ARTICLE
A Randomized, Controlled Trial of the Effectiveness
of an Early-Intervention Program in Reducing
Parenting Stress After Preterm Birth
Per Ivar Kaaresen, MDa,b, John A. Rønning, PhDb, Stein Erik Ulvund, PhDb,c, Lauritz B. Dahl, MD, PhDa,b
aPediatric Department, University Hospital of North Norway Trust, Tromsø, Norway;bInstitute of Clinical Medicine, University of Tromsø, Tromsø, Norway;cInstitute for
Educational Research, University of Oslo, Oslo, Norway
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
BACKGROUND.Preterm birth has been associated with increased parenting stress in
early infancy, and some reports have found this to be a risk factor for later behavioral problems. There are, however, few studies and conflicting results. Information about the fathers is scarce.
OBJECTIVES.Our goal was to study the effects of an early-intervention program on
parenting stress after a preterm birth until 1 year corrected age.
METHODS.A randomized, controlled trial was conducted including infants with a
birth weight ⬍2000 g treated at the University Hospital of North Norway Trust, which serves the 2 northern-most counties in Norway, to examine the effects of a modified version of the Mother-Infant Transaction Program on parenting stress measured by the Parenting Stress Index. A term control group was also recruited. The Parenting Stress Index was administered to the mothers at 6 and 12 months’ corrected age and to the fathers at 12 months’ corrected age. The intervention consisted of 8 sessions shortly before discharge and 4 home visits by specially trained nurses focusing on the infant’s unique characteristics, temperament, and developmental potential and the interaction between the infant and the parents.
RESULTS.Seventy-one infants were included in the preterm intervention group, and
69 were included in the preterm control group. The preterm groups were well balanced. Seventy-four infants were included in the term control group. Com-pared with the preterm controls, both the mothers and fathers in the preterm intervention group reported significant lower scores in child domain, parent domain, and total stress on all occasions except the mother-reported child domain at 12 months. These differences were not related to birth weight or gestational age. The level of stress among the preterm intervention group was comparable to their term peers. Both parents in the intervention group reported consistently lower scores within the distractibility/hyperactivity, reinforces parents, competence, and attachment subscales compared with the preterm control group. There were no
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-1491
doi:10.1542/peds.2005-1491
Key Words
preterm infants, parenting stress, early intervention, randomized, controlled trial
Abbreviations
UNN—University Hospital North Norway Trust
BW— birth weight GA— gestational age
MITP—Mother-Infant Transaction Program PSI—Parenting Stress Index
ICC—intraclass correlation coefficient CI— confidence interval
ANCOVA—analysis of covariance VLBW—very low birth weight
Accepted for publication Jan 19, 2006
Address correspondence to Per Ivar Kaaresen, MD, Pediatric Department, UNN, N-9038 Tromsø, Norway. E-mail: per.ivar.kaaresen@ unn.no
differences in mean summary stress scores between the mothers and fathers in the 2 preterm groups at 12 months, but the intraclass correlation coefficient was higher in the intervention group.
CONCLUSIONS.This early-intervention program reduces
par-enting stress among both mothers and fathers of preterm infants to a level comparable to their term peers. We are now studying whether this will result in long-term ben-eficial effects.
G
IVING BIRTH TOa preterm infant is considered to bea stressful event for parents. Many studies have shown that mothers of these infants experience in-creased levels of stress in the neonatal period compared with mothers of term infants,1–4and they are more likely to suffer from depression and anxiety at the time of hospital discharge.5,6 Recently, Carter et al7 found in-creased depressive symptoms also among fathers of pre-term infants during the NICU stay. The long-pre-term adap-tation of the mothers to a normal life after a preterm birth is less studied, and the results are conflicting.8–10 There is even less information about the fathers’ adap-tation.
Today there is increasing knowledge and concern about the long-term outcome in children born prema-turely. Both cognitive delay and behavioral and emo-tional problems are reported in a large percentage of very preterm infants.11,12 Different early-intervention programs have had limited success in preventing these long-term sequelae and the behavioral problems in par-ticular. Increased parenting stress during the first year of the infant’s life has been found to be an important risk factor for later behavioral problems in some studies,13–17 but not all of them.18 It is assumed that increased par-enting stress could interfere with the parent-child rela-tionship during early childhood and consequently in-crease the risk for later behavioral problems. Reduced parenting stress might increase the parents’ sensitivity to different signals from their child and improve the par-ent-child interaction.
We therefore initiated a randomized, controlled trial of an early-intervention program that focuses on the interaction between the parents and their premature infant to examine whether the intervention could pre-vent later cognitive and behavioral problems in children born prematurely.
The main purpose of this first report is to examine if an early-intervention program could reduce parenting stress in both mothers and fathers during the first year after a premature birth.
PATIENTS AND METHODS
This study took place at the University Hospital North Norway Trust (UNN), Tromsø, Norway, in which the
only level III NICU serving the 2 northern-most counties in Norway (Troms and Finnmark) is located. The recruit-ment period was from March 1999 to August 2002. All infants born at UNN with a birth weight (BW) below 2000 g and without congenital anomalies and whose mothers’ native language was Norwegian were eligible for this study. Outborn infants were included if they were transferred to the NICU in Tromsø within 1 week after birth. Triplets were excluded because of the char-acter of the intervention. Infants who were unable to go through the planned test program because of neurologic sequelae were withdrawn from the study.
