IJPSR (2019), Volume 10, Issue 3 (Review Article)
Received on 14 July 2018; received in revised form, 29 September 2018; accepted, 05 October 2018; published 01 March 2019 A CRITICAL REVIEW ON COLON TARGETED DRUG DELIVERY SYSTEMS FOR MANAGEMENT OF INFLAMMATORY BOWEL DISEASE
Meenakshi Jaiswal * and S. K. Lanjhiyana
Department of Pharmaceutics, SLT Institute of Pharmaceutical Sciences, Guru Ghasidas Vishwavidyalaya, Koni, Bilaspur - 495009, Chhattisgarh, India.
ABSTRACT: Inflammatory bowel disease (IBD) refers to the inflammation of the colon and small intestine of the body, in which Crohn's disease and ulcerative colitis are the principal types of IBD. This article covers most of the information related to a drug delivery system for treatment regarding intestinal diseases more emphasized to inflammatory bowel diseases. Currently, using delivery systems for targeting drugs to colon are osmotic drug delivery system, chronotropic system, pulsinicap system, multiparticulate system, port system, COLAL-Pred system, gas empowered drug delivery system have included in this article. An approach for targeting drugs to the colon is a probiotic approach has also included in this article. These delivery systems are being used to improve the bioavailability of the poorly absorbed drug. The purpose of this review article is to study about techniques employed in colon targeting for the prevention and treatment of IBD.
INTRODUCTION: Novel drug delivery system (NDDS) is an approach of delivering drugs to the desired site in optimal dosage with more patient compliance and safety in comparison to other conventional delivery systems 1. NDDS can minimize the harmful effects of drugs, increases bioavailability and accumulation at the targeted site due to its control over pharmacokinetics and pharmacodynamic profile of the drug. In addition to this, NDDS are non-immunogenic and non-toxic 2. This system involves several carriers’ (soluble
polymers, natural and synthetic polymers, lipoproteins, liposomes, micelles, etc.) for proper delivery of drugs to the required zone 3.
QUICK RESPONSE CODE
DOI:
10.13040/IJPSR.0975-8232.10(3).985-92
The article can be accessed online on
www.ijpsr.com
DOI link: http://dx.doi.org/10.13040/IJPSR.0975-8232.10(3).985-92
This approach has been used successfully in targeting drugs to the colon site. Colon-specific drug delivery system (CDDS) has become the most selective approach for the local treatment of inflammatory bowel diseases (IBDs). IBD is the condition of chronic inflammation of the gastrointestinal tract that leads to the generation of specific diseases like ulcerative colitis and Crohn's disease. Other types of IBDs include colonic cancer, amoebiasis, and local colonic infections.
This system specifically delivers the drug to the colon site and prevent its degradation at the stomach and small intestine 4, 5. Protein and peptide drugs generally degrade at gastric pH; the treatment will be more effective by using CDDS to deliver drugs directly to colonic mucosa. These novel approaches may target one or more aspects of gastrointestinal physiology such as colonic microflora, pH, enzymes, etc. 6 However, certain drawbacks are associated with this delivery system such as variation of pH in colon region, variation of Keywords:
Colon-specific drug delivery, Colonic disease, Inflammatory disease, Gastrointestinal tract, Evaluation of drugs targeting colon
Correspondence to Author: Mrs. Meenakshi Jaiswal
Assistant Professor,
Institute of Pharmaceutical Sciences Guru Ghasidas Vishwavidyalaya, Bilaspur - 495009, Chhattisgarh, India.
gastric emptying time, drug transit due to colonic disease and hindrance due to peristaltic movement 7
. IBD is a pathological immune response due to the attack of microbes. The body starts producing antibodies against microbial antigens; accumulation of T-cells and cell adhesion molecules cause inflammation of the affected organ 8. The anti-tumor necrosis factor (anti-TNF) antibody therapy had significant success against IBD. There are several drugs approved for treatment of IBDs including infliximab, a first approved drug for induction and maintenance of Crohn's disease; adalimumab, a tumor necrosis factor (TNF-α) antagonist had approved for both Crohn's disease and ulcerative colitis 9. However, this therapy was not effective in every patient for controlling IBD because the response of drugs decreases with time.
