Table of Contents
I. Introduction
A. Overview of Diabetes and DSME B. Diabetes and DSME in North Carolina
II. North Carolina Diabetes Education Recognition Program A. History and Goals of NCDERP
B. Reach, Costs, and Outcomes of NCDERP III. Challenges and Strategies for NCDERP
IV. Conclusion V. References
VI. Appendix: List of Acronyms
Note: This paper follows the format of a manuscript to be submitted to Preventing Chronic Disease, as a special topic. To submit this paper, among the required revisions would be shortening the length to 2500 words.
Abstract: Diabetes is a huge and costly epidemic in North Carolina. Effective treatment for diabetes includes Diabetes Self-Management Education (DSME). North Carolina’s Diabetes Education
Section I. Introduction
A. Overview of Diabetes and Diabetes Self-Management Education
Diabetes Mellitus is a health epidemic in our country with significant health and financial implications. Diabetes is “a group of diseases marked by high levels of blood glucose resulting from problems in how insulin is produced, how insulin works, or both.” In 2012, 29.1 million people or 9.3% of the U.S. population had diabetes. Health complications associated with diabetes include heart disease, stroke, blindness, kidney disease, and non-traumatic lower limb amputations, among others (1). The average medical expenditures among individuals diagnosed with diabetes are 2.3 times higher than the expenditures among those without diabetes, after adjusting for population age and sex differences (2).
Effective management of diabetes requires more than standard medical care, as Konen (3) explains: “People with diabetes need education and steady support...Today, self-management education is such a critical part of diabetes care that medical treatment without it is considered inadequate.” Diabetes self-management education (DSME) is an evidence-based strategy defined as “the ongoing process of facilitating the knowledge, skill, and ability necessary for diabetes self-care...The overall objectives of DSME are to support informed decision-making, self-care behaviors, problem-solving and active collaboration with the health care team and to improve clinical outcomes, health status, and quality of life,” (4).
The Centers for Medicare and Medicaid Services (CMS), as well as many other insurance
providers, will reimburse for DSME only when the program provider is accredited by either the American Diabetes Association (ADA) or the American Association of Diabetes Educators (AADE). Each has a formal application process that requires supporting documentation, fees, annual reports, and audits (5).
B. Diabetes and DSME in North Carolina
In North Carolina, diabetes is the seventh leading cause of death and decreases life expectancy by up to 15 years. The annual health care costs for this epidemic in North Carolina could surpass $17 billion by 2025 (3). The percent of people who responded “yes” to the question “Has a doctor, nurse, or other health professional ever told you that you have diabetes?” was 11.4% statewide in 2013. The burden was higher in specific groups: 12.9% of rural county residents responded yes, versus 9.7% of non-rural county residents. Among those North Carolinians whose household income is less than $15,000 annually, 17.9% responded yes (6).
Figure 1. Diabetes prevalence and location of diabetes self-management programs in North Carolina. Source: CCCPH 2014 (8).
Section II. North Carolina Diabetes Education Recognition Program
A. History and goals of NCDERP
In order to help meet the need for quality, comprehensive DSME, the North Carolina Division of Public Health (NC DPH) founded the North Carolina Diabetes Education Recognition Program
(NCDERP) in 2006. Its purpose is: “to increase access to self-management training for people with diabetes across the state, while providing a mechanism for reimbursement to local health departments.” (9). NCDERP is a statewide umbrella program, consisting of NC DPH, which maintains the accreditation and provides technical assistance and training to local staff; the NC Public Health Foundation, which facilitates program administration; and local health departments (LHDs), which provide DSME services (8). This is the first such statewide program in the U.S. The goal is that “by increasing the infrastructure of local health departments, the program ensures that DSME is available to people who have no other resources for education. The program increases the quality of patient care by providing evidence-based guidelines for diabetes care and education. In addition, the program implements systems change, so that persons with diabetes receive adequate and vital education earlier and more consistently, to increase quality of life and decrease complications,” (9).
