A Multicenter Collaborative Approach to Reducing
Pediatric Codes Outside the ICU
abstract
OBJECTIVES: The Child Health Corporation of America formed a mul-ticenter collaborative to decrease the rate of pediatric codes outside the ICU by 50%, double the days between these events, and improve the patient safety culture scores by 5 percentage points.
METHODS: A multidisciplinary pediatric advisory panel developed a comprehensive change package of process improvement strategies and measures for tracking progress. Learning sessions, conference calls, and data submission facilitated collaborative group learning and implementation. Twenty Child Health Corporation of America pitals participated in this 12-month improvement project. Each hos-pital identified at least 1 noncritical care target unit in which to implement selected elements of the change package. Strategies to improve prevention, detection, and correction of the deteriorating patient ranged from relatively simple, foundational changes to more complex, advanced changes. Each hospital selected a broad range of change package elements for implementation using rapid-cycle methodologies. The primary outcome measure was reduction in codes per 1000 patient days. Secondary outcomes were days between codes and change in patient safety culture scores.
RESULTS:Code rate for the collaborative did not decrease significantly (3% decrease). Twelve hospitals reported additional data after the col-laborative and saw significant improvement in code rates (24% de-crease). Patient safety culture scores improved by 4.5% to 8.5%.
CONCLUSIONS: A complex process, such as patient deterioration, requires sufficient time and effort to achieve improved outcomes and create a deeply embedded culture of patient safety. The collaborative model can accelerate improvements achieved by individual institutions.
Pediatrics2012;129:e785–e791
AUTHORS:Leslie W. Hayes, MD,aEmily L. Dobyns, MD, FCCM,bBruno DiGiovine, MD, MPH,cAnn-Marie Brown, MSN, CPNP-AC/PC, CCRN,dSharon Jacobson, MBA, BSN, RN, CPHQ,eKelly H. Randall, MSW, LGSW, CPHQ,aBeth Wathen, MSN, CCRN,bCarolyn Schwab, RN, BSN, MA, CNAA,fKathy D. Duncan, RN,gJodi Thrasher, RN, MS, FNP-BC,bTina R. Logsdon, MS,hMatthew Hall, PhD,hand Barry Markovitz, MD, MPHi
aDepartment of Pediatrics, Children’s Hospital of Alabama, University of Alabama, Birmingham, Alabama;bDepartment of Pediatrics, Children’s Hospital Denver, Aurora, Colorado;cQuality Department, Wayne State University, Detroit, Michigan;dCritical Care, Akron Children’s Hospital, Akron, Ohio;eQuality Department, Texas Children’s Hospital, Texas Medical Center, Houston, Texas; fClinical Operations, Children’s Healthcare of Atlanta, Atlanta, Georgia;gInstitute for Healthcare Improvement;hChild Health Corporation of America, Shawnee Mission, Kansas; and iDepartment of Pediatrics, Children’s Hospital Los Angeles, Los Angeles, California
KEY WORDS
quality improvement, collaboration, outcomes research
ABBREVIATIONS
AHRQ HSOPS—Agency for Healthcare Research and Quality’s Hos-pital Survey on Patient Safety Culture
CHCA—Child Health Corporation of America CI—confidence interval
MET—medical emergency team RRT—rapid response teams
www.pediatrics.org/cgi/doi/10.1542/peds.2011-0227
doi:10.1542/peds.2011-0227
Accepted for publication Oct 10, 2011
Address correspondence to Leslie W. Hayes, MD, Children’s Hospital of Alabama, 1600 7th Ave South, ACC Suite 504, Birmingham, AL 35233. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
individual institutions, is a significant public health care issue. Analysis of data collected by the Child Health Cor-poration of America (CHCA, Shawnee Mission, KS) from 2003 to 2006 revealed events involving “failed escalation of care” accounted for 16% of all events reported by the 19 contributing hospi-tals (Children’s Hospitals Advancing Patient Safety, unpublished shared sentinel event database, 2003-2006).1 Although infrequent in pediatric in-patients, cardiopulmonary arrest re-quiring cardiac compressions for pulselessness has a survival rate of only 27%; survival increases to 80% if patient deterioration is recognized earlier. Addi-tional analysis of event characteristics uncovered missed opportunities to rec-ognize and intervene before cardiopul-monary arrest. These data together with published research demonstrating that adult patients experience signs of de-terioration hours before they arrest1,2 suggest that recognizing deterioration earlier in a patient’s hospital course could reduce the frequency of codes and improve outcomes.
