Original
Article
Serum Total and HDL-Cholesterol
in Ischemic and Hemorrhagic
Stroke
Abstract
Objective: To determine frequency of dyslipidemia (hypercholesterolemia or low HDL-Cholesterol) among strokes patients and compare frequency of dyslipidemia between ischemic and hemorrhagic strokes patients.
Study design: Descriptive case series
Setting and Duration of Study: Department of Medicine, Holy Family Hospital, Rawalpindi, from Jan. 2013 to Dec. 2013.
Materials and Methods: 370 consecutive patients of stroke, both males and females, above 18 years of age were included in the study. Patients on lipid lowering therapy were excluded. Informed consent was obtained and data was collected on a written proforma. Serum samples for total cholesterol and HDL-C were obtained on the morning after overnight fast and CT scan brain was performed.
Results: Based on Brain CT scan findings, 370 patients (229 females and 141 males) were divided into two groups, Ischemic stroke (190) and Hemorrhagic stroke (180). Mean age (yrs) of stroke patients was 58.1+15. Mean total cholesterol level (mg/dl) was 173.8+66.7, whereas mean HDL-cholesterol level was 40.0+13.2. Out of 370 patients, 88 (23.7%) patients presented with hypercholesterolemia (serum TC > 200 mg/dl) in which frequency of hypercholesterolemia was significantly higher (p-value 0.009) in patients with Ischemic stroke as compared to hemorrhagic stroke (29.4% Vs 17.8%).
Similarly, out of 370 patients, 136 (36.7%) patients presented with reduced HDL-C levels (serum HDL-C < 35 mg/dl). Ischemic stroke patients had significantly more frequency (p-value 0.005) of reduced HDL-C than hemorrhagic stroke patients (43.7% Vs 29.4%). Out of 370 patients, 18 (4.9%) patients had both hypercholesterolemia and low HDL. Frequencies for other modifiable risk factors were 74.6% with hypertension, 28.3% with IHD, 20.5% diabetic and 17.8% cigarette smokers.
Conclusions: Ischemic stroke patients had significantly higher frequency of hypercholesterolemia and reduced HDL-Cholesterol levels than patients of hemorrhagic stroke. Screening dyslipidemia for high risk patients for stroke and lipid lowering therapy are recommended as preventive measures.
Key words: Stroke, Total Cholesterol, HDL-Cholesterol
Muhammad Nazim Khan* Hina Dilruba Khan** Masood Ahmad*** Muhammad Umar****
*Assistant Professor of Surgery Department of Surgery
RIHS (Bahria University), Islamabad.
**Post Graduate Student Medical Unit-I,
Holy Family Hospital, Rawalpindi ***Associate Professor of Medicine Medical Unit-I,
Holy Family Hospital, Rawalpindi ****Professor of Medicine, Medical Unit-I,
Holy Family Hospital, Rawalpindi
Address for Correspondence
Dr. Muhammad Nazim Khan Assistant Professor of Surgery Department of Surgery
RIHS (Bahria University), Islamabad.
mnazimkhan@yahoo.com
Introduction
Stroke, also referred to as cerebrovascular accident (CVA) is the rapid loss of brain function due to disturbance in the blood supply to the brain. This can be
due to ischemia caused by blockage
(thrombosis, arterial embolism) or a hemorrhage.1 Stroke is a global health problem. It is the leading cause of adult disability and the second leading cause of
mortality worldwide.2 Between 1990 and 2010 the number of strokes decreased by approximately 10% in the developed world and increased by 10% in the developing world.3 In the United States, stroke is a leading cause of disability, and recently declined from the third leading to the fourth leading cause of death.4 There are no sizeable community based epidemiologic studies on stroke from Pakistan. A community based study on Pushtoon people residing in Karachi reported a prevalence of 4.8%, both for males and females.5
Stroke is a medical emergency and can cause permanent neurological damage and death. There are various risk factors associated with stroke such as age, gender, race and ethnicity. There are also modifiable risk factors like hypertension, cardiac disease, diabetes mellitus, dyslipidemia, smoking, alcohol abuse, obesity, carotid stenosis, transient ischemic attack.
