All rights reserved
Use of Postmenopausal Hormone Replacement Therapy: Estimates from a
Nationally Representative Cohort Study
Kate M. Brett1 and Jennifer H. Madans2
The objective of this study was to describe trends in the use of hormone replacement therapy (HRT) in the United States by demographic, life-style, and heart disease risk factors. Data were obtained from the Epidemiologic Followup Study to the First National Health and Nutrition Examination Survey, a nationally representative cohort followed from the mid-1970s until 1992. A total of 5,602 women who had become menopausal by their last follow-up interview were included. An estimated 45% of the cohort of menopausal US women 25-74 years of age in the early 1970s used HRT for at least one month and 20% continued use for 5 or more years. Between 1987 and 1992, as the younger members of the cohort became menopausal, the proportion of this cohort who had ever used HRT and used it for 5 or more years increased by 32% and 54%, respectively. A higher probability of HRT use was found among women who were white, who were more highly educated, and who lived in the West, or who had experienced a surgical menopause. Women who were overweight or who abstained from alcohol were less likely to use HRT. These data support the hypothesis that HRT use is associated with sociodemographic factors, and that women tend to discontinue use within several years. Am J Epidemiol 1997;145:536-45.
cohort studies; estrogen replacement therapy; menopause; risk factors
Use of postmenopausal hormone replacement ther-apy (HRT) has fluctuated over the past 50 years due to changes in the perception of its risks and benefits. Although first approved in the 1940s, unopposed es-trogen replacement therapy became widely used start-ing in the 1960s (1). Use declined in the 1970s after the publication of reports of an association between estrogen use and uterine carcinoma (2, 3). With the introduction of combined estrogen/progestin hormone therapy in the 1980s, HRT has regained its popularity (4, 5). These drugs are currently among the most commonly prescribed medications in the United States, and were taken by an estimated 2.9 million women in 1986 (6, 7), increasing to an estimated 6 million women in 1992 (8).
The identification of several important effects of HRT beyond the reduction of menopausal symptoms, both protective and adverse, has increased interest in
Received for publication October 17, 1994, and accepted for publication November 1, 1996.
Abbreviations: Cl, confidence interval; HRT, hormone replace-ment therapy; NHANES I, First National Health and Nutrition Exam-ination Survey; NHEFS, NHANES I Epidemiologic Followup Study; OR, odds ratio.
1 Division of Epidemiology, National Center for Health Statistics,
CDC.
2 Office of vital and Health Statistics Systems, National Center for Hearth Statistics, CDC.
Reprint requests to Dr. Kate M. Brett, NCHS/DivisJon of Epide-miology, 6525 Belcrest Rd., Room 730, Hyattsville, MD 20782.
this drug therapy. Unopposed estrogen therapy ap-pears to be associated with a reduced risk of both heart disease (9-11) and osteoporotic fractures (12), espe-cially among current and long-term users. However, postmenopausal estrogen use increases the risk of uter-ine cancer (9) and may increase the risk of breast cancer (13). While the addition of progestin to HRT is not expected to change its association with osteoporo-sis, its effect on the risk of heart disease and breast cancer is less certain (9).
Several cross-sectional and cohort studies in the United States have reported estimates of HRT use (5, 14-22). These studies have yielded estimates of the proportion of postmenopausal women who take HRT in the selected studied populations ranging from 12 percent (17) to 47 percent (20). This disparity is due to many factors, including the time at which the data were collected, and the demographics and location of the study population. Women who take HRT appear to be healthier, more affluent, and more likely to under-take health promotion and disease prevention activities (6, 23-25). This has led to the conclusion by some that the association between HRT use and reduced heart disease incidence may be partially due to selection bias, although this remains controversial (26, 27).
Because the estimates of HRT use to date have been derived from studies of specific communities or occu-pational groups, they may not be generalizable to the
United States as a whole. This is especially true be-cause regional variation in use has previously been identified, with women in the Northeast having the lowest prevalence of use and women in the West the highest (4, 28). In this paper, we examine the cumu-lative incidence of HRT use and covariates of HRT use within a representative cohort derived from a representative sample of US women. We document the pattern of use in terms of duration and whether combination therapy was used in order to more fully describe the experience of US women in this birth cohort.
MATERIALS AND METHODS
The study population used for this analysis was taken from the Epidemiologic Followup Study to the First National Health and Nutrition Examination Sur-vey (NHEFS). This is a prospective cohort study of subjects who completed the First National Health and Nutrition Survey (NHANES I) in 1971 to 1975. Follow-up waves have been conducted in 1982-1984, 1986, 1987, and 1992 (29-31). The 1986, 1987, and 1992 NHEFS interviews were conducted by tele-phone, whereas the 1982-1984 interviews were con-ducted in person. Reproductive questions in 1982— 1984 were obtained through the use of self-administered written questionnaires in an effort to provide subject privacy.