The parents were informed about the study by the coordinating study nurse approximately 2 weeks before planned discharge and signed an informed consent form if they agreed to participate. The infants were randomly assigned into either the preterm intervention group or preterm control group. Both twins were always ran-domly assigned to the same group because of the char-acter of the intervention. Randomization was arranged in random blocks of 4 and 6 using computer-generated random numbers and stratified by gestation (⬍28 and ⱖ28 weeks). The allocation was performed by using sealed opaque envelopes, identified by stratification group and consecutively numbered, which were opened after the completion of various questionnaires. The en-velopes were prepared before the study started by the Office for Clinical Research at UNN and opened by the coordinating study nurse. A group of term controls with a gestational age (GA) ⱖ37 weeks and BW ⬎2800 g, without congenital anomalies and with an uneventful pregnancy and birth, was also recruited from the hospi-tal’s well-infant nursery. Using the hospihospi-tal’s birth reg-istry, the parents of the first term infant born after a preterm infant had been allocated to the preterm inter-vention group were asked to participate, and if they declined, the parents of the next born (and so forth) were approached.
Intervention
The intervention program was a modified version of the Mother-Infant Transaction Program (MITP),19 which was developed for and used in the Vermont Intervention Study.20The modifications included an initial session in which the parents could vent experiences from the hos-pital stay and possibly their feelings of grief. Such feel-ings include feelfeel-ings of grief for not having “a normal infant,” guilt and blame about possible reasons for the preterm birth, anxiety about their infant’s survival, and concerns for the future normality of their infant.1 Sec-ond, we tried to adopt a more active participation from both the mother and the father in evaluating and han-dling the infants and their cues.
developmental potential. Furthermore, the intervention tries to sensitize the parents to their infant’s cues, espe-cially those that signal stimulus overload, distress, and readiness for interaction, and teaches the parents to respond appropriately to those cues to facilitate mutually satisfying interactions. After the initial grief-handling session, the intervention was implemented by neonatal nurses through 1-hour daily sessions with the parents and infant on 7 consecutive days starting 1 week before planned discharge at a GA of at least 34 weeks. These daily sessions were followed-up by 4 home visits by the same intervention nurse 3, 14, 30, and 90 days after discharge. A detailed outline of the MITP and the con-tent of the different interventional sessions has been given by Rauh et al19and the Norwegian Manual (un-published manuscript, 1997).
Eight experienced neonatal nurses working in the department were specially trained for the intervention. They kept a detailed logbook of every interventional session, and the logbooks were regularly reviewed and supervised by the coordinating nurse and a psychologist (J.A.R.) to maintain the consistency of the intervention. The preterm control group followed the unit’s stan-dard protocol for discharge of preterm infants, which includes an examination and offer of training in infant massage from the unit’s physical therapist, a clinical examination including visual and hearing screening, and a discharge consultation with one of the doctors.
The term control group went through a routine clin-ical examination on the third day of life. No other inter-ventions were offered.
Instruments
The Parenting Stress Index22(PSI) was used to measure stress in the parent-child relation. The PSI has been standardized with parents and children ranging in age from 1 month to 12 years in different cultures and is considered to be a reliable instrument across cultures. The self-reported questionnaire consists of 101 items that are scored on a 5-point Likert scale. The Norwegian version used was translated and back-translated by Abi-din and J.A.R. The PSI consists of a child domain and a parent domain. The child domain score reflects parental stress associated with the child’s individual characteris-tics as measured on 6 subscales: distractibility/hyperac-tivity, adaptability, reinforces parent, demandingness, mood, and acceptability. The parent domain reflects pa-rental stress associated with the papa-rental role and is measured on 7 subscales: competence, isolation, attach-ment, health, role restriction, depression, and spouse. Overall scores for the child and parent domains are obtained by summing the scores of their respective sub-scales, and a combination of the domain scores gives the total stress score. Higher scores indicate more stress. The life stress dimension of the PSI was also calculated. This dimension is a measure of negative life experience
dur-ing the last 12 months. Missdur-ing values on different items were handled according to the PSI manual,22 so the numbers with valid summary scores, therefore, will vary slightly. The PSI was filled out by the mothers when the infant was at 6 months’ corrected age and by both par-ents at 12 months’ corrected age.
Perinatal variables were abstracted from the medical charts. GA was based on ultrasound examinations at 16 to 18 weeks of gestation. The Score for Neonatal Acute Physiology23 and Clinical Risk Index for Babies24 were calculated for the preterm infants as an indicator of severity of initial disease. Small for GA was defined as a BW⬎2 SD below the mean for GA. Norwegian BW data were used.25 Intraventricular hemorrhage was graded according to Papile et al,26and periventricular leukoma-lacia was defined as the presence of echolucencies by cranial ultrasound. Social variables used in the analysis were obtained at discharge with a separate question-naire.
All infants were examined clinically by an experi-enced neonatologist (L.B.D.) at 6 and 12 months’ cor-rected age for possible neurologic sequelae. The exam-iner was blinded to the infants’ group allocation.
Outcomes
Primary outcomes were the differences between the pre-term intervention group and prepre-term control group in the PSI summary scores of child domain, parent domain, and total stress reported by the mothers at 6 and 12 months’ corrected age and by the fathers at 12 months’ corrected age.
Secondary outcomes were differences in the PSI sub-scales between the 2 preterm groups, differences in in-tervention effects related to BW, GA, and social factors, changes over time in group effects in stress scores re-ported by the mothers at 6 and 12 months’ corrected age, and differences between mothers and fathers.
Power Calculations
This study is part of a more comprehensive interven-tional study with long-term follow-up of the infants, and the study size was originally calculated on the basis of differences between the preterm groups in cognitive de-velopment at 2 years’ adjusted age. This power analysis indicated that 60 preterm infants needed to be included in the intervention and control groups, respectively. Al-lowing for loss in follow-up, the target group size was 70 infants, and a similar number of term controls were recruited. With group sizes of 70, there was 80% chance to detect a difference between the 2 preterm groups of .48 SD in the PSI scores with a level of significance of .05.
