EXPERIENCE & REASON
Endocarditis After Closure of Ventricular Septal
Defect by Transcatheter Device
Oded Scheuerman, MDa,b, Elchanan Bruckheimer, MDb,c, Nufar Marcus, MDa,b, Vered Hoffer, MDa,b, Ben-Zion Garty, MDa,b
Departments ofaPediatrics B andcPediatric Cardiology, Schneider Children’s Medical Center of Israel, Petah Tiqva;bSackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
Advances in interventional cardiology have enabled the treatment of severe congenital heart defects without the need for surgery. The percutaneous closure of atrial septal defects and, more recently, ventricular septal defects is considered a safe procedure with fewer complications and less morbidity compared with surgery. We report on a 2-year-old child who developed endocarditis after ventricular septal defect closure with an Amplatzer device. The patient recovered after intravenous antibiotics and anticoagulation. To the best of our knowledge, this is the first report of endocarditis associated with ventricular septal defect closure device insertion.
A
DVANCES IN INTERVENTIONALcardiology have made it possible to treat congenital heart malformations percutaneously, without the need for surgery. The Am-platzer septal occluder was designed for the percutane-ous transcatheter occlusion of septal defects. It is a self-expandable, double-disk device with a connecting waist made from Nitinol wire mesh. Dacron patches are sewn into each disk and the connecting waist to occlude the blood flow through the device. The ventricular septal defect (VSD) occluder is available with waist diameters of 4 to 18 mm. Amplatzer septal occlusion is considered effective and safe, with lower morbidity and mortality rates than reported for surgery.1,2However, theimplan-tation of a foreign body in the heart raises the possibility of intracardiac thrombus and infection. We describe a child with infective endocarditis caused byKingella deni-trificansinfection of an Amplatzer closure device.
CASE REPORT
A 22-month-old female infant was admitted after a fe-brile disease of 1 month’s duration. She had been born after a normal pregnancy and delivery with a birth weight of 3100 g. On the 10th day of life, signs of congestive heart failure appeared, and echocardio-graphic study established the diagnosis of a large mus-cular VSD and coarctation of the aorta. After hemody-namic stabilization, the patient underwent coarctation repair and pulmonary artery banding. Because the mus-cular VSD failed to close spontaneously, at the age of 20 months, the patient underwent percutaneous VSD
oc-clusion with a 14-mm Amplatzer device (AGA Medical Corporation, Golden Valley, MN) and balloon debanding of the pulmonary artery. Intravenous cefonicid (50 mg/ kg) was administered before the procedure. Both proce-dures were successful; there were no residual VSDs or intraoperative or postoperative complications.
One month later, a daily fever up to 40°C (104°F) developed and lasted for 4 weeks. The fever failed to respond to a 10-day course of amoxicillin, given for suspected otitis media, and the child was admitted to our department for additional investigation. At admission, her temperature was 39°C (102.2°F), heart rate was 170 beats per minute, respiratory rate was 40/minute, and blood pressure was 95/60 mm Hg. There were no splin-ter hemorrhage or Roth’s spots. A systolic murmur (3/6) was heard in the mid-left sternal border. The rest of the physical examination was unremarkable.