Dyslipidemia is abnormal amounts of the lipids in the blood such as elevated plasma cholesterol and triglycerides or a low high-density lipoprotein (HDL) level that contributes to the development of atherosclerosis. Dyslipidemia can lead to symptomatic vascular disease, including coronary artery disease (CAD), stroke, and peripheral arterial disease. A linear relation probably exists between lipid levels and cardiovascular risk. However, the association between dyslipidemia and stroke may not be as straight forward as for coronary heart disease. Among various components of lipid profile, serum total cholesterol (TC) and HDL-C have attracted more attention.Large epidemiological studies in which ischemic and hemorrhagic strokes were distinguishable, have shown a modest association of elevated total cholesterol6 as well as low HDL-C with increased risk of ischemic stroke.7
Serum lipid levels have an established effect on short term morbidity due to strokes. It is important to evaluate the difference in serum lipid levels in subtypes of strokes to guide lipid-lowering therapy which can reduce incidence of stroke and related morbidity by adapting primary and secondary preventive measures.
The objective of the study was to determine frequency of dyslipidemia among strokes patients and to compare frequency of dyslipidemia (hypercholesterolemia and low HDL-Cholesterol) between ischemic and hemorrhagic strokes patients.
Materials and Methods
The study was conducted at In-patient department of Medical Unit-I, Holy Family Hospital, Rawalpindi from
Jan. 2013 to Dec. 2013. According to WHO sample size calculator, 370 stroke patients were included in the study, based on consecutive non-probability sampling technique.
Inclusion criteria: Patients, both males and females, above 18 years of age, admitted with diagnosis of stroke were included in the study.
Exclusion Criteria: Patients on lipid lowering therapy were excluded from study.
Operational Definitions: Stroke was diagnosed on clinical assessment of neurological deficit, confirmed and subdivided into two groups, Ischemic and hemorrhagic stroke, based on findings of CT scan brain without contrast injection. Dyslipidemia was diagnosed on hypercholesterolemia and reduced HDL-Cholesterol only. Cut off levels were serum Total Cholesterol >200 mg/dl and serum HDL-Cholesterol <35 mg/dl respectively. Other lipid fractions like triglyceride, LDL and VLDL were not studied.
Data Collection and Analysis Procedure: Informed consent was obtained from all participating patients. Demographic data was collected on a written proforma. Past medical and personal history for cigarette smoking, arterial hypertension, Diabetes mellitus and ischemic heart disease was sought. Serum samples were obtained after 8 hours of overnight fasting, on the next morning after admission. Data was analyzed using SPSS version 16. Chi-square test was used to compare frequency of hypercholesterolemia and low HDL-cholesterol in Ischemic and Hemorrhagic stroke groups. P-value <0.05 was taken as significant.
Results
A total of 370 patients of stroke were enrolled in the study according to the inclusion and exclusion criteria of the study. Age of patients ranged from 20 to 95 years, in which mean + standard deviation of age (years) was 58.11+15.292. Gender wise 229 (61.9%) were females and 141 (38.1%) males patients.
Out of 370 patients, mean cholesterol level (mg/dl) was 173.84+66.784 whereas mean HDL-cholesterol level was 40.09+13.285, as shown in Table No. I.