B. Reach, costs, and outcomes of NCDERP
The annual cost to NC DPH of administering NCDERP, as of October 2014:
Staff administration: $78,509.63 (calculated as the fraction of time that each of two NC DPH staff members spends on NCDERP, multiplied by their salaries)
Regional consultants: $60,000 ($12,000 for each of the five regional consultants) Billing specialist: $15,000 (this amount will increase to $30,000 in 2015)
Total: $153,509.63. In addition, NCDERP in most cases pays the ADA recognition fees, which are $1100 per LHD, plus $100 for each additional site associated with an LHD, for a four year cycle (12).
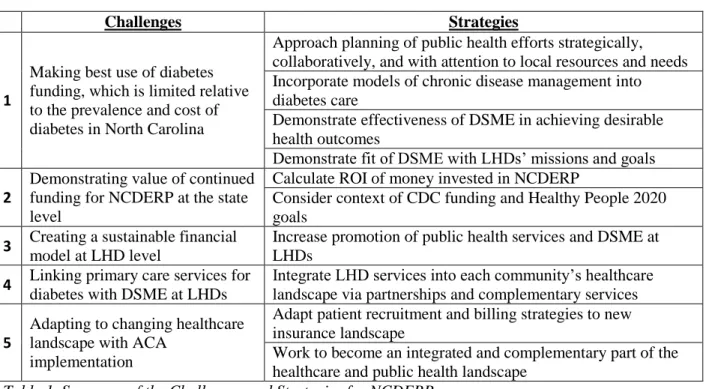
Section III. Challenges and Strategies for NCDERP
Challenges Strategies
1
Making best use of diabetes funding, which is limited relative to the prevalence and cost of diabetes in North Carolina
Approach planning of public health efforts strategically, collaboratively, and with attention to local resources and needs Incorporate models of chronic disease management into diabetes care
Demonstrate effectiveness of DSME in achieving desirable health outcomes
Demonstrate fit of DSME with LHDs’ missions and goals
2
Demonstrating value of continued funding for NCDERP at the state level
Calculate ROI of money invested in NCDERP
Consider context of CDC funding and Healthy People 2020 goals
3 Creating a sustainable financial
model at LHD level
Increase promotion of public health services and DSME at LHDs
4 Linking primary care services for
diabetes with DSME at LHDs
Integrate LHD services into each community’s healthcare landscape via partnerships and complementary services
5
Adapting to changing healthcare landscape with ACA
implementation
Adapt patient recruitment and billing strategies to new insurance landscape
Work to become an integrated and complementary part of the healthcare and public health landscape
Table 1. Summary of the Challenges and Strategies for NCDERP
Challenge 1: Making best use of diabetes funding, which is limited relative to the prevalence and cost of diabetes in North Carolina
Strategy 1A: Approach planning of public health efforts strategically, collaboratively, and with attention to local resources and needs
We can draw guidance from the community strategic planning tool Mobilizing for Action through Planning and Partnerships (MAPP). MAPP was created by NACCHO and the CDC over a four year period of collaborative research and development. Parts of this process could be lessons for NCDERP: using content expertise, support from leadership, and effective technology and communication
mechanisms; a collaborative environment with mutual respect and trust among participants; and diversity in participants’ perspectives. Other important components of strategic planning described by MAPP include assessing the community’s health and the current public health systems; developing partnerships and strategies; and performing evaluations after action is taken (13).
Strategy 1B: Incorporate models of chronic disease management into diabetes care
In crafting an effective strategy for chronic disease treatment, we need to look beyond the traditional medical model. Primary care practice was largely designed to treat acute problems, via diagnosis and treatment of symptoms; however, patients with chronic illness have different needs, particularly for education and training to self-manage their condition on a daily basis (14). The NC DPH can use chronic disease management models both in offering DSME at LHDs, and also in working with primary care providers to inform how to better care for patients with diabetes. LHDs could partner with local primary care providers to share strategies and resources for implementing chronic disease
management with patients. If put into practice, this use of chronic disease management strategies would shift the focus of diabetes care from treating the acute complications of diabetes (for example, a physician tending to a patient’s foot ulcer) to training the patients with diabetes, early on, about how to prevent and manage potential complications on their own (for example, showing patients how to check their feet daily at home). In doing so, healthcare providers could help to prevent some of the costly complications that contribute to the more than $5 billion spent on diabetes medical care and lost productivity in North Carolina (3).
