15, 2010
10. McDonald CJ. Computerization can create safety hazards: a bar-coding near miss.
Ann Intern Med. 2006;144(7):510–516
11. Howanitz PJ, Renner SW, Walsh MK. Con-tinuous wristband monitoring over 2 years decreases identification errors: a College of American Pathologists Q-Tracks Study.
Arch Pathol Lab Med. 2002;126(7):809–815
12. Greenly MA. Helping Hippocrates: a cross-functional approach to patient identifi ca-tion.Jt Comm J Qual Patient Saf. 2006;32 (8):463–469
13. Hain PD, Joers B, Rush M, et al. An in-tervention to decrease patient identifi ca-tion band errors in a children’s hospital.
Qual Saf Health Care. 2010;19(3):244–247
14. Gray JE, Suresh G, Ursprung R, et al. Patient misidentification in the neonatal intensive care unit: quantification of risk.Pediatrics.
2006;117(1). Available at: www.pediatrics. org/cgi/content/full/117/1/e43
15. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations.Milbank Q. 2004;82 (4):581–629
16. Rubenstein LV, Pugh J. Strategies for pro-moting organizational and practice change by advancing implementation research.
J Gen Intern Med. 2006;21(suppl 2):S58– S64
17. Young PC, Glade GB, Stoddard GJ, Norlin C. Evaluation of a learning collaborative to improve the delivery of preventive services by pediatric practices.Pediatrics. 2006;117 (5):1469–1476
18. Auerbach AD, Landefeld CS, Shojania KG. The tension between needing to improve care and knowing how to do it. N Engl J Med. 2007;357(6):608–613
19. Mittman BS. Creating the evidence base for quality improvement collaboratives. Ann Intern Med. 2004;140(11):897–901
20. Schouten LM, Hulscher ME, van Everdingen JJ, Huijsman R, Grol RP. Evidence for the impact of quality improvement collabo-ratives: systematic review. BMJ. 2008;336 (7659):1491–1494
21. Griffith KS. Column: the growth of a just culture.Jt Commiss Perspect Patient Saf. 2009;9(12):8–9
DOI: 10.1542/peds.2011-1911 originally published online May 7, 2012;
2012;129;e1587
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/129/6/e1587
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/129/6/e1587#BIBL
This article cites 19 articles, 6 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/quality_improvement_ Quality Improvement
e_management_sub
http://www.aappublications.org/cgi/collection/administration:practic Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2011-1911 originally published online May 7, 2012;
2012;129;e1587
Pediatrics
Shannon Connor Phillips, Michele Saysana, Sarah Worley and Paul D. Hain
Reduction in Pediatric Identification Band Errors: A Quality Collaborative
http://pediatrics.aappublications.org/content/129/6/e1587
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2012/05/02/peds.2011-1911.DCSupplemental
Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.