International Journal of Medical Science and Current Research (IJMSCR)
Available online at: www.ijmscr.com
Volume2, Issue 3,Page No: 407-411
May-June 2019
407
Medicine ID-101739732
Correlation of Serum Vitamin D in Psoriasis in a Tertiary Care Hospital
1
Mohd Ramzan Bhatti, 2Shabnam Sarfraz, 3Majid Ali Sarfraz 1
MD Dermatology, Senior Resident, 2MD Pathology, Senior Resindent, 3Resident ENT, GMC Rajouri J&K
*Corresponding Author: Shabnam Sarfraz
MD Pathology, Senior Resindent GMC Rajouri J&K
Type of Publication: Original Research Paper Conflicts of Interest: Nil
ABSTRACT
Aims: To study relationship between vitamin D3 and Psoriasis. Material and Methods: Hospital based case control study with 20 patients of psoriasis and 20 age and sex matched control were undertaken. A detailed history was taken and examination including PASI was done. Other systemic involvement like psoriatic arthropathy, nail involvement was also noted. Results: Mean vitamin D3 level was not significantly different between psoriasis patients and controls. Mean vitamin D3 level in cases was 20.48 ± 8.51and that in controls was22.80 ± 9.46. However, vitamin D3 level were significantly lower in females as compared to males in both cases and controls Conclusion: In our study there is no correlation between vitamin D3 level and severity of psoriasis.
Keywords: Psoriasis, Vitamin D, Dermatologist.
INTRODUCTION
Psoriasis is chronic systemic immune mediated polygenic dermatological disorder [1] with a prevalence of 2-3% in general population worldwide [2]. Although cause of psoriasis remains idiopathic, there is increased evidence suggesting that psoriasis is a complex systemic disorder caused by interaction of multiple genes, environmental factors and immune system [3]. Low level of vitamin D is associated with development of some autoimmune diseases [4]. Vitamin D regulates both innate and adaptive immunity [5]. Vitamin D is important in proliferation and differentiation of keratinocytes. Recently the role of vitamin D in the pathogenesis of various skin diseases including psoriasis has been reported [6-8]. From many years vitamin D analogues are used for treatment of psoriasis. In this study we analyse possible correlation between vitamin D and psoriasis.
Materials and Methods
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
408
examination including type of lesions, extent of disease, body mass index (BMI), PASI of patient along with local examination of psoriatic plaque were undertaken. Estimation of serum vitamin D level were undertaken. Severity of PASI score was graded as mild, moderate and severe with scores of <5, 5-10, >10 respectively. Revised body mass index (BMI) for Asian Indian recommended by World Health Organisation (WHO). WHO was considered as reference value and interpreted as follows, <18.5- underweight, 18.5-23- Normal, 23-27.5- overweight, >27.5- obese. Deficiency, insufficiency and normal level of serum vit D was considered at level <20ng/ml, 20-30ng/ml and 30-100ng/ml respectively.
Results
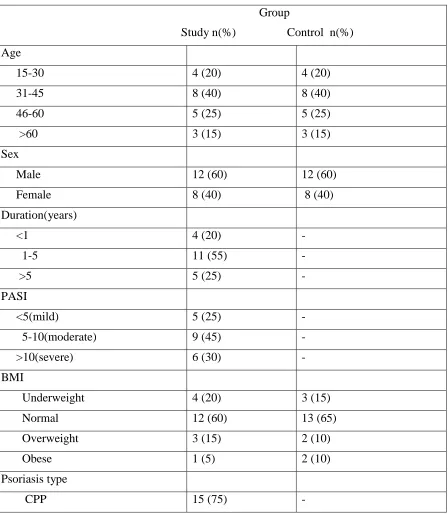
A total of 20 patients with psoriasis and 20 age and sex matched controls were included in this study. 12 were Male and 8 were female with Male: Female ratio of 3:2. Average age was 43.05 ±16.11 years in cases and 43.30±15.94 years in controls. Majority of psoriasis patients (65%) belongs to age group 31-60yrs. Table 1 showing demographic profile and clinical characteristics. Table 2 showing mean and standard deviation of various parameters in patients with and without psoriasis.
15 (75%) patients has psoriasis for <5 years duration whereas 5 (25%) has >5 years duration. The mean duration of psoriasis was 3.72 years. Out of 20 patients. 1(5%) patients had associated psoriatic arthropathy, 2(10%) had guttate psoriasis and 1(5%) patients had each Erythrodermic psoriasis and Pustular psoriasis. 1(5%) patient consume alcohol and 3(15%) patients smoke on regular basis. It was significantly less in control, only 2(10%) smoked and none was consuming alcohol. Among 20 patients with psoriasis 6(30%) has severe disease, 9(45%) has moderate disease. 5(25%) patients has mild disease. The mean PASI with psoriasis was 8.61. There was a/no significant association between duration of the disease and severity of psoriasis ( P = 0.001) In our study 90% of patients with psoriasis and 85% of patients without psoriasis had lower levels of Vitamin D. There is no significant difference seen in levels of
Vitamin D among cases and controls (P = 0.21). We
found that psoriasis patients with severe disease were among those with Vitamin D deficiency. However, it was not significant correlation between severity of
association was found between serum Vitamin D levels and duration of disease (P = 0.275).