Therefore, it was a need to identify some more suitable disease targets and the discovery of drugs for the treatment of IBD. Recently, it has found that the IBD patients exhibited higher amounts of cytokine oncostatin M (OSM) in the inflamed tissue. OSM is a protein linked to inflammation, OSM receptor (OSMR) responds to OSM that leads to the production of several pro-inflammatory mediators (e.g., interleukins, leukocyte adhesion factor, and chemokines) 10. Targeting interleukins may be an effective therapy for the treatment of IBD. Specifically, interleukin-6 (IL-6) involves in the pathogenesis of colorectal cancer. The increased amount of IL-6 has found in colonic mucosa and serum of patients with IBD 4. The objective of the present work was to compile several approaches employing for targeting colon in the treatment IBDs with more emphasis on biodegradable polysaccharides.
Disease Affecting Intestine and Abdominal Problems: There are several diseases affecting colon or large intestine represents a diagnostic problem in patients with abdomen problems. Colon diseases usually occur due to obstruction of our digestive processes such as gas, acidity, irregular bowel movements, constipation, diarrhea, and mild hemorrhoids. Crohn’s disease is an ulcerative bowel disease usually associated with granulomatous inflammation 11. Ulcerative colitis is defined as a chronic disease affecting the mucosa and sub-mucosa of the rectum. It causes bloody diarrhea, severe abdominal pain, and dehydration in
its fulminant condition 12. Amoebiasis is a protozoal disease that affects colon site caused by infection of Entamoeba histolytica 13. Diverticulosis is herniation of mucosa and submucosa, abdominal pain and intermittent bleeding. Its inflammatory form is termed as diverticulitis 14.
Colonic Diseases: Colon is also known as large intestine one of the organs present in the gastrointestinal tract (GIT). It is a hollow tube surrounded by the muscles about 5 feet long and 2.5 inches in diameter 15. The human large intestine plays an important role in maintaining gastrointestinal homeostasis throughout life. However, the component of microbiota may sometimes become the risk factor for disease in susceptible hosts. The mutualism of host-microbe breaks down during gastrointestinal diversity and inflammatory and metabolic disorders 16. Colon cancer is the third most common cause of cancer worldwide and the leading cause of deaths for the patients 17.
It is generally considered that several environmental factors such as diet, smoking, and physical activities are responsible for generating colon cancer. Histologically, intestinal type adenocarcinoma, mucinous adenocarcinoma, and signet-ring cell carcinoma are major subtypes of colorectal cancer 18. Some colorectal cancer occurs due to germline mutation when cancer cells invading submucosa are termed as malignant polyps. Adenomatous polyposis syndrome (FAP) is associated with mutations in tumor suppressor gene 19
.
individual’s immune system attacks its element in digestive system 21. These diseases are generally associated with increased morbidity and decreased the quality of life. Few researchers reported that fatigue is associated with IBD due to its effect on the central nervous system interacting with chronic disease pathways like stress-induced changes in corticotropin-releasing hormone (CRH) regulation of the hypothalamic-pituitary axis 22. Alteration in luminal pH is also responsible for generating IBD. It has reported that reduced intracolonic pH in ulcerative colitis impairs bioavailability of several pH-dependent release formulation such as 5-aminosalicylic acid, sulphasalazine, olsalazine, balsalazide, etc. 23 The therapy for IBD has changed with several agents and novel techniques. New targets have been identified by researchers for therapeutic alteration in IBD to restore immune dysregulation and inhibition of proinflammatory mediators. It includes tumor necrosis factor and interleukins such as IL-6, IL-13, IL-17, IL-18, and IL-21. 24
Drugs Targeting Colon: Intestinal site is suitable for both local and systemic delivery of drugs. The treatment therapy will be more effective if we can deliver drugs directly to the intestine. It will reduce systemic side effects. It also allows oral administration of protein and peptide drugs that are normally inactive in the upper parts of the body 6. Novel approaches targeting intestinal site includes pressure controlled colonic delivery capsules, osmotic controlled drug delivery and several other techniques that are unique in achieving site specificity and feasibility of production 25. These novel techniques have overcome preliminary techniques including pH, time-dependent systems, prodrugs and microbially triggered delivery system due to several limitations and low rate of success 26. The pH of gastrointestinal tract varies from region to region, i.e. stomach-1.5, duodenum- 6.1, jejunum- 5.4, ileum- 7.8, rectum- 7 to 8. 27 Drug targeting colon is used for the treatment of diseases like inflammatory bowel disease, amoebiasis, colonic cancer, ulcerative colitis, Crohn's disease,
etc. 28 Intestinal mucoadhesive drug delivery system increases the residence time of the dosage form at the targeted site and facilitates absorption that contributes to improved therapeutic performance 29. Drugs showing narrow therapeutic
index are highly effective if targeted to the desired site of the GIT 30.