Two recent important strategies to prevent codes have been the use of early warning systems (or in pediatrics, pe-diatric early warning systems) and the development of rapid response teams (RRTs; also called medical emergency teams [MET]). Early warning systems are intended to improve recognition of patient deterioration with the use of an easily applied scoring system to more objectively identify changes in patient status.3–6 RRTs first emerged in the early 1990s in Australia and typically comprise ICU physicians, nurses, and respiratory therapists who bring criti-cal care expertise to the bedside of a patient in a general care unit.
In addition to effective clinical inter-ventions, understanding factors infl u-encing an organization’s patient safety
reliability industries, such as aviation, shows an association between a posi-tive safety culture and reduced errors.8 The Agency for Healthcare Research and Quality’s Hospital Survey on Patient Safety Culture (AHRQ HSOPS)9assesses hospital staff perception of patient safety issues, medical error, and event reporting. In 2007, the lowest positive response categories within pediatric units were “Nonpunitive Response to Error” (43% positive responses) and
“Handoffs and Transitions”(45% posi-tive responses),10highlighting the need for improvement in these areas.
This report describes CHCA’s multidis-ciplinary improvement collaborative of 20 children’s hospitals, which imple-mented a suite of prevention, detection, and correction strategies on targeted inpatient units with the stated aim of reducing the number of inpatient pe-diatric cardiopulmonary arrests (re-ferred to in this article as codes) by 50% and improving the culture of pa-tient safety scores by 5 percentage points in each of 3 key domains (Non-punitive Response to Error, Handoffs and Transitions, and Communication Openness, chosen as a third category that bestfit with our change package).
METHODS Study Population
Twenty CHCA hospitals participated in a 12-month improvement project to
“eliminate codes and associated mor-tality on inpatient units”(Group A). This collaborative was offered to all 42 CHCA owner hospitals. Each participating hospital determined if internal review board assessment was necessary and, if appropriate, obtained local approval or waiver before project initiation. The purpose of this collaborative was to es-tablish reliable systems that rescue the deteriorating patient, focusing on 3 key change areas: prevention, detection, and
collaborative. Each hospital assembled a multidisciplinary team with designated administrative and/or physician spon-sors. Each team identified“target”units (typically 1–3 units per hospital) from among noncritical care inpatient units, emergency department/emergency de-partments, operating rooms, and ICUs. Four hospitals focused on all noncritical care units during the project.
Collaborative Process
Collaborative Development
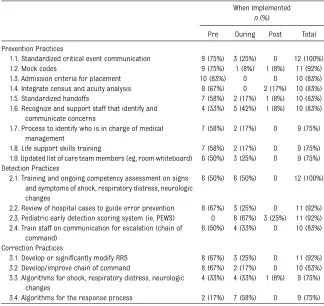
The collaborative was designed by a multidisciplinary pediatric advisory panel, including participating hospital staff and external subject matter experts. A comprehensive, pediatric-specific change package of practices with evidence supporting their efficacy, low risk of harm, and feasibility of implementation and measurement was developed. The interventions focused on change in practice to improve pre-vention, detection, and intervention of the deteriorating patient (Table 1). Three categories of changes with in-creasing complexity were identified. Foundational changes were relatively simple to implement and recom-mended to be put into practice early in the collaborative (eg, implementing
“SBAR,” or Situation, Background, As-sessment, Recommendation). Midlevel changes, such as developing a RRT, were implemented as the foundational changes were accomplished. Advanced changes (eg, family activation of the RRT) were considered more complex and were generally implemented once several other change types had been achieved. Teams were instructed to select a broad range of change pack-age elements for implementation.