Strategy 1C: Demonstrate effectiveness of DSME in achieving desirable health outcomes Another strategy for dealing with limited public health funding is to choose a type of diabetes care that is effective and cost-effective, particularly in the setting of an LHD. We will argue here that DSME is effective in achieving specific health-improvement outcomes among participants. Currently there is little data demonstrating the outcomes of DSME offered by LHDs; this is an area in which more outcome data from NCERP could help build a case for effectiveness and more funding.
Jack Jr (15) reviewed eight studies on DSME, and concluded that the studies demonstrate DSME’s effectiveness in improving intermediate- and short-term outcomes: DSME had favorable effects on HbA1C, cholesterol, body mass index, blood pressure, and fasting glucose. Strine (16) looked at the association of DSME with preventive health practices and behaviors among 22,682 persons with type 2 diabetes. Individuals with type 2 diabetes who had attended at least one DSME course were significantly more likely than those without training to be physically active, have an annual eye exam and flu vaccine, check their blood sugar daily, and have a physician or other health professional check their feet and their HbA1C level. Strine concludes that DSME is valuable in encouraging health practices that could prevent or delay complications of type 2 diabetes
showed lower cost patterns than those who had not; further, patients who had multiple episodes of DSMT were more likely to receive the recommended medical care and to take the recommended diabetic
prescriptions. This resulted in positive clinical quality outcomes and cost savings, with a dose-response effect of repeated DSMT encounters. The authors conclude that the DSME/T has positive benefits that outweigh the costs of providing the services.
Strategy 1D: Demonstrate fit of DSME with LHDs’ missions and goals
In making best use of limited funding to address diabetes, we must make sure that public health agencies are offering services that are appropriate to their mission. The Ten Essential Public Health Services describe the responsibilities that individuals should reasonably expect their LHD to fulfill. Two of these ten services are particularly applicable to DSME: (3) “Inform, educate, and empower people about health issues,” and (7) “Link people to needed personal health services and assure the provision of health care when otherwise unavailable” (18). If a community does not have enough DSME program offerings accessible to all in the community, then the LHD’s role is to identify ways to close this gap, possibly by offering DSME at the health department. The role of linkage may be especially important here; many patients with diabetes do not see primary providers at LHDs, thus connecting with primary providers in the community becomes especially important (see Challenge 4). Birdsell (19) describes the fit of DSME with LHDs further: “Local health departments are often viewed as the experts when dealing with public health and have staff easily accessible to provide the program without hiring additional staff. Health departments know the community and the population and are committed to providing this
education.” In 2011, 45% of the 2794 LHDs in the U.S. provided screening for diabetes, and 53% of LHDs provided population-based primary prevention services for the prevention of chronic disease (20).
Challenge 2: Demonstrating value of continued funding for NCDERP at the state level
As described in the introduction, NC DPH invests money and staff time into NCDERP. Does this investment of state public health money have demonstrable value, and does this use of money fit with state public health directives?
Strategy 2A: Calculate ROI of money invested in NCDERP
One analysis looked specifically at NCDERP’s return on investment (ROI), conducted by Chenoweth (21). The study used data from 310 NCDERP participants from 18 counties, comparing pre- and post-participation HbA1c values. Results showed that participants lowered their level of excess diabetes risk by more than 17% of their baseline level. Applying this risk reduction to the per capita annual medical cost for diabetes (estimated to be $2647), the cost-avoidance of the NCDERP program for these 310 participants was $140,892. Using information on the costs of developing and operating
NCDERP, the total programming costs for the 310 participants was estimated at $116,250 annually. Comparing these benefit and cost estimates yields a +21% ROI. Thus, this analysis showed that NCDERP generated $1.21 in medical care cost-avoidance benefits for every $1 spent on the program, implying a favorable ratio of benefits to costs in the time frame considered (21).
Strategy 2B: Consider context of CDC funding and Healthy People 2020 goals
set in 2010 by the U.S. Department of Health and Human Services. Healthy People 2020 establishes benchmarks and monitors progress in many areas of national health, including diabetes. Goal D-14 of Healthy People 2020 is, “Increase the proportion of persons with diagnosed diabetes who receive formal diabetes education.” The baseline is 56.8% of adults aged 18 years and older with diagnosed diabetes who reported they ever received formal diabetes education in 2008; the target is to increase this to 62.5%. In North Carolina, this baseline was only 55.5% (22).