Drugs targeting colon allows to release drug at the desired site and prevents its degradation at stomach as shown in Fig. 1. The effective way of targeting drugs to large intestine is to increase release periods or slow release rates by applying thicker layers of enteric coatings. The absorption of the drug at this site is affected by the nature and pH of GIT.
The preliminary methods of targeting drugs to colon are the formation of a prodrug, polymer coatings, coating with a biodegradable polymer, poly-saccharides designed drugs, including novel techniques like pressure-controlled drug delivery systems and osmotic pressure controlled systems 5. Drugs delivered using this system are more suitable for peptides and protein drugs to achieve reduced dosing frequency, delay drug delivery to attain high concentration and deliver drugs to the region those less hostile metabolically. The colon targeted drug delivery system comprised with certain advantages of reduced side effects in the treatment of colonic diseases, avoid first-pass metabolism, prevents gastric irritation and protects peptide drugs from hydrolysis and enzymatic degradation 31.
FIG. 1: PATHWAY OF ORAL DRUGS TARGETING COLON
[image:3.612.315.567.443.537.2]absorption 32. The drugs targeting colon should have following properties, i.e. the drug should be absorbed at large intestine rather than the stomach and small intestine, it should be compatible with a carrier molecule, it should be stable at alkaline pH, and the drug should have both local and systemic effects 5.
Colon Targeted Drug Delivery Systems: Targeted delivery systems are desirable for the treatment of a range of inflammatory bowel disease and other colon diseases. There are several systems that have been reported for delivery of drugs to the colon. It involves use of formulation components that interact with one or more aspects of gastrointestinal (GI) physiology, such as the difference in the pH along the GI tract, the presence of colonic microflora, and enzymes, to achieve colon targeting. Various novel delivery systems overcome the limitations of conventional systems. However, conventional systems are still using because of their ease and economic value. Here, we will discuss several delivery systems that have been using for targeting drugs to the colon.
Multi-particulate Systems: Multi-particulate systems have a small particle size for easy delivery typically consisting of thousands of spherical particles with a diameter of 0.05-2.00 mm. They reach the colon quickly since pass the gastrointestinal tract more easily. It includes microspheres, pellets, nanoparticles, etc. Micro-spheres are prepared using biodegradable components like chitosan, polysaccharides, pectin and guar gum with pH-sensitive polymers. Pellets are small particles or granules produced by agglomeration of fine powders with a binder solution.
Nanoparticles show improved bioavailability due to their increased surface area and thus increased contact with biological surfaces. These particles are taken up by macrophages at the colon and allow remaining at the targeted site for a longer period 6. The advantages of this system include avoidance of dose dumping, increased bio-availability, faster gastric emptying, improved reproducibility of transit time, a high degree of GIT dispersion, less likely to cause local irritation, improved stability, patient comfort, and compliance. This system is not devoid of certain drawbacks such as low drug
loading, high amount of excipients, tedious formulation steps, higher cost of production, etc. 33
Osmotic Drug Delivery: This device delivers drug through an orifice by the generation of osmotic pressure followed by a constant influx of water. It delivers drug through zero order kinetic. It is composed of osmotically active drug core surrounded by the semipermeable membrane. This is further coated with Eudragit S100 an enteric polymer. This coating protects the drug from degradation at the stomach; however, it dissolves in the small intestine and the intestinal fluid enters into tablet core generates osmotic pressure and then finally reaches to the colon, where osmotic pressure core breaks and release drug, e.g. OROS-CT 34. Fig. 2 exhibits the delivery of drug at colon site using osmotic pressure.