Approach and Organization of the Collaborative
emphasizes small tests of change (Plan-Do-Study-Act), as developed by Asso-ciates in Process Improvement and adopted by the Institute for Healthcare Improvement.11 The process included a well-defined aims statement, 3 face-to-face learning sessions, communica-tion strategies (eg, monthly conference calls, collaborative listserv, and project Web page), and monthly data submis-sion. Hospitals were free to apply ad-ditional improvement methods used in their facilities, such as Six Sigma.12 On a monthly basis, participants re-ported their project measures to CHCA through a secure Web-based data re-pository hosted by Institute for Health-care Improvement.
The aims of the collaborative were to reduce the rate of codes by 50%, double the days between codes, and improve the patient safety culture scores by 5 percentage points in the target units.
The primary outcome measure was reduction in codes per 1000 patient days, with the secondary outcomes being the days between codes and change in patient safety culture scores (see Supplemental Information). Three process measures were also collected: RRT response time compliance, RRT activations per 1000 patient days, and RRT activation before a code. A goal of 95% compliance with RRT response time compliance was established. Each hospital set its own expected response time, typically 15 minutes.
Data Reporting to the Collaborative
Hospitals agreed to collect and submit monthly data during the study period of July 1, 2007 through June 30, 2008. Additionally, baseline data from the preceding 12 months (July 1, 2006–June 30, 2007) regarding codes and un-planned transfers to a higher level of
care and from the preceding 3 months (April 1, 2007–June 30, 2007) for the process measures were collected from each hospital as baseline. Approximately 18 months after the collaborative ac-tion period concluded, a postcolla-borative survey was conducted to collect an additional 12 months of code data. Twelve of the original 20 hospitals submitted postcollaborative data (Group B). Definitions of a“code” and an“unplanned transfer”were not standardized across institutions; each institution used their existing defi -nitions throughout the data collection period.
Patient safety culture was measured via the AHRQ HSOPS and focused on 3 domains: (1) communication openness, (2) handoffs and transitions, and (3) nonpunitive response to error. The survey was conducted 3 times during the project: at the beginning of the project, midproject, and at the conclu-sion of the action period. Although only 3 domains were analyzed for the collab-orative, teams were instructed to con-duct the entire survey to minimize potential bias.
Statistical Methods
Data are expressed as median with interquartile ranges and 95% confidence intervals. Mann-Whitney was used for nonparametric tests with an exactP,
.05 considered statistically significant. Pairedttest was used for AHRQ survey data, with an exactP,.05 considered statistically significant. Analyses were performed utilizing Minitab version 15 (Minitab, State College, PA).
RESULTS
Before joining the project, hospitals’ efforts related to patient deterioration focused primarily on various preven-tive practices, review of hospital cases, staff training, RRT, and improvement in the chain of command process (Table 1).