Statistics
in-teraction terms were used in subgroup analysis. Repeat-ed-measures analysis of variance was used to test changes in group differences at 6 and 12 months’ cor-rected age. Pairedttests and intraclass correlation coef-ficients (ICCs)27 were used to test differences between stress scores in mothers and fathers at 12 months’ cor-rected age. Differences in continuous variables are given as mean difference with 95% confidence intervals (CIs) unless otherwise stated. Cohen’sd was used as a mea-sure of effect size.28Cohen’s dis the ratio between the mean difference and the pooled SDs for the sample. Analysis of covariance (ANCOVA) was used in a pre-planned secondary analysis to adjust for possible con-founding effects of socioeconomic status. All results are reported as intention to treat. All analyses were per-formed by using Stata 8.0.29The study was approved by the Regional Committee for Medical Research Ethics and the Norwegian Data Inspectorate.
RESULTS
During the recruitment period, a total of 203 preterm infants with a BW⬍2000 g were born at or transferred to UNN. This represents 96% (203 of 212) of all infants with a BW⬍2000 g born in Troms and Finnmark coun-ties during the recruitment period. One hundred forty-six infants were randomly assigned to a preterm inter-vention or preterm control group. Seventy-five infants were recruited to the term control group during the same period. Figure 1 shows the patient flow until 12 months’ corrected age. The infants whose parents de-clined to participate were slightly more mature than the preterm infants who were included (GA: 32.5 vs 30.1 weeks, respectively;P⫽.001), but there was no signif-icant difference in BW (1419 vs 1398 g, respectively;P⫽ .1). Almost all mothers completed the PSI at both 6 and 12 months’ corrected age, whereas the overall response rate for the fathers was 79%: 86% in the preterm inter-vention group and 74% and 78% in the preterm and term control groups, respectively. The nonresponding fathers were not different from the responders regarding number of years of education or their infant’s BW or GA. The 4 families that did not attend the 12-month exam-ination still want to participate in the study.
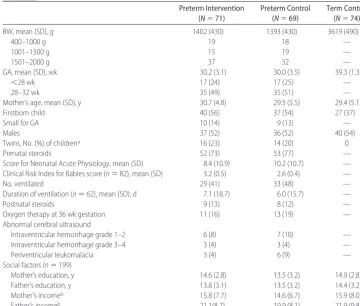
Patient characteristics and social variables are listed in Table 1. The preterm groups were well balanced except for a small but significant difference in the preterm mothers’ number of years of education (mean differ-ence: 1.1 year; 95% CI: 0.03 to 2.2;P⫽.04).
Three infants were diagnosed with cerebral palsy at the clinical examination at 12 months’ corrected age (1 in the preterm control group and 2 in the intervention group). Four infants (2 in each preterm group) had visual defects and required glasses, and 1 infant in the intervention group had reduced hearing on one side. Seven infants (3 in the preterm control and 4 in the
intervention group) were considered developmentally delayed by⬎2 months. All children were included in the analysis.
Intervention
One infant allocated to the preterm intervention group did not receive the planned intervention. This infant is included in the intervention group in the analysis (in-tention to treat). All mothers participated in every inter-vention session, whereas 60 (94%) of 64 fathers partic-ipated in ⱖ1 session. The fathers participated in a median of 6 of 12 intervention sessions (home visits included) (interquartile range: 4 –9 sessions).
Primary Outcome
Table 2 shows the child-domain, parent-domain, and total stress scores for the different groups of infants at 6 and 12 months’ corrected age for prematurity. The pre-term intervention group had significantly lower scores in all scores at both 6 and 12 months compared with the preterm control group except child domain reported by the mothers at 12 months, where the difference was only borderline significant (P⫽.08). The effect sizes of the interventions were small to moderate, with Cohen’s d ranging from .30 to .50 (Table 2). There were no significant differences between the 2 preterm groups in the life stress dimension reported by the mothers at 6 and 12 months and fathers at 12 months.
Secondary Outcomes
Subgroup Analysis
To examine whether the observed differences between the 2 preterm groups in child domain, parent domain, and total stress scores varied by BW, GA, mothers’ and fathers’ education (number of years) or income, or num-ber of older siblings, we fitted multiple-regression mod-els including an interaction term between the group allocation and these variables. There were no significant interactions, indicating that the observed differences did not vary by these factors.
Subscales
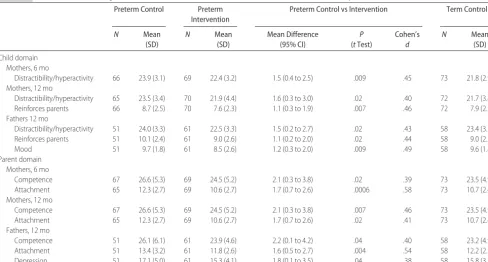
The parents in the preterm intervention group had con-sistently lower scores than those in the preterm control group in all subscales in both the child and parent do-mains. However, the only subscales in which these dif-ferences reached statistical significance are shown in Table 3. The most consistent differences between the 2 preterm groups were found in the subscales of distract-ibility/hyperactivity, reinforces parents, competence, and attachment.
Changes Over Time
and preterm control groups (the possible intervention effect) changed between 6 and 12 months, we per-formed repeated-measures analysis of variance. There
were no significant time-by-group interactions on any of the summary scores: child domain (P ⫽ .89), parent domain (P⫽.46), or total stress (P⫽.68).
