Gabriel Lingesh1, Selina Khoo2, Mohd. Nahar Azmi Mohamed1, Nur Aishah Taib3And MyBCC Group
1 Sport Medicine Department, University Malaya Medical Centre, University of Malaya 2 Sports Centre, University of Malaya
3 Surgery Department, Faculty of Medicine, University of Malaya
The work was supported by the University of Malaya/Ministry of Higher Education (UM.C/HIR/MOHE/06) High Impact Research Grant MyBCC and approved by our Medical Ethics Committee (Mec no. 866.31 22/7/2011).
Abstract
Objectives: There is strong evidence that regular physical activity (PA) is associated with significant health benefits for individuals of all ages. Therefore, it is necessary to have an accurate assessment of PA levels to ensure that individuals participate in sufficient PA to gain health benefits. This study compared PA levels obtained from the Malay language versions of the International Physical Activity Questionnaire (IPAQ-L: M) and Global Physical Activity Questionnaire (GPAQ: M) with those from a PA log and accelerometer. Study Design: Experimental–Cross Sectional study Methods: Data were collected from 43 female nurses aged 24 to 55 years (44.48 ± 8.38 years). In this cross-sectional study, participants answered the IPAQ-L:M or GPAQ:M and wore the accelerometer for seven consecutive days and answered GPAQ:M or IPAQ-L:M and PA log on the eight day. Physical activity levels (low, moderate and high) and total MET-min/week−1 were calculated and compared to determine if
individuals have sufficient energy expenditure during Physical activity . Results: All forty three participants reported high levels of PA on both questionnaires (IPAQ-L: M = 81.4%; GPAQ: M = 67.4%). However, all participants were categorised as low PA with the Sense Wear accelerometer. There was no significant difference in the moderate (IPAQ-L: M 2.3%; GPAQ: M = 18.6%) and low (IPAQ-L: M = 16.3%; GPAQ: M = 14%) levels of PA reported in the IPAQ and GPAQ (p > 0.05). Conclusion: The PA self-assessment instruments (questionnaires) yielded high overestimation in classifying PA level and underestimation in terms of Metabolic Equivalent of Task. Therefore, when classifying people as active or inactive, special attention must be given to the assessment method used. Further study is needed to produce a more accurate subjective measure which is equivalent to objective measures like the accelerometer.
INTRODUCTION
There is rising concern in the global pandemic for physical inactivity due to the lack of attention given to the importance of an active lifestyle [1]. However in Malaysia, the National Health and Morbidity Survey 2015 reported that the overall prevalence of physical activity in adults was 66.5% where males (71.1%) were significantly more active than females (61.7%). There is strong evidence that regular physical activity (PA) is associated with significant physiological and psychological health benefits for individuals of all ages [2]. PA has also been associated with improved chronic and non-communicable diseases such as diabetes, high blood pressure, cardiovascular diseases and cancer [3-6]. The psychological benefits of PA include improved mood, self-esteem and quality of life as well as reduction in symptoms of depression and anxiety [7].
The World Health Organization (WHO) recommends that adults aged 18–64 years should do at least 150 minutes of moderate-intensity or 75 minutes of vigorous-moderate-intensity aerobic PA or a combination of moderate- and vigorous-intensity PA per week. Therefore, it is necessary to have an accurate assessment of PA to ensure that individuals participate in adequate PA to gain health benefits [8]. There are various objective and subjective tools and methods available to measure PA. Objective measures include pedometers, accelerometers and heart rate monitors whereas subjective measures are self-report questionnaires, PA logs and diaries. However, all these methods have advantages and disadvantages [9]. The
most cost-effective and practical method of measuring PA is by using questionnaires, especially for large scale studies. Questionnaires can provide an estimate of frequency, duration, and intensity of PA.