TABLE 1 Most Commonly Implemented Practices Collected via Postcollaborative Survey When Implemented
n(%)
Pre During Post Total
Prevention Practices
1.1. Standardized critical event communication 9 (75%) 3 (25%) 0 12 (100%) 1.2. Mock codes 9 (75%) 1 (8%) 1 (8%) 11 (92%) 1.3. Admission criteria for placement 10 (83%) 0 0 10 (83%) 1.4. Integrate census and acuity analysis 8 (67%) 0 2 (17%) 10 (83%) 1.5. Standardized handoffs 7 (58%) 2 (17%) 1 (8%) 10 (83%) 1.6. Recognize and support staff that identify and
communicate concerns
4 (33%) 5 (42%) 1 (8%) 10 (83%)
1.7. Process to identify who is in charge of medical management
7 (58%) 2 (17%) 0 9 (75%)
1.8. Life support skills training 7 (58%) 2 (17%) 0 9 (75%) 1.9. Updated list of care team members (eg, room whiteboard) 6 (50%) 3 (25%) 0 9 (75%) Detection Practices
2.1. Training and ongoing competency assessment on signs and symptoms of shock, respiratory distress, neurologic changes
6 (50%) 6 (50%) 0 12 (100%)
2.2. Review of hospital cases to guide error prevention 8 (67%) 3 (25%) 0 11 (92%) 2.3. Pediatric early detection scoring system (ie, PEWS) 0 8 (67%) 3 (25%) 11 (92%) 2.4. Train staff on communication for escalation (chain of
command)
6 (50%) 4 (33%) 0 10 (83%)
Correction Practices
3.1. Develop or significantly modify RRS 8 (67%) 3 (25%) 0 11 (92%) 3.2. Develop/improve chain of command 8 (67%) 2 (17%) 0 10 (83%) 3.3. Algorithms for shock, respiratory distress, neurologic
changes
4 (33%) 4 (33%) 1 (8%) 9 (75%)
3.4. Algorithms for the response process 2 (17%) 7 (58%) 0 9 (75%)
Table includes only practices implemented in at least 75% of responding hospitals (change package included 15 prevention, 9 detection, and 5 correction practices).n= 12 of 20 participating hospitals; PEWS, Pediatric Early Warning System.
were in the use of staff training and competency in recognition of deterio-ration and response algorithms. The most dramatic change implemented was the use of pediatric early warning system, starting out in no hospitals and implemented in 92% of hospitals within 12 months of the end of the collaborative period. Table 1 describes when practices were initially imple-mented; many practices that were in place before the collaborative began
lished mock code processes.
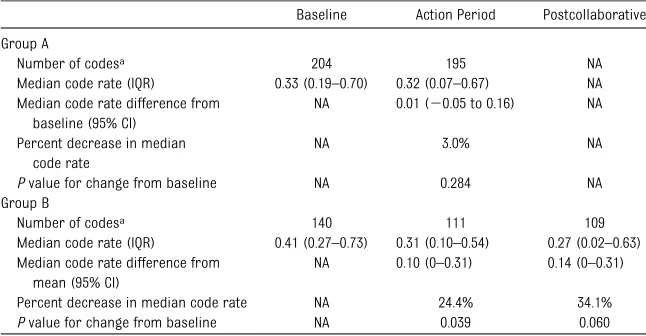
The primary outcome measure was reduction in codes outside the ICU per 1000 patient days. The change in median code rate did not reach statistical sig-nificance for Group (difference in rate 0.01, 95% confidence interval [CI]: – 0.05, 0.16, P= .284; Fig 1, Table 2). For Group B, the decrease in median code rate was statistically significant from baseline performance to action period performance (difference in rate 0.10,
median code rate than the 8 teams not reporting postcollaborative data, although this did not reach statistical significance (P= .066); Group B also had a lower pooled median code rate during the action period, although this again did not reach statistical signifi -cance (P= .399).
Although 75% of the hospitals in each of these groups began the collaborative with an existing RRT, there were dif-ferences noted between Groups A and B in RRT implementation during the project. In Group B, 100% had a RRT in place by the end of the action period. At the conclusion of the action period in the group of 8 hospitals not report-ing postcollaborative data, no addi-tional hospitals had implemented a RRT.