FIGURE 1
Differences Between Mothers and Fathers
To test whether there were any differences in the re-ported stress between mothers and fathers at 12 months, we compared their reported mean stress scores by paired ttests and calculated the ICCs within each group (Table 4). There were no significant differences in mean scores between the genders in child or parent domain or total stress, although the differences in means tended to be
somewhat lower in the preterm intervention group. In child domain, the ICC was substantially higher in the preterm intervention group than in the preterm control group and lowest in the term control group.
There was a significant negative correlation between the number of intervention sessions in which the fathers participated and the father-reported total stress score at 12 months (Spearman’s⫽ ⫺0.33;P⫽.01).
TABLE 1 Infant Characteristics and Social Factors
Preterm Intervention (N⫽71)
Preterm Control (N⫽69)
Term Control (N⫽74)
BW, mean (SD), g 1402 (430) 1393 (430) 3619 (490)
400–1000 g 19 18 —
1001–1500 g 15 19 —
1501–2000 g 37 32 —
GA, mean (SD), wk 30.2 (3.1) 30.0 (3.5) 39.3 (1.3)
⬍28 wk 17 (24) 17 (25) —
28–32 wk 35 (49) 35 (51) —
Mother’s age, mean (SD), y 30.7 (4.8) 29.5 (5.5) 29.4 (5.1)
Firstborn child 40 (56) 37 (54) 27 (37)
Small for GA 10 (14) 9 (13) —
Males 37 (52) 36 (52) 40 (54)
Twins, No. (%) of childrena 16 (23) 14 (20) 0
Prenatal steroids 52 (73) 53 (77) —
Score for Neonatal Acute Physiology, mean (SD) 8.4 (10.9) 10.2 (10.7) — Clinical Risk Index for Babies score (n⫽82), mean (SD) 3.2 (0.5) 2.6 (0.4) —
No. ventilated 29 (41) 33 (48) —
Duration of ventilation (n⫽62), mean (SD), d 7.1 (18.7) 6.0 (15.7) —
Postnatal steroids 9 (13) 8 (12) —
Oxygen therapy at 36 wk gestation 11 (16) 13 (19) —
Abnormal cerebral ultrasound
Intraventricular hemorrhage grade 1–2 6 (8) 7 (10) —
Intraventricular hemorrhage grade 3–4 3 (4) 3 (4) —
Periventricular leukomalacia 3 (4) 6 (9) —
Social factors (n⫽199)
Mother’s education, y 14.6 (2.8) 13.5 (3.2) 14.9 (2.8)
Father’s education, y 13.8 (3.1) 13.5 (3.2) 14.4 (3.2)
Mother’s incomeb 15.8 (7.7) 14.6 (6.7) 15.9 (8.0)
Father’s incomeb 21.1(8.7) 19.9 (8.1) 21.9 (9.8)
Numbers are given as number (%) of infants unless otherwise stated. — indicates not relevant.
aBoth twins survived.
bAverage monthly income (SD) in 1000 Norwegian kroner.
TABLE 2 PSI Summary Scores at 6 and 12 Months’ Corrected Age
Preterm Control Preterm
Intervention
Preterm Control vs Intervention Term Control
N Mean (SD) N Mean (SD) Mean Difference
(95% CI)
P
(tTest)
Cohen’s
d
N Mean (SD)
Mothers, 6 mo
Child domain 63 94.8 (15.2) 67 88.0 (14.6) 6.8 (1.6 to 12.0) .01 .45 71 84.3 (13.3)
Parent domain 61 117.0 (20.9) 63 108.6 (19.4) 8.4 (1.2 to 15.6) .02 .41 72 110.4 (20.3)
Total stress 59 212.2 (34.2) 62 195.4 (30.3) 16.9 (5.2 to 28.5) .005 .50 69 194.8 (30.5)
Mothers, 12 mo
Child domain 61 92.5 (14.6) 69 87.2 (17.6) 5.0 (⫺0.6 to 10.7) .08 .30 71 86.1 (15.4)
Parent domain 61 116.5 (20.7) 69 107.8 (20.7) 8.7 (1.5 to 15.9) .02 .41 71 110.1 (20.5)
Total stress 59 208.6 (33.2) 68 194.9 (35.5) 13.7 (1.6 to 25.9) .03 .39 70 195.3 (33.0)
Fathers, 12 mo
Child domain 51 96.0 (13.9) 59 89.3 (15.8) 6.7 (1.0 to 12.3) .02 .44 58 89.3 (12.3)
Parent domain 51 113.5 (21.2) 59 105.3 (19.6) 8.2 (0.5 to 15.9) .02 .40 57 106.3 (15.3)
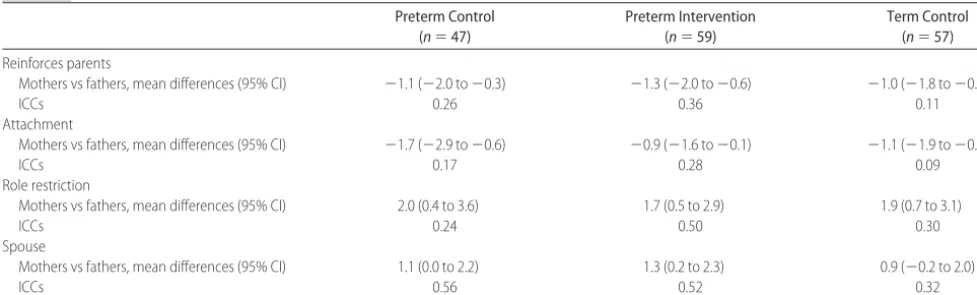
When this analysis was repeated on the various PSI subscales, we found a consistent pattern in which the fathers reported significantly higher mean scores in the subscales of reinforces parents and attachments within all 3 infant groups compared with the mothers at 12 months (Table 5). The ICCs were generally low, again with the highest values in the preterm intervention group and lowest in the term control group, although the differences were small. The mothers reported higher scores in the role-restriction subscale within all groups, whereas the mothers in both preterm groups reported higher scores in the spouse subscale (Table 5).