HRT questions were first asked as part of the 1982— 1984 follow-up. At subsequent follow-up interviews, women who were not previously interviewed or were not previously menopausal were asked the entire bat-tery of retrospective questions while those who had provided information on HRT in a prior interview were only asked to update their previous responses.
The wording and type of the HRT questions changed over the course of the follow-up period to take into account changes in the type of HRT forma-tion in use at the time. Hormone use was derived primarily from the questions which asked whether or not a woman had taken "hormone pills for reasons related to menopause," the age at last use of these pills, and the total number of months or years of use. These questions were asked at every follow-up. An addi-tional question about the use of "an estrogen or hor-mone skin patch" was included in the last follow-up, when this mode of administration had become more common. Questions regarding whether the respondent took progestin were asked of women who were current HRT users at the 1987 follow-up and of all women who had ever used HRT at the 1992 follow-up. There-fore, designation of the type of HRT (estrogen only or combination estrogen and progestin) could only be made for a subsample of HRT users. NHEFS did not
ask the name of the drug, nor has an attempt been made to verify drug data.
Because the validity and reliability of information obtained from self-administered questionnaires such as that used in the 1982-1984 follow-up are lower than information obtained by an interviewer, especially in low education populations (32), data regarding HRT use were taken from the 1987 survey even when the same information was also available from the self-administered 1982 questionnaire (i.e., for women who ceased use before the 1982 interview, 244 of the 1,902 women in this category changed their responses to questions concerning the total number of months of use, but did not to change response regarding ever use of HRT). Data from interviews conducted with proxies were also excluded from this analysis because proxies would be less able to accurately answer medication and menopausal questions.
A variety of sociodemographic, health behavior, and heart disease predictor variables were included in these analyses. The covariates obtained by self-report at the baseline interview were the following: highest grade of education completed (<high school, high school, >high school), ethnicity (black, white, other), alcohol consumption (never, < 1 drink/month, 1 drink/ month-<l drink/day, ^ 1 drink/day), recreational ac-tivity (low, moderate-high), and oral contraceptive use (ever, never). Baseline smoking status (current, former, never) was obtained either at baseline, the first follow-up interview, or, if both of these sources of information were missing, imputed using data from respondents of the same gender and age (33). Self-reported health (excellent, good, fair-poor) was ob-tained from the follow-up interviews because it was not included in the baseline interview. Medical risk factors considered from the baseline interview were history of self-reported diabetes mellitus, hypertension (defined by self-report of hypertension, or having sys-tolic blood pressure over 160 mmHg or diassys-tolic blood pressure over 95 mmHg), high serum cholesterol (^200 mg/dl), and being overweight (body mass in-dex (weight [kg]/height[m]2) >120 percent of the national average of 27.3 kg/m2). Type of menopause was derived from the first interview administered after menopause. This was defined as follows: 1) natural menopause—having no periods or having irregular periods because they are going through the change of life; 2) surgical menopause—having had a bilateral oophorectomy before natural menopause; or 3) after hysterectomy—having had a hysterectomy without oophorectomy before natural menopause. Age at menopause was defined as the age when menses had stopped for 12 months for natural menopause, age at bilateral oophorectomy, or imputed as the average age
at natural menopause (48 years) for women who ex-perienced hysterectomy without bilateral oophorec-tomy. Year of menopause was birth year plus age at menopause.
Several criteria were used to determine eligibility for inclusion in this analysis. Of the 8,596 women examined in NHANES I, 1,681 were eliminated be-cause they had not been personally interviewed during any of the follow-up interviews (i.e., they were either lost to follow-up or a proxy was interviewed due to the death or incapacitation of the subject). An additional 1,142 women had not become menopausal at the time of the last interview. Nineteen women were missing information on HRT use and an additional 152 women were missing information on one or more of the co-variates of interest and were therefore eliminated, leaving 5,602 for analysis. This cohort of women has been followed for an average of 17.5 years and ranged in age from 25 to 74 years at the baseline examination. Several analyses were conducted whose purpose was the identification of covariates of HRT use. In-formation on these potential covariates was obtained either at baseline or at the first follow-up. For many women, menopause occurred many years prior to the measurement of the covariates, which would not allow us to identify the temporal relation between covariates and outcome. To control for this, we limited analyses of covariates to women who had become menopausal during or after the year of the baseline examination. This reduced the analytic sample to 2,784 women. The age of women in this group ranged from 25 to 66 years at the baseline examination. This group of women has been followed for an average of 18.8 years.
HRT use was described for the whole cohort in terms of ever use and length of use. Age at last use and use for more than 5 years were investigated using only those women who indicated use for at least one month. Use of estrogen only or combination HRT was also analyzed for the 1,990 women who indicated ever use of HRT in the 1992 follow-up wave (complete infor-mation on combination therapy was not available from earlier waves).