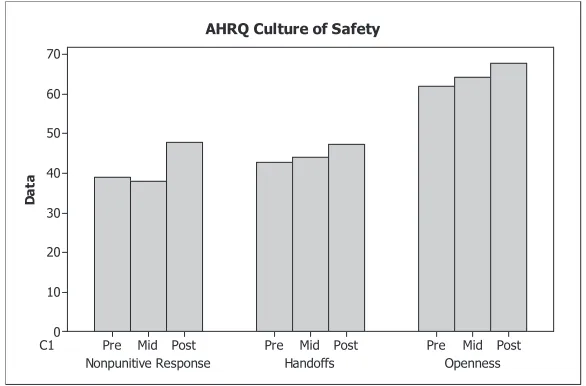
Patient safety culture scores improved in all 3 targeted domains of the AHRQ HSOPS for the 14 hospitals (70%) that conducted the survey (Fig 3). When comparing the baseline andfinal sur-veys, the domains improved between 4.5 and 8.5 percentage points compared with the collaborative goal of 5 per-centage points. The only statistically significant improvement was seen in
“nonpunitive response to error” (39% positive response baseline, 47% positive response postcollaborative,P= .02). The remainder of the survey improvements were not statistically significant.
DISCUSSION
Our report of this multicenter collab-orative process improvement initiative to reduce codes demonstrates mixed results and failed to achieve the a priori goal of a 50% reduction in codes after 1 year. Across all 20 hos-pitals, a modest 3% decrease in the median code rate was realized dur-ing the 1-year implementation period (Table 2). Interestingly, the variabil-ity of the code rates across the
FIGURE 1
Median code rate over time for all 20 hospitals (Group A). UCL, upper control limit; LCL, lower control limit.
TABLE 2 Code Numbers, Medians, and Interquartile Ranges
Baseline Action Period Postcollaborative
Group A
Number of codesa 204 195 NA
Median code rate (IQR) 0.33 (0.19–0.70) 0.32 (0.07–0.67) NA Median code rate difference from
baseline (95% CI)
NA 0.01 (20.05 to 0.16) NA
Percent decrease in median code rate
NA 3.0% NA
Pvalue for change from baseline NA 0.284 NA Group B
Number of codesa 140 111 109
Median code rate (IQR) 0.41 (0.27–0.73) 0.31 (0.10–0.54) 0.27 (0.02–0.63) Median code rate difference from
mean (95% CI)
NA 0.10 (0–0.31) 0.14 (0–0.31)
Percent decrease in median code rate NA 24.4% 34.1%
Pvalue for change from baseline NA 0.039 0.060
IQR, interquartile ranges; NA, not applicable.
aSample sizes varied by hospital because of differences in hospital sizes and the number of targeted beds in the hospital;
collaborative dramatically increased during the action period, suggesting that some institutions saw meaningful improvements but others did not. In an effort to explore this variability and obtain follow-up data, Group B was evaluated separately, and its median code rate declined by 24.4% (inter-quartile range: 0.10–0.54; P = .04) during the action period and 34.1% from baseline (interquartile range: 0.02–0.63;P= .06) during the following year.
Convincing data exist that survival to discharge for inpatient codes is dis-mal.13 It seems nearly as convincing that the rates of such events can be reduced, and the most dramatic evi-dence has been published in the con-text of RRT implementation in several children’s hospitals. The inpatient code rate declined by 59% (0.27–0.11 per 1000 patient days) at Cincinnati Child-ren’s Hospital Medical Center after implementation of a medical emergency team.14 At Lucile Packard Children’s
Hospital, a 71.7% reduction in code rate was realized following RRT imple-mentation; this was accompanied by an 18% reduction in hospital-wide mortality.15 At the Royal Children’s Hospital in Melbourne, Australia, the inpatient“preventable”code rate also declined by 65%, accompanied by a dramatic 45% drop in total hospital mortality, after implementation of a MET.16
The variability of our results is pre-dictable for several reasons. First, each hospital was starting from a different place along a continuum of existing systems, and each then implemented different elements of the change package to varying degrees. In addition, each hospital used their own internal definition of a “code”; depending on the definition, some may have been more preventable than others. The interventions employed were process improvement/systems changes and were likely implemented with varying levels of zeal and acceptance at dif-ferent institutions. Indeed, the collab-orative monthly progress reports ranged from the equivalent of barely getting started to successful comple-tion of all the institucomple-tion’s goals and objectives. Tempting as it may be to try to correlate institutional progress with the collaborative change package imple-mentation success and outcomes (ie, change in code rates), the variability across institutions was too great to perform such analysis. Likely attribut-able to each institution’s own change in safety culture during the period of anal-ysis, no consistent pattern of change package implementation was seen in either the top- or bottom-performing hospitals. Certainly significant changes were seen in 1 of the AHRQ survey ques-tions targeted for improvement during this collaborative, whereas the other 2 domains trended toward improvement. This represents important improvement in a relatively short time frame.
