Outcome at 5 Years of Age of Children 23 to 27 Weeks’ Gestation:
Refining the Prognosis
Lex W. Doyle, MD, FRACP, for the Victorian Infant Collaborative Study Groupa
ABSTRACT. Objectives. To determine the changes with postnatal age for survival, with and without major sensorineural disability, to 5 years of age in very preterm infants and to contrast their prognosis with normal birth weight (NBW) control participants.
Methods. A geographically determined cohort study was conducted in Victoria, Australia. Consecutive live births of 23 to 27 weeks’ gestational age born during 1991 to 1992 and randomly selected contemporaneous NBW control participants were studied. The main outcome measures were survival and rates of major disability at 5 years of age, determined for those offered intensive care, after day 7, after day 28, and at hospital discharge.
Results. Of 401 live births of 23 to 27 weeks’ gesta-tion, 225 (56.1%) survived to 5 years of age. The survival rate rose significantly with increasing gestational age at birth in those offered intensive care and by day 7 but not by day 28. The survival rate free of major disability rose significantly with increasing gestational age at all post-natal ages but was not an independent predictive vari-able by day 28; other adverse events were more impor-tant. In the absence of adverse events, the rate of survival free of major disability for very preterm infants who had survived to discharge was 93.2%, similar to the rate of 95.5% for NBW control participants.
Conclusions. The prognosis for very preterm infants changes substantially with postnatal age. Counseling of families should be repeated at intervals, and the advice offered should vary with perinatal events. Pediatrics 2001;108:134 –141;preterm infant, survival, disability.
ABBREVIATIONS. NBW, normal birth weight; SGA, small for gestational age; LGA, large for gestational age; CVH, cerebroven-tricular hemorrhage; PVL, perivencerebroven-tricular leukomalacia; BPD, bronchopulmonary dysplasia; WPPSI-R, Wechsler Preschool and Primary Scale of Intelligence–Revised; CI, confidence interval; OR odds ratio.
W
hen parents are counseled about the out-come for very preterm children, they want to know not only whether their child will survive but also whether their child will survive with or without a major sensorineural disability. The prognosis varies between regions1–10and withinre-gions,11reflecting, in part, different attitudes toward
treatment. Counseling of parents has to reflect these regional differences. Certain variables associated with adverse outcome, diagnosed at varying times, also will influence the prognostication. However, ex-actly how perinatal events, including attitudes to-ward treatment, interact to influence the prognosis for very preterm infants is not well described. More-over, to know whether rates of problems are exces-sive or not, the outcome for very preterm children has to be described relative to that for nonpreterm or normal birth weight (NBW) control participants.
The aim of this study was to determine the changes in prognosis with perinatal events, includ-ing postnatal age, for survival and for survival with and without major sensorineural disability at 5 years of age in very preterm infants 23 to 27 weeks’ gesta-tional age and to contrast their prognosis with NBW control participants.
METHODS
The very preterm cohort comprised 401 consecutive live-born children at 23 to 27 completed weeks of gestational age in the 2-year period from January 1, 1991, in Victoria, Australia. There were no survivors born before 23 weeks of gestational age during this period. Gestational age was calculated from dates obtained by menstrual history, usually confirmed by ultrasound before 20 weeks’ gestation. Details of the multiple data sources used to determine survival were reported previously.12
For children who were born outside level III perinatal centers and not transferred after birth, only limited perinatal data (place of birth, mode of delivery, gestational age, and birth weight) were obtained. For the remaining children, more extensive perinatal data were recorded.5However, data on many perinatal variables
still were lacking for those who were born outside level III peri-natal centers and transferred after birth to level III centers. Some children who were born in level III perinatal centers were not offered intensive care either because they were considered too immature or because they had lethal anomalies. Birth weight ratio was calculated by dividing the child’s weight by the median weight expected for gestational age and gender of Australian children.13Children with a birth weight ratio⬍.80 were small for
gestational age (SGA), and children with a birth weight ratio ⬎1.25 were large for gestational age (LGA). Cerebroventricular hemorrhage (CVH) was diagnosed during the first week and graded according to Papile et al.14Cystic periventricular
leukoma-lacia (PVL) was diagnosed before discharge and defined as any cystic lesions developing in periventricular white matter of the brain after birth. Postnatal corticosteroid therapy was prescribed for some children after the first week, as described elsewhere.15
Children who required surgery during the primary hospitaliza-tion, mostly involving a general anesthetic but occasionally a local anesthetic for minor surgery such as inguinal hernia repair, were noted. Bronchopulmonary dysplasia (BPD) was diagnosed in chil-dren with respiratory distress and an oxygen requirement after 28 days of age.
Surviving children were enrolled in a longitudinal follow-up study of growth and development. The NBW control participants comprised children whose birth weights were⬎2499 g and who From the Department of Obstetrics and Gynaecology, Royal Women’s
Hospital, Carlton, Australia.
aSee “Appendix” for a list of the Victorian Infant Collaborative Study Group
participants.
Received for publication Sep 19, 2000; accepted Jan 16, 2001.
Address correspondence to (L.W.D.) Department of Obstetrics and Gynae-cology, Royal Women’s Hospital, 132 Grattan St, Carlton, Australia, 3053. E-mail: [email protected]
were randomly selected from births in each of the 3 level III perinatal centers in Victoria and matched with the preterm chil-dren for gender, health insurance status, and mother’s country of origin, as described elsewhere.5Social class was determined by the
occupation of the main income earner in the family and dichoto-mized into higher (professional, skilled, and semiskilled) and lower (unskilled or unemployed) classes. Informed, written con-sent was obtained from the parents of the NBW control partici-pants but not the preterm cohort as follow-up was considered to be part of their normal care. The study was approved by the Research and Ethics Committees of the Royal Women’s Hospital, Melbourne.