Secondary Multivariate Analysis
In a preplanned secondary ANCOVA, we adjusted for the potential confounding effect of various social factors on total stress scores. The covariates were chosen on the
basis of previous knowledge about their prognostic im-portance and plausibility.
The mothers’ and fathers’ education and income, number of siblings, and the mothers’ age were entered as independent variables in addition to group allocation (preterm control versus intervention). Total stress scores at the different time points were used as dependent variables. We first examined whether there were any significant interactions between the group variable and the other covariates, which would render the ANCOVA invalid. There were no such significant interactions.
These ANCOVAs resulted in adjusted group differ-ences of 17.3 (95% CI: 5.4 to 29.2; P⫽ .005) for the mother-reported total stress score at 6 months and 13.4 (95% CI: 1.1 to 25.8; P⫽ .03) at 12 months. For the fathers, the adjusted group difference at 12 months was 12.2 (95% CI:⫺0.5 to 25.0;P⫽.06).
TABLE 3 PSI Subscales With Significant Differences Between Preterm Control and Intervention Groups
Preterm Control Preterm
Intervention
Preterm Control vs Intervention Term Control
N Mean (SD)
N Mean (SD)
Mean Difference (95% CI)
P
(tTest)
Cohen’s
d
N Mean (SD)
Child domain Mothers, 6 mo
Distractibility/hyperactivity 66 23.9 (3.1) 69 22.4 (3.2) 1.5 (0.4 to 2.5) .009 .45 73 21.8 (2.9) Mothers, 12 mo
Distractibility/hyperactivity 65 23.5 (3.4) 70 21.9 (4.4) 1.6 (0.3 to 3.0) .02 .40 72 21.7 (3.4)
Reinforces parents 66 8.7 (2.5) 70 7.6 (2.3) 1.1 (0.3 to 1.9) .007 .46 72 7.9 (2.2)
Fathers 12 mo
Distractibility/hyperactivity 51 24.0 (3.3) 61 22.5 (3.3) 1.5 (0.2 to 2.7) .02 .43 58 23.4 (3.3)
Reinforces parents 51 10.1 (2.4) 61 9.0 (2.6) 1.1 (0.2 to 2.0) .02 .44 58 9.0 (2.2)
Mood 51 9.7 (1.8) 61 8.5 (2.6) 1.2 (0.3 to 2.0) .009 .49 58 9.6 (1.8)
Parent domain Mothers, 6 mo
Competence 67 26.6 (5.3) 69 24.5 (5.2) 2.1 (0.3 to 3.8) .02 .39 73 23.5 (4.9)
Attachment 65 12.3 (2.7) 69 10.6 (2.7) 1.7 (0.7 to 2.6) .0006 .58 73 10.7 (2.4)
Mothers, 12 mo
Competence 67 26.6 (5.3) 69 24.5 (5.2) 2.1 (0.3 to 3.8) .007 .46 73 23.5 (4.9)
Attachment 65 12.3 (2.7) 69 10.6 (2.7) 1.7 (0.7 to 2.6) .02 .41 73 10.7 (2.4)
Fathers, 12 mo
Competence 51 26.1 (6.1) 61 23.9 (4.6) 2.2 (0.1 to 4.2) .04 .40 58 23.2 (4.9)
Attachment 51 13.4 (3.2) 61 11.8 (2.6) 1.6 (0.5 to 2.7) .004 .54 58 12.2 (2.3)
Depression 51 17.1 (5.0) 61 15.3 (4.1) 1.8 (0.1 to 3.5) .04 .38 58 15.8 (3.2)
TABLE 4 Comparison of PSI Summary Scores as Reported by Mothers and Fathers at 12 Months’ Corrected Age Preterm Control Group
(n⫽47)
Preterm Intervention Group (n⫽59)
Term Control Group (n⫽57)
Child domain
Mothers vs fathers, mean differences (95% CI) 2.3 (⫺7.9 to 1.3) 1.9 (⫺5.7 to 1.8) 2.2 (⫺7.1 to 1.9)
ICCs 0.45 0.64 0.22
Parent domain
Mothers vs fathers, mean differences (95% CI) 3.2 (⫺3.5 to 9.4) 2.6 (⫺0.8 to 9.7) 2.5 (⫺1.3 to 8.7)
ICCs 0.46 0.51 0.42
Total stress
Mothers vs fathers, mean differences (95% CI) ⫺1.0 (⫺11.5 to 9.4) 2.2 (⫺6.1 to 10.6) 0.3 (⫺8.4 to 7.7)
DISCUSSION
The main finding from this study is that an early-inter-vention program, as implemented here, reduces parent-ing stress in both mothers and fathers durparent-ing the first year after a preterm birth to a level comparable to their term peers. To our knowledge, this is the first random-ized, controlled trial of an early-intervention program to report reduced parenting stress in both mothers and fathers after a preterm birth. Deater-Deckard and Bulk-ley30recently reviewed the findings from different ran-domized, controlled trials that evaluated the effects of different interventions on subsequent parent adaptation and parent behaviors after a premature birth. They found a consistent pattern of positive effects on maternal adaptation, parent-child interaction, and more general aspects of the home environment. However, parenting stress, as measured by the PSI, had not been studied in randomized, controlled studies until Als et al31 recently were the first to report a significant reduction in parental stress measured at 2 weeks after an expected day of confinement in a group of very low BW (VLBW) (BW⬍ 1250 g, GA⬍28 weeks) infants who were treated with individualized developmental care, compared with a control group in a multicenter randomized, controlled trial. Although they included smaller infants and their interventions were different in both timing and content compared with this study, there are similarities in the underlying theoretical framework for the interventions, and our results extend their findings of reduced parent-ing stress both in length of follow-up and by includparent-ing the fathers.