However, they are influenced by the respondent’s capacity to recall past PA behaviour [10-12]. Because of that, individual self-report PA measures are less appropriate for research looking at PA levels because of the susceptibility to information bias and misclassification [13,14]. Self-report measures are generally used to estimate PA characteristics of a population. PA log can be a powerful subjective tool in terms of accuracy and to provide precise data [9]. However, the need to constantly record daily activity at every given point of time is demanding and time consuming. Accelerometers are the most practical and effective compromise between accuracy and feasibility for measuring PA and energy expenditure [15]. However, the limitations of accelerometers include the inability to record non-ambulatory activity, the relative high cost in addition to variability and reliability of different brands. Although there are more than 90 different PA questionnaires, two of most commonly used are the International Physical Activity Questionnaire (IPAQ) and the Global Physical Activity Questionnaire (GPAQ). The IPAQ has two forms: the long form (IPAQ-L) comprises 27 items and the short form (IPAQ-S) which consists of 7 items. The IPAQ-L is designed specifically for population surveillance of PA among individuals aged 15 to 69 years. The IPAQ long and short forms are being used as an evaluation tool in intervention studies for different populations, for example, cancer, diabetes, arthritis and older adults [16-18]. The 16-item GPAQ was designed specifically for surveillance studies in developing countries and has been used to measure a wide range of health-enhancing PA in various countries [10, 19-22].
reported that they were not as accurate and reliable as they should be as they were dependent on lifestyle patterns and the capability of the respondents in recalling and answering the questionnaire [2, 36, 37]. Previous studies have reported that the GPAQ showed better reliability and accuracy for persons with stable work patterns compared to persons with more variable PA patterns [20]. The IPAQ-L has been found to overestimate PA levels [2, 13].
Studies have not compared subjective and objective measures between the IPAQ-L, GPAQ, daily PA log and accelerometer. A compilation of all types of available PA questionnaires can be found in the study by Helmerhorst et al. (2012). However, it is unclear how accurate the subjective measures are compared to the accelerometer. Therefore, the purpose of this study was to compare PA levels obtained from the Malay versions of the IPAQ (IPAQ-L: M) and GPAQ (GPAQ: M) with those from a PA log and accelerometer.
METHODS
A cross-sectional method was used in this study. The sample comprised female hospital nurses who had good command of the Malay language. Nurses with physical illness or disabilities that would limit daily physical activities such as walking were excluded from the study. Participants volunteered to take part in this study and provided informed consent prior to participation. This study was approved by the university ethics committee. Sample size was determined based on power analysis. A sample size of 33 was needed for this study to provide an 80% power to detect a significant response in self-report MET-min/week−1value
at p < 0.05. To plan against 30% attrition, we recruited a total of 43 nurses.
Assessment of physical activity by IPAQ and GPAQ
The Malay versions of the IPAQ (IPAQ-L: M; r = 0.7 - 0.9) and GPAQ (GPAQ: M; r = 0.7 - 0.8) [10,11] were used. Based on the total amount of PA scores obtained, participants were classified into one of three PA
levels (low, moderate or high). For the IPAQ-L: M, the following Kilocalories and Metabolic Equivalent of Task (METs) values were used: walking = 3.3 METs, moderate activity = 4.0 METs, and vigorous activity = 8.0 METs. High PA level is defined as vigorous-intensity activity on at least three days achieving a minimum total physical activity of at least 1,500 MET-minutes/week or seven days of any combination of walking, moderate-intensity or vigorous-intensity activities achieving a minimum total PA of at least 3,000 MET-minutes/week. Moderate PA level is classified as five or more days of any combination of walking, moderate-intensity or vigorous intensity activities achieving a minimum total PA of at least 600 MET-minutes/week. A person who does not meet the high or moderate PA level criteria is classified as low PA.
For the GPAQ: M, METs were calculated based on the following: walking = 4.0 METs, moderate = 4.0 METs and vigorous = 8.0 METs. The MET-min week−1 was
calculated as minutes of activity/day × days per week × MET level. High PA level is defined as vigorous-intensity activity on at least 3 days achieving a minimum of at least 1,500 MET-min week−1 or- 7 or more days of any
combination of walking, moderate or vigorous intensity activities achieving a minimum of at least 3,000 MET-min week−1. Moderate PA
level is defined as 3 or more days of vigorous-intensity activity of at least 20 minutes per day or 5 or more days of moderate-intensity activity or walking of at least 30 minutes per day or 5 or more days of any combination of walking, moderate- or vigorous intensity activities achieving a minimum of at least 600 MET-min week−1. A person who does not meet either the
high or moderate PA level criteria falls in this category.