Details of the survival rates to 2 years of age for these children have been reported.5No child was known to have died between 2
and 5 years of age.
Surviving children were assessed at 5 years of age, corrected for prematurity, by pediatricians and psychologists who were un-aware of perinatal details, as described elsewhere.15The
psycho-logical assessment included the Full, Verbal and Performance Scales of the Wechsler Preschool and Primary Scale of Intelligence-Revised (WPPSI-R).16Some children could complete only 1 of the
major subscales (Performance or Verbal) of the WPPSI-R, either because English was not their primary language or because of physical limitations. Several children were assessed with alterna-tive IQ tests when the WPPSI-R was unavailable, and that score was taken to represent the child’s IQ. Children who were untest-able by any psychological test because of severe intellectual im-pairment were assigned an IQ score of 40. Children had a major sensorineural disability if they had any of the following: blindness (bilateral vision worse than 6/60), sensorineural deafness requir-ing hearrequir-ing aids, cerebral palsy of such severity that the child was either not walking or walking with considerable difficulty, or an IQ score⬍⫺2 SD below the mean for the NBW control partici-pants. Some children were not seen at 5 years of age but had been evaluated at 2 years of age.5The status of these children with
respect to major sensorineural disability was assumed to be the same at 5 years of age, and their results are included in this article. Data were edited and analyzed with the use of SPSS for Win-dows (version 9.0.1; SPSS Inc, Chicago, IL). Univariate analyses included2tests for dichotomous variables and mean differences
and 95% confidence intervals (CIs) for normally distributed con-tinuous variables. To determine the significant predictive vari-ables, dichotomous outcomes were analyzed by forward condi-tional logistic regression; odds ratios (ORs) and 95% CIs were computed from the regression coefficients. Predictive variables were added appropriate with the age at diagnosis; CVH from day 7 and postnatal corticosteroid therapy, cystic PVL, surgery, and BPD from day 28. The logistic model was considered a good fit of the observed data when the Hosmer-Lemeshow goodness-of-fit test17was not statistically significant. Predicted probabilities were
computed for individual children on the basis of their values for statistically significant variables for 2 situations: 1) survival for infants offered intensive care and 2) survival free of major disabil-ity for infants discharged from the hospital. The predicted rates of outcomes computed from logistic regression for subgroups of children with identical predictive variables then were compared with the actual rates of each outcome. Predicted probabilities were computed also for survival, survival with no major disability, and survival with major disability and plotted by both gestational age
and postnatal age. The level of agreement in the classification of major disability in children in the preterm group assessed at both 2 and 5 years of age was tested by the Kappa statistic. Any bias in the estimate of disability was evaluated by McNemar’s test. For all tests,P⬍.05 was considered statistically significant.
RESULTS
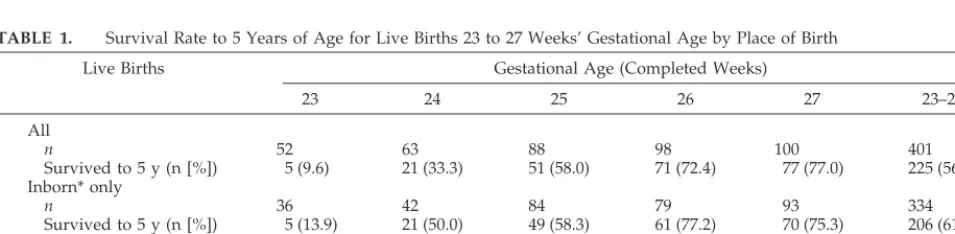
There were 401 consecutive live births with gesta-tional ages 23 to 27 weeks, of whom 225 (56.1%) survived to 5 years of age. The survival rate rose significantly with increasing gestational age (OR: 2.2; 95% CI: 1.8, 2.6, for each week of increase in gesta-tional age; Table 1). The survival rate for those born in a level III center was significantly higher than the survival rate for those born outside a level III center (OR: 3.1; 95% CI: 1.6, 5.9, adjusted for gestational age). Of the 67 live births outside level III centers, 57 were in level II hospitals (hospitals with obstetricians and paediatricians available), 7 were in level I hos-pitals, and 3 were outside any hospital.
Of the 176 preterm children who died, most (57%) did so on the first day of life, with progressively diminishing proportions as postnatal age increased (Table 2). First-day deaths were more frequent with lower gestational age. Of the 101 deaths on the first day, 66 were not offered intensive care, including 36 infants who were born outside a level III center and not transferred after birth. Those who were not of-fered intensive care had significantly lower gesta-tional ages and birth weights than those who were offered intensive care (gestational age, weeks, mean difference: ⫺2.0; 95% CI: ⫺2.3, ⫺1.7; mean birth weight, g, mean difference: ⫺238; 95% CI: ⫺283, ⫺192). All infants who were born outside a level III center and transferred did so on the first day of life; those who were not transferred all died on the first day of life.