One might argue that a preintervention measurement of parenting stress to demonstrate that there was no imbalance between the preterm groups at baseline would have strengthened our study. The PSI, however, is only validated in infants from 1 month of age. Despite this, we did in fact administer the PSI to the mothers before the intervention. Because of a vast number of unanswered items (up to two thirds in some items), it was impossible to use these results in the analysis. The
strict randomization procedures undertaken in this study should result in comparable groups, and we found the preterm groups to be well balanced regarding GA, BW, initial disease severity, various neonatal complica-tions, and different social factors. Furthermore, there were no differences between the groups in reported life stress on any occasions. Thus, there is substantial reason to attribute the observed reduction in parenting stress to the intervention program. The small, but significant dif-ference in the length of the preterm mothers’ education is a result of chance. The importance of such an imbal-ance primarily depends on the correlation between the factor and outcome. We performed a preplanned ANCOVA as a secondary analysis to adjust for potential confounding effects of various social variables. The dif-ferences in total stress between the 2 preterm groups as reported by the mothers were only slightly changed by this adjustment. Among the fathers, the potential inter-ventional effect was reduced from 14.8 to 12.2, which might indicate some confounding, although the change is small.
There was a significant negative correlation between total stress and the number of interventional sessions in which the fathers participated, which suggests a direct interventional effect. The effect among fathers could also, at least partly, be an indirect effect from the mother (ie, more confident and less stressed mothers could lead to reduced stress among their husbands).
The intervention effect was not related to differences in BW or GA, and there were no changes in the effect among mothers from 6 to 12 months.
The size of the interventional effect is somewhat dif-ficult to interpret. A reduction in the total-stress score of 16.9 points as observed between preterm mothers at 6 months has no obvious meaning when compared with a similar reduction in, for example, intelligence quotients. We therefore used Cohen’sdas a measure of effect size. This is an extensively used measurement of effect size in behavioral research, and some researchers argue that it should be preferred to P values. A Cohen’s d of .5 is
TABLE 5 Differences Between Mothers and Fathers in PSI Subscales Preterm Control
(n⫽47)
Preterm Intervention (n⫽59)
Term Control (n⫽57)
Reinforces parents
Mothers vs fathers, mean differences (95% CI) ⫺1.1 (⫺2.0 to⫺0.3) ⫺1.3 (⫺2.0 to⫺0.6) ⫺1.0 (⫺1.8 to⫺0.2)
ICCs 0.26 0.36 0.11
Attachment
Mothers vs fathers, mean differences (95% CI) ⫺1.7 (⫺2.9 to⫺0.6) ⫺0.9 (⫺1.6 to⫺0.1) ⫺1.1 (⫺1.9 to⫺0.3)
ICCs 0.17 0.28 0.09
Role restriction
Mothers vs fathers, mean differences (95% CI) 2.0 (0.4 to 3.6) 1.7 (0.5 to 2.9) 1.9 (0.7 to 3.1)
ICCs 0.24 0.50 0.30
Spouse
Mothers vs fathers, mean differences (95% CI) 1.1 (0.0 to 2.2) 1.3 (0.2 to 2.3) 0.9 (⫺0.2 to 2.0)
generally regarded as a moderate effect size, meaning that the intervention led to a .5 SD change in outcome. We found an effect size of .30 to .50, which compares favorably to other early preventive intervention studies in early childhood as found in a recent meta-analyses by Bakermans-Kranenburg et al.32
The effect of the intervention was also examined on the different PSI subscales. This must be considered as an exploratory analysis and the results interpreted with care because of the multiple comparisons that were per-formed. However, a quite distinct pattern emerged, in-dicating that the intervention had the greatest effects on the distractibility/hyperactivity, reinforces parents, com-petence, and attachment subscales, with some variation in both the fathers and mothers. We find this effect plausible in light of the character of the intervention. The interventional program (as described in “Patients and Methods”) was focused on enabling the parents to interpret and act according to their infant’s cues, thereby strengthening the parent-infant relationship and making them feel more competent in handling their preterm infant.
Many studies have shown that mothers experience more stress than fathers both during the NICU stay and also later after discharge.10,33–35We found no mean dif-ferences between the fathers and mothers in any of the PSI summary scores 12 months after the premature birth. However, we found a markedly higher ICC in the child domain in the preterm intervention group com-pared with both control groups. It is possible that this may be a result of the intervention, which focused on teaching the parents to respond adequately to the in-fant’s cues. We speculate that this could result in more consistent judgements between the parents of stress re-lated to the child also in later infanthood. Similarly, less involvement by the fathers in the infant’s newborn pe-riod and possibly later because of different social roles could explain the low ICCs in child domain found in the term control group.
Tommiska et al10 found a nonsignificant increase in total stress score measured by the Swedish Parenthood Stress Questionnaire (SPSQ) among mothers compared with fathers of extremely low BW infants 2 years after birth, the difference being largest in the incompetence and spouse-relationship subscales. However, the SPSQ measures stress mainly in dimensions included in the PSI parent domain and has no dimensions parallel to the PSI child domain, and the response rate from the fathers was very low. When analyzing the differences between mothers and fathers in the PSI subscales, we found a consistent pattern within both preterm groups but also in the term control group. The fathers scored higher in the child-related reinforces parents and attachment sub-scales, whereas the mothers scored higher in the parent-related role restriction and spouse subscales. This finding is consistent with the Tommiska et al findings, with
increased maternal stress in the parent domain sub-scales. Our finding that these differences between moth-ers and fathmoth-ers were similar across the different infant groups indicates that these differences are related to traditionally different roles of mothers and fathers in our societies and families, not to prematurity per se. This finding underlines the importance of including a term control group in studies such as this.