Beginning with a new Funding Opportunity Announcement (FOA) in 2013, the CDC changed the way it provides funding to state chronic disease programs. This FOA, called the 1305 grant, “supports statewide implementation of cross-cutting approaches to promote health and prevent and control chronic diseases and their risk factors,” (22). At NC DPH, this grant consolidates the efforts and funding of four previous branches: Diabetes Prevention and Control, Heart Disease and Stroke Prevention, School Health, and Physical Activity and Nutrition. The 1305 grant activity is carried out under a new branch,
Community & Clinical Connections for Prevention & Health. This branch emphasizes connecting community and clinical health services. Offering DSME at LHDs, if done in partnership with local clinical services, can be a great example of this linkage (see Challenge 4).
Challenge 3: Creating a sustainable financial model at LHD level
A huge challenge for NCDERP has been navigating billing and payment strategies to create a sustainable financial model (19). The payer mix is crucial, as the income from insured patients must compensate for the cost of treating patients who are uninsured or indigent (9).
In a report summarizing interviews with seventeen NCDERP sites, budgetary and billing data were analyzed, revealing that none of the seventeen programs had achieved the goal of sustaining
themselves through billing and reimbursement. In fact, “The highest level of cost recovery being achieved by a LHD is at 33%...Half of the programs were recovering less than 5% of their costs through billing.” Most of the LHD-based DSME programs relied on county allocations to the LHD as their primary means of covering program costs. This reliance on external funding underscores the importance of recognizing and quantifying the value that these DSME programs provide to the community in healthcare cost savings (24).
Another aspect of the challenge for financial stability is that some providers and patients,
particularly those with health insurance, have stigma associated with visiting LHDs (19). This stigma may occur because community members view the LHD as a place for those without any other treatment options, rather than as a provider of services on par with other health professionals. Potential patients who perceive such stigma may be hesitant to go to the LHD for DSME, due to concerns about what others would think of them.
Strategy 3: Increase promotion of public health services and DSME at LHDs
Promoting the importance and achievements of public health programs, both qualitative stories and quantitative outcomes, can be crucial in securing public support, legislative backing, and ongoing funding. The evidence is there, as research shows that public health dollars are good investments. A study by Mays (25) looked at changes in spending by public health agencies over thirteen years and the
activities is a wise health investment, particularly in low resource areas or those with historically low levels of public health spending (25). The NCDERP’s umbrella model of facilitating for LHDs to bill for DSME builds capacity at the local level to provide DSME for both uninsured and underinsured
individuals (11). The key here is to find ways to get this message out, though marketing, networking, or promotional activities. Public health agencies cannot take it as a given that the public understands the value of their work. LHDs could use inexpensive channels such as radio PSAs or social media to broadcast the value and achievements of public health work. In particular, advertising DSME services at the LHD, and sharing patient success stories, could be valuable in attracting new patients.
Challenge 4: Linking primary care services for diabetes with DSME at LHDs
The ability of NCDERP to receive patient referrals, create a sustainable payer mix, retain patients, and earn a positive reputation largely hinges on how well LHDs link with health care providers and organizations. One challenge is ensuring physicians refer patients to local NCDERP branches, which is crucial for building up clientele. Stigma, as discussed earlier, may be an issue in getting providers to refer to LHDs; the strategy of a promotional campaign is thus also relevant to this challenge.
Strategy 4: Integrate LHD services into each community’s healthcare landscape via partnerships and complementary services
A local health department is only one player in a community’s healthcare system. In order for DSME at LHDs to be accessible, impactful, and sustainable, the program must have productive
relationships with other elements of the local healthcare scene. There are two reasons that integration into the local health care system is important: (1) providing complete care to patients, and (2) financial sustainability of the DSME program.