FIGURE 2
Median Code rate over time for Group B. UCL, upper control limit; LCL, lower control limit.
FIGURE 3
AHRQ Patient Safety Scores for the 3 target domains, Precollaborative, Midcollaborative, and Post-collaborative.
strated meaningful results for focused interventions. Pronovost et al demon-strated near elimination of catheter-associated bloodstream infections across 108 ICUs in Michigan.17Miller et al showed a 43% reduction in catheter-associated bloodstream infections in a 29 PICU collaborative.18 Similarly, Wirtschafter et al were able to reduce central line–associated bloodstream infections by 25% across 13 neonatal ICUs.19 In addition, CHCA has a track record of successful multicenter pro-cess improvement collaboratives, demonstrating reduction in catheter-associated bloodstream infections in 26 PICUs20and narcotic-related adverse drug events across 14 hospitals.21 As complex and difficult to eradicate as these infections and adverse drug events have been, the pathophysiology and the implementation strategies involved in these collaboratives were relatively straightforward. Without intent to diminish the tremendous results, all involved“bundles” of be-haviors, short checklists, or discrete process improvements to reduce the risk of infections or errors. Assuming compliance with these behaviors can be monitored and enforced, particu-larly during the active study phase, the results can be observed in a short time frame.
Preventing codes, in comparison, is far more complicated, and our change package introduced interventions that represent upheavals in care para-digms. Indeed, some of these care paradigm changes are truly cultural shifts. A nurse“going over the head”of a resident who is not responding to a deteriorating patient properly and calling the attending or activating an RRT on his or her own is an example of cultural shift. When residents ac-knowledge they need help in the middle of the night and call the attending for
field, particularly health care, takes time and a concerted and consistent focus. The implementation of a new, multifactorial way of monitoring patients cannot possibly be performed consis-tently and effectively in a short time frame, even for 1 institution, not to mention 12 or 20.
As noted earlier, the 1 systems change process that has, at least in before and after retrospective studies, been shown to reduce codes is the RRT. Of more than passing interest, then, must be the recognition that 75% of our partici-pating institutions reported an RRT in place at the beginning of the collabo-rative. Depending on how effective such implementations were at each center, it is possible that little additional“ code-reducing”behaviors could be exacted from these hospitals. On the other hand, just having an RRT in place does not mean it is being used effectively. The 1 cluster randomized controlled trial of an MET (in adults) was unable to show a crude difference in code rates between hospitals randomized to develop a MET and those without one.22However, when data from this study were retrospectively analyzed, it was clear that as the number of MET calls increased, inpatient code rates decreased.23Many hospitals assigned to implement a MET simply were not calling the team as often as necessary.
Allowing extrapolation from the median code rate change from the group of 12 hospitals during the postcollaborative period, for a hypothetical average-sized children’s hospital with 225 licensed beds and 50 000 patient days per year, this would represent 7 to 8 codes averted annually. If the mortality rate after inpatient pediatric codes is
∼75%,1 then 5 to 6 fewer deaths per year might be expected for such an in-stitution. Of course, this is speculative but entirely consistent with the existing
Measuring 1 aspect of patient safety culture, the improvement seen in the AHRQ HSOPS was modest but in most domains met the goal of 5 percentage point increase recommended by AHRQ. A culture of patient safety has been clearly linked to improved patient out-comes including recently in the highest risk environment of the ICU. For each 10% reduction in “ICU perceptions of management” percent-positive score, the odds ratio for hospital mortality was 1.24 (95% CI: 1.07–1.44; P= .005) across 30 adult ICUs.24
Our time frame merits discussion in reference to changing patient safety culture, because sufficient time must be allowed to enable deeply embedded culture to change. There is evidence to support this notion with regard to the effects of the RRT. Santamaria et al report on code rates at a single stitution up to 4 years after MET in-troduction.25Their code rates did not drop significantly (45%) until 2 years after MET implementation but then declined an additional 42% after 2 more years. This may explain the results of our collaborative for the 12 hospitals that submitted data for an additional year. Of course, it may also be that these hospitals were funda-mentally different in their ability to implement elements of our change package successfully; being interested and able to submit data 1 year later may be evidence of such a commitment.