FIG. 2: RELEASE OF DRUG AT COLON THROUGH OSMOTIC PRESSURE
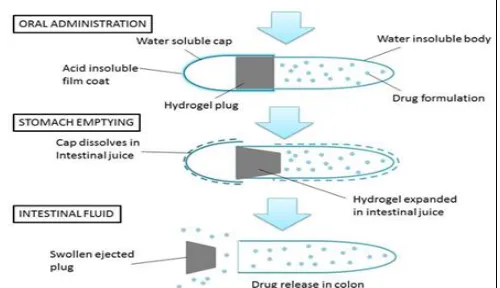
Pulsincap System: It contains a capsule shaped non-disintegrating body and water-soluble cap. The body part fills with drug molecule and sealing with hydrophilic hydrogel, which is covered with a water-soluble cap.
FIG. 3: MECHANISM OF THE PULSINCAP
[image:4.612.314.566.309.455.2] [image:4.612.316.566.572.716.2]The cap drilled to make a hole and sealed with an enteric polymer that gets dissolved into the small intestine and intestinal fluid enter into the capsule due to hydrophilic nature of hydrogel. It absorbs water, starts swelling and then ejects from the body. Drug release duration depends upon the length of hydrogel used 35. Fig. 3 shows pulsincap drug releasing mechanism at colon site.
Port System: It is hard gelatin capsule coated with a cellulosic semi-permeable membrane containing drug formulation along with an osmotically active agent and plugged. In an aqueous medium, the semipermeable membrane diffuses water, results in the generation of hydrostatic pressure that ejects plug in the large intestine. The drug release duration or lag time depends upon plug, which gets pushed away by swelling or erosion. The drug release pattern from the port system has shown in Fig. 4, where A is Dissolution of capsule’s cap leads to immediate release, B is Energy source is activated by controlled permeation of GI fluid, C is Time-release plug is expelled, D is Pulse or sustained release of second dose 36.
FIG. 4 DRUG RELEASE MECHANISM OF PORT SYSTEM
Gas Empowered Drug Delivery System
(GEDD): In this drug delivery system, the proteins and peptides targeted to colon using mucoadhesive polymer polyethylene oxide and trimethylated chitosan (TMC) as penetration enhancer using CO2 37
. The drug adhered to the mucous layer due to the mucoadhesive polymer and opens at the tight junctions of the colon because of TMC to promote drug absorption through the paracellular pathway. In GEDD, CO2 produces a driving force to push the drug to the absorbing membrane and protects the drug from enzymatic and proteolytic degradation 38
.
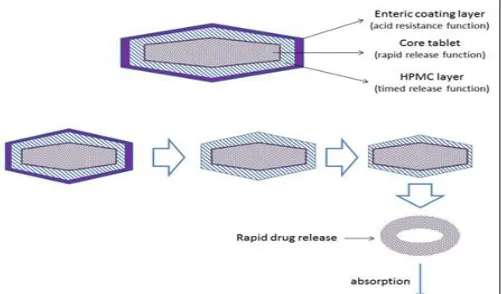
Chronotropic System: This system of drug delivery is beneficial in the treatment of disease affected by circadian rhythms, rheumatoid arthritis, asthma, and hypertension. This system contains hydroxypropylmethylcellulose (HPMC) coated drug-containing core that is responsible for the lag phase in the onset of release. The differences in gastric emptying time can be overcome by using an enteric film. It also helps in releasing drug at the colon site. The thickness and viscosity of HPMC can control the lag time of drug release 35. A system defining time-dependent release of a capsule is shown in Fig. 5.
FIG. 5: RELEASE PATTERN OF DRUG FROM CHRONOTROPIC SYSTEM
COLAL-Pred System: This delivery system is specifically designed for the treatment of ulcerative colitis. It is the combination of COLAL (colonic drug delivery system) and prednisolone (an approved generic steroid). This system provides an effective anti-inflammatory treatment for ulcerative colitis whose no competitor products available in the market. COLAL-Pred has a coating, breaks only in the large intestine due to colonic bacteria. It is used in topical delivery of prednisolone in ulcerative colitis 39.
An Approach for Targeting Drug to Colon: Along with delivery system an approach is also used to deliver drug at colon site, i.e. probiotic approach. In this approach, the beneficial micro-organism is introduced into the body for the treatment of a particular disease. It promotes a healthy digestive tract and a healthy immune system.