As Bovbjerg (26) states, “Partnering goes beyond simple contracting out for specialized services or ones that can be accomplished more efficiently by others...It means working across agencies and sectors to develop strategies and to implement activities or initiatives.” LHDs can think about partners broadly, including governmental organizations, nonprofits, private healthcare providers, schools, and commercial enterprises. A single LHD cannot meet all potential needs of clients (which may include mental health, drug abuse, or economic challenges), so it is important that a DSME program has connections to refer patients to other services as needed. These cross agency referrals can provide improved patient care and also help both agencies with patient recruitment. Bovbjerg gives the example of how public health and clinical medical services could collaborate through public health screenings by referring patients to private caregivers, while caregivers look to public health providers to treat behavioral issues or other problems not well suited to the medical model of service provision. NC DPH has the potential to play a crucial role here in facilitating dialogue and cooperation among LHDs, private providers, and others. For example, the state could organize regional diabetes summits, or distribute training materials to LHDs focused on community outreach and clinical connections.
Challenge 5: Adapting to changing healthcare landscape with ACA implementation
The Affordable Care Act (ACA), passed in 2010, expands healthcare coverage to many who were previously uninsured, through the expansion of Medicaid in many states (though North Carolina opted out of this expansion), tax subsidies for insurance, and health insurance exchanges. Also, the ACA
Strategy 5A: Adapt patient recruitment and billing strategies to new insurance landscape
As previously uninsured individuals obtain insurance, LHDs may be able to improve their payer mix by receiving insurance reimbursement for providing services to these patients. Further, public health agencies may be important in helping the newly insured to navigate the insurance landscape. Finally, it is important to remember that there will still be many North Carolinians without health insurance; LHDs will continue to play an important role in providing care to this population.
Strategy 5B: Work to become an integrated and complementary part of the healthcare and public health landscape
As federal funding for public health prevention efforts focuses increasingly on clinical-community connections, it is important for public health agencies to embrace the interconnected healthcare landscape, and to be proactive about forming relationships. When two agencies provide redundant services in the same small community, resources are wasted and program sustainability suffers. When health services are offered in isolation from each other, patients and providers must both work harder to find each other. LHDs must look to the future of public health, considering how to best serve the needs of the community going forward and how to partner with other community organizations to
accomplish common goals.
Section IV. Conclusion
Currently, there are some important unanswered questions about the impact and sustainability of NCDERP. Future analysis should include more rigorous tracking of the costs and outcome measures of NCDERP sites; the accessibility of DSME in the counties of North Carolina, including where more DSME may be needed at LHDs; how much the current NCDERP program sites could expand, or whether they are providing services to capacity; and surveys of patients with diabetes and their doctors, to
determine what they are looking for in DSME programs. As it decides how to move forward, NCDERP could also conduct a SWOT analysis, which is an accounting of strengths, weaknesses, opportunities, and threats to the program.
References
1. Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States, 2014. Atlanta, GA: U.S. Department of Health and Human Services; 2014.
2. American Diabetes Association. "Economic costs of diabetes in the US in 2012." Diabetes Care 36.4 (2013): 1033-1046.
3. Joseph Konen and Joyce Page. The State of Diabetes in North Carolina, 72 N.C. MeD. J 375 (2011); National Diabetes Statistics, National Diabetes Information Clearinghouse (NDIC) (2011).
4. Funnell, Martha M., et al. "National standards for diabetes self-management education." Diabetes care 34.Supplement 1 (2011): S89-S96.
5. "Diabetes DSME Resource." National Association of Chronic Disease Directors. 1 Jan. 2013. Web. 27 Oct. 2014. <http://www.chronicdisease.org/?page=DiabetesDSMEresource>.
6. N.C. State Center for Health Statistics: 2013 BRFSS survey results: North Carolina: Diabetes: Have you ever taken a course or class in how to manage your diabetes yourself? Available from http://www.schs.state.nc.us/data/brfss/2013/nc/all/topics.htm#d. Accessed 24 October 2014. 7. County Specific Snapshots for NC Medicaid Services. NC Department of Health and Human
Services, 2011. Web. <http://www.ncdhhs.gov/dma/countyreports/>.
8. Community and Clinical Connections for Prevention and Health Branch, Chronic Disease and Injury Section, Division of Public Health, NC Department of Health and Human Services. Selected Evidence-Based Strategy Overview for Local Health Departments to Address Diabetes. June 2014 <http://publichealth.nc.gov/lhd/cha/docs/Diabetes-EBSelectedStrategy-June2014.pdf>. 9. Rinker, Joanne, Laura Emerson Edwards, and Debbie Widener. "Facilitating Self-Management of
Diabetes Through Education." NC Med J 72.5 (2011): 387-389. 10. Kolbe, Mary Bea. Email to the author. 31 October 2014.