Laboratory tests showed an erythrocyte sedimenta-tion rate of 130 mm/hour, C-reactive protein of 11 mg/dL (reference: 0 – 0.5 mg/dL), white blood cell count of 8600/mm3with 42% polymorphonuclears and 40%
Key Words:VSD, device closure, endocarditis
Abbreviations:VSD, ventricular septal defect; PFO, patent foramen ovale www.pediatrics.org/cgi/doi/10.1542/peds.2005-2498
doi:10.1542/peds.2005-2498
Accepted for publication Dec 21, 2005
Address correspondence to Oded Scheuerman, MD, Department of Pediatrics, Schneider Children’s Medical Center of Israel, Petah Tiqva 49202, Israel. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2006 by the American Academy of Pediatrics
e1256 SCHEUERMAN et al
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
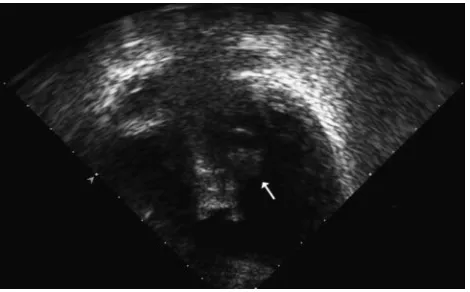
lymphocytes, hemoglobin of 10 g/dL, and platelet count of 330 000/mm3; 7 blood cultures were taken. Urinalysis showed microscopic hematuria. A chest radiograph re-vealed mild cardiomegaly with increased flow to the pulmonary vessels. Color Doppler echocardiography demonstrated a vegetation that measured 10⫻12 mm in diameter on the left side of the Amplatzer device in the left ventricle (Fig 1). No residual VSD was noted. There was mild aortic insufficiency and good biventricu-lar function.K denitrificans grew in 1 blood culture; the other cultures were negative. The diagnosis of infective endocarditis was made.
It was decided to attempt a course of antibiotics and not device removal at this stage. Treatment with vanco-mycin (40 mg/day) and gentamicin (7.5 mg/kg per day) was initiated. When the culture result was obtained, treatment was changed to cefuroxime (100 mg/kg per day). Defervescence occurred in 2 days. The patient was treated intravenously for 6 weeks. Anticoagulation treatment with heparin was given during the first 2 weeks of treatment; thereafter, aspirin was administered for 3 months. After 6 weeks of treatment, the vegetation disappeared, there was no sign of valvular dysfunction, and the child was discharged.
During the subsequent 6 months, she was doing well, with no signs, symptoms, or echocardiographic evidence of relapse. The VSD is closed.
DISCUSSION
Percutaneous VSD device closure is being used increas-ingly in recent years1,2 with encouraging results. In
se-lected cases, it is an alternative to surgical intervention. Arora et al3reported successful closure of muscular and
perimembranous VSDs in 130 of 137 patients with a variety of devices, with no mortality. Complications, which were uncommon, included device dislodgement, transient conduction defects, and, rarely, hemolysis. The incidence of thrombus formation was variable, in the
range of 3% to 27%; however, when the Amplatzer device was used, the rate was lower.4 This difference
probably is attributable to the different structure and composition of the devices and the duration of endothe-lialization. Despite the presence of a foreign body, only a few cases of Amplatzer device–associated endocarditis have been reported.5–7
There is a single report of a child in whom Staphylo-coccus aureusendocarditis developed after Nissen fundo-plication, performed 1 month after percutaneous patent foramen ovale (PFO) closure. The bacteria were isolated from a skin wound that might have been the portal of entry, and the child was treated surgically.7In addition,
endocarditis was reported in 2 adults after closure of an atrial septal defect and PFO.5,6
TheKingellaspecies are part of the normal respiratory flora. Although considered a relatively rare cause of infection, they are emerging as an important pathogen in young children.8Kingellaspecies are included in the
HACEK group (Haemophilus, Actinobacillus, Cardiobacte-rium, Eikenella, and Kingella), which previously were considered to be a cause of culture-negative endocarditis because of the special requirements of the bacteriologic culture.9,10 Among the Kingella species, K kingae is the
most prevalent pathogen in children.K denitrificanshas been reported rarely as a bacterial cause of prosthetic valve endocarditis11–13 and never as a cause of
device-associated endocarditis.
CONCLUSIONS
Device-associated endocarditis is a rare but important complication of percutaneous closure of atrial septal de-fect, PFO, and, currently, VSD. To the best of our knowl-edge, this is the first report of a child who had endocar-ditis after VSD closure with an Amplatzer device and was treated successfully with conservative treatment. This case has significant clinical implications, because despite the rarity of this complication, failure of conservative treatment could necessitate major open-heart surgery. The complication occurred despite intravenous cefonicid treatment before VSD closure. The increasing use of intracardiac devices may require a reevaluation of the possible need for administration of prophylactic antibi-otics before, during, or after the procedure and the type of antibiotics to be given. This case further emphasizes the importance of close follow-up, including color Dopp-ler echocardiography, after intracardiac device insertion to exclude thrombosis and the development of infective endocarditis.
REFERENCES
1. Holzer R, Hijazi ZM. Interventional approach to congenital heart disease.Curr Opin Cardiol.2004;19:84 –90
FIGURE 1
Shortened apical 2-dimensional 4-chamber–view echocardiography showing the VSD Amplatzer device and, on the left ventricular side, a large pedunculated vegetation (white arrow) on the superior aspect of the disk.
PEDIATRICS Volume 117, Number 6, June 2006 e1257
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
2. Thanopoulos BD, Tsaousis GS, Karansios E, Eleftherakis NG, Paphitis C. Transcatheter closure of perimembranous ventric-ular septal defects with the Amplatzer asymmetric ventricventric-ular septal defect occluder: preliminary experience in children.J In-terv Cardiol.2003;16:399 – 407
3. Arora R, Trehan V, Kumar A, Karla GS, Nigam A. Transcath-eter closure of congenital ventricular septal defects: experience with various devices.J Interv Cardiol.2003;16:83–91
4. Anzai H, Child J, Natterson B, et al. Incidence of thrombus formation on the CardioSEAL and the Amplatzer interatrial closure devices.Am J Cardiol.2004;93:426 – 431
5. Calachanis M, Carrieri L, Grimaldi R, Veglio F, Orzan F. Infec-tive endocarditis after transcatheter closure of a patent foramen ovale.Catheter Cardiovasc Interv.2004;63:351–354
6. Bullock AM, Menachem S, Wilkinson JL. Infective endocarditis on an occluder closing an atrial septal defect. Cardiol Young.
1999;9:65– 67
7. Goldstein JA, Beardslee MA, Haodong X, Sundt TM, Lasala JM.
Infective endocarditis resulting from CardioSEAL closure of a patent foramen ovale. Catheter Cardiovasc Interv. 2002;55: 217–220
8. Yagupsky P, Dagan R. Kingella kingae: an emerging cause of invasive infection in young children. Clin Infect Dis.1997;24: 860 – 869
9. Feder HM Jr, Roberts JC, Salazar JC, Leopold HB, Toro-Salazar O. HACEK endocarditis in infants and children: two cases and a literature review.Pediatr Infect Dis J.2003;22:557–562 10. Ferber B, Bruckheimer E, Schlesinger Y, et al. Kingella kingae
endocarditis in a child with hair-cartilage hypoplasia.Pediatr Cardiol.1997;18:445– 446
11. Hassan IJ, Hayek L. Endocarditis caused byKingella denitrificans.
J Infect.1993;27:291–195
12. Swann RA, Holmes B. Infective endocarditis caused byKingella denitrificans.J Clin Pathol.1984;37:1384 –1387
13. Khan JA, Sharp S, Mann KR, Brewer J.Kingella denitrificans
prosthetic endocarditis.Am J Med Sci.1986;291:187–189
e1258 SCHEUERMAN et al
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2005-2498 originally published online May 1, 2006;
2006;117;e1256
Pediatrics
Ben-Zion Garty
Oded Scheuerman, Elchanan Bruckheimer, Nufar Marcus, Vered Hoffer and
Endocarditis After Closure of Ventricular Septal Defect by Transcatheter Device
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/6/e1256
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/6/e1256#BIBL
This article cites 13 articles, 1 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_sub Cardiology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2005-2498 originally published online May 1, 2006;
2006;117;e1256
Pediatrics
Ben-Zion Garty
Oded Scheuerman, Elchanan Bruckheimer, Nufar Marcus, Vered Hoffer and
Endocarditis After Closure of Ventricular Septal Defect by Transcatheter Device
http://pediatrics.aappublications.org/content/117/6/e1256
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2006 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news