Data cleaning were based on IPAQ and GPAQ analysis guides. Each participant must have a valid response for at least one domain and have no invalid responses for any domains. Data entry which did not meet these requirements were excluded.
We used the SenseWear Mini (SWA; BodyMedia, Inc., Pittsburgh, Pennsylvania) accelerometer (software V.7.0, algorithm V.2.2.4) which has been widely used in research [2, 11, 16, 18,]. The SWA provides objective information such as PA level, energy expenditure, METs value, and sleep estimation. PA was reported as minutes per day of sedentary time, moderate activity and vigorous activity and as MET-minutes (where 1 MET is equivalent to resting energy expenditure) of moderate-to-vigorous PA (minutes of moderate activity × 4.0 METs + minutes of vigorous activity × 8.0 METs). These specific METs values within the moderate (3.0 – 6.0 METs) and vigorous (> 6.0 METs) intensity ranges were chosen for consistency with the MET values assigned for moderate and vigorous activity in the IPAQ and GPAQ scoring protocol. Anything below these values were considered low PA levels. Kilocalories and METs were converted into kcal/kg/hour. Data cleaning is based on SWA analysis guide which include device must be worn for more than 14 hours a day for seven consecutive days. Device that did not meet the requirements were excluded.
Assessment by PA log
All participants receive a PA log diary to record their daily activity for seven days. Accuracy of reporting in the PA log depended on the participant’s precise recording of daily activities. Activities were converted to the following MET values: walking = 3.3 METs, moderate activity = 4.0 METs and vigorous activity = 8.0 METs. Classification of PA levels was also classified according to similar categories with IPAQ.
Procedure
A cross-over method was used to compare the IPAQ-L: M and GPAQ: M. Participants were randomly divided into two groups. Participant demographic information was collected as to height and weight measurements. Group 1: During the first visit, participants answered the GPAQ:M and given a PA log to record daily activities for a week and the SWA to wear for seven consecutive
days except when bathing, showering or participating in water activities. On Day 8, participants returned the SWA and answered the IPAQ-L: M. Group 2: During the first visit, participants answered the IPAQ-L: M and given a PA log book to record daily activities for a week and the SWA to wear for seven consecutive days except when bathing, showering or participating in water activities. On Day 8, participants returned the SWA and answered the GPAQ: M. All questionnaires were self-administered.
Statistical analysis
Data was analysed using SPSS version 20. Descriptive statistics (means and standard deviations) were calculated for all variables. Participants were categorised into three PA categories (low, moderate or high) based on their total PA scores. The PA scores, described as mean METs-min week-1, were used to
compare data obtained from the questionnaires, PA log and accelerometer. METs calculations for the IPAQ-L: M and GPAQ: M were based on the respective analysis guides [38,39]. In many previous studies, minutes of PA were used to determine PA levels. We, however, used METs-min/week-1 because energy
expenditure is a more reliable and accurate measurement for PA level. This is because time-based work can be easily misconstrued by the intensity on the work performed. Comparison between these four instruments (IPAQ-L: M, GPAQ: M, PA log and SWA) was done using Pearson correlations. Paired sample t-tests were used to determine the mean difference in MET-min week-1between GPAQ:
RESULTS
A sample of 43 female participants aged between 24 to 55 years (44.48 ± 8.38 years) participated in the study. Their mean weight was 71.32 ± 10.91 kg, mean height 155.72 ± 5.71 cm and mean BMI 28.98 ± 4.39. Table 1 shows the descriptive statistics on SWA, GPAQ: M, IPAQ-L: M and PA log.
Table 1: Descriptive Statistics on SWA, GPAQ: M, IPAQ-L: M and PA log
SWA GPAQ:
M
IPAQ-L:
M PAL
Mean 15818.2 1
6495.02 7475.06 11256.5 1
Std.