We also were interested in identifying potential ef-fect modifiers of these associations. Year and type of menopause, ethnicity, and education were examined as potential effect modifiers in the analysis of ever use of HRT. Due to limited sample sizes for other use vari-ables, interactions were not investigated in their anal-ysis. Interactions were considered significant if the p value of the Wald statistic was less than 0.10 and all the stratified sample sizes were at least 30 (1 percent of the cohort).
Bivariate analyses were conducted using contin-gency tables. Logistic regression models were used to
control for several factors simultaneously. While NHEFS data are best analyzed using techniques that take the differing lengths of follow-up into account (34), the lack of a beginning date of HRT use for 6 percent of HRT users precluded the use of survival techniques. Test-based confidence intervals were con-structed around relative risk estimates. The NHEFS cohort was derived from a national probability sample with selection probabilities that varied by age, sex, residence, and income. In order to obtain representa-tive estimates of US women, SUDAAN software was used to calculate weighted estimates of the various associations with HRT use and the corrected standard errors of these estimates (35). Statements regarding the sample were obtained from simple, unweighted calculations.
RESULTS
The mean reported age at menopause for the 83 percent of women in the NHEFS sample who had experienced menopause was 45.9 years (range 16-77 years). Twenty-two percent of the study cohort expe-rienced menopause as a result of a bilateral oophorec-tomy; the age at menopause among this group was 40.1 years compared with 47.5 years among women who had experienced menopause naturally. Age at menopause would be slightly higher had 100 percent of the study population experienced menopause, as the women still premenopausal by follow-up end were slightly older. By the last interview, the average age of the study cohort was 66.4 years.
Table 1 presents information regarding the study cohort by year of birth. Because not all women born in 1935 or later had experienced menopause at the time of their last interview, a smaller proportion of these birth cohorts were included in this study and their average age at menopause was younger than in the earlier cohorts because a large proportion of meno-pausal women in this birth cohort experienced surgical menopause. The use of HRT increases with year of birth. Only 19 percent of women born between 1885 and 1904 used HRT while 46 percent of those born between 1925 and 1934 used HRT. Usage in the youngest cohort is higher, which reflects the relatively small proportion of the cohort that had experienced menopause and the higher prevalence of surgical menopause in this group. Variation in usage by cohort reflects the availability of HRT when these cohorts became menopausal as well as beliefs concerning HRT at these times.
As estimated by this sample, 45 percent (95 percent confidence interval (CI) 43-47) of US women born between 1897 and 1950 who were menopausal by 1992 had used HRT for at least one month. The
TABLE 1. Menopausal status and use of hormonal replacement therapy (HRT) by year of birth among woman In the NHEFS* from the mid-1970s through 1992 (unweighted analyses)
Birth year 1895-1904 1905-1914 1915-1924 1925-1934 1935-1944 1945-1954 Total No. 677 1,017 1,011 1,594 1,878 738 6,915 Menopausal (%) 100 100 100 99 71 23 83 Effective no.t 630 972 982 1,543 1,312 163 5,602
Mean age (years) at menopause Natural 47.5 47.7 47.7 48.2 46.8* 41.6* 47.5 Surgical 42.0 40.0 48.9 41.6 38.7* 37.3* 40.1 Ever used HFIT (%) 19 27 46 46 52 63 42 * NHEFS, Epidemiologic Foliowup Study to the Rrst National Health and Nutrition Examination Survey. t Sample sizes were after removal of women who were either not yet menopausal or missing data for important covariates.
* Because the whole cohort was not yet menopausal, the mean age at menopause oniy included the women who had entered menopause at a relatively early age.
estimate of use for the whole cohort may change as the remainder of the cohort experiences menopause. Use varied greatly by year and type of menopause (figure 1). Among women who experienced menopause due to a bilateral oophorectomy, the group most likely to use HRT throughout the time period, use increased from 37 percent among women who became meno-pausal before 1945 to 71 percent for women who became menopausal in 1990-1992. In this group of women, the prevalence peaked among those who ex-perienced menopause between 1965 and 1969 and then remained relatively stable. The proportion of women who underwent menopause naturally who were ever-users has increased from 11 percent among
women who were menopausal earliest to 46 percent among women who were menopausal in 1990-1992, 38 percent less than women who had a oophorectomy. In this group, prevalence increased for each cohort until the early 1970s when it declined somewhat and then began rising at a slower pace starting among those who were menopausal in the early 1980s. Al-though the estimates are less precise among women who had hysterectomies without bilateral oophorec-tomy, the use of HRT among this group tended to be between the other two groups.