11. Rinker, Joanne, and Marti Wolf. "NC Diabetes Education Recognition Program: ADA Recognition for a Combined Program at Local Health Departments and Community Health Centers in North Carolina." Clinical Diabetes 30.3 (2012): 110-114.
12. Reese, April. Email to the author. 5 November 2014.
13. Corso, Liza C., Paul J. Wiesner, and Patrick Lenihan. "Developing the MAPP community health improvement tool." Journal of Public Health Management and Practice 11.5 (2005): 387-392. 14. Wagner, Edward H. "Chronic disease management: what will it take to improve care for chronic
illness?." Effective clinical practice: ECP 1.1 (1997): 2-4.
15. Jack Jr, Leonard. "Diabetes self-management education research." Disease Management & Health Outcomes 11.7 (2003): 415-428.
16. Strine, Tara W., et al. "The impact of formal diabetes education on the preventive health practices and behaviors of persons with type 2 diabetes." Preventive medicine 41.1 (2005): 79-84.
17. Duncan, Ian, et al. "Assessing the value of the diabetes educator." The Diabetes Educator 37.5 (2011): 638-657.
19. Birdsell, Maggi; Miller, Jennifer; Potru, Parvati; and McVicker, Monica. “Sustainability and Quality Improvement for the North Carolina Diabetes Education Recognition Program: Business Plan.” North Carolina Diabetes Education Recognition Program (2011).
20. Carda-Auten, Jessica, and Julie Nelson Ingoglia. "News From NACCHO: Local Health Departments' Response to the Diabetes Epidemic." Journal of Public Health Management and Practice 17.2 (2011): 190-192.
21. North Carolina Diabetes Prevention and Control Program (2012). Benefit--‐Cost Analysis. Department of Health & Human Services (conducted by Chenoweth & Associates, Inc.) 22. US Department of Health and Human Services, and Office of Disease Prevention and Health
Promotion. "Healthy People 2020. Washington, DC." (2012).
23. "State Public Health Actions to Prevent and Control Diabetes, Heart Disease, Obesity and Associated Risk Factors and Promote School Health (1305)." Centers for Disease Control and Prevention. Centers for Disease Control and Prevention, 16 July 2014. Web. 21 Nov. 2014. <http://www.cdc.gov/chronicdisease/about/statepubhealthactions-prevcd.htm>.
24. “Key Themes from Interviews with 17 Programs”, a report prepared for Kate B. Reynolds Charitable Trust and Northwest Community Care Network by Doug Easterling and Lucinda Brogden.
25. Mays, Glen P., and Sharla A. Smith. "Evidence links increases in public health spending to declines in preventable deaths." Health Affairs 30.8 (2011): 1585-1593.
26. Bovbjerg, Randall R., Barbara A. Ormond, and Timothy A. Waidmann. "What Directions for Public Health under the Affordable Care Act?." Washington, DC: Urban Institute. http://www. urban. org/publications/412441. html (2011).
27. "Prevention and Public Health Fund." Open Government at HHS. U.S. Department of Health and Human Services, 2014. Web. 20 Nov. 2014.
Appendix: List of Acronyms AADE: American Association of Diabetes Educators
ADA: American Diabetes Association
BRFSS: Behavioral Risk Factor Surveillance Survey CDC: Centers for Disease Control and Prevention
US DHHS: United States Department of Health and Human Services DSME: Diabetes Self-Management Education
DSMT: Diabetes Self-Management Training FOA: Funding Opportunity Announcement FTE: Full time equivalent
HbA1C: Hemoglobin A1C. This is a blood test that measures the percent of glycated hemoglobin in an individual’s blood, which is a marker of blood sugar control over the previous three months. HbA1C values of 6.5 mmol/mol or lower are considered good targets for patients with diabetes.
LHD: Local Health Department
MAPP: Mobilizing for Action through Planning and Partnerships (community strategic planning tool developed by the CDC and NACCHO)
NACCHO: National Association of City and County Health Officials NC DERP: North Carolina Diabetes Education Recognition Program
NC DPH: North Carolina Division of Public Health, which is part of the North Carolina Department of Health and Human Services