Discussion
Psoriasis is a chronic systemic disorder that affects 2-3% 0f world population. Multiple factors are involved in pathogenesis of psoriasis. There are strong evidences that genetic factors play an important role in the development of psoriasis. In a north India study 9.8% of children had a family history of psoriasis [9]. Figure was as high as 28% in another study from Kuwait [10]. Psoriasis has been associated with many HLA haplotypes. It is a known fact that the genetic predisposition in psoriasis is vitamin D dependent if the genes have vitamin D receptor in their promoter region. In addition, vitamin D metabolism may be abnormal in psoriasis. Vitamin D was found to upregulate anti-inflammatory cytokine such as IL-10 and downregulate or inhibit proinflammatory cytokines such as IL-6 and TNF-α [11]. In psoriatic skin the cytokines IL-1, IL-6 and TNF-α are upregulated [1]. Vitamin D 3 and active metabolite of vitamin D is known to regulate both innate and adaptive immunity and also have a role of modulation of dendritic cell [3][4][12][13][14]. Activated T cells are believed to be the primary modulators in pathogenesis of psoriasis. Environment factors are involved in expression of disease. Several factors like physical trauma, psychological stress, drugs [15], and infections may trigger the disease in genetically predisposed individuals.
Hallmark of psoriasis are hyperproliferation and abnormal differentiation of epidermal keratinocyte, infiltration of T lymphocytes and various endothelial vascular changes in the dermal layer such as angiogenesis, dilatation and high endothelial venule (HEV) formation. In our study we observed that majority of population had low serum levels of vitamin D. Vitamin D deficient patients had severe form of the disease. However, a correlation couldn’t be established between the severity of disease and serum vitamin D levels. Various studies showing association/ no association between serum vitamin D levels and psoriasis are given in Table 3.
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
Pag
e
409
psoriasis. Vitamin D deficiency of 70-100% was observed in studies conducted in different parts of India in seemingly healthy individuals. Various factors have been observed in these patients such as low intake of vitamin D, insufficient sun exposure, vegetarian diet, high phytate/calcium ratio, genetic and epigenetic factors [16]. Thus, we observed that Indian population could have been adapted to the relatively low level of vitamin D and hence any
significance drawn from the above findings of low serum vitamin D levels may be erroneous. The limitation of this study includes small sample size which may not be the actual reflection of general population.
Conclusion
The severity of psoriasis did not correlate with vitamin D levels.
Table 1: Demographic and clinical characteristics
Group
Study n(%) Control n(%)
Age
15-30 4 (20) 4 (20)
31-45 8 (40) 8 (40)
46-60 5 (25) 5 (25)
>60 3 (15) 3 (15)
Sex
Male 12 (60) 12 (60)
Female 8 (40) 8 (40)
Duration(years)
<1 4 (20) -
1-5 11 (55) -
>5 5 (25) -
PASI
<5(mild) 5 (25) -
5-10(moderate) 9 (45) -
>10(severe) 6 (30) -
BMI
Underweight 4 (20) 3 (15)
Normal 12 (60) 13 (65)
Overweight 3 (15) 2 (10)
Obese 1 (5) 2 (10)
Psoriasis type
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
410
CPP+ psoriatic arthritis 1 (5) -
Guttate 2 (10) -
Erythroderma 1 (5) -
Pustular psoriasis 1 (5) -
Serum vitamin D
Deficient 12 (60) 10 (50)
Insufficient 6 (30) 7 (35)
Sufficient 2 (10) 3 (15)
CPP: Chronic plaque psoriasis, PASI: Psoriasis Area and Severity Index, BMI: Body mass index.
Table 2: Mean and standard deviation of various parameters in patients with and without psoriasis
Patients with Control without
Psoriasis psoriasis
Mean±SD Mean±SD
Age (years) 43.05 ± 16.11 43.30 ± 15.94
BMI (kg/m²) 21.03 ± 16.11 21.54 ± 3.40
PASI 8.61 ± 4.64 NA
Vitamin D (ng/ml) 20.48 ± 8.51 22.80 ± 9.46
PASI: Psoriasis Area and Severity Index, BMI: Body mass index.