Among women who experienced menopause no ear-lier than the baseline examination (n = 2,784), surgi-cal menopause, white race, and higher alcohol
con-100
80
60
40
20
0
% ever using HRT
"Natural «*Hysterectomy w?Oophorectomy
\
JYear of Menopause
<$>
FIGURE 1. Use of hormone replacement therapy (HFIT) among US women interviewed in the Epidemiologic Foliowup Study to the Rrst National Health and Nutrition Examination Survey (NHEFS), by year of menopause (n = 5,602).
sumption were independently associated with an increased probability of HRT use (table 2). HRT use also varied by residence, with women in the West most likely to use HRT, and those who resided in the Northeast the least likely. Not being overweight and taking oral contraceptives were also found to be asso-ciated with increased probability of HRT use. How-ever, after controlling for other factors, HRT use did not vary significantly by self-reported health, recre-ational activity, or smoking. Fifty-six percent of women who had previously used oral contraceptives also had used HRT at some point, resulting in an estimated 28 percent having taken both drug therapies. In this and all subsequent analyses, serum cholesterol level, diabetes mellitus, and hypertension were not associated with HRT use and so were not included in the logistic models. There were no significant interac-tions found in the association with HRT use.
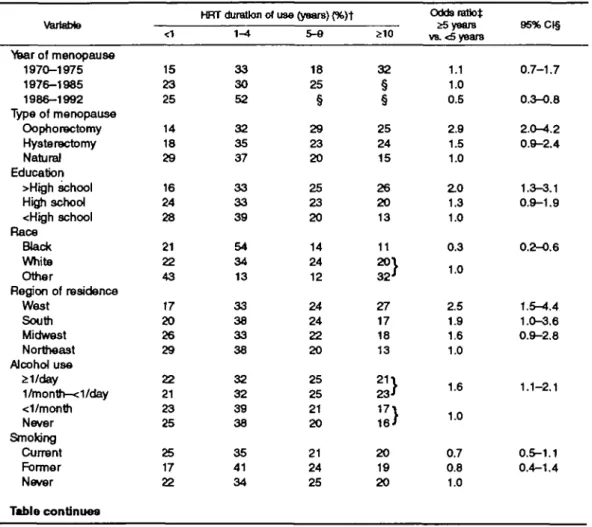
The length of HRT use was available for 2,287 of the 2,342 women (98 percent) in the sample who ever used HRT. The median length of use was 36 months, while the mean length of use was 6.6 years. Forty-three percent (95 percent CI39-47) of ever users used HRT for at least 5 years, and 20 percent of all women in the cohort used HRT for at least this long.
In a multivariate analysis of the 1,036 women who had used HRT and were followed for at least 5 years after menopause, women who had experienced meno-pause after bilateral oophorectomy were 1.9 times more likely to continue HRT use for at least 5 years than women who had a natural menopause (table 3). Women with more than a high school education were significantly more likely to continue HRT use for at least 5 years compared with women with less than a high school education. Black women were less than one-third as likely to continue HRT use for 5 years (odds ratio (OR) = 0.3, 95 percent CI 0.2-0.6) as women of other races. Women who were more than 20 percent overweight were also less likely to use HRT for at least 5 years than women who had a low body mass index (OR = 0.6, 95 percent CI 0.4-1.0). Res-idents of the West were significantly more likely than women who lived in the Northeast to continue HRT use for 5 years, but were not significantly different from women who lived in the Midwest and South. Finally, women who consumed at least one alcoholic beverage per month were more likely to continue HRT use than women who consumed little or no alcohol.
Thirty-one percent (95 percent CI 28-33) of women interviewed in 1992 who had used HRT took progestin while the remaining 69 percent of the women indi-cated they used estrogen only. Several of the variables which were associated with use of any HRT were also associated with use of combination therapy rather than
estrogen only: non-black race, college education, use of oral contraceptives, and body mass index less than 120 percent of average (table 4). Natural menopause was associated with more than three times the likeli-hood of combination HRT use compared with either menopause after bilateral oophorectomy or hysterec-tomy.
DISCUSSION
While the NHEFS cohort has the strength of being a nationally representative cohort study, this study de-sign has limitations relevant to this investigation. Self-report of menopausal estrogen use has been previously found to be fairly well reported, although the more detail requested, the less reliable the data become (36, 37). The agreement between physicians' records and interview data in one study was 87 percent (36), both for use and non-use. When we duplicated the analysis of ever-use including only the 3,523 women who were no more than 10 years beyond menopause at baseline and therefore more likely to reliably report HRT use (36), similar results were obtained.
We were able to check the consistency of HRT reporting among the women who completed at least two interviews in which they answered HRT ques-tions. Only 4 percent said they had used HRT during the one interview but contradicted this information in a subsequent interview. Of the women who said they had used HRT, however, more than 30 percent re-duced the length of time they reported using HRT by more than 6 months in either 1987 or 1992 compared with what they reported in 1982, while only 13-15 percent estimated their length of use to have increased by more than the time between the survey waves.
The wording of the NHEFS questions may have underestimated total HRT use. In the 1970s, injectable estrogens were used with about equal frequency as oral estrogens (4). The question used in this study prior to 1992 only asked about "hormone pills." Fur-thermore, noncontraceptive estrogen was used during this time period for indications other than "reasons related to menopause," such as prevention of osteopo-rosis (7).
