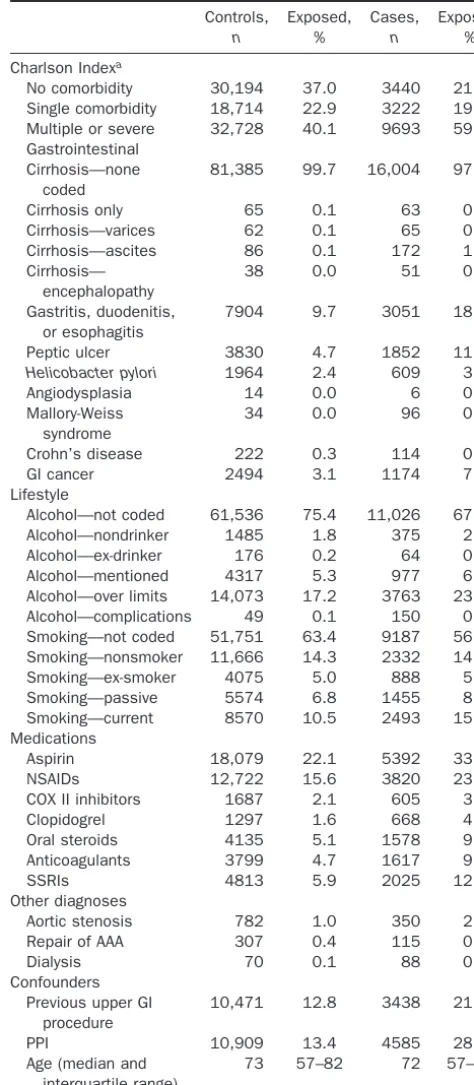
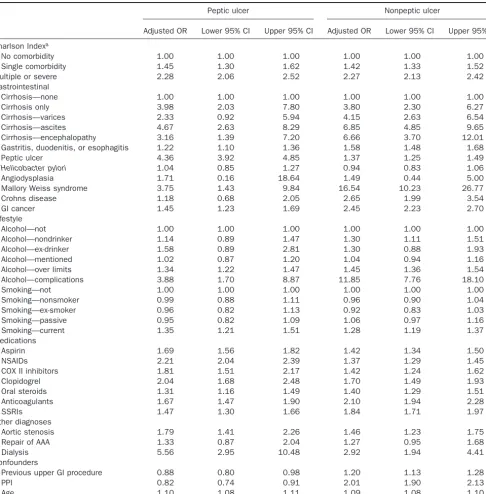
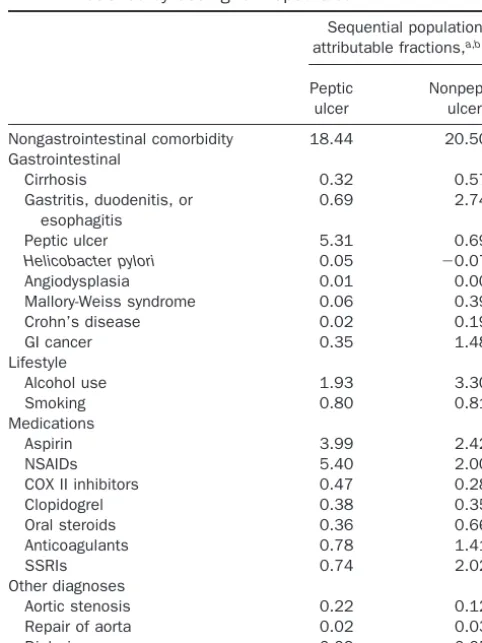
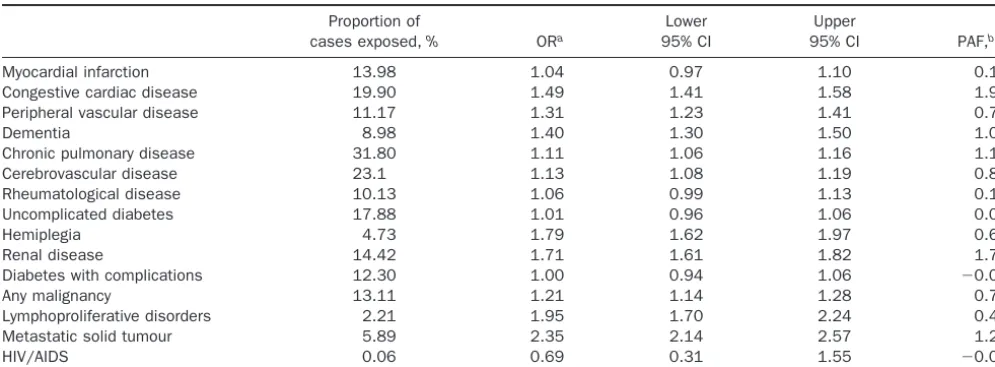
Comorbidities affect risk of nonvariceal upper gastrointestinal bleeding
Full text
Figure


Related documents
Those results indicate that high levels of formal training positively influence the reading and interpretation results of the map and that there is no evidence that the
The paper is organized as follows: In the introduction we list the interactivist objections to the classical representations; in the second section we describe the
The increase of grain yield with either nitrogen or biochar application is a consequence of better maize growth, The higher yield of nitrogen plus biochar maize, again
In Figure 4.6 we can see the main window of the application where the user can create a new guide or access to the list of guides already created.. Figure 4.6 Main Window
2005 R Aggarwal, Department of Biosurgery and Surgical Technology, Imperial College London and Regional Vascular Unit, St Mary’s Hospital, London Acquisition of endovascular skills
In this paper we look at various cryptographic techniques proposed by other researchers and propose an effective cryptographic technique for securing data stored
Here, we in- fer the palaeoclimate during the MMCT and the succeeding cooling phase for a middle Miocene (14.8–13.2 Ma) intra- montane basin in southwestern Anatolia using
The vertical layer averaging affects the flux estimate, but the choice of raw wind or mass-balanced wind is more impor- tant than the thickness of the vertical averaging for