Dev
1845.83 7304.85 8303.56 3424.29
SWA = SenseWear Accelerometer, GPAQ:M = Global Physical Activity Questionnaire: Malay Version, IPAQ-L: M = International Physical Activity Questionnaire long Form: Malay Version, PAL = Physical activity log
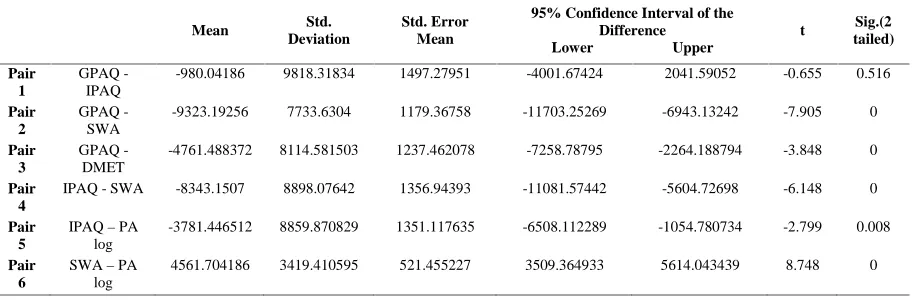
Table 2 (see next page) shows the mean total METs min per week-1 compared using
paired sample t-tests. Significant differences were found in the mean MET-min week-1
between IPAQ-L: M with SWA and PA log as well as between GPAQ: M with SWA and PA log (p < 0.05). There was no significant difference between the mean MET-min week-1
between the IPAQ-L: M and GPAQ: M. In addition, standard deviations around the means were substantially greater in IPAQ-L: M and GPAQ: M indicating greater variance in self-reported activity levels. Paired sample t-tests showed significant differences between IPAQ-L: M and SWA, GPAQ: M and SWA, IPAQ-IPAQ-L: M and PA log, GPAQ: M and PA log, SWA and PA log. However, there was no significant difference between IPAQ-L: M and GPAQ: M. Therefore a Bland-Altman plot was created which indicated that there was no proportional bias and there was an agreement between IPAQ-L: M and GPAQ: M.
Table 3 (See next page) shows the comparison of PA levels between GPAQ: M,
IPAQ-L: M and SWA. More than half the participants reported high levels of PA on both questionnaires (GPAQ: M = 67.4%; IPAQ-L: M = 81.4%). Participants reported more moderate PA in the GPAQ: M (18.6%) compared to the IPAQ-L: M (2.3%). There were nearly equal numbers of participants who reported low PA (GPAQ: M = 14%; IPAQ-L: M = 16.3%) on both questionnaires. All 43 participants were categorised as low PA based on METs-kcal/kg/hour (1.36 ± 0.17) on the SWA despite having high (15818.21 ± 1845.83) MET-min week-1values.
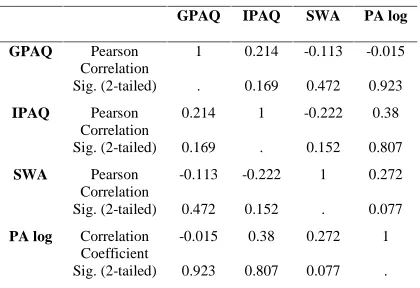
Table 4: Pearson Correlation between GPAQ: M, IPAQ-L: M, SSWA & PA log METs-min/week-1
GPAQ IPAQ SWA PA log
GPAQ Pearson Correlation
1 0.214 -0.113 -0.015 Sig. (2-tailed) . 0.169 0.472 0.923 IPAQ Pearson
Correlation
0.214 1 -0.222 0.38 Sig. (2-tailed) 0.169 . 0.152 0.807
SWA Pearson
Correlation
-0.113 -0.222 1 0.272 Sig. (2-tailed) 0.472 0.152 . 0.077 PA log Correlation
Coefficient
-0.015 0.38 0.272 1 Sig. (2-tailed) 0.923 0.807 0.077 .
SWA = SenseWear Accelerometer, GPAQ:M = Global Physical Activity Questionnaire: Malay Version, IPAQ-L: M = International Physical Activity Questionnaire long Form: Malay Version, PAL = Physical activity log
* Coefficientsa (constant p = .833, GPAQ vs
IPAQ mean p = .405)
Table 4 shows the correlations between GPAQ: M, IPAQ-L:M, SSWA and PA log METs-min/week-1. The Pearson correlation coefficient
revealed a negligible negative correlation (r = -0.222, p > 0.05) between IPAQ-L: M and SWA, a negligible negative correlation (r = -0.113, p
> 0.05) between GPAQ: M and SWA and a positive correlation between SWA and PA log (r = 0.272, p = 0.077) and no significant correlation between IPAQ and GPAQ (r = 0.214, p > 0.05). There is negative correlation between GPAQ and PA log (r = -0.015, p > 0.05) and a positive correlation between IPAQ-L: M and PA log (r = 0.038, p > 0.05).
DISCUSSION
This study aimed to find a reliable and accurate subjective measure of PA which is conceptually equivalent to the more accurate objective measure which is the accelerometer. We found that there were no correlations between the IPAQ-L: M and SWA as well as GPAQ: M and SWA. Recent studies have also reported no correlation between the short form of the IPAQ and accelerometer [13,14]. This indicated that both questionnaires were not reliable and accurate when quantifying PA scores in METs-min/week-1.
Table 2: Paired sample t-test on METs-min week-1(of SWA, GPAQ: M, IPAQ-L: M and PA log)
Mean Std.
Deviation
Std. Error Mean
95% Confidence Interval of the Difference
Lower Upper
t Sig.(2
tailed)
Pair 1
GPAQ -IPAQ
-980.04186 9818.31834 1497.27951 -4001.67424 2041.59052 -0.655 0.516
Pair 2
GPAQ -SWA
-9323.19256 7733.6304 1179.36758 -11703.25269 -6943.13242 -7.905 0
Pair 3
GPAQ -DMET
-4761.488372 8114.581503 1237.462078 -7258.78795 -2264.188794 -3.848 0
Pair 4
IPAQ - SWA -8343.1507 8898.07642 1356.94393 -11081.57442 -5604.72698 -6.148 0
Pair 5
IPAQ–PA log
-3781.446512 8859.870829 1351.117635 -6508.112289 -1054.780734 -2.799 0.008
Pair 6
SWA–PA log
4561.704186 3419.410595 521.455227 3509.364933 5614.043439 8.748 0
Table 3: METs-min week-1comparison on PA level between GPAQ, IPAQ & SWA
GPAQ PA Level IPAQ PA level SSWA PA level
Low 923.33 667.46 6 550.78 208.05 7 15818.21 1845.83 43
Moderate 1243 197.01 8 1200 . 1 - -
-High 9096.62 7642.56 29 9039.20 8462.68 35 - -
-Total 6495.02 7304.85 43 7475.06 8303.56 43 15818.21 1845.83 43
However, there was a weak positive correlation between the IPAQ-L: M and GPAQ: M. Studies which investigated the relationship between the short form of the IPAQ and GPAQ also reported a weak relationship between both measures (r = .2 - .4) [11, 12, 40]. This showed that both questionnaires were almost similar in quantifying PA scores using METs-min/week -1. In this study, the MET-min/week-1 values
calculated from both questionnaires underestimated the METs value when compared to the SWA and PA log. This suggests that the participants’ ability to recall the previous week’s PA was less accurate compared to the PA log. The PA log showed a weak correlation with the SWA (p > 0.05).
In terms of PA levels, SWA shows that all participants fell into the low PA category based on METs-kcal/kg/hour. Results of METs-kcal/kg/hour on the SWA device showed a mean of 1.36 ± 0.17 METs-kcal/kg/hour despite having high (15818.21 ± 1845.83) MET-min week-1 values. The cut-off
point for moderate PA levels is more than 3.0 METs-kcal/kg/hour and for high PA levels more than 6.0 METs-kcal/kg/hour. However, currently IPAQ and GPAQ do not use METs-kcal/kg/hour to classify PA levels. Both the IPAQ-L: M and GPAQ: M overestimated PA levels when compared to the SWA. This was similar to other studies where healthy adults overestimated their PA by as much as 17% to 67% [10, 22, 23]. This indicated that two subjective measures (IPAQ, GPAQ) were not accurate when compared to the objective measure (SWA). This was also seen in this study where our Bland-Altman plot analysis indicated that GPAQ and IPAQ showed agreement as both questionnaires provide similar scores. When compared to the SWA, the PA log reported more accurate scores than the IPAQ-L: M and GPAQ: M. This indicated
that daily recording of PA have shown to be better in providing reliable PA scores compared to both questionnaires which require one week recall. When answering both questionnaires, participants may forget to record short-duration activities, such as active transport, leading to an underreporting of these activities.