Only data that were obtained from the subject, and not a proxy, were used to increase the reliability of the HRT use estimates. Follow-up interviews were ob-tained with 90 percent of the 4,584 women in the NHEFS study population who were still experiencing menses within 12 months of the baseline examination, and 97 percent of these women were personally inter-viewed at least once. If women who are healthier, and therefore do not need a proxy respondent, tend to use HRT, the estimates of use may have been inflated.
TABLE 2. U*e of honnone replacement therapy (HRT) by sociodemographic factors and coronary hoart disease risk factors among women who became menopausal between 1970 and 1992: NHEFS' (n = 2,784) Variable Year of menopause 1970-1975 1976-1985 1986-1992 Type of menopause Oophorectomy Hysterectomy Natural Education >High school High school <High school Race Black White Other Region of residence West South Midwest Northeast Alcohol use 21/day 1/month—e1/day <1/month Never Smoking Current Former Never Oral contraceptives Ever use Never use Body mass index
£120% average <120% average Recreational activity High/moderate Low Self-reported health Excellent Good Fair-poor Serum cholesterol £200mg/dl <200mg/dl Diabetes meHitus In history No history Hypertension In history No history No. 431 1,760 593 598 423 1,763 645 1,290 849 417 2,328 39 738 730 716 600 271 1,017 803 693 1,105 294 1,385 1,392 1,392 734 2,050 1,466 1,316 678 1,609 497 1,327 1,359 62 2,722 581 2,203 Ever used HRT(%)t 50.1 47.3 54.9 73.0 60.7 39.2 54.9 48.5 45.1 3£7 51.4 -i 55.1 / 60.3 47.9 50.2 37.6 56.3 53.3 47.4 42.2 48.8 52.9 49.0 56.3 41.8 36.7 53.3 55.6 50.0 48.8 49.0 48.3 47.1 51.6 47.6 49.5 44.3 50.7 Odds ratio (adjured*) 1.2 1.0 1.1 4.2 2.4 1.0 1.3 1.0 1.0 0.5 1.0 2.2 1.6 1.6 1.0 1.6 1.4 1.1 1.0 0.8 1.1 1.0 1.4 1.0 0.6 1.0 1.0 1.0 0.9 1.0 1.2 U H H U D D 95%Ct§ 0.9-1.6 0.9-1.4 3.3-5.5 1.8-3.1 0.9-1.7 0.8-1.3 0.3-0.7 1.5-3.1 1.1-2.3 1.1-2.3 1.2-2.3 1.1-1.9 0.8-1.4 0.7-1.1 0.8-1.5 1.2-1.8 0.4-0.7 0.8-1.2 0.7-1.1 0.9-1.7
* NHEFS, Epidemblogic Followup Study to the Rrst National Health and Nutrition Examination Survey. f All percents were standardized for year of menopause.
i Odds ratios were adjusted for all other variables listed. § Cl, confidence interval.
TABLE 3. Duration of hormone replacement therapy (HRT) use by soctodemographlc factors and coronary heart disease risk factors among women who became menopausal between 1970 and 1992 and who ever used HRT: NHEFS* (n = 1,313)
Variable
HRT duration of use (years) (%)t
<1 1-4 5-0 Odds ratio* £5 years vs. <5 years 95%CI§ Veer of menopause 1970-1975 1976-1985 1986-1992 Type of menopause Oophorectomy Hysterectomy Natural Education >High school High school <High school Race Black White Other Region of residence West South Midwest Northeast Alcohol use ;>i/day 1/month—e1/day <1/month Never Smoking Current Former Never Table continues 15 23 25 14 18 29 16 24 28 21 22 43 17 20 26 29 22 21 23 25 25 17 22 33 30 52 32 35 37 33 33 39 54 34 13 33 38 33 38 32 32 39 38 35 41 34 18 25 § 29 23 20 25 23 20 14 24 12 24 24 22 20 25 25 21 20 21 24 25 32 § § 25 24 15 26 20 13 11 20\ 32J 27 17 18 13 2 1) 2 3 •» 17} 16/ 20 19 20 1.1 1.0 0.5 2.9 1.5 1.0 ZO 1.3 1.0 0.3 1.0 2.5 1.9 1.6 1.0 1.6 1.0 0.7 0.8 1.0 0.7-1.7 0.3-0.8 2.0-^*.2 0.9-Z4 1.3-3.1 0.9-1.9 0.2-0.6 1.5-4.4 1.0-3.6 0.9-2.8 1.1-2.1 0.5-1.1 0.4-1.4
This bias would not be great due to the small propor-tion of lost subjects.
Many of the variables identified in this study to be associated with HRT use have previously been iden-tified as covariates. The consistent association be-tween HRT use and lean body size (5, 14-22) and surgical menopause (5, 17, 19-22) probably reflects the targeting of HRT toward women with lower ex-posure to endogenous estrogen. Education or socio-economic status (15-17, 19, 21) and race (17) may be indicators of differential in health behaviors and ac-cess to health care. The temporal trends in HRT use found here are well established (7), although they have tended to be addressed as an association between age and HRT use (5, 14, 16-19, 21, 39).