Table 3: Studies showing association between vitamin D and psoriasis
Study by Place of study Cases (n) Control
(n)
Mean value (ng/ml) P
Chandrashekar et
al.17
Puducherry, India
43 43 Cases -13.3±6.9
Control-22.4±18.4 0.004
Al-Mutairi et al.18 Kuwait 100 100 Cases-31.5±14.41
Control-53.5±19.6 0.005
Atwa et al.11 Egypt 43 43 Cases-11.74±1.74
Control-24.55±9.3 0.000
Studies showing no association between vitamin D and psoriasis
Zuchi et al.19 Brazil 20 20 Cases-23.55±7.60
Control-22.35±3.10
0.735
Morimoto et al.20 Japan 34 24 Cases-22±7
Control-21±15
NS
Wilson 5 USA 148 5693 Cases-24.2±1.5
Control- 23.6±0.9
Pag e
411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
Pag e411
References1. Van de Kerkhof PC, Nestle FO. Psoriasis. In: Bolognia JL, editor. Dermatology. 3rd ed. Spain: Elsevier Ltd; 2012. P. 135-57.
2. Napolitano M, Caso F, Scarpa R, Megna M, Patri A, Balato N, Costa L. Psoriatic arthritis and psoriasis: differential diagnosis. Clin Rheumatol. 2016; 35(8): 1893-1901. doi: 10.1007/s10067-016-3295-9.
3. Suarez-Varela MM, Reguera-Leal P, Grant
WB, Rubio-Lopez N, Llopis-Gonzalez A. Vitamin D and psoriasis pathology in the Mediterranean region, Valencia (Spain). Int J Environ Res Public Health 2014; 11: 12108-17.
4. Grazio S, Nagli DB, Ani B, Grubisi F, Bobek
D,Bakula M, et al. Vitami D serum level, disease activity and functional ability in different rheumatic patients. Am J Med Sci 2015; 349: 46-9.
5. Wilson PB. Serum 25-hydroxy vitamin D
status in individuals with psoriasis in the general population. Endocrine 2013; 44: 537-9.
6. Mattozzi C, Paolino G, Richetta AG, Calvieri S. Psoriasis, Vitamin D and the importance of the cutaneous barrier’s integrity: an update. J Dermatol. 2016; 43(5): 507-514. Doi: 10.1111/1346-8138.13305.
7. Wadhwa B, Relhan V, Goel K, Kochhar AM,
Garg VK. Vitamin D and skin diseases: a review. Indian J Dermatol Venereol Leprol. 2015; 81(4): 344-355. doi: 10.4103/0378-6323.159928.
8. Soleymani T, Hung T, Soung J. The role of vitamin D in psoriasis: a review. Int J
Dermatol. 2015; 54(4): 383-392. doi:
10.1111/ijd.12790.
9. Nanda A, Kaur S, Kaur I, Kumar B.
Childhood psoriasis: an epidemiologic survey of 112 patients. Pediatr Dermatol 1990; 7: 19-21.
10. al-Fouzan AS, Nanda A. A survey of
childhood psoriasis in Kuwait. Pediatr Dermatol 1994; 11: 116-9.
11. Atwa MA, Balara MG, Hussein AM, Abdel Rahman NI, Elminshawy HH. Serum 25-hydroxy vitamin D concentration in patients with psoriasis and rheumatoid arthritis and its association with disease activity and serum tumor necrosis factor-α. Saudi Med J 2013; 34: 806-13.
12. Gisondi P, Rossini N, Di Cesare A, Idolazzi L, Farina S, Beltrami G et al. Vitamin D status in patients with chronic plaque psoriasis. Br J Dermatol 2012; 116: 505-10. 13. Kincse G, Bhattoa PH, Heredi E, Varga J,
Szegedi A, Keri J et al. Vitamin D3 levels and bone mineral density in patients with psoriasis and / or psoriatic arthritis. J Dermatol 2015; 42: 679-84.
14. Pavlov SI, Ivanova II, Gerova D. Vitamin D status in patients with psoriasis. Scr Sci Med 2016; 8: 50-4.
15. Basavaraj KH, Ashok NM, Rashmi R,
Praveen TK. The role of drugs in the induction and / or exacerbation of psoriasis. Int J Dermatol 2010; 49: 1351-61.
16. G R, Gupta A. Vitamin D deficiency in India: Prevalance, casualities and interventions. Nutrients 2014; 6: 729-75.
17. Chandrashekar L, Kumarit GR, Rajappa M,
Revathy G, Munisamy M, Thappa DM, et al.
25- hydroxy vitamin D and ischaemia- modified albumin levels in psoriasis and their association with disease severity. Br J Biomed Sci 2015; 72: 56-60.
18. Al-Mutairi N, El Eassa B, Nair V.
Measurement of vitamin D and cathelicidin (LL-37) levels in patients of psoriasis with co-morbidities. Indian J Dermatol Venereol Leprol 2013; 79: 492-6.
19. Zuchi MF, Azevedo PO, Tanaka AA,
Schmitt JV, Martins LE. Serum levels of 25-hydroxy vitamin D in psoriatic patients. An Bras Dermatol 2015; 90: 430-2.
20.Morimoto S, Yoshikawa K, Fukuo K,