Based on CT Brain findings of 370 stroke patients, the frequency of Ischemic Stroke was 190 (51.4%) and Hemorrhagic Stroke was 180 (48.6%) respectively. Out of 370 patients, 88 (23.7%) patients presented with hypercholesterolemia (serum TC > 200 mg/dl). Frequencies of hypercholesterolemia in Ischemic and
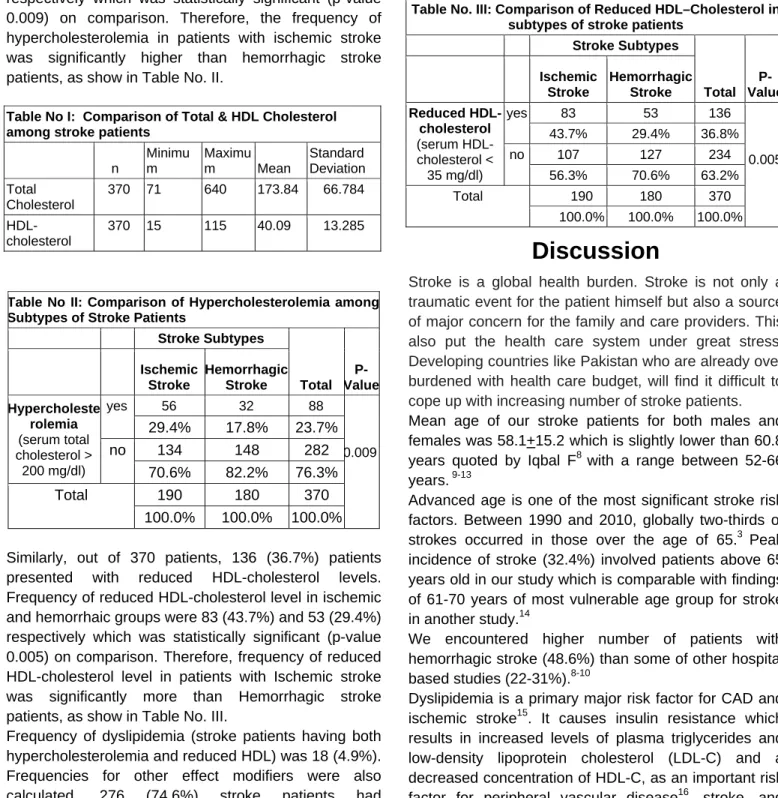
respectively which was statistically significant (p-value 0.009) on comparison. Therefore, the frequency of hypercholesterolemia in patients with ischemic stroke was significantly higher than hemorrhagic stroke patients, as show in Table No. II.
Table No II: Comparison of Hypercholesterolemia among Subtypes of Stroke Patients
Stroke Subtypes Total P-Value Ischemic Stroke Hemorrhagic Stroke Hypercholeste rolemia (serum total cholesterol > 200 mg/dl) yes 56 32 88 0.009 29.4% 17.8% 23.7% no 134 148 282 70.6% 82.2% 76.3% Total 190 180 370 100.0% 100.0% 100.0% Similarly, out of 370 patients, 136 (36.7%) patients presented with reduced HDL-cholesterol levels. Frequency of reduced HDL-cholesterol level in ischemic and hemorrhaic groups were 83 (43.7%) and 53 (29.4%) respectively which was statistically significant (p-value 0.005) on comparison. Therefore, frequency of reduced HDL-cholesterol level in patients with Ischemic stroke was significantly more than Hemorrhagic stroke patients, as show in Table No. III.
Frequency of dyslipidemia (stroke patients having both hypercholesterolemia and reduced HDL) was 18 (4.9%). Frequencies for other effect modifiers were also calculated. 276 (74.6%) stroke patients had hypertension, 105 (28.3%) ischemic heart disease (IHD), 76 (20.5%) diabetes mellitus and 66 (17.8%) patients were cigarette smokers.
Discussion
Stroke is a global health burden. Stroke is not only a traumatic event for the patient himself but also a source of major concern for the family and care providers. This also put the health care system under great stress. Developing countries like Pakistan who are already over burdened with health care budget, will find it difficult to cope up with increasing number of stroke patients.