The association between regular alcohol consump-tion and average amount consumed has been found in some studies but not all studies (14, 15, 17, 19, 20, 22, 39). Because alcohol consumption by women at mod-erate levels is positively related to socioeconomic sta-tus (38), the increased use of HRT by women who also
consumed alcohol may be identifying another compo-nent of the positive association between socioeco-nomic status and HRT which was not captured by education level. Alternatively, alcohol consumption may influence HRT use through some other pathway. The finding that women who exercised regularly at baseline were no more likely to use HRT than non-exercisers when other factors were controlled is incon-sistent with several other studies' results (18-22, 39). When the data were reanalyzed using the most recent self-report of recreational activity to define exercise levels, HRT users were significantly more likely to exercise than nonusers, although this difference is not significant after controlling for other variables. The baseline exercise questions were not detailed and so may not have differentiated exercise in sufficient de-tail.
High serum cholesterol, hypertension, smoking, and diabetes mellitus, factors that are strongly related to heart disease, had no independent relation with HRT use. Neither blood pressure (10, 14, 21, 39) nor total
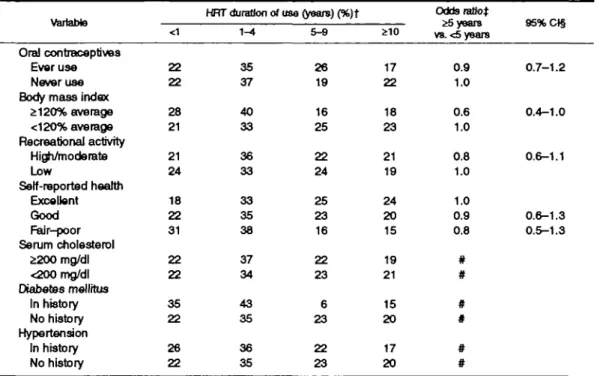
TABLE 3. Continued
Variable
<1
HRT duration of use (years) (%)t 1^4 5^9 Odds ratio:* ^5 years V8.<5 years Oral contraceptives Ever use Never use Body mass index
£120% average <120% average Recreational activity High/moderate Low Self-reported health Excellent Good Fair-poor Serum cholesterol £200mg/dl <200mg/dl Diabetes mellrtus In history No history Hypertension In history No history 22 22 28 21 21 24 18 22 31 22 22 35 22 26 22 35 37 40 33 36 33 33 35 38 37 34 43 35 36 35 95%Ct§ 26 19 16 25 22 24 25 23 16 22 23 6 23 22 23 17 22 18 23 21 19 24 20 15 19 21 15 20 17 20 0.9 1.0 0.6 1.0 0.8 1.0 1.0 0.9 0.8 # # # # # # 0.7-1.2 0.4-1.0 0.6-1.1 0.6-1.3 0.5-1.3
* NHEFS, Epidemiologic Followup Study to the First National Health and Nutrition Examination Survey, t All pencents were standardized for year of menopause.
£ Adjusted odds ratios, controlling for all other variables considered significant Analysis was conducted on the 1,036 women followed for at least 5 years after menopause.
§ Cl, confidence interval.
H A substantial proportion of women were not at risk of being exposed to HRT for this length of time due to the timing of menopause and so estimates are not given.
# These variables were not included in the multivariate models.
cholesterol (10, 21, 39) has been found to have a significant association with HRT use in previous stud-ies, although HRT users have been found to have higher high density lipoprotein and lower low density lipoprotein cholesterol levels (5, 14, 15, 21, 39). No consistent association has been found between HRT use and smoking.
The use of progestin is important to reduce the risk of endometrial cancer among HRT users with intact uteri (9). Even though women in this study who un-derwent a natural menopause were more than three times as likely to have taken progestin as women who experienced menopause after either a hysterectomy or oophorectomy, 20 to 30 percent of women who had undergone a hysterectomy and therefore were not at risk of uterine cancer reported using progestin. Use of progestin may lessen the potential benefit of estrogen use on coronary artery disease risk (9). Additionally, the effects of long-term use of progestin in combina-tion with estrogen remain unknown (8), which raises concern regarding the use of progestin, especially by women who are not at risk of uterine cancer.
The data from this study suggest that 20 percent of women who experienced menopause between 1970
and 1992 used HRT for at least 5 years, while 25 percent took HRT for at least one month but for less than 5 years. White race, higher education, alcohol consumption, and menopause that occurred between 1960 and 1974 were independently associated with increased probability of use, while residence in the Northeast and obesity decreased the probability of use. These data also indicate that several demographic and health indicators were related to sustained use over 5 or more years and to the use of progestin. These data also suggest national use of HRT is increasing among the birth cohorts studied, because use increased from 38 to 50 percent between the 1987 and 1992 follow-ups. Additional information in regard to national use patterns among all birth cohorts is needed to validate this finding.
ACKNOWLEDGMENTS
The authors thank Drs. Robert Spiritas and Joseph Kelaghan for their helpful comments.
TABLE 4. Use of combination estrogen/progastjn therapy among women who became menopausal between 1970 and 1992 and who ever used hormone replacement therapy (HRT): NHEFS»(n = 1,131) Variable Year of menopause 1985-1992 1975-1984 1965-1974 Type of menopause Oophorectomy Hysterectomy Natural Education >High school High school <High school Race Black White Other Region of residence West South Midwest Northeast Alcohol use 21/day 1/month—e1/day <1/month Never Smoking Current Former Never Oral contraceptives Ever use Never use Body mass index
£120% average <120% average Recreational activity High/moderate Low Serf-reported hearth Excellent Good Fair-poor Serum cholesterol £200 mg/dl <200 mg/dl Diabetes mellitus In history No history Hypertension In history No history %ol HHT userst 47 44 27 30 21 57 54 40 29 15 4 4 1 2 7 i 52 42 33 43 4 6 1 48 i 3 9 1 31 * 4 1 1 4 0 J 50 45 38 28 45 39 44 54 41 27 43 41 36 42 37 42 Odds ratio* 1.1 1.0 0.6 0.3 02 1.0 1.9 1.2 1.0 0.3 1.0 0.7 0.6 0.7 1.0 1.2 1.0 1.0 1.6 1.5 1.0 ' 0.6 1.0 0.9 1.0 1.8 1.6 1.0 D 1 H H 1 H 95%C1§ 0.8-1.5 0.3-1.1 0.2-0.4 0.1-0.3 1.2-3.1 0.8-1.9 0.1-0.6 0.4-1.4 0.3-1.1 0.4-1.1 0.8-1.7 1.0-2.5 1.1-2.2 0.4-0.9 0.7-1.2 1.0-3.3 0.9-2.7
• NHEFS, EpidemkXogtc Followup Study to the F*st National Health and Nutrition Examination Survey.
t AB percents were standardized by year ot menopause.
t Adjusted odds ratio, controllng for aO other variables considered
aJg-nrdcant.
§ Cl, confidence Interval.
H These variables were not included in the mulhariate models.
REFERENCES
1. Scalley EK, Henrich JB. An overview of estrogen replacement therapy in postmenopausal women. J Women's Health 1993; 2:289-94.
2. Smith DC, Prentice R, Thompson DJ, et al. Association of exogenous estrogen and endometrial carcinoma. N Engl J Med 1975;293:1164-7.
3. Ziel HK, Finkle WD. Increased risk of endometrial carcinoma among users of conjugated estrogens. N Engl J Med 1975; 293:1167-70.
4. Hemminki E, Kennedy DL, Baum C, et al. Prescribing of noncontraceptive estrogens and progestins in the United States, 1974-1986. Am J Public Health 1988;78:1478-81. 5. Barrett-Connor E, Wingard DL, Criqui MH. Postmenopausal
estrogen use and heart disease risk factors in the 1980s: Rancho Bernardo, Calif, revisited. JAMA 1989;261: 2095-2100.
6. Rosenberg L. Hormone replacement therapy: the need for reconsideration. Am J Public Health 1993;83:1670-3. 7. Kennedy DL, Baum C, Forbes MB. Noncontraceptive
estro-gens and progestins: use patterns over time. Obstet Gynecol 1985;65:441-6.
8. Wysowski DK, Golden L, Burke L. Use of menopausal estro-gens and medroxyprogesterone in the United States,
1982-1992. Obstet Gynecol 1995;85:6-10.
9. Emster VL, Bush TL, Huggins GR, et al. Benefits and risks of menopausal estrogen and/or progestin hormone use. Prev Med 1988;17:201-23.
10. Stampfer MJ, Colditz GA. Estrogen replacement therapy and coronary heart disease: a quantitative assessment of the epi-demiologic evidence. Prev Med 1991;20:47-63.
11. Hunt K, Vessey M, McPherson K. Mortality in a cohort of long-term users of hormone replacement therapy: an updated analysis. Br J Obstet Gynaecol 199O;97:1080-6.
12. Lindsay R, Cosman F, Nieves J. Estrogen: effects and actions in osteoporosis. Osteoporosis Int 1993;3(Suppl l):S150-2. 13. Steinberg KK, Thacker SB, Smith SJ, et al. A meta-analysis of
the effect of estrogen replacement therapy on the risk of breast cancer. JAMA 1991;265:1985-90.
14. Wilson PWF, Garrison RJ, Castelli WP. Postmenopausal es-trogen use, cigarette smoking, and cardiovascular morbidity in women over 50: the Framingham Study. N Engl J Med 1985; 313:1038-43.