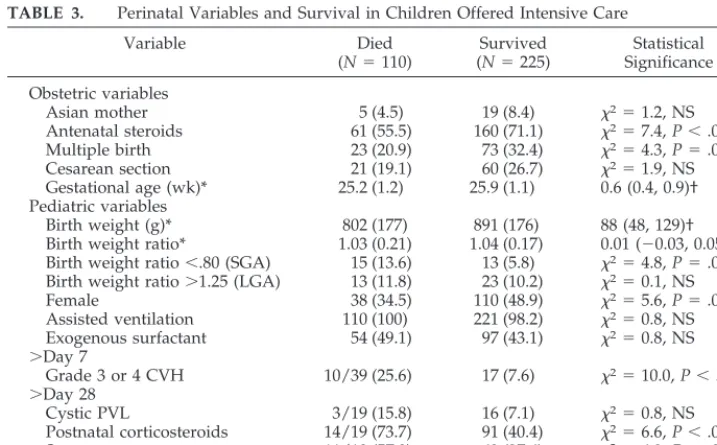
For infants who were offered intensive care on day 1, many perinatal variables differed significantly on univariate analysis between preterm children who died and those who survived (Table 3). On multivar-iate analysis, however, the only variables that were associated positively with survival were increasing maturity (OR for 1 week’s increase: 1.8; 95% CI: 1.4, 2.2), antenatal corticosteroid therapy (OR: 1.9; 95% CI: 1.1, 3.2), being a multiple birth (OR: 2.1; 95% CI: 1.1, 3.7), being female (OR: 2.5; 95% CI: 1.5, 4.3), and not being SGA (OR: 7.4; 95% CI: 2.9, 18.4). As post-natal age increased, different variables were
associ-TABLE 1. Survival Rate to 5 Years of Age for Live Births 23 to 27 Weeks’ Gestational Age by Place of Birth
Live Births Gestational Age (Completed Weeks)
23 24 25 26 27 23–27
All
n 52 63 88 98 100 401
Survived to 5 y (n [%]) 5 (9.6) 21 (33.3) 51 (58.0) 71 (72.4) 77 (77.0) 225 (56.1) Inborn* only
n 36 42 84 79 93 334
Survived to 5 y (n [%]) 5 (13.9) 21 (50.0) 49 (58.3) 61 (77.2) 70 (75.3) 206 (61.7) Outborn† only
n 16 21 4 19 7 67
Survived to 5 y (n [%]) 0 (0.0) 0 (0.0) 2 (50.0) 10 (52.6) 7 (100) 19 (28.4)
ated significantly with survival. Of note, antenatal corticosteroid therapy and multiple pregnancy were not important after day 1, and grade 3 or 4 CVH had an adverse association on day 7 only (OR: 0.22; 95% CI: 0.09, 0.55) but not by day 28. Gestational age was not important by 28 days of age. Being female and not being SGA had persistent survival advantages through each postnatal age (day 7 female OR: 3.3; 95% CI: 1.5, 7.3; not SGA OR: 3.3; 95% CI: 1.03, 10.4; day 28 female OR: 5.3; 95% CI: 1.5, 17.9; not SGA OR: 7.3; 95% CI: 1.8, 29.3). Postnatal steroid therapy, BPD, and surgery were not associated significantly with survival after adjustment for gender and SGA status. For the combinations of perinatal variables in which the number of children in subgroups exceeded 15, the observed rates of survival in those who were
offered intensive care, related to the presence or ab-sence of adverse prognostic variables, were similar to those predicted from the logistic regression (Table 4). Of the 265 NBW control participants in 1991 to 1992, 2 died before 5 years of age, 229 were assessed at 5 years of age, and data were available from for-mal developmental assessments at 2 years of age in another 16 children. The mean WPPSI-R Full Scale IQ was 105.8 (SD: 14.0) for the 222 NBW children who were able to complete the test at 5 years of age. Including an IQ of 40 for 2 untestable children and the results from the Performance Scale of the WPPSI-R for the other 5 children, the mean IQ score for the NBW control participants was 105.3 (SD: 15.1). Of the NBW control participants, none had cerebral palsy, blindness, or deafness; disability in TABLE 2. Outcome to 5 Years of Age for Live Births 23 to 27 Weeks’ Gestational Age by Postnatal Age
Parameter Gestational Age (Completed Weeks)
23 24 25 26 27 23–27
Livebirths(n) 52 63 88 98 100 401
Died(n) 47 42 37 27 23 176
Day 1 (n[% deaths]) 42 (89) 30 (71) 14 (38) 9 (33) 6 (26) 101 (57)
no intensive care (n[% deaths]) 36 (77) 22 (52) 5 (14) 2 (7) 1 (4) 66 (38)
intensive care (n[% deaths]) 6 (13) 8 (19) 9 (24) 7 (26) 5 (22) 35 (20)
Days 2–7 (n[% deaths]) 2 (4) 8 (19) 10 (37) 8 (30) 8 (35) 36 (20)
Days 8–28 (n[% deaths]) 2 (4) 3 (7) 7 (19) 5 (19) 3 (13) 20 (11)
After day 28 to discharge (n[% deaths]) 1 (2) 1 (2) 6 (16) 5 (19) 6 (26) 19 (11)
Post discharge (n[% deaths]) 0 (0) 0 (0) 0 (0) 1 (4) 1 (4) 2 (1)
Survived without major disability(n) 3 14 38 54 72 181*
% of all live births (95% CI) 6 (1, 16) 22 (13, 34) 43 (33, 54) 55 (45, 65) 72 (62, 80) 45† (40, 50) % if discharged home (95% CI) 60 (15, 95) 67 (43, 85) 75 (60, 86) 75 (63, 84) 92 (84, 97) 80† (74, 85)
Survived with major disability(n) 2 7 13 17 5 44
% of all live births (95% CI) 4 (0, 13) 11 (5, 22) 15 (8, 24) 17 (10, 26) 5 (2, 11) 11 (8, 14) % if discharged home (95% CI) 40 (5, 85) 33 (15, 57) 25 (14, 40) 24 (14, 35) 6 (2, 14) 19‡ (14, 24)
* Assumes 4 survivors not assessed (n⫽1 at 26 weeks,n⫽3 at 27 weeks) had no disability. † Statistically significant increase with increasing gestational age.