[image:5.612.315.566.245.392.2] [image:5.612.49.299.392.563.2]Lactobacillus), microbially digestible carrier and triggering temperature. These strains get active at body temperature and start digesting the carrier and releasing drug at large intestine.
Table 1 shows different diseases for which a probiotic approach can be useful.
TABLE 1: PROBIOTIC MICROBIAL STRAINS USED
FOR THE TREATMENT OF GIT DISEASES 40
Diseases Strain
Intestinal dysbiosis Lactobacillus strain Irritable bowel syndrome Bifidobacterium infantis
Escherichia coli
Traveler’s diarrhea Lactobacillus GG
Lactobacillus plantarum
Crohn’s disease Escherichia coli
Colon cancer Enterococcus faecium
Ulcerative colitis Lactobacillus acidophilus Escherichia coli
Peptic ulcer disease Lactobacillus acidophilus
Evaluation of Colon Targeted Drugs: Few in-vitro and in-vivo models are available for evaluation of colon targeted drug release. However, these techniques are not standardized due to its dependence on variable conditions of GIT such as pH, volume, stirring, bacteria, enzyme and other components of food. In vitro models used for drug delivery are:
In-vitro Dissolution Test: Dissolution of colon targeted drugs can be determined as the dissolution method described in United States Pharmacopoeia (USP). It is used to characterize the dissolution pattern of drugs at different pH likely to encounter at various locations in the gastrointestinal tract (GIT). The dissolution of the colon targeted drug is generally evaluated at pH 6.8 to pH 7.4. 5
In-vitro Enzymatic Test: This test is used to evaluate the effect of drugs in the presence of the enzyme at GIT. The in-vitro test is performed to determine the release of drug at a different time interval, which is done outside the body in a buffer medium containing enzymes ezypectinase or dextranase. The degradation of polymer carrier defines the release of drug in particular time 5.
In-vivo Evaluation: In-vivo evaluation of drugs targeting colon is determined on animals. Guinea pigs are the animals of choice for experimental IBD model. The following in-vivo method is adopted to evaluate colon targeting formulations:
Drug Delivery Index (DDI): It is pharmacokinetic parameter defines the release of oral colon targeted drug. DDI is the relative ration of relative colonic tissue exposure to the drug to the relative amount of drug in the blood, i.e. relative systemic exposal to the drug. High drug DDI value indicates better colon drug delivery. It can be determined by the formula given below:
Relative colonic tissue exposure to the drug The relative amount of drug in the blood Gamma Scintigraphy: In this technique, the gamma radiations are used to determine the transit time of dosage form through the GIT and to identify the sites of drug absorption. It is a non-invasive technique of evaluation, where energy is transformed into light scintillation and amplified to give digitalized results. Gamma scintigraphy is also provided the facility of visualization of drug delivery process 41.
DISCUSSION AND CONCLUSION: The colon targeted drug delivery system has been gaining interest in the comparison of other formulations for the treatment of inflammatory bowel diseases in recent years. The drugs like proteins and peptides targeting colon are being explored for its systemic actions in addition to local effects 42. The oral route is one of the most preferred routes for drug delivery due to its feasibility, patient compliance, and economic value. However, this route has several critical barriers makes the drug delivery less efficient like GI epithelia, high mucus turnover, variable pH range, absorption barrier, first pass metabolism, longer time to achieve a therapeutic level, and rapid luminal enzymatic degradation.
Thus, colon targeted drug delivery system may avoid all these drawbacks of orally giving drugs and delivery it to the specific site. The micro-particulate systems are more efficient for the treatment of IBD than sustained release devices such as tablet and capsules due to their micron size avoids rapid GI transit in the condition of diarrhea 28
. However, osmotic drug delivery has the advantage of zero-order release over an extended period irrespective of the environmental factors 34. The delivery systems that consist of natural materials and degraded by colonic bacterial enzymes are more likely to be used for colon targeting 26. However, due to sophistication
concern of colon-specific drug delivery systems, challenges prevail for scientists and researchers to develop validated method can be used routinely in an industry setting for the evaluation of large intestine drug delivery system. The novel materials and technologies are constantly developing and the goal of manufacturing for ideal drug delivery is realizing rapidly. Further, the new molecular targets are needed to identify to increase the drug’s effectiveness and reduce side effects.