There has been some controversy in the literature about parenting stress after a preterm birth. Increased stress among the mothers during a stay in the NICU or during the first few months after discharge has been a common finding in various studies using different in-struments, although the mothers in some studies seem to adapt rather quickly to their situation.34,36,37 Some cross-sectional studies have found a more sustained in-crease in parenting stress,33,38 whereas others have not.9,10,39In one of the few longitudinal studies using the PSI to date, Singer et al8 found an increase in child domain scores in mothers of VLBW infants with bron-chopulmonary dysplasia compared with mothers of term infants, but there was no difference in the parent do-main. They found no differences between mothers of low-risk VLBW infants compared with their term peers. Our study was not designed to examine different risk strata of preterm infants, so a direct comparison is not possible, but a substantial part of our infants were low-risk preterm infants (Table 1). Our results when com-paring the preterm and term control groups are in line with those studies finding a persistent increase in par-enting stress at least during the first year after a preterm birth (Table 2). Our finding that the increased parenting stress is primarily due to an increase in the child domain is in accordance with other studies using the PSI.8,38
Reducing parenting stress may be important by itself, leading to better lives for families with a preterm child. However, because some studies have shown that par-enting stress is a risk factor for later behavioral problems in both preterm13–17 and other40 children, the reduction in parenting stress during the infant’s first year of life may potentially be an important factor in reducing long-term behavioral problems in these infants. To date, no studies have examined this possible effect of reduced parenting stress, but this will be an important aspect of the long-term follow-up of the infants included in our study.
STRENGTHS AND WEAKNESSES
more difficult to generalize. However, the growth-re-stricted infants were evenly distributed between the 2 preterm groups and should not influence the group dif-ferences found. The number of extremely preterm in-fants is rather limited in this study. This is a consequence of the sparsely populated area we serve, with a limited number of extremely preterm infants. An alternative could have been to prolong the inclusion period. How-ever, the inclusion period was, even with this design, rather long. No important changes in the treatment of preterm infants except for the intervention program were introduced in our NICU during the inclusion pe-riod. The potential spillover effect from the intervention group to the control group was minimized by late ran-domization, and only selected, trained nurses performed the intervention. If a spillover effect still occurred, it would have tended to reduce the observed effects of the intervention program.
CONCLUSIONS
We have shown a persistent increased parenting stress in both mothers and fathers of preterm infants compared with their term peers. A limited, structured, clearly de-fined early-intervention program can prevent the par-enting stress in both mothers and fathers to the same level as found in term parents. We are now studying the long-term effect of this on later cognitive and behavioral outcome in these infants.
ACKNOWLEDGMENTS
This study was funded by grants from the Norwegian Research Council, Norwegian Council for Mental Health, Norwegian Foundation for Health and Rehabil-itation, and Northern Norway Regional Health Author-ity.
We thank Bjørn Helge Handegård for statistical advice and the Office for Clinical Research at the University Hospital of North Norway Trust for help with the ran-domization procedures. We thank the neonatal nurses who implemented the intervention program and the coordinating nurse, Jorunn Tunby, in particular. With-out their efforts, this study would not have been possi-ble. We also thank the families and infants for partici-pating.
REFERENCES
1. Pederson DR, Bento S, Chance GW, Evans B, Fox AM. Mater-nal emotioMater-nal responses to preterm birth.Am J Orthopsychiatry.
1987;57:15–21
2. Spear ML, Leef K, Epps S, Locke R. Family reactions during infants’ hospitalization in the neonatal intensive care unit.
Am J Perinatol.2002;19:205–213
3. Hughes MA, McCollum J. Neonatal intensive care: mothers and fathers perceptions of what is stressful. J Early Interv.
1994;18:258 –268
4. Young SR, Watson MA, Corff KE, Odle P, Haase J, Bowerman
JL. Parent stress and coping in NICU and PICU.J Pediatr Nurs.
1997;12:169 –177
5. Blumberg NL. Effects of neonatal risk, maternal attitude, and cognitive style on early postpartum adjustment.J Abnorm Psy-chol.1980;89:139 –150
6. Singer LT, Davillier M, Bruening P, Hawkins S, Yamashita TS. Social support, psychological distress, and parenting strains in mothers of very low birthweight infants.Fam Relat.1996;45: 343–350
7. Carter JD, Mulder RT, Bartram AF, Darlow BA. Infants in a neonatal intensive care unit: parental response.Arch Dis Child Fetal Neonatal Ed.2005;90:F109 –F113
8. Singer LT, Salvator A, Guo S, Collin M, Lilien L, Baley J. Maternal psychological distress and parenting stress after the birth of a very low-birth-weight infant. JAMA. 1999;281: 799 – 805
9. Halpern LF, Brand KL, Malone AF. Parenting stress in mothers of very-low-birth-weight (VLBW) and full-term infants: a function of infant behavioral characteristics and child-rearing attitudes.J Pediatr Psychol.2001;26:93–104
10. Tommiska V, Ostberg M, Fellman V. Parental stress in families of 2 year old extremely low birthweight infants.Arch Dis Child Fetal Neonatal Ed.2002;86:F161–F164
11. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. JAMA. 2002;288: 728 –737
12. Saigal S. Follow-up of very low birthweight babies to adoles-cence.Semin Neonatol.2000;5:107–118
13. Ong LC, Boo NY, Chandran V. Predictors of neurodevelopmen-tal outcome of Malaysian very low birthweight children at 4 years of age.J Paediatr Child Health.2001;37:363–368 14. Saylor CF, Boyce GC, Price C. Early predictors of school-age
behavior problems and social skills in children with intraven-tricular hemorrhage (IVH) and/or extremely low birthweight (ELBW).Child Psychiatry Hum Dev.2003;33:175–192
15. Miceli PJ, Goeke-Morey MC, Whitman TL, Kolberg KS, Miller-Loncar C, White RD. Brief report: birth status, medical com-plications, and social environment—individual differences in development of preterm, very low birth weight infants.J Pe-diatr Psychol.2000;25:353–358
16. Benzies KM, Harrison MJ, Magill-Evans J. Parenting stress, marital quality, and child behavior problems at age 7 years.