Mean age of our stroke patients for both males and females was 58.1+15.2 which is slightly lower than 60.8 years quoted by Iqbal F8 with a range between 52-66 years. 9-13
Advanced age is one of the most significant stroke risk factors. Between 1990 and 2010, globally two-thirds of strokes occurred in those over the age of 65.3 Peak incidence of stroke (32.4%) involved patients above 65 years old in our study which is comparable with findings of 61-70 years of most vulnerable age group for stroke in another study.14
We encountered higher number of patients with hemorrhagic stroke (48.6%) than some of other hospital based studies (22-31%).8-10
Dyslipidemia is a primary major risk factor for CAD and ischemic stroke15. It causes insulin resistance which results in increased levels of plasma triglycerides and low-density lipoprotein cholesterol (LDL-C) and a decreased concentration of HDL-C, as an important risk factor for peripheral vascular disease16, stroke, and CAD.17 Serum HDL-cholesterol has anti-atherogenic properties with ability to trigger the flux of cholesterol from peripheral cells to the liver and thus having a protective effect.18 Studies from neighboring countries like India19 and Bangladesh20 found a statistically positive correlation between elevated serum Total cholesterol and stroke.
Table No I: Comparison of Total & HDL Cholesterol among stroke patients
n Minimu m Maximu m Mean Standard Deviation Total Cholesterol 370 71 640 173.84 66.784 HDL-cholesterol 370 15 115 40.09 13.285
Table No. III: Comparison of Reduced HDL–Cholesterol in subtypes of stroke patients
Stroke Subtypes Total P-Value Ischemic Stroke Hemorrhagic Stroke Reduced HDL-cholesterol (serum HDL-cholesterol < 35 mg/dl) yes 83 53 136 0.005 43.7% 29.4% 36.8% no 107 127 234 56.3% 70.6% 63.2% Total 190 180 370 100.0% 100.0% 100.0%
The reported frequency for dyslipidemia in some of local studies on stroke patients includes 9.9%21, 18%22 and 57.5%23. We found dyslipidemia to be the second most frequent modifiable risk factor for stroke after hypertension. Our frequency of 60.5% for dyslipidemia (23.7% hypercholesterolemia and 36.8% reduced HDL together) stands close to 60.7% reported by Ahmad24 from Islamabad. Similarly, our frequency for hypercholesterolemia (23.7%) is slightly higher than 21% reported by Mahmood et al.25
On comparison, Ischemic stroke patients had statistically significant higher levels of serum total cholesterol than patients with hemorrhagic stroke (29.4% Vs 17.9%). Similarly, patients with Ischemic stroke had significantly lower HDL-cholesterol levels than those with hemorrhagic stroke (43.7% Vs 29.4%). Arshad Mahmood 25 reported similar results.
Burden of other major vascular risk factors i.e. hypertension, diabetes mellitus, and smoking is enormous in Pakistan. Hypertension is the most important modifiable risk factors for both ischemic and hemorrhagic stroke26. A cross sectional survey at a community health center in a tertiary care hospital revealed 19% prevalence for hypertension among healthy adults presented for routine preventive checkups. Only 40% of hypertensive patients had controlled blood pressure.27Jaffar28 similarly reported that more than 70% of people with hypertension were unaware of their condition, and less than 3% had adequately controlled blood pressure. 276(74.6%) of our stroke patients were hypertensive. This is in consistence with previously published studies in Pakistan.23,24,29,30
Diabetes mellitus is another known modifiable risk factor for stroke. Pakistan has more than 5 millions diabetic patients which is expected to rise to 3.9 millions by 2020, leading Pakistan to 4th most populous country accommodating patients with diabetes mellitus.31 76(20.5%) of our patients were diabetic. Others found frequency of 39.2%29 and 26.3%30 for diabetes.
Ischemic heart disease (IHD) is an important vascular disorder which increases the risk of ischemic stroke. In a population-based cross-sectional survey in Karachi, among 320 randomly selected adults aged 40 years or above, the overall prevalence of IHD was 26.9%32 28.3% of the studied patients had Ischemic heart disease. This is in line with figures of 22%33 28.8%24 and 30%23 from some of Pakistani studies.
Cigarette smoking is a powerful risk factor, especially for MI, peripheral artery disease, and stroke.34 Smoking has a negative effect of cholesterol and LDL-C to HDL-C ratio. Based on the data of National Health Survey of Pakistan, the overall prevalence of smoking among individuals aged 15 years or older was 15.2%.35 17.8% of stroke patients in the present study were smokers which is slightly lower than noted by others.23,24
Stroke is costly and the cost in human terms, to patients and their families, is impossible to estimate. Prevention is therefore an important public health issue. Since association of dyslipidemia with risk of stroke is well established, therefore, high risk patients not only be screened for dyslipidemia but also treated by lipid lowering therapy like statins which reduce dyslipidemia related mortality by 24-29%.36
Conclusion
Ischemic stroke patients had significantly higher frequency of hypercholesterolemia and reduced HDL-Cholesterol levels than patients of hemorrhagic stroke.
RECOMMENDATIONS:
Stroke is costly; prevention is therefore an important public health concern. Screening for dyslipidemia in high risk patients as primary prevention and use of lipid lowering therapy as secondary prevention for stroke are strongly recommended.
References
1. Sims NR, Muyderman H. Mitochondria, oxidative metabolism and cell
death in stroke. Biochimica et Biophysica Acta. September
2009:1802 (1): 80–91.
2. Mathers, CD; Boerma, T; Ma Fat, D. Global and regional causes of
death. British medical bulletin 2009:92: 7–32.
3. Feigin, Valery L; Forouzanfar, Mohammad H; Krishnamurthi, Rita; et
al. Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. The Lancet. 2013:(13)61953-4.
4. Towfighi A, Saver JL. Stroke declines from third to fourth leading
cause of death in the United States: historical perspective and challenges ahead. Stroke. August 2011; 42(8): 2351–5.
5. Jafar TH. Blood pressure, diabetes and increased dietary salt
associated with stroke- results from a community-based study in Pakistan. J Hum Hypertens 2006;20:83-85
6. Ebrahim S, Sung J, Song YM, Ferrer RL, Lawlor DA, Davey Smith G.
Serum cholesterol, haemorrhagic stroke, ischaemic stroke, and myocardial infarction: Korean national health system prospective cohort study. BMJ. 2006;333:22.
7. Sanossian N, Saver JL, Navab M, Ovbiagele B. High-density
lipoprotein cholesterol: an emerging target for stroke treatment. Stroke. 2007;38: 1104–1109.
8. Iqbal F. Patient profile of 200 cases of stroke: A hospital based study. Shaikh Zayed Postgrad Med Inst. 2001; 15:11-22.
9. Syed NA, Khealani BA, Ali S, Hasan A, Akhtar N, Brohi H et al.
Ischemic stroke subtypes in Pakistan: the Aga Khan University Stroke Data Bank. J Pak Med Assoc. 2003; 53: 584-88.
10. Vohra EA, Ahmed WU, Ali M. Aetiology and prognostic factors of
patients admitted for stroke. J Pak Med Assoc. 2000; 50: 234-36.
11. Khan H, Afridi AK, Ashraf S. A hospital based study on stratification of
risk factors of stroke in Peshawar. Pak J Med Sci 2006;22:304-07
12. Alam I, Haider I, Wahab F, Khan W, Taqweem MA, Nowsherwan. Risk
factors stratification in 100 patients of acute Stroke. J Postgrad Med Inst 2004;18:583-91.
13. Qureshi M A , Jamshaid T D , Siddiqui A M . Stroke - A study of clinical
patterns and risk factors. Ann King Edward Med Coll Jun 2003;9:98-100.
14. Khan NI, Naz L, Mushtaq S, Rukh L, Ali S, Hussain Z. Ischaemic
stroke: prevalence of modifiable risk factors in male and female patients in Pakistan. Pak J Pharm Sci 2009; 22:62-7.
15. Nicholls S, Lundman P. The emerging role of lipoproteins in
atherogenesis: beyond LDL cholesterol. Semin Vasc Med. 2004;4:187-195.
16. Wild SH, Byrne CD, Tzoulaki I, et al. Metabolic syndrome, haemostatic
and inflammatory markers, cerebrovascular and peripheral arterial disease: The Edinburgh Artery Study. Atherosclerosis. 2009;203:604-609.
17. Rodriguez-Colon SM, Mo J, Duan Y, et al. Metabolic syndrome
clusters and the risk of incident stroke: the atherosclerosis risk in communities (ARIC) study. Stroke. 2009;40:200-205.
18. Jia L, Bai H, Fu M, Xu Y, Yang Y, Long S. Relationship between
plasma HDL subclasses distribution and apoA-I gene polymorphisms.
Clinica Chimica Acta 2005; 360:37-45.
19. Sreedhar K, Srikant B, Joshi L, Usha G. Lipid profile in
non-diabetic stroke--a study of 100 cases. J Assoc Physicians India. 2010 Sep;58:547-51.
20. Uddin MJ, Alam B, Jabbar MA, Mohammad QD, Ahmed S. Association
of lipid profile with ischemic stroke. Mymensingh Med J. 2009 Jul;18(2):131-5.
21. Khan J, Rehman AU, Ali SA, Jielani A. Frequency of hypertension in
stroke patients presenting at Ayub Teaching Hospital. J Ayub Med Coll
Abbottabad 2006; 18:59-61.
22. Kamal A, Aslam S, Khattak S. Frequency of risk factors in stroke
patients admitted to DHQ teaching hospital D.I. khan. Gomal J Med Sci Jul - Dec 2010;8(2):200-3.
23. Siddiqui M, Khan FS, Khatri IA. Clinical patterns and risk factors for stroke in 120 troke patients in a tertiary care hospital with designated stroke center. Pak J Neurol Sci. 2006;1:58.
24. Ahmad A, Usman F, Hassan A. Risk factors and pattern of stroke in
Islamabad. Rawal Med J. Jan - Jun 2009;34(1):47-50.
25. Mahmood A, Sharif MA, Khan MN, Ali UZ. Comparison of Serum Lipid
Profile in Ischaemic and Haemorrhagic Stroke. J Coll Physicians Surg
Pak 2010, Vol. 20 (5): 317-320.
26. Khealani BA, Hameed B, Mapari UU, Stroke in Pakistan. J Pak Med
Assoc July 2008;58:7:400-3.
27. Iqbal SP, Dodani S, Qureshi R. Risk factors and behaviors for coronary
artery disease (CAD) among ambulatory Pakistanis. J Pak Med Assoc 2004;54:261-66.
28. Jafar TH, Levey AS, Jafary FH, White F, Gul A, Rahbar MH, et al.
Ethnic subgroup differences in hypertension in Pakistan. J Hypertens 2003;21:905-12.
29. Barech MS, Sadiq SM, Zarkoon AK, Dam G, Ullah K. Risk factors for
ischemic stroke in patients attending a tertiary hospital in Quetta. Pak J Neurological Sci Jan - Mar 2010;5(1):1-5
30. Aquil N, Begum I, Ahmed A, Vohra EA, Soomro BA. Risk Factors in
Various Subtypes of Ischemic Stroke According to TOAST Criteria J
Coll Physicians Surg 2011, Vol. 21 (5): 280-283
31. Jafar TH, Jafary FH, Jessani S, Chaturvedi N. Heart disease epidemic
in Pakistan: women and men at equal risk. Am Heart J. 2005;150:221-26.
32. Jafar TH, Chaturvedi N, Pappas G. Prevalence of overweight and
obesity and their association with hypertension and diabetes mellitus in an Indo-Asian Population. CMAJ 2006;24:1071-77.
33. Basharat RA, Yousaf M, Iqbal J, Khan MM. Frequency of known risk
factors for stroke in poor patients admitted to Lahore General Hospital in 2000. Pak J Med Sci 2002; 18: 280-3.
34. Karen L. Furie, Scott E. Kasner, Robert J. Adams et al. Attack:
Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association.
Stroke. 2011;42:227-276
35. Rizvi SF, Khan MA, Kundi A, Marsh DR, Samad A, Pasha O. Status of
rheumatic heart disease in rural Pakistan. Heart 2004;90:394-99.
36. Goldstein LB. Statins for stroke prevention. CurrAtheroscler Rep 2007;