ACKNOWLEDGMENT: The authors are
thankful to the Guru Ghasidas Vishwavidyalaya, Koni for providing all facilities required for writing this article.
CONFLICT OF INTEREST: The authors
declared no conflict of interest.
REFERENCES:
1. Bhagwat RR and Vaidhya IS: Novel drug delivery systems: an overview. IJPSR 2013; 4(3): 970-982
2. Toppo FA and Pawar RS: Novel drug delivery strategies and approaches for wound healing. Innovare Academic Sciences 2015; 2(2).
3. Devi VK, Jain N and Valli KS: Importance of novel drug delivery systems in herbal medicines. Pharmacogn Rev 2010; 4(7): 27-31.
4. McLean MH, Neurath MF and Durum SK: Targeting
interleukins for the treatment of inflammatory bowel disease - What lies beyond anti-TNF therapy? Inflamm Bowel Dis 2014; 20(2): 389-97.
5. Philip A and Philip B: Colon targeted drug delivery systems: A Review on primary and novel approaches. Oman Med J 2010; 25(2): 70-8.
6. Amidon S, Brown JE and Dave VS: Colon-targeted oral drug delivery systems: Design trends and approaches. AAPS Pharm Sci Tech 2015; 16(4): 731-41.
7. Patel MP, Patel JK, Patel J, Patel A, Patel J and Solanki S: Novel approaches and recent innovations in colon targeted drug delivery system-A review 2011; 4(2).
8. Mosli MH, Rivera-Nieves J and Feagan BG: T-cell trafficking and anti-adhesion strategies in inflammatory bowel disease: Current and prospects. Drugs 2014; 74(3): 297-311.
9. Leiman DA and Lichtenstein GR: Therapy of
inflammatory bowel disease: What to expect in the next decade. Curr Opin Gastroenterol 2014; 30(4): 385-90.
10. West NR, Hegazy AN, Owens BMJ, Bullers SJ, Linggi B
and Buonocore S: Oncostatin M drives intestinal inflammation and predicts response to tumor necrosis factor–neutralizing therapy in patients with inflammatory bowel disease. Nat Med 2017.
11. Freeman HJ and FACP F: Granuloma-positive Crohn’s disease 2007; 21(9): 583-7.
12. Parray FQ, Wani ML, Malik AA, Wani SN, Bijli AH and
Irshad I: Ulcerative colitis: A challenge to surgeons. Int J Prev Med 2012; 3(11): 749-63.
13. Ximénez C, Morán P, Rojas L, Valadez A, Gómez A and Ramiro M: Novelties on amoebiasis: A neglected tropical disease. J Glob Infect Dis 2011; 3(2): 166.
14. Tursi A: Diverticulosis today: Unfashionable and still under-researched. Therap Adv Gastroenterol 2016; 9(2): 213-28.
15. Thenmozhi MK, Anees RS, Vaishnavi M, Ramya DD and
Vedha BN. Development of a novel drug delivery system to treat inflammatory bowel disease. IJAPR 2014; 5(2): 104-114.
16. Shanahan F: The colonic microbiota and colonic disease. Curr Gastroenterol Rep 2012; 14(5): 446-52.
17. Bostanci O, Kemik O, Kemik A, Battal M, Demir U and Purisa S: A novel screening test for colon cancer: Talin-1. Eur Rev Med Pharmacol Sci 2014; 18(17): 2533-7. 18. Tamas K, Walenkamp AME, de Vries EGE, van Vugt
MATM, Beets-Tan RG and van Etten B: Rectal and colon cancer: Not just a different anatomic site. Cancer Treatment Reviews 2015; 41: 671-679
19. Aarons CB, Shanmugan S and Bleier JIS: Management of malignant colon polyps: Current status and controversies. World J Gastroenterol 2014; 20(43): 16178-83.
20. Ali SA, Malekzadeh R and Keshavarzian A: Current Therapeutic approaches in inflammatory bowel disease. Curr Pharm Des 2010; 16(33): 3668-83.