Public Health Nurs.2004;21:111–121
17. Assel MA, Landry SH, Swank PR, Steelman L, Miller-Loncar C, Smith KE. How do mothers’ childrearing histories, stress and parenting affect children’s behavioural outcomes?Child Care Health Dev.2002;28:359 –368
18. Magill-Evans J, Harrison MJ. Parent-child interactions and development of toddlers born preterm.West J Nurs Res.1999; 21:292–307; discussion 308 –312
19. Rauh VA, Nurcombe B, Achenbach T, Howell C. The Mother-Infant Transaction Program: the content and implications of an intervention for the mothers of low-birthweight infants.Clin Perinatol.1990;17:31– 45
20. Achenbach TM, Howell CT, Aoki MF, Rauh VA. Nine-year outcome of the Vermont intervention program for low birth weight infants.Pediatrics.1993;91:45–55
21. Sameroff AJ, Fiese BH. Transactional regulation: the develop-mental ecology of early intervention. In: Shonkoff JP, Meisels SJ, eds.Handbook of Early Childhood Intervention. Cambridge, United Kingdom: Cambridge University Press; 2000:135–159 22. Abidin RR.Parenting Stress Index. 3rd ed. Odessa, FL:
Psycho-logical Assessment Resources, Inc; 1995
24. The CRIB (Clinical Risk Index for Babies) score: a tool for assessing initial neonatal risk and comparing performance of neonatal intensive care units. The International Neonatal Net-work.Lancet.1993;342:193–198
25. Skjaerven R, Gjessing HK, Bakketeig LS. Birthweight by ges-tational age in Norway. Acta Obstet Gynecol Scand. 2000;79: 440 – 449
26. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm.
J Pediatr.1978;92:529 –534
27. Shrout PE, Fleiss J. Intraclass correlations: uses in assessing rater reliability.Psychol Bull.1976;86:420 – 428
28. Cohen J. Statistical power analysis for the behavioral sciences. Revised ed. New York, NY: Academic Press; 1997
29. Stata Statistical Software[computer program]. Release 8.0. Col-lege Station, TX: Stata Corp; 2003
30. Deater-Deckard K, Bulkley J. Parent concerns in long-term follow-up.Semin Neonatol.2000;5:171–178
31. Als H, Gilkerson L, Duffy FH, et al. A three-center, randomized, controlled trial of individualized developmental care for very low birth weight preterm infants: medical, neurodevelopmen-tal, parenting, and caregiving effects [published correction ap-pears inJ Dev Behav Pediatr. 2004;25:224 –225].J Dev Behav Pediatr.2003;24:399 – 408
32. Bakermans-Kranenburg MJ, van IJzendoorn MH, Juffer F. Less is more: meta-analyses of sensitivity and attachment in-terventions in early childhood.Psychol Bull.2003;129:195–215
33. Cronin CM, Shapiro CR, Casiro OG, Cheang MS. The impact of very low-birth-weight infants on the family is long lasting: a matched control study. Arch Pediatr Adolesc Med. 1995;149: 151–158
34. Trause MA, Kramer LI. The effects of premature birth on parents and their relationship.Dev Med Child Neurol.1983;25: 459 – 465
35. Miles MS, Funk SG, Kasper MA. The stress response of mothers and fathers of preterm infants. Res Nurs Health. 1992;15: 261–269
36. Stjernqvist KM. Extremely low birth weight infants less than 901 g: impact on the family during the first year.Scand J Soc Med.1992;20:226 –233
37. Stjernqvist K, Svenningsen NW. Extremely low-birth-weight infants less than 901 g: development and behaviour after 4 years of life.Acta Paediatr.1995;84:500 –506
38. Ong LC, Chandran V, Boo NY. Comparison of parenting stress between Malaysian mothers of four-year-old very low birth-weight and normal birthbirth-weight children.Acta Paediatr.2001; 90:1464 –1469
39. Lee SK, Penner PL, Cox M. Impact of very low birth weight infants on the family and its relationship to parental attitudes.
Pediatrics.1991;88:105–109
DOI: 10.1542/peds.2005-1491
2006;118;e9
Pediatrics
Per Ivar Kaaresen, John A. Rønning, Stein Erik Ulvund and Lauritz B. Dahl
Program in Reducing Parenting Stress After Preterm Birth
A Randomized, Controlled Trial of the Effectiveness of an Early-Intervention
Services
Updated Information &
http://pediatrics.aappublications.org/content/118/1/e9
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/118/1/e9#BIBL
This article cites 36 articles, 4 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-1491
2006;118;e9
Pediatrics
Per Ivar Kaaresen, John A. Rønning, Stein Erik Ulvund and Lauritz B. Dahl
Program in Reducing Parenting Stress After Preterm Birth
A Randomized, Controlled Trial of the Effectiveness of an Early-Intervention
http://pediatrics.aappublications.org/content/118/1/e9
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.