Feedback from participants after the study indicated that the GPAQ; M was easier to answer compared to the IPAQ-L: M because the questions were fewer in number and more straightforward. The GPAQ: M was also less time-consuming compared to the PA log. This indicates that the GPAQ:M is more suitable to be used among nurses in this study. However, a limitation of this study is the small sample size which made it difficult to draw a firm conclusion on the accuracy of the subjective versus the objective measures.
Conclusions
PA self-assessment instruments overestimated PA levels and underestimated METs values. Therefore, when classifying people as active or inactive for clinical purposes, special attention must be given to the assessment method used. Results suggest that there was no significant difference in the accuracy between the IPAQ-L: M and GPAQ: M. Our data suggested that it is important to improve the sensitivity and specificity of the questionnaires especially with Malay speaking participants.
Acknowledgments
UM.C/HIR/MOHE/06 from the Ministry of Higher Education of Malaysia.
Author Contributions
GL, SK & MNAM conceived and designed the experiments. GL, SK & MNAM performed the
experiments. GL analysed and interpreted the data. GL, SK, MNAM & NAT contributed reagents/materials/analysis tools. GL, SK & MNAM drafted the original manuscript. NAT provided critical revision of manuscript for intellectual content.
REFERENCES
1. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect Of Physical Inactivity On
Major Non-Communicable Diseases Worldwide: An Analysis Of Burden Of Disease And Life Expectancy.
Lancet 2012; 380: 219–29.
2. Sebastiao, E., Gobbi, S., Chodzko-Zajko, W., Schwingel, A., Papini, C. B., Nakamura, P. M., Netto, A. V., Kokubun, E., The International Physical Activity Questionnaire-long form overestimates self-reported
physical activity of Brazilian adults. Public health 2012.
3. World Health Organization. Global Recommendations on Physical Activity for Health. Geneva, Switzerland: World Health Organization 2010.
4. Disease Control Division. Malaysia NCD Surveillance 2006:NCD Risk Factors in Malaysia. Putrajaya, Malaysia: Disease Control Division 2006.
5. World Health Organization, Global health risks. Mortality And Burden Of Disease Attributable To
Selected Major Risks. World Health Organization 2009.
6. World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases. Geneva, Switzerland: World Health Organization; 2003.
7. Warburton, D. E., Katzmarzyk, P. T., Rhodes, R. E., Shephard, R. J., Evidence-Informed Physical
Activity Guidelines For Canadian Adults. Canadian Journal Of Public Health Revue Canadienne De Sante
Publique 2007, 98 Suppl 2: p. 16-68.
8. Nicaise, V., Crespo, N. C., Marshall, S., Agreement Between the IPAQ and Accelerometer for
Detecting Intervention-Related Changes in Physical Activity in a Sample of Latino Women. Journal Of
Physical Activity & Health 2013.
9. Scheers, T., Philippaerts, R., Lefevre, J., Assessment Of Physical Activity And Inactivity In Multiple
Domains Of Daily Life: A Comparison Between A Computerized Questionnaire And The Sensewear Armband Complemented With An Electronic Diary. The International Journal Of Behavioral Nutrition And Physical
Activity 2012, 9:71.
10. Soo, K. L., Wan Abdul Manan, W. M., Wan Suriati, W. N., The Bahasa Melayu Version of the Global
Physical Activity Questionnaire: Reliability and Validity Study in Malaysia. Asia-Pacific Journal Of Public
Health 2012.
11. Chu, A. H., Moy, F. M., Reliability and Validity of the Malay International Physical Activity
Questionnaire (IPAQ-M) Among a Malay Population in Malaysia. Asia-Pacific Journal Of Public Health 2013.
12. Grimm, E. K., Swartz, A. M., Hart, T., Miller, N. E., Strath, S. J., Comparison Of The IPAQ-Short
Form And Accelerometry Predictions Of Physical Activity In Older Adults. Journal of Aging And Physical
Activity 2012, 20: p. 64-79.