21. Leppkes M, Neurath MF, Herrmann M and Becker C: Immune deficiency vs. immune excess in inflammatory bowel diseases-STAT3 as a rheo-STAT of intestinal homeostasis. J Leukoc Biol 2016; 99(1): 57-66.
22. Langenberg DR and Gibson PR: Systematic review: Fatigue in inflammatory bowel disease. Aliment Pharmacol Ther 2010; 32: 131-143.
23. Nugent SG, Kumar D, Rampton DS and Evans DF: Intestinal luminal pH in inflammatory bowel disease: Possible determinants and implications for therapy with aminosalicylates and other drugs. Gut 2001; 48(4): 571-7. 24. Katsanos KH and Papadakis KA: Inflammatory bowel
disease: Updates on molecular targets for biologics. Gut Liver 2017; 11(4): 455-63.
25. Nemade MS, Chaudhari RY and Patil VR: Novel
approaches to colon targeted drug delivery system: A review. RRJPPS 2014; 3(2): 63-69.
26. Tiwari G, Tiwari R, Wal P, Wal A and Rai AK: Primary and novel approaches for colon targeted drug delivery-A review. Int J Drug Deliv 2010; 2(1): 1-11.
27. Badoni A, Ojha A, Gnanarajan G and Kothiyal P: Review on gastro retentive drug delivery system. The Pharma Innovation 2012; 1(8): 32-42
28. Patel A, Bhatt N, Patel KR, Patel NM and Patel MR: Colon targeted drug delivery system : A review system. J Pharm Sci Biosci Res 2011; 1(1): 37-49.
29. Pedreiro LN, Cury BSF, Chaud MV and Gremião MPD: A
novel approach in mucoadhesive drug delivery system to improve zidovudine intestinal permeability. Brazilian J Pharm Sci 2016; 52(4): 715-26.
30. Rathee P, Jain M, Garg A, Nanda A and Hooda A: Gastrointestinal mucoadhesive drug delivery system: A review. J Pharm Res 2011; 4(5): 1448-53.
31. Kumar JR, Muralidharan S, Dhanaraj SA and Umadevi SK: A novel drug delivery systems of colon targeted: A review. J Pharm Sci Res 2013; 5(2): 42-7.
32. Pleuvry BJ: Factors affecting drug absorption and distribution. Anaesthesia and Intensive Care Medicine 2005; 6: 135-138
33. Gandhi B and Baheti J: Multiparticulates drug delivery systems : A review. Int J Pharm Chem Sci 2013; 2(3): 1620-6.
35. Reddy RB, Malleswari K, Prasad G and Pavani G: Colon targeted drug delivery system: a review. IJPSR 2013; 4(1): 42-54.
36. Patel VR and Patel VP: Pulsatile drug delivery system-A review. Int J Pharm Sci Res 2015; 6(9): 3676-88.
37. Qureshi AM, Momin M, Rathod S, Dev A and Kute C: Colon targeted drug delivery system: A review on current approaches. Indian J Pharm Biol Res 2013; 1(4): 130-47.
38. Sadeghi AM, Avadi MR, Ejtemaimehr Sh, Abashzadeh S,
Partoazar A, Dorkoosh F, Faghihi M, Rafiee-Tehrani M, and Junginger HE: Development of a gas empowered drug delivery system for peptide delivery in the small intestine. Journal of Controlled Release 2008; 134: 11-7.
39. Singh G, Kumar D, Singh M, Sharma D and Kaur S: Emerging techniques and challenges in colon drug delivery systems. J Appl Pharm Sci 2012; 2(3): 139-47. 40. Amara AA and Shibl A: Role of probiotics in health
improvement, infection control and disease treatment and management. Saudi Pharm J 2015; 23(2): 107-14. 41. Sarangi MK and Padhi S: Colon targeted drug delivery
system-an approach for treating colonic ailments. J Crit Rev 2(3): 9-10.
42. Singh KI, Singh J, Sharma D and Sharma A: Colon-specific drug delivery system: review on novel approaches. IJPSR 2012; 3(3): 637-647.
All © 2013 are reserved by International Journal of Pharmaceutical Sciences and Research. This Journal licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License.
This article can be downloaded to Android OS based mobile. Scan QR Code using Code/Bar Scanner from your mobile. (Scanners are available on Google Play store)
How to cite this article: