Comparative Practice Patterns of Emergency Medicine Physicians and
Pediatric Emergency Medicine Physicians Managing Fever
in Young Children
Daniel J. Isaacman, MD*; Kimberly Kaminer, MD‡; Hari Veligeti, MD*; Michael Jones, BA*; Paris Davis, BA*; and Jon D. Mason, MD‡
ABSTRACT. Background/Objective. The management
of fever in young children is a controversial topic. This study seeks to compare the management approaches be-tween general emergency medicine physicians (GEMPs) and pediatric emergency medicine physicians (PEMPs) and correlate them to existing practice guidelines.
Design/Methods. All charts of children age 3 to 36 months presenting with the complaint of fever at both a children’s hospital emergency department (ED) and a general ED from June 1, 1998 to September 1, 1998; De-cember 1, 1998 to April 1, 1999; and June 1, 1999 to September 1, 1999 were retrospectively reviewed. Fever was defined as>39°C. Patients with a history of immu-nodeficiency, chronic illness, ventriculoperitoneal shunt, antibiotic use in the past 48 hours, or focal infection noted on examination were excluded. Data collected in-cluded focal exam findings, laboratory tests, diagnosis, treatment, and disposition. Variances from the practice guidelines were tabulated and compared.
Results. One thousand three hundred twenty-three eligible children met exclusion criteria and were seen by PEMPs; 755 were eliminated because of exclusion criteria (526 because of focal infection). Twenty-two (4%) of 568 remaining patients were admitted to the hospital. Two hundred twenty-eight eligible children were seen by GEMPs; 147 were excluded (109 because of focal infec-tion). No patients were admitted to the hospital. PEMPs ordered more complete blood counts (324/568 vs 27/81), more blood cultures (321/568 vs 27/81), and more urine cultures (208/568 vs 20/81) than GEMPs. GEMPs ordered more chest radiographs and cerebrospinal fluid analyses than PEMPs; GEMPs ordered less complete blood counts, blood cultures, and urine cultures than PEMPs. GEMPs diagnosed more focal infections (109/228 vs 526/1323), and conflicted more often with the practice guidelines (66/79 vs 225/498) than PEMPs. Patients spent an average of 2.26 ⴞ 0.16 hours in the pediatric ED versus 3.0 hoursⴞ0.18 hours in the general ED.
Conclusions. Significant differences in the manage-ment of the young child with fever and no source exist between these two groups of physicians. These varia-tions affect both cost and standard of care. Future studies assessing whether these strategies affect patient out-comes would further elucidate their clinical implication.
Pediatrics2001;108:354 –358;laboratory utilization, prac-tice patterns, child.
ABBREVIATIONS. ED, emergency department; PEMP, pediatric emergency medicine physician; GEMP, general emergency medi-cine physician; UTI, urinary tract infection; CSF, cerebrospinal fluid.
F
ever continues to be a frequent chief complaint of children presenting for emergency care. While the presentation of a young child with high fever and no obvious focus of infection on ex-amination is a common occurrence, the management of this clinical situation may vary considerably. Al-though several reports have commented on the different management approaches between commu-nity-based and hospital-based practitioners, the ma-jority of these studies were based on the surveyed responses of groups of physicians.1–5 Few studieshave evaluated actual practice patterns to compare and contrast management styles.
The majority of children who present for emer-gency services in the United States are seen in gen-eral emergency departments (EDs). These centers are generally comprised of emergency physicians trained in the delivery of emergency care to both children and adults. A smaller percentage of children are seen in pediatric EDs. These centers are generally staffed by physicians trained in general pediatrics, that have completed fellowship training in pediatric emergency medicine. To date, no studies have com-pared the management of febrile young children pre-senting to these 2 types of EDs. The purpose of this study was to compare the practice patterns of a general ED with that of a pediatric ED regarding the management of the child 3 to 36 months of age with fever and no source.
MATERIAL AND METHODS
All charts of patients 3 to 36 months of age presenting with fever documented at triage ofⱖ39°C at either an urban children’s hospital ED or a suburban general ED from June 1, 1998 to September 1, 1998; December 1, 1998 to April 1, 1999; and June 1, 1999 to September 1, 1999 were retrospectively reviewed. Review dates were divided as above to collect equal numbers of patients presenting in both winter and summer months. The children’s hospital ED was located in an urban setting with an annual census of 35 000 patients per year. Sixty percent of the population carried Medicaid, Medicare, or no health insurance. The general ED was located 10 miles east of the children’s hospital in a suburban setting that sees 52 000 patients annually, 19% of which are
chil-From the *Division of Pediatric Emergency Medicine, Departments of Pe-diatrics and ‡Emergency Medicine, Eastern Virginia Medical School, Nor-folk, Virginia.
Received for publication Sep 18, 2000; accepted Dec 18, 2000.
Reprint requests to (D.J.I.) Children’s Hospital of The King’s Daughters, 601 Children’s Ln, Norfolk, VA 23505. E-mail: [email protected]
dren. Fifty-eight percent of the population carried Medicaid, Medicare, or no health insurance. Both centers used resident phy-sicians to assist in the delivery of care.
Charts were identified through daily review of the triage log. All charts of patients presenting with chief complaints of fever, or “warm to the touch” were reviewed. Charts were reviewed by 1 of 4 co-investigators (K.K., H.V., M.J., P.D.) using predetermined criteria. Patients outside the 3- to 36-month age range or with a history of immunodeficiency, chronic illness (including sickle cell anemia, cystic fibrosis, and steroid-dependent asthma), ventricu-loperitoneal shunt, or antibiotic use in the past 48 hours, were excluded. Patients with focal bacterial infection noted on exami-nation (including findings suggestive of cellulitis, meningitis, oti-tis, pharyngioti-tis, pneumonia, or bone and joint infections) were entered into the database but excluded from additional analysis regarding management. Data collected on each patient included physical examination findings, laboratory tests, diagnosis, treat-ment, total time spent in the ED, and disposition. Management of each of these patients was compared with existing guidelines for this clinical problem.6Variations from the guidelines were
quan-tified and categorized. Those practices counted as variations in-cluded: 1) failure to perform a complete blood count in a febrile child sent home with no parenteral antibiotic treatment; 2) failure to obtain a urinalysis in a febrile boy⬍6 months of age or febrile girl⬍2 years of age; 3) obtaining a urinalysis and culture via bag specimen; 4) treating a patient with ceftriaxone without obtaining a blood culture; or 5) treating a nontoxic febrile patient with a white blood cell count⬍15 000/mm3with ceftriaxone.
Data were entered and analyzed using SPSS for windows soft-ware (SPSS Inc, Chicago, IL). Categorical data were compared using 2testing for standard dichotomous variables or Fisher’s
exact test for dichotomous variables where an expected cell value was⬍5. Continuous data were compared using Student’sttest. Significance was determined asP⬍.05.
RESULTS
One thousand three hundred twenty-three eligible children met inclusion criteria and were seen at the pediatric ED. Seven hundred fifty-five were ex-cluded (526 because of focal infection and 229 be-cause of other exclusions), leaving 568 patients for analysis. Two hundred twenty-eight eligible children were seen in the general ED. One hundred forty-seven were excluded (109 because of focal infection, and 38 because of other exclusions), leaving 81 study patients. No differences between the mean ages (16.3⫾8.8 months vs 18.0⫾9.8 months;P⫽.11) and mean presenting temperatures (39.7 ⫾ 0.5°C vs 39.8 ⫾ 0.5°C; P ⫽ .16) were noted between the 2 groups. Management styles between the physician groups are presented for the categories of laboratory testing, final diagnoses, correlation with practice guidelines, and time spent in the ED.
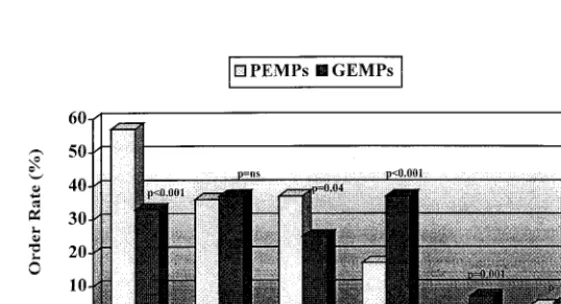
Laboratory Testing
The frequency of laboratory testing differed be-tween the 2 groups (Fig 1). In general, pediatric emergency medicine physicians (PEMPs) more fre-quently ordered complete blood counts, blood cul-tures, and urine cultures than did general emergency physicians (GEMPs) and were less likely to order chest radiographs and perform lumbar punctures than their general ED counterparts. No differences between groups were noted in the frequency of uri-nalysis or electrolyte testing.
Final Diagnoses
Focal bacterial infection (an exclusion criterion) was noted in 41% of patients screened. GEMPs diag-nosed more focal bacterial infections than did PEMPs (109/228 vs 526/1323;P⫽ .015).
The frequency of final diagnoses among the co-horts of included children consisted primarily of a nonspecific diagnosis of fever, the diagnosis of an occult bacterial infection, or the diagnosis of a spe-cific viral illness. The most common final diagnosis given by both physician groups was acute febrile illness. Diagnoses suggesting specific viral infection were given in 72 children (11.1% of cases). Specific viral infections were diagnosed more frequently by PEMPs than GEMPs (70/568 vs 2/81;P⫽.003). The specific viral diagnoses given by PEMPs included bronchiolitis (20), herpangina/hand, foot, and mouth, disease (20), croup (19), varicella (6), and influenza (5). Varicella (2) was the only specific viral diagnosis given by GEMPs. The 70 febrile patients seen by PEMPs with presentations suggesting spe-cific viral illnesses received significantly less labora-tory testing and antibiotic treatment than those who had fever with no source (Table 1). As the practice guidelines suggest empiric laboratory testing only for children “with no focus of infection”, these 72 children were omitted from analysis regarding prac-tice guideline compliance.
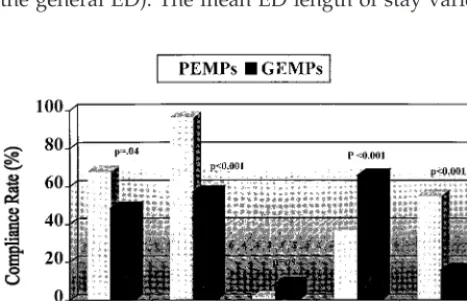
Correlation With Practice Guidelines
Seventy-two patients were diagnosed with classic viral illnesses and were omitted from analysis re-lated to management, leaving 577 patients for anal-ysis. Although both groups of physicians frequently deviated from the practice guidelines, GEMPs did so
more frequently than did PEMPs (66/79 vs 225/498;
P⬍ .001). Individual variations from the guidelines are compared between groups (Fig 2). GEMPs were less likely to obtain urine cultures in boys⬍6 months of age and girls⬍2 years of age (17/35 vs 147/217;
P⫽.04), whereas GEMPs were more likely to obtain urine via bag method rather than via catheterization or suprapubic aspiration (12/28 vs 6/159;P⬍.001). GEMPs utilized parenteral antibiotics in the man-agement of their patients more frequently than did PEMPs (31/79 vs 83/498;P⬍.001), but ordered less complete blood counts than their pediatric emer-gency medicine counterparts (27/79 vs 314/498;P⬍
.001). Both GEMPs and PEMPs treated the majority of patients with fever and leukocytosis (3/4 vs 55/ 68, respectively; P ⫽ not significant). GEMPs were more likely to treat patients with white blood cell counts less than 15 000/mm3(15/23 vs 26/246;P ⬍
.001). This difference remained present when the patients in each group who had occult bacterial in-fection (4 urinary tract inin-fection [UTI], 2 pneumonia) were excluded from analysis (13/21 vs 22/242;P ⬍
.001).
Time in ED
Information was available regarding total time spent in the ED for 188 patients (114/571 patients seen in the pediatric ED and 74/81 patients seen in the general ED). The mean ED length of stay varied
between PEMPs and GEMPs (2. 3 ⫾ 0.16 hours vs 3.0⫾0.18 hours, respectively;P⬍ .01).
Admission Rates
Twenty-two (4%) of the 581 patients seen in the children’s ED were admitted to the hospital, whereas none of the patients seen in the general ED were admitted (P ⫽.05).
DISCUSSION
Our study uncovered a number of differences in the management of the young child with fever be-tween these 2 groups of ED physicians. These differ-ences have significant ramifications in terms of com-parative treatment costs and the extent to which occult infections might be diagnosed between the 2 populations. Although we did not compare the out-comes between the 2 groups, clearly, this measure could also be affected by these markedly different management approaches.
We deliberately chose the clinical problem of fever without source in the young child as it is a common clinical problem and because a widely disseminated practice guideline exists offering a recommended di-agnostic and treatment approach. It is particularly interesting to note that the heterogeneity in diagnos-tic and treatment approach remains despite the fact that this practice guideline was developed and cir-culated to both the pediatric and emergency medi-cine academic communities.6
Our study uncovered variability between the di-agnostic testing, management approaches, and lengths of stay for febrile children evaluated in the 2 EDs. Although such differences in management style may be expected, the characterization of these differ-ences is useful from several perspectives. Physicians may differ in their approach to laboratory testing and treatment based on their perspectives regarding the risk of disease prevalence, the risk of morbidity resultant from untreated disease, the reliability of follow-up, and the concerns regarding side effects connected with potential treatment. These precon-ceptions may also affect their attitudes toward exist-ing guidelines.7
When comparing diagnostic testing between the groups, general ED physicians were more likely to
TABLE 1. Difference in Test Ordering for PEMPS Test Specific Viral Illness
N⫽70
No Specific Viral Illness
N⫽498
P
Value
Number Ordered
Percentage Number Ordered
Percentage
Complete blood count 11 15.7 311 62.7 ⬍.001
SMA-6 1 1.4 19 3.8 .55
Urinalysis 0 0 207 41.7 ⬍.001
Urine culture 0 0 208 41.9 ⬍.001
Urine (catheterization or suprapubic) 0 0 197 39.7 ⬍.001
Blood culture 11 15.7 308 62.1 ⬍.001
Lumbar puncture/CSF analysis 0 0 6 1.2 .45
Chest radiograph 10 14.3 88 17.7 .32
Rapid strep 0 0 15 3.0 .13
Throat culture 0 0 6 1.2 .46
Antibiotics 2 2.9 94 19.0 ⬍.001
Intravenous antibiotics 1 1.4 81 16.3 ⬍.001
Fig 2. Variations from Practice Guidelines6noted by PEMPs and
obtain chest radiographs and perform lumbar punc-tures, yet less likely to obtain complete blood counts, blood cultures, and urine cultures than their pediat-ric ED counterparts. The differences in chest radio-graphs and cerebrospinal fluid (CSF) evaluation may result from less reliance on the clinical examination by general ED physicians and therefore heightened concern regarding the consequences of a missed pneumonia or meningitis. Likewise, the differences in urine and blood culturing may stem from a num-ber of possibilities: 1) a feeling that the prevalence of these diseases is too low to merit screening; 2) a lower concern regarding the consequences of missed bacteremia or UTI; or 3) an extension of the approach to the adult with signs of UTI where a urinalysis without culture is often used as the sole screening test for the presence of infection.
It was interesting to note that children managed in the pediatric facilities seemed to have shorter lengths of stay in the ED than those managed in the adult facility. Although this information is intriguing, we were only able to collect this information in a minor-ity of the patients studied. The large amount of miss-ing data from the pediatric center limits the strength of this observation. It is possible that selection bias may have altered the generalizability of this data. It is also possible that factors other than physician ef-ficiency contributed to the differences detected.
When comparing treatment profiles, it was evident that general ED physicians were far more likely to use parenteral antibiotics than were pediatric ED physicians. This was probably the management dif-ference with the widest potential ramifications. Of note was the high frequency of cases with normal white blood cell counts that were still treated with parenteral antibiotics by the adult ED physicians. Perhaps this difference reflects differences in reliance on the physical examination, uncertainty regarding follow-up, or concern regarding potential ramifica-tions of missed occult infection. Whatever the ratio-nale, the decision to use parenteral antibiotics on such a high percentage of febrile children has wide implications in terms of cost, potential antibiotic side effects, and inability to rely on clinical signs in fol-low-up.8,9 The most important question is whether
this increased antibiotic usage was associated with any differences in patient outcome. Unfortunately, our design could not address this issue.
Although others have compared the practice patterns between adult and pediatric emergency physicians, the reviews have been limited to survey studies or retrospective reviews. Scribano et al10
pre-sented survey data documenting differences in deci-sion-making regarding time to termination of resus-citation efforts between PEMPs and GEMPs. Krauss et al11 compared survey responses regarding
seda-tion use from 84 children’s hospital EDs with those from 154 general hospital EDs and found a signifi-cant decrease in the use of sedation in the general hospitals. More recently, Hampers et al12 reviewed
455 cases of children presenting to either a pediatric ED or a general ED with a complaint of febrile sei-zure. Their findings based on 330 charts from the
children’s ED and 125 charts from the adult centers showed that patients presenting to the general ED were more likely to have a lumbar puncture, receive parenteral antibiotics, and be admitted or trans-ferred. Our findings show a similar trend in an increased reliance on chest radiographs, CSF evalu-ation, and an increased antibiotic usage among gen-eral ED physicians. Furthermore, we noted a de-creased hospitalization rate of children seen at the general ED with no sign that these children were transferred to admission elsewhere. This finding re-mains unexplained.
Agreement with the practice guidelines was low in both groups of physicians. Others have documented low compliance with these guidelines by other phy-sicians in a variety of practice settings.13–16Although
these guidelines were developed with a formal evi-dence-based approach, a Delphian approach was used to generate recommendations where existing data were weak or missing. A recent review by Bar-aff17 has suggested revisions to the guidelines
gen-erated in 1993 to address some of the changes in the epidemiology of occult bacteremia that have oc-curred over the past decade. Studies looking at out-comes of patients managed in ways that differ from the guidelines are necessary to confirm or reject the efficacy of alternate management approaches.
It should be noted that presentations that were suggestive of a classic viral illness were still included in this study. Pediatric emergency physicians were more likely to formally diagnose these illnesses than were the general ED physicians. Although it is un-derstandable that many physicians will limit their diagnostic work-up in a febrile child with signs of a classic viral illness, we found it intriguing that such a significant difference in the frequency of such di-agnoses existed between these 2 groups of physi-cians. As the practice guidelines only apply to the management of children with fever without source, we omitted these children from analysis regarding management.
CONCLUSION
Significant differences in the management of the young child with fever and no source exist between PEMPs and GEMPs. These variations affect both cost and standard of care. The use of the pneumococcal vaccine for the prevention of invasive infection re-lated to Streptococcus pneumoniae may radically change the approach to this clinical problem. Future studies assessing whether differences in manage-ment approaches continue and the effect of these potential differences on patient outcomes are needed to refine existing guidelines for the future.
ACKNOWLEDGMENTS
We thank Peter Ermis for help with data entry and analysis and Kimberley Kelly for help with manuscript preparation.
REFERENCES
1. Procop GW, Hartman J, Sedor F. Lab tests in evaluation of acute febrile illness in pediatric emergency room patients.Am J Clin Pathology. 1997; 107:114 –121
2. Leduc DG, Pless IB. Pediatricians and general practitioners: a compar-ison of the management of children with febrile illness.Pediatrics. 1982; 70:511–515
3. Schweich P, Smith K, Dowd D, Walkley E. Pediatric emergency medi-cine practice patterns: A comparison of pediatric and general emer-gency physicians.Pediatr Emerg Care. 1998;14:89 –94
4. Wittler RR, Cain K, Bass JW. A survey about management of febrile children without source by primary care physicians.Pediatr Infect Dis J. 1998;17:271–277
5. Baraff LJ. Management of the febrile child: a survey of pediatric and
emergency medicine residency directors.Pediatr Infect Dis J. 1991;10: 795– 800
6. Baraff LJ, Bass JW, Fleisher GR, et al. Practice guideline for the man-agement of infants and children 0 to 36 months of age with fever without source.Pediatrics. 1993;92:1–12 andAnn Emerg Med.1993;22: 1198 –1210
7. Green SM, Rothrock SG. Evaluation styles for well-appearing febrile children: Are you a “risk minimizer or a test minimizer”?Ann Emerg Med. 1999;33:211–214
8. Long S. Antibiotic therapy in febrile children: “best laid plans.”J Pediatr. 1994;124:585–588
9. Wald E, Dashefsky B. Cautionary note on the use of empiric ceftrizxone for suspected bacteremia.Am J Dis Child. 1991;145:1359 –1361 10. Scribano PV, Baker MD, Ludwig S. Factors influencing termination of
resuscitative efforts in children: a comparison of pediatric emergency medicine and adult emergency medicine physicians.Pediatr Emerg Care. 1997;13:320 –324
11. Krauss B, Zurakowki D. Sedation patterns in pediatric and general community hospital emergency departments.Pediatr Emerg Care. 1998; 14:99 –103
12. Hampers LC, Trainor JL, Listernick R, et al. Setting-based practice variation in the management of simple febrile seizures.Acad Emerg Med. 2000;7:21–27
13. Kramer MS. Management of the young febrile child: a commentary on recent practice guidelines.Pediatrics. 1997;100:128 –134
14. Schringer DL. Clinical guidelines in the setting of incomplete evidence. Pediatrics. 1997;100:136
15. Bauchner H, Pelton SI. Management of the young febrile child: a con-tinuing controversy.Pediatrics. 1997;100:128 –134
16. Young PC. The management of febrile infants by primary-care pedia-tricians in Utah: comparison with published practice guidelines. Pedi-atrics. 1995;95:623– 627
17. Baraff LJ. Management of fever without source in infants and children. Ann Emerg Med. 2000;36:602– 614
“Few things are harder to put up with than the arrogance of a good example.”
DOI: 10.1542/peds.108.2.354
2001;108;354
Pediatrics
Jon D. Mason
Daniel J. Isaacman, Kimberly Kaminer, Hari Veligeti, Michael Jones, Paris Davis and
Emergency Medicine Physicians Managing Fever in Young Children
Comparative Practice Patterns of Emergency Medicine Physicians and Pediatric
Services
Updated Information &
http://pediatrics.aappublications.org/content/108/2/354 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/108/2/354#BIBL This article cites 17 articles, 5 of which you can access for free at:
Subspecialty Collections
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.108.2.354
2001;108;354
Pediatrics
Jon D. Mason
Daniel J. Isaacman, Kimberly Kaminer, Hari Veligeti, Michael Jones, Paris Davis and
Emergency Medicine Physicians Managing Fever in Young Children
Comparative Practice Patterns of Emergency Medicine Physicians and Pediatric
http://pediatrics.aappublications.org/content/108/2/354
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.