13. Nicaise, V., Crespo, N. C., Marshall, S., Agreement Between The IPAQ And Accelerometer For
Detecting Intervention-Related Changes In Physical Activity In A Sample Of Latina Women. Journal Of Physical
Activity & Health 2014, 11: p. 846-852.
14. Curry, W. B., Thompson, J. L., Comparability Of Accelerometer- And IPAQ-Derived Physical Activity
And Sedentary Time In South Asian Women: A Cross-Sectional Study. European Journal Of Sport Science 2014:
p. 1-8.
15. Johannsen, D. L., M. A. Calabro, J. Stewart, W. Franke, J. C. Rood, and G. J. Welk, Accuracy of
Armband Monitors for Measuring Daily Energy Expenditure in Healthy Adults. Med Sci Sports Exercise
2010, 42: p. 2134–2140.
16. Bertheussen, G. F., Oldervoll, L., Kaasa, S., Sandmael, J. A., Helbostad, J. L., Measurement of
Cancer 2013, 21: p. 449-458.
17. Mynarski, W., Psurek, A., Borek, Z., Rozpara, M., Grabara, M., Strojek, K., Declared And Real
Physical Activity In Patients With Type 2 Diabetes Mellitus As Assessed By The International Physical Activity Questionnaire And Caltrac Accelerometer Monitor: A Potential Tool For Physical Activity Assessment In Patients With Type 2 Diabetes Mellitus. Diabetes Res Clin Pract 2012.
18. Tomioka, K., Iwamoto, J., Saeki, K., Okamoto, N., Reliability and validity of the International
Physical Activity Questionnaire (IPAQ) in elderly adults: the Fujiwara-kyo Study. Journal of Epidemiology /
Japan Epidemiological Association 2011, 21: p. 459-465.
19. Hoos, T., Espinoza, N., Marshall, S., Arredondo, E. M., Validity of the Global Physical Activity
Questionnaire (GPAQ) in adult Latinas. Journal of Physical Activity & Health 2012, 9: p. 698-705.
20. Au, T. B., Blizzard, L., Schmidt, M., Pham, L. H., Magnussen, C., Dwyer, T., Reliability and validity
of the global physical activity questionnaire in Vietnam. Journal of Physical Activity & Health 2010, 7: p.
410-418.
21. Trinh, O. T., Nguyen, N. D., van der Ploeg, H. P., Dibley, M. J., Bauman, A., Test-retest repeatability
and relative validity of the Global Physical Activity Questionnaire in a developing country context. Journal of
Physical Activity & Health 2009, 6 Suppl 1: p. 46-53.
22. Bull, F. C., Maslin, T. S., Armstrong, T., Global Physical Activity Questionnaire (GPAQ): nine
country reliability and validity study. Journal of Physical Activity & Health 2009, 6: p. 790-804.
23. Blikman, T., Stevens, M., Bulstra, S. K., Akker-Scheek, I. V., Reininga, I. H., Reliability and Validity
of the Dutch Version of the International Physical Activity Questionnaire (IPAQ) in Patients After Total Hip and Knee Arthroplasty. The Journal of Orthopaedic and Sports Physical Therapy 2013.
24. Chun M.Y., Validity and reliability of korean version of international physical activity questionnaire
short form in the elderly. Korean Journal Of Family Medicine 2012, 33: p. 144-151.
25. Cerin, E., Barnett, A., Cheung, M. C., Sit, C. H., Macfarlane, D. J., Chan, W. M., Reliability and
validity of the IPAQ-L in a sample of Hong Kong urban older adults: does neighborhood of residence matter?
Journal Of Aging And Physical Activity 2012, 20: p. 402-420.
26. Ottevaere, C., Huybrechts, I., De Bourdeaudhuij, I., Sjostrom, M., Ruiz, J. R., Ortega, F. B.,
Hagstromer, M., Widhalm, K., Molnar, D., Moreno, L. A., et al, Comparison of the IPAQ-A and actigraph in
relation to VO2max among European adolescents: the HELENA study. Journal Of Science And Medicine In
Sport 2011, 14: p. 317-324.