15. Bush TL, Barrett-Connor E, Cowan LD, et al. Cardiovascular mortality and noncontraceptive use of estrogen in women: results from the Lipid Research Clinics Program Follow-up Study. Circulation 1987;75:1102-9.
16. Criqui MH, Suarez L, Barrett-Connor E, et al. Postmenopausal estrogen use and mortality: results from a prospective study in a defined, homogeneous community. Am J Epidemiol 1988; 128:606-14.
17. Egeland GM, Matthews KA, Kuller LH, et al. Characteristics of noncontraceptive hormone users. Prey Med 1988:17: 403-11.
18. Harris RB, Laws A, Reddy VM, et al. Are women using postmenopausal estrogen? A community survey. Am J Public Health 1990;80:1266-8.
19. Cauley JA, Cummings SR, Black DM, et al. Prevalence and determinants of estrogen replacement therapy in elderly women. Am J Obstet Gynecol 1990;163:1438-44.
20. Stampfer MJ, Colditz GA, Willett WC, et al. Postmenopausal estrogen therapy and cardiovascular disease: ten-year fol-low-up from the Nurses' Health Study. N Engl J Med 1991; 325:756-62.
21. Derby CA, Hume AL, Barbour MM, et al. Correlates of postmenopausal estrogen use and trends through the 1980s in two southeastern New England communities. Am J Epidemiol
1993;137:1125-35.
22. Johannes CB, Crawford SL, Posner JG, et al. Longitudinal patterns and correlates of hormone replacement therapy use in middle-aged women. Am J Epidemiol 1994; 140:439-52.
23. Barrett-Connor E. Postmenopausal estrogen and prevention bias. Ann Intern Med 1991 ;115:455-6.
24. Posthuma WFM, Westendorp RGJ, Vandenbroucke JP. Car-dioprotective effect of hormone replacement therapy in post-menopausal women: is the evidence biased? BMJ 1994;308:
1268-9.
25. Rosenberg L, Palmer JR, Shapiro S. A case-control study of myocardial infarction in relation to use of estrogen supple-ments. Am J Epidemiol 1993;137:54-63.
26. Duncan MH. Hormone replacement therapy: cardioprotective effect is genuine. (Letter). BMJ 1994;309:191.
27. Stevenson JC, Baum M. Hormone replacement therapy should be used selectively. (Letter). BMJ 1994;309:191.
28. Rosenberg L, Shapiro S, Kaufman DW, et al. Patterns and determinants of conjugated estrogen use. Am J Epidemiol 1979;109:676-86.
29. Cohen BB, Barbano HE, Cox CS, et al. Plan and operation of the NHANES I Epidemiologic Followup Study, 1982-84. Hyattsville, MD: National Center for Health Statistics, 1987. (Vital and health statistics, Series 1: Programs and collection procedures, no. 22) (DHHS publication no. (PHS) 87-1324). 30. Finucane FF, Freid VM, Madans JH, et al. Plan and operation of the NHANES I Epidemiologic Followup Study, 1986. Hyattsville, MD: National Center for Health Statistics, 1990. (Vital and health statistics, Series 1: Programs and collection procedures, no. 25) (DHHS publication no. (PHS) 90-1307). 31. Cox CS, Rothwell ST, Madans JH, et al. Plan and operation of the NHANES I Epidemiologic Followup Study, 1987. Hyatts-ville, MD: National Center for Health Statistics, 1992. (Vital
and health statistics, Series 1: Programs and collection proce-dures, no. 27) (DHHS publication no. (PHS) 92-1303). 32. Dillman DA. Mail and telephone surveys: the total design
method. New York: John Wiley & Sons, 1978.
33. Kleinman JC, Donahue RP, Harris MI, et al. Mortality among diabetics in a national sample. Am J Epidemiol 1988;128: 389-401.
34. Ingram DD, Makuc MD. Statistical issues in analyzing the NHANES I Epidemiologic Followup Study. Hyattsville, MD: National Center for Health Statistics, 1994. (Vital and health statistics, Series 2: Data evaluation and methods research, no. 121) (DHHS publication no. (PHS) 94-1395).
35. Shah BV, Barnwell BG, Bieler GS. SUDAAN user's manual: software for analysis of correlated data, release 6.40. Research Triangle Park, NC: Research Triangle Institute, 1995. 36. Goodman MT, Nomura AMY, Wilkens LR, et al. Agreement
between interview information and physician records on his-tory of menopausal estrogen use. Am J Epidemiol 1990; 131: 815-25
37. Jannausch ML, Sowers MR. Consistency of perimenopausal estrogen use reporting by women in a population-based pro-spective study. Maturitas 1992;14:161-9.
38. Darrow SL, Russell M, Cooper ML, et al. Sociodemographic correlates of alcohol consumption among African-American and white women. Women Health 1992; 18:35-51.
39. Nabulsi AA, Folsom AR, White A, et al. Association of hormone-replacement therapy with various cardiovascular risk factors in postmenopausal women. N Engl J Med 1993;328: 1069-75.