studies of new medications and expen-sive devices.
Certainly included in the role of health care providers is the goal of continually improving the care we provide our patients. The ultimate goal is preventing
errors, such as “failed escalation of care.”A multifactorial process, such as codes after patient deterioration, likely requires a multidimensional approach to prevention. Changing patient safety culture is an ongoing process that is
closely tied to improved patient out-comes. Not only is measuring changes in rates of relatively rare events chal-lenging, maintaining sustained control of such improvements requires con-tinual attention.
REFERENCES
1. Nadkarni VM, Larkin GL, Peberdy MA, et al; National Registry of Cardiopulmonary Re-suscitation Investigators. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults.JAMA. 2006;295(1):50–57 2. Reis AG, Nadkarni V, Perondi MB, Grisi S,
Berg RA. A prospective investigation into the epidemiology of in-hospital pediatric cardiopulmonary resuscitation using the international Utstein reporting style. Pedi-atrics. 2002;109(2):200–209
3. Duncan H, Hutchison J, Parshuram CS. The Pediatric Early Warning System score: a severity of illness score to predict urgent medical need in hospitalized children.
J Crit Care. 2006;21(3):271–278
4. Sharpley JT, Holden JC. Introducing an early warning scoring system in a district general hospital.Nurs Crit Care. 2004;9(3):98–103 5. Hodgetts TJ, Kenward G, Vlachonikolis IG,
Payne S, Castle N. The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team.Resuscitation. 2002;54(2): 125–131
6. Buist M, Bernard S, Nguyen TV, Moore G, Anderson J. Association between clinically abnormal observations and subsequent in-hospital mortality: a prospective study.
Resuscitation. 2004;62(2):137–141 7. Grant MJ, Donaldson AE, Larsen GY. The
safety culture in a children’s hospital.
J Nurs Care Qual. 2006;21(3):223–229 8. Pronovost PJ, Weast B, Holzmueller CG,
et al. Evaluation of the culture of safety: survey of clinicians and managers in an academic medical center.Qual Saf Health Care. 2003;12(6):405–410
9. AHRQ. Surveys on Patient Safety Culture. Available at: www.ahrq.gov/qual/patient-safetyculture. Accessed January 6, 2012
10. AHRQ Hospital Survey on Patient Safety Culture. 2007 Comparative Database Report. Available at: www.ahrq.gov/qual/hospsurveydb/ hospsurveydb1.pdf. Accessed January 6, 2012 11. Institute For Healthcare Improvement. How to improve. Available at: www.ihi. org/knowledge/Pages/HowtoImprove/default. a s p x“www.ihi.org/kno w le d ge /Pa ge s/ HowtoImprove/default.aspx Accessed January 6, 2012
12. Schoeder RG. 2000. Six Sigma quality im-provement: what is Six Sigma and what are the important implications? In: Proceedings of the Fourth Annual International POMS Con-ference; August 27–September 1; Seville, Spain 13. Donoghue AJ, Nadkarni VM, Elliott M, Durbin D; American Heart Assocation National Registry of Cardiopulmonary Resuscitation Investigators. Effect of hospital character-istics on outcomes from pediatric cardio-pulmonary resuscitation: a report from the national registry of cardiopulmonary re-suscitation.Pediatrics. 2006;118(3):995–1001 14. Brilli RJ, Gibson R, Luria JW, et al. Imple-mentation of a medical emergency team in a large pediatric teaching hospital prevents respiratory and cardiopulmonary arrests outside the intensive care unit.Pediatr Crit Care Med. 2007;8(3):236–246, quiz 247 15. Sharek PJ, Parast LM, Leong K, et al. Effect
of a rapid response team on hospital-wide mortality and code rates outside the ICU in a children’s hospital. JAMA. 2007;298(19): 2267–2274
16. Tibballs J, Kinney S. Reduction of hospital mortality and of preventable cardiac arrest and death on introduction of a pediatric medical emergency team.Pediatr Crit Care Med. 2009;10(3):306–312
17. Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU.