‡ Statistically significant decrease with increasing gestational age.
Total numbers offered intensive care comprise all deaths offered intensive care and all survivors.
TABLE 3. Perinatal Variables and Survival in Children Offered Intensive Care
Variable Died
(N⫽110)
Survived (N⫽225)
Statistical Significance
Obstetric variables
Asian mother 5 (4.5) 19 (8.4) 2⫽1.2, NS
Antenatal steroids 61 (55.5) 160 (71.1) 2⫽7.4,P⬍.01
Multiple birth 23 (20.9) 73 (32.4) 2⫽4.3,P⫽.039
Cesarean section 21 (19.1) 60 (26.7) 2⫽1.9, NS
Gestational age (wk)* 25.2 (1.2) 25.9 (1.1) 0.6 (0.4, 0.9)† Pediatric variables
Birth weight (g)* 802 (177) 891 (176) 88 (48, 129)†
Birth weight ratio* 1.03 (0.21) 1.04 (0.17) 0.01 (⫺0.03, 0.05)† Birth weight ratio⬍.80 (SGA) 15 (13.6) 13 (5.8) 2⫽4.8,P⫽.026
Birth weight ratio⬎1.25 (LGA) 13 (11.8) 23 (10.2) 2⫽0.1, NS
Female 38 (34.5) 110 (48.9) 2⫽5.6,P⫽.018
Assisted ventilation 110 (100) 221 (98.2) 2⫽0.8, NS
Exogenous surfactant 54 (49.1) 97 (43.1) 2⫽0.8, NS
⬎Day 7
Grade 3 or 4 CVH 10/39 (25.6) 17 (7.6) 2⫽10.0,P⬍.01
⬎Day 28
Cystic PVL 3/19 (15.8) 16 (7.1) 2⫽0.8, NS
Postnatal corticosteroids 14/19 (73.7) 91 (40.4) 2⫽6.6,P⬍.02
Surgery 11/19 (57.9) 62 (27.6) 2⫽6.3,P⬍.02
BPD 17/19 (89.5%) 156 (69.3%) 2⫽2.5, NS
Data aren(%), unless otherwise indicated. NS indicates not significant.
* Mean (SD).
the control participants, therefore, was assessed solely on the basis of psychological tests. A total of 10 of the 245 NBW control participants (4.1%; 95% CI: 2.0%, 7.4%) had a major sensorineural disability, and survival free of major sensorineural disability at 5 years was 95.5% (253 of 265; 95% CI: 92.2%, 97.6%) for those discharged from the hospital, assuming that the 18 children with no data did not have a disability.
Of the 225 preterm survivors to 5 years of age, outcome data were available for 221 (98.2%), includ-ing 8 children assessed at 2 years of age. Twenty-five of the 221 survivors (11.3%) assessed had some form of cerebral palsy, but the disability was major only in 15. Four children (1.8%) were blind, 2 children (0.9%) required hearing aids for sensorineural deafness, and 34 children (15.4%) had IQ scores⬍⫺2 SD compared with NBW control participants. In the preterm co-hort, 44 of the 225 children (19.6%; 95% CI: 14.4%, 24.7%) had a major sensorineural disability, assum-ing that the 4 survivors who were not assessed had no disability. The rate of survival without a major sensorineural disability for preterm infants dis-charged from the hospital was 79.7% (181 of 227; 95% CI: 74.5%, 85.0%). The rate of survival without major disability rose significantly with increasing gesta-tional age, with the denominator being any of all live births (Table 2; OR for 1 week’s increase: 2.18, 95%
CI: 1.81, 2.63), live births offered intensive care (OR for 1 week’s increase: 1.75; 95% CI: 1.42, 2.14), or those discharged from the hospital alive (Table 2; OR for 1 week’s increase: 1.63; 95% CI: 1.20, 2.20). Con-versely, increasing gestational age was not related significantly to the rate of survival with a major disability with the denominator either all live births (Table 2; OR for 1 week’s increase: 1.02; 95% CI: 0.81, 1.29) or live births offered intensive care (OR for 1 week’s increase: 0.78; 95% CI: 0.60, 1.02). Increasing gestational age was, however, related significantly to a lower rate of survival with major disability in sur-vivors to hospital discharge (Table 2; OR for 1 week’s increase: 0.59; 95% CI: 0.43, 0.80).
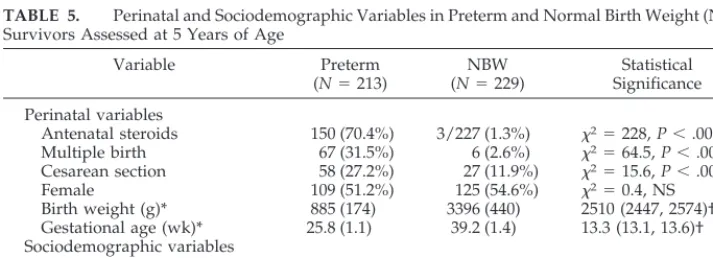
For children who were seen at 5 years of age, as expected there were many significant differences in perinatal variables between the preterm and NBW groups (Table 5). There were, however, no significant differences in gender or socioeconomic variables.
On multivariate analysis, the variables that were associated significantly with survival free of major sensorineural disability were similar to those associ-ated with survival per se at each postnatal age through day 7, with the exceptions that surfactant was associated with a significant reduction in sur-vival free of major disability at both day 1 (OR: 0.57; 95% CI: 0.35, 0.91) and day 7 (OR: 0.51; 95% CI: 0.29, 0.91), and multiple pregnancy was unimportant on TABLE 4. Observed and Predicted Rates of Survival to 5 Years for Very Preterm Children Offered
Intensive Care Related to Common Combinations of Perinatal Variables, Averaged Over All Gesta-tional Ages
Combination of Perinatal Variables
No. births
Survival
Observed Predicted*
N % (95% CI) % (95% CI)
ANS, girl, not SGA, multiple 27 23 85 (66, 96) 88 (86, 91)
ANS, girl, not SGA, singleton 61 48 79 (66, 88) 80 (78, 83)
ANS, boy, not SGA, multiple 35 31 89 (73, 97) 77 (73, 80)
ANS, boy, not SGA, singleton 75 47 63 (51, 74) 65 (62, 68)
No ANS, girl, not SGA, singleton 37 25 68 (50, 82) 63 (57, 69) No ANS, boy, not SGA, singleton 49 25 51 (36, 65) 50 (46, 54) No ANS, boy, not SGA, multiple 18 10 56 (31, 78) 64 (58, 70)
ANS indicates antenatal steroids. * Predicted from logistic regression.
Hosmer-Lemeshow goodness-of-fit test,P⫽.75, as described in “Methods.”
TABLE 5. Perinatal and Sociodemographic Variables in Preterm and Normal Birth Weight (NBW) Survivors Assessed at 5 Years of Age
Variable Preterm
(N⫽213)
NBW (N⫽229)
Statistical Significance
Perinatal variables
Antenatal steroids 150 (70.4%) 3/227 (1.3%) 2⫽228,P⬍.0001
Multiple birth 67 (31.5%) 6 (2.6%) 2⫽64.5,P⬍.0001
Cesarean section 58 (27.2%) 27 (11.9%) 2⫽15.6,P⬍.001
Female 109 (51.2%) 125 (54.6%) 2⫽0.4, NS
Birth weight (g)* 885 (174) 3396 (440) 2510 (2447, 2574)†
Gestational age (wk)* 25.8 (1.1) 39.2 (1.4) 13.3 (13.1, 13.6)† Sociodemographic variables
Asian mother 18 (8.5%) 12 (5.2%) 2⫽1.3, NS
Higher social class 110 (51.6%) 129 (56.3%) 2⫽0.8, NS
No English-speaking at home 13 (6.1%) 9 (3.9%) 2⫽0.7, NS
Data aren(%), unless otherwise indicated. NS indicates not significant.
* Mean (SD).
day 1. However, by day 28, other events after birth became more important than those associated with survival per se: grade 3 or 4 CVH (OR: 0.29; 95% CI: 0.10, 0.85), cystic PVL (OR: 0.25; 95% CI: 0.08, 0.74), surgery during the primary hospitalization (OR: 0.34; 95% CI: 0.17, 0.67), and requiring postnatal cor-ticosteroid therapy (OR: 0.23, 95% CI: 0.11, 0.45) were the only variables that were associated significantly with a lower rate of survival free of major sensori-neural disability. In other words, these variables were associated positively with either death or dis-ability.
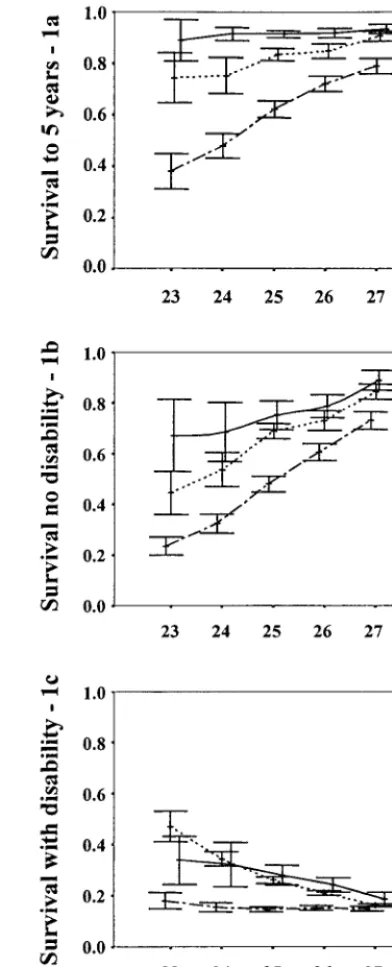
The relationships between survival, survival free of major disability, and survival with major disabil-ity on the one hand and postnatal age and gestational age on the other hand are illustrated in Fig 1. The probability of survival rose progressively with in-creasing postnatal age (Fig 1A). The probability of survival rose significantly with increasing gesta-tional age only for postnatal ages before day 28 (Fig 1A). The probability of survival without a major sensorineural disability rose significantly with in-creasing postnatal age (Fig 1B). The probability of survival without a major sensorineural disability rose significantly with increasing gestational age at all postnatal ages (Fig 1B). The probability of sur-vival with a major disability was higher with increas-ing postnatal age (Fig 1C). The probability of sur-vival with a major disability was not significantly negatively related to gestational age on day 1 but only on day 7 and day 28 (Fig 1C).
If children with no outcome data at either 2 or 5 years of age were considered to have a disability or be dead, rather than without a disability and alive, or if the analyses were limited to only those who were assessed at 5 years of age, then few statistical con-clusions were altered. The minor exception was that antenatal steroid therapy was no longer associated significantly with survival free of disability on day 1 (OR: 1.5; 95% CI: 0.92, 2.5). In the 210 children in the preterm group who were assessed at both 2 and 5 years of age, the classification of major disability or not was the same at both 2 and 5 years in 190 (90.5%). The level of agreement between the 2- and 5-year assessments was highly significant ( ⫽ 0.691, t ⫽
10.0,P⬍⬍.0001). There was no significant bias in the assessment of major disability at 2 years of age; dis-ability at 5 years of age was underestimated in 9 children and overestimated in 11 children at 2 years of age (McNemar test,P ⫽.82, NS).
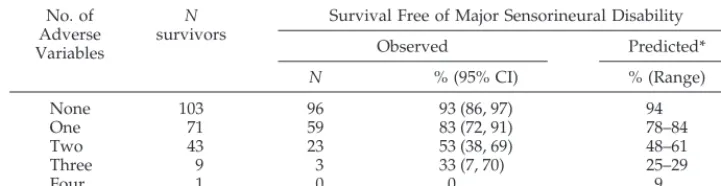
For preterm children who were discharged from the hospital, the adverse prognostic variables that were associated significantly with survival free of major disability at 5 years of age were grade 3 or 4 CVH (OR: 0.29; 95% CI: 0.10, 0.90), cystic PVL (OR: 0.24; 95% CI: 0.07, 0.74), surgery during the primary hospitalization (OR: 0.35; 95% CI: 0.17, 0.67), and requiring postnatal corticosteroid therapy (OR: 0.26; 95% CI: 0.12, 0.57). Almost one half had none of these adverse prognostic variables, and their rate of sur-vival free of major sensorineural disability was 93.2% (Table 6), not significantly different from the rate of 95.5% for NBW children (2⫽0.6, NS). However, the
rate of survival free of major sensorineural disability
fell as the number of adverse prognostic variables increased (Table 6). The observed rates of survival free of major sensorineural disability related to the number of adverse prognostic variables were close to those predicted from the logistic regression.
DISCUSSION
Although this study deals with⬍1% of all children born, they are the most controversial group with respect to active treatment. Attitudes toward their care differ; hence, their prognosis varies consider-ably between regions.1–10
ing the outcome for all very preterm children to be determined, not just those in perinatal centers that have selective referral patterns. Both survival and sensorineural disability are included, allowing an estimate of the interplay between these important events. Outcome has been determined at 5 years of age, enabling a more certain estimate of sensorineu-ral morbidity than studies of outcome earlier in childhood. The follow-up rate is high, particularly for the preterm cohort, and therefore the uncertainty about children not assessed is reduced. There are contemporaneous NBW control participants with which to compare the outcome measures for very preterm children. The altered prognosis with chang-ing events in the perinatal period has been estimated. No other study has been as rigorous in determining the prognosis for very preterm infants.
As well as some of the advantages of regional studies, listed above, there are limitations. We are less certain about care and decision making around the time of birth for infants who are born outside level III perinatal centers than we are within the 3 level III perinatal centers in Victoria. Most infants who were born outside level III centers were born in level II centers, with the ability to provide short-term assisted ventilation pending the arrival of the trans-port team. We also are unsure about the diagnosis of some other potentially important prognostic vari-ables, such as chorioamnionitis and antepartum hemorrhage, in those born outside level III centers; hence, we could not include these variables in our analyses. Our data, however, might be considered as an estimate of the outcomes to be expected, averaged over other prognostic variables that could not be included because of lack of data. Another potential limitation of our study is that we included 2-year data on some children who were not assessed at 5 years of age. We also assumed that those with no follow-up data at all had no major disability, because this was the most likely outcome given the low rate of major disability, especially in the NBW control participants. Whether these children were included in analyses or not had little effect on the statistical conclusions of the study.
There has been increasing regionalization of peri-natal intensive care in Victoria. Fewer very preterm or tiny children have been born outside level III perinatal centers over time; consequently, the sur-vival difference between inborn and outborn
chil-dren has widened.11Lorenz18recently reviewed the
survival rates reported from 10 studies for extremely preterm infants born in North America in the 1990s. However, none of the studies quoted comprised a regional cohort and cannot be compared directly with our study. In several recent regional cohort studies reported from the United Kingdom,6,8,10the
survival rates have been similar to or lower than those in our study. The survival rate increased within our own region later in the 1990s.9 Possible
reasons for differences in regional survival rates be-tween the United Kingdom and Australia have been described elsewhere.9
Apart from place of birth and attitude toward treatment, in our study the other significant prognos-tic variables that were associated with improved sur-vival in those who were offered intensive care were also reported by Draper et al8 (female gender,
in-creasing gestational age, not being SGA, and multi-ple birth). In addition, antenatal corticosteroid ther-apy, not included by Draper et al,8 is known to
improve survival rates in preterm infants.19 In our
study, the importance of these prognostic variables changed with postnatal age. The effect of antenatal corticosteroids was obvious only early, whereas oth-ers (gender and SGA) poth-ersisted throughout the new-born period. The association of decreased survival of children who survived to day 7 with the presence of grade 3 or 4 CVH may reflect the degree of illness of some of these children or the withdrawal of intensive care in others. Interestingly, mother’s race, birth weight, being LGA, and mode of delivery were not associated with improved survival after allowing for other, more important prognostic variables. There was, however, limited power to expect significant relationships with mother’s race and being LGA. For more common combinations of significant prognos-tic variables, the probability of survival predicted from the logistic regression was close to the observed rates of survival. If these prognostic variables can be confirmed in an independent cohort, it means that prognostication can be refined further for infants with and without these characteristics. Draper at al8
provided outcomes for 2 time periods; first, for fe-tuses alive at labor onset, and second, for those ad-mitted to neonatal units. The current study extends the time frame for prognostication at intervals from day 1 for those offered intensive care, up to the time of discharge home. Cooper et al20described changes
TABLE 6. Observed and Predicted Rates of Survival Free of Major Sensorineural Disability for Very Preterm Children Discharged Home Related to the Number of Adverse Variables
No. of Adverse Variables
N
survivors
Survival Free of Major Sensorineural Disability
Observed Predicted*
N % (95% CI) % (Range)
None 103 96 93 (86, 97) 94
One 71 59 83 (72, 91) 78–84
Two 43 23 53 (38, 69) 48–61
Three 9 3 33 (7, 70) 25–29
Four 1 0 0 9
Assumes 4 children not assessed had no disability. * Predicted from logistic regression.
in survival rate with increasing postnatal age in very preterm infants. We extended these observations by also describing changes in sensorineural outcome with increasing postnatal age.
Several groups of investigators recently reported rates of sensorineural disabilities in regional cohorts of very preterm infants born in the 1990s. Tin et al6
reported that 27% of survivors (25 of 93) who were born at 23 to 27 weeks’ gestational age in the North-ern Region of England in 1991 to 1994 had a severe disability at 1 year of age, similar to the rate of major disability of 20% (44 of 225) in our study for children with the same gestational ages. More recently, the EPICure Study Group10reported that 23% of
survi-vors (64 of 283) who were born at 22 to 25 weeks’ gestational age in the United Kingdom and Ireland in 1995 had a severe disability at 2.5 years of age, sim-ilar to the rate of major disability in our study of 29% (22 of 77) for survivors at 23 to 25 weeks’ gestational age. It is difficult to make direct comparisons, how-ever, as disabilities were not defined identically in all studies, and the ages of assessment also differed.
Early in the neonatal period, most of the variables that were associated with survival in our study also were associated with survival free of major sensori-neural disability, because the number of children who died exceeded the number who survived with major disability. With increasing postnatal age, as the mortality rate dropped, the important prognostic variables that were associated with a lower rate of survival free of sensorineural disability were as ex-pected, having been described elsewhere as being associated with adverse sensorineural outcome (CVH,21 PVL,21 postnatal corticosteroid therapy,15
and surgery during the primary hospitalization22).
What is unique in the current study is an estimate of the additive contribution of these adverse variables on the rate of survival free of major sensorineural disability. Knowledge of the presence or absence of these variables during the primary hospitalization will facilitate counseling of parents whose children are being cared for in the nursery. Of note is that almost one half of very preterm survivors had no adverse prognostic variables, and their outcome was not significantly different from the contemporaneous NBW control participants. It also is noteworthy that at the time of deciding whether to offer intensive care, there is no clear relationship between survival with major disability and gestational age. For those who wish to avoid completely the birth of a infant who ultimately survives with a major disability, there is no gestational age, including term, that is totally free of that outcome. Indeed, at the time of initiating intensive care on day 1, the rate of survival with a major disability is the same at 23 weeks’ gestation as it is in the NBW control participants, largely because most of those at 23 weeks ultimately die. Moreover, although the rate of disability in sur-vivors to discharge falls with gestational age, there is no clear distinction between 23 and 26 weeks, inclu-sive. However, survivors at 27 weeks do almost as well as NBW control participants.
CONCLUSION
The prognosis for very preterm children varies with the place of birth (level III perinatal center or not), the attitude of both obstetricians and pediatri-cians toward care and hence the interventions they use, gestational age, postnatal age, and then later comorbidities. Because the prognosis changes sub-stantially with postnatal age, counseling of families should be repeated at intervals, and the advice of-fered should vary with perinatal events.
APPENDIX: PARTICIPANTS OF THE VICTORIAN INFANT COLLABORATIVE STUDY GROUP Convenor: Lex W. Doyle, MD, FRACP, pediatrician*. Collabo-rators (in alphabetical order): Ellen Bowman, MB, BS, FRACP, pediatrician*¶; Catherine Callanan, RN, research nurse*; Elizabeth Carse, MB, BS, FRACP, pediatrician§; Dan Casalaz, MB, BS, FRACP, pediatrician‡; Margaret P. Charlton, MEd Psych, psychol-ogist§; Noni Davis, MB, BS, FRACP, pediatrician*; Geoffrey Ford, MB, BS, FRACP, pediatrician*; Simon Fraser, MB, BS, FRACP, pediatrician‡; Jane Halliday, PhD, epidemiologist#, Marie Hayes, RN, research nurse§; Elaine Kelly, MA, psychologist*‡; Anne Rick-ards, PhD, psychologist*; Michael Stewart, MB, BS, FRACP, pedi-atrician储; Andrew Watkins, MB, BS, FRACP, pediatrician‡; Heather Woods, RN, research nurse‡; and Victor Yu, MD, FRACP, pediatrician§.
From the *Royal Women’s Hospital, ‡Mercy Hospital for Women, §Monash Medical Centre, 储Royal Children’s Hospital, ¶Newborn Emergency Transport Service, and #Victorian Perinatal Data Collection Unit, Melbourne, Australia.
ACKNOWLEDGMENT
This study was funded in part by the Department of Human Services, Victoria, Australia.
REFERENCES
1. van Zeben-van der Aa TM, Verloove-Vanhorick SP, Brand R, Ruys JH. Morbidity of very low birthweight infants at corrected age of 2 years in a geographically defined population.Lancet. 1989;1:253–255
2. Wariyar U, Richmond S, Hey E. Pregnancy outcome at 24 –31 weeks’ gestation: neonatal survivors.Arch Dis Child. 1989;64:678 – 686 3. Johnson A, Townshend P, Yudkin P, Bull D, Wilkinson AR. Functional
abilities at age 4 years of children born before 29 weeks of gestation.Br Med J. 1993;306:1715–1718
4. Doyle LW, for the Victorian Infant Collaborative Study Group. Out-come to five years of age of children born at 24 –26 weeks’ gestational age in Victoria.Med J Aust. 1995;163:11–14
5. The Victorian Infant Collaborative Study Group. Outcome at 2 years of children 23–27 weeks’ gestation born in Victoria in 1991–92.J Paediatr Child Health.1997;33:161–165
6. Tin W, Wariyar U, Hey E. Changing prognosis for babies of less than 28 weeks’ gestation in the north of England between 1983 and 1994. Northern Neonatal Network.Br Med J1997;314:107–111
7. Cartlidge PH, Stewart JH. Survival of very low birthweight and very preterm infants in a geographically defined population.Acta Paediatr. 1997;86:105–110
8. Draper ES, Manktelow B, Field DJ, James D. Prediction of survival for preterm births by weight and gestational age: retrospective population based study.Br Med J. 1999;319:1093–1097
9. Doyle LW, Morley CJ, Halliday J. Prediction of survival for preterm births. Data on the quality of survival are needed.Br Med J. 2000;320:648 10. Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR, for the EPICure Study Group. Neurologic and developmental disability after extremely preterm birth.N Engl J Med. 2000;343:378 –384
11. The Victorian Infant Collaborative Study Group. Changing outcome for infants of birthweight 500 –999 g born outside level-III centres in Vic-toria.Aust N Z J Obstet Gynaecol. 1997;37:253–257
12. Doyle LW, Kitchen WH, Lumley J, et al. Accuracy of mortality rates for livebirths 500 –999 g birthweight [letter].Med J Aust. 1991;156:72 13. Beeby PJ, Bhutap T, Taylor LK. New South Wales population-based
birthweight percentile charts.J Paediatr Child Health. 1996;32:512–518 14. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of
15. The Victorian Infant Collaborative Study Group. Postnatal corticoste-roids and sensorineural outcome at 5 years of age.J Paediatr Child Health. 2000;36:256 –261
16. Wechsler D.Wechsler Preschool and Primary Scale of Intelligence–Revised. New York, NY: The Psychological Corporation; 1989
17. Lemeshow S, Hosmer DW Jr. A review of goodness of fit statistics for use in the development of logistic regression models.Am J Epidemiol. 1982;115:92–106
18. Lorenz JM. Survival of the extremely preterm infant in North America in the 1990s.Clin Perinatol. 2000;27:255–262
19. Crowley P. Corticosteroids prior to preterm delivery (Cochrane
Re-view). In: The Cochrane Library, Issue 2. Oxford: Update Software; 1998. Updated quarterly
20. Cooper TR, Berseth CL, Adams JM, Weisman LE. Actuarial survival in the premature infant less than 30 weeks’ gestation.Pediatrics. 1998;101: 975–978
21. Doyle LW, Betheras FR, Ford GW, Davis NM, Callanan C. Survival, cranial ultrasound and cerebral palsy in very low birthweight infants: 1980s versus 1990s.J Paediatr Child Health. 2000;36:7–12
22. The Victorian Infant Collaborative Study Group. Surgery and the tiny baby: sensorineural outcome at 5 years of age.J Paediatr Child Health. 1996;32:167–172
THE ATTENTION-DEFICIT DISORDER EPIDEMIC
In 1980 it was estimated that somewhere between 270,000 and 541,000 elemen-tary school students were taking Ritalin. By 1987, around 750,000 were. And the use of the drug didn’t really take off until the 1990s. In 1997 around 30,000 pounds were produced —an increase of more than 700% over the 1990 production level.
Far from all of that Ritalin goes to elementary school kids, but the Ritalin that does is prescribed most frequently in upper-middle-class suburban districts— where, one suspects, the achievement ethos is strongest. Some physicians believe that 10% of all children have the sort of conduct disorder—attention-deficit disor-der, oppositional defiant disorder—that could be eased with Ritalin or some other drug. It is stunning how quickly we have moved from the idea that children should be given freedom to chart their own learning to a belief that adults have a responsibility to reshape the minds of kids whose behavior deviates form the standard.
Brooks D. The organization kid.Atlantic Monthly.April 2001
DOI: 10.1542/peds.108.1.134
2001;108;134
Pediatrics
Lex W. Doyle and for the Victorian Infant Collaborative Study Group
Prognosis
Outcome at 5 Years of Age of Children 23 to 27 Weeks' Gestation: Refining the
Services
Updated Information &
http://pediatrics.aappublications.org/content/108/1/134
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/108/1/134#BIBL
This article cites 20 articles, 5 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.108.1.134
2001;108;134
Pediatrics
Lex W. Doyle and for the Victorian Infant Collaborative Study Group
Prognosis
Outcome at 5 Years of Age of Children 23 to 27 Weeks' Gestation: Refining the
http://pediatrics.aappublications.org/content/108/1/134
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.