27. Nang, E. E., Gitau Ngunjiri, S. A., Wu, Y., Salim, A., Tai, E. S., Lee, J., Van Dam, R. M., Validity of
the International Physical Activity Questionnaire and the Singapore Prospective Study Program physical activity questionnaire in a multiethnic urban Asian population. BMC Medical Research Methodology 2011, 11:
p. 141.
28. Lee, P. H., Macfarlane, D. J., Lam, T. H., Stewart, S. M., Validity of the International Physical
Activity Questionnaire Short Form (IPAQ-SF): A Systematic Review. The International Journal Of Behavioral
Nutrition And Physical Activity 2011, 8: p. 115.
29. Criniere, L., Lhommet, C., Caille, A., Giraudeau, B., Lecomte, P., Couet, C., Oppert, J. M., Jacobi, D., Reproducibility And Validity Of The French Version Of The Long International Physical Activity
Questionnaire In Patients With Type 2 Diabetes. Journal Of Physical Activity & Health 2011, 8: p. 858-865.
30. Cerin, E., Barnett, A., Cheung, M. C., Sit, C. H., Macfarlane, D. J., Chan, W. M., Reliability and
validity of the International Physical Activity Questionnaire - Long Form in a sample of Hong Kong urban elders: does neighborhood of residence matter? Journal Of Aging And Physical Activity 2011.
31. Saglam, M., Arikan, H., Savci, S., Inal-Ince, D., Bosnak-Guclu, M., Karabulut, E., Tokgozoglu, L., International physical activity questionnaire: reliability and validity of the Turkish version. Perceptual And Motor Skills 2010, 111: p. 278-284.
32. Maddison, R., Ni Mhurchu, C., Jiang, Y., Vander Hoorn, S., Rodgers, A., Lawes, C. M., Rush, E.,
International Physical Activity Questionnaire (IPAQ) and New Zealand Physical Activity Questionnaire (NZPAQ): a doubly labelled water validation. The International Journal Of Behavioral Nutrition And Physical
Activity 2007, 4: p. 62.
33. Macfarlane, D. J., Lee, C. C., Ho, E. Y., Chan, K. L., Chan, D. T., Reliability and validity of the
Chinese version of IPAQ (short, last 7 days). Journal Of Science And Medicine In Sport 2007, 10: p. 45-51.
34. Craig, C. L., Marshall, A. L., Sjostrom, M., Bauman, A. E., Booth, M. L., Ainsworth, B. E., Pratt, M., Ekelund, U., Yngve, A., Sallis, J. F., Oja, P., International physical activity questionnaire: 12-country
35. Benitez-Porres, J., Delgado, M., Ruiz, J. R., Comparison of physical activity estimates using
International Physical Activity Questionnaire (IPAQ) and accelerometry in fibromyalgia patients: The Al-Andalus study. Journal Of Sports Sciences 2013.
36. Meeus, M., Van Eupen, I., Willems, J., Kos, D., Nijs, J., Is the International Physical Activity
Questionnaire-short form (IPAQ-SF) valid for assessing physical activity in Chronic Fatigue Syndrome?
Disability and rehabilitation 2011, 33: p. 9-16.
37. Hagstromer, M., Bergman, P., De Bourdeaudhuij, I., Ortega, F. B., Ruiz, J. R., Manios, Y., Rey-Lopez, J. P., Phillipp, K., von Berlepsch, J., Sjostrom, M., Concurrent validity of a modified version of the
International Physical Activity Questionnaire (IPAQ-A) in European adolescents: The HELENA Study. Int J
Obes 2008, 32 Suppl 5: p. 42-48.
38. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. http://www.who.int/chp/steps/ resources/GPAQ_Analysis_Guide.pdf. 2002. Accessed November 10, 2008.
39. IPAQ Research Committee. Guidelines for data processing and analysis of the International Physical
Activity Questionnaire (IPAQ)—Short and Long Forms. http://www.ipaq.ki.se/scoring.htm. Accessed August 25, 2011.
40. Oyeyemi, A. L., Oyeyemi, A. Y., Adegoke, B. O., Oyetoke, F. O., Aliyu, H. N., Aliyu, S. U., Rufai, A. A., The Short International Physical Activity Questionnaire: cross-cultural adaptation, validation and