N Engl J Med. 2006;355(26):2725–2732
18. Miller MR, Griswold M, Harris JM II, et al. De-creasing PICU catheter-associated bloodstream infections: NACHRI’s quality transforma-tion efforts. Pediatrics. 2010;125(2):206– 213
19. Wirtschafter DD, Pettit J, Kurtin P, et al. A statewide quality improvement collaborative to reduce neonatal central line-associated blood stream infections.J Perinatol. 2010; 30(3):170–181
20. Jeffries HE, Mason W, Brewer M, et al. Prevention of central venous catheter-associated bloodstream infections in pedi-atric intensive care units: a performance improvement collaborative. Infect Control Hosp Epidemiol. 2009;30(7):645–651 21. Sharek PJ, McClead RE, Jr;Taketomo C,
et al. An intervention to decrease narcotic-related adverse drug events in children’s hospitals.Pediatrics. 2008;122(4). Available at: www.pediatrics.org/cgi/content/full/122/4/e861 22. Hillman K, Chen J, Cretikos M, et al; MERIT study investigators. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lan-cet. 2005;365(9477):2091–2097
23. Chen J, Bellomo R, Flabouris A, Hillman K, Finfer S; MERIT Study Investigators for the Simpson Centre; ; ANZICS Clinical Trials Group. The relationship between early emergency team calls and serious ad-verse events. Crit Care Med. 2009;37(1): 148–153
24. Huang DT, Clermont G, Kong L, et al. In-tensive care unit safety culture and out-comes: a US multicenter study.Int J Qual Health Care. 2010;22(3):151–161
25. Santamaria J, Tobin A, Holmes J. Changing cardiac arrest and hospital mortality rates through a medical emergency team takes time and constant review. Crit Care Med. 2010;38(2):445–450
DOI: 10.1542/peds.2011-0227 originally published online February 20, 2012;
2012;129;e785
Pediatrics
Thrasher, Tina R. Logsdon, Matthew Hall and Barry Markovitz
Jacobson, Kelly H. Randall, Beth Wathen, Carolyn Schwab, Kathy D. Duncan, Jodi
Leslie W. Hayes, Emily L. Dobyns, Bruno DiGiovine, Ann-Marie Brown, Sharon
Services
Updated Information &
http://pediatrics.aappublications.org/content/129/3/e785 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/129/3/e785#BIBL This article cites 21 articles, 5 of which you can access for free at:
Subspecialty Collections
e_management_sub
http://www.aappublications.org/cgi/collection/administration:practic Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2011-0227 originally published online February 20, 2012;
2012;129;e785
Pediatrics
Thrasher, Tina R. Logsdon, Matthew Hall and Barry Markovitz
Jacobson, Kelly H. Randall, Beth Wathen, Carolyn Schwab, Kathy D. Duncan, Jodi
Leslie W. Hayes, Emily L. Dobyns, Bruno DiGiovine, Ann-Marie Brown, Sharon
ICU
A Multicenter Collaborative Approach to Reducing Pediatric Codes Outside the
http://pediatrics.aappublications.org/content/129/3/e785
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2012/02/15/peds.2011-0227.DCSupplemental Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.