Preparedness for practice : experiences of newly qualified professional nurses in a private hospital setting
154
0
0
Full text
(2) PREPAREDNESS FOR PRACTICE: EXPERIENCES OF NEWLY QUALIFIED PROFESSIONAL NURSES IN A PRIVATE HOSPITAL SETTING. By Charlene Belinda Muruvan. DISSERTATION. Submitted in fulfilment of the requirements for the degree. MAGISTER CURATIONIS in NURSING EDUCATION in the FACULTY OF HEALTH SCIENCES at the UNIVERSITY OF JOHANNESBURG. Supervisor: Dr. Charlené Downing Co-supervisor: Mrs. Irene Kearns. October 2018.
(3) DEDICATION. I dedicate this study to the Lord Most High. “Now to him who is able to do immeasurably more than we can ask or imagine, to him be glory forever and ever…Amen”. Ephesians 3:20. iii.
(4) ACKNOWLEDGEMENTS I thank God for the provision of his great strength and abundant grace afforded to me to commence and complete this research study I would like to acknowledge and thank these special people from the bottom of my heart for their valued and appreciated contribution towards my research study, whom without, this research study would not have been completed:. • My supervisor, Dr. Charlené Downing, thank you for your encouraging support, your wonderful guidance and expertise throughout my research study. You taught me what defines me as a person in life. Thank you for your passion and dedication that shone through always. May God’s blessings forever enrich your life.. •. My co-supervisor Mrs. I. Kearns, thank you for your kind words and support. May God’s blessings always be upon you. • To all the participants who shared their amazing life stories in this study, the most valued people of our nursing profession, I thank you for your time and courage to share with me your treasured experiences.. • To my wonderful husband, Jeremiah Muruvan, I thank you for all you do. Your continued support throughout the years is most appreciated. Thank you most of all for helping me follow my dreams.. • To my children, Jaiden and Cailey Muruvan, thank you for love and laughter including all the chores you both helped with so that I could work on my studies. Love you both with all my heart.. iv.
(5) • To my mother, with all my heart, I thank you for your support and encouragements throughout my education.. • My late dad (Benjamin Daniel) and brother (Donovan Daniel), you are no longer with us, but will always remain in my heart forever and ever. I know that you are my angels watching over me. Love you both always.. • To my encouraging friend, Jennifer Subke. Thank you my friend for your kindness, support and laughter in those very dark days.. • To all of my wonderful family (back home) and friends, thank you for remaining supportive and understanding through the time of my research study, I love each one of you dearly.. • My Nursing Service Manager, thank you for your kindness and continued support towards nursing education.. • To all my colleagues who understood the importance of my research study and stood in the gap when it was most needed thank you so much. Sr. Roanne Jagath, thank you for holding the fort and keeping me strong to finish this race, Sr. Rosemary Palmer, thank you for the encouraging notes, Mr. F.P. Fleming, thank you for the kind words of wisdom. God bless each of you abundantly.. • My independent coder Dr. Douline Minaar and language editor, Leatitia Romero, thank you for your availability and expert work on this study.. • The faculty Librarian of Health Sciences, Dorcas Dikomo Rathaba, I thank you so much for your generous assistance through my research study. May everything that you put your hands to always prosper.. v.
(6) ABSTRACT Preparedness of newly qualified professional nurses has become a concern in clinical practice. The importance of quality care and patient safety issues in healthcare has increased the expectations of the new professional nurse. The reality of working in a clinical setting for newly qualified professional nurses can prove to be overwhelming, resulting in a lack of confidence in their ability to perform effective patient care. The purpose of this study was to acquire an understanding of the newly qualified professional nurses’ experience of preparedness for practice in the private hospital setting in order to provide recommendations to support newly qualified professional nurses. A qualitative, exploratory, descriptive and contextual research design using a phenomenological approach was employed to explore and describe the lived experiences of newly qualified professional nurses’ preparedness for practice. The target population was newly qualified professional nurses working six months to a year in a private hospital setting in Gauteng. Purposive sampling was used to select participants. for. this. study.. Data. were. collected. through. eight. in-depth. phenomenological individual interviews, which were transcribed and analysed utilising Giorgi’s method of analysis. Themes and a central storyline were identified by means of thematic analysis. The findings emerged that newly qualified professional nurses felt ill-prepared for the huge leadership role and responsibility they had to step into; as a result, they profoundly doubted their own competence. At an interpersonal level the participants realised that they have to acquire a range of skills in order to deal with various role players and to ensure a high standard of nursing care. The newly qualified professional nurses felt that they needed time to grow into competent and confident professional nurses. Trustworthiness was ensured by means credibility, transferability, dependability and confirmability. Ethical considerations focused on autonomy, beneficence, nonmaleficence and justice. Recommendations for nursing education, nursing. vi.
(7) management, nursing practice, nursing research and policy development were suggested in the study to facilitate a smoother process of transition to support newly qualified professional nurses into their new role, improving preparedness for practice, enhancing confidence and delivering quality patient care.. Keywords: New Nurses, Preparedness, Transition, Phenomenology, Education. vii.
(8) TABLE OF CONTENT DECLARATION ...........................................................................................................i TURNITIN REPORT ................................................................................................... ii DEDICATION ............................................................................................................. iii ACKNOWLEDGEMENTS .......................................................................................... iv ABSTRACT ................................................................................................................ vi CHAPTER 1 OVERVIEW OF RESEARCH STUDY 1.1. BACKGROUND AND RATIONALE ................................................................. 1. 1.2. RESEARCH PROBLEM STATEMENT ........................................................... 4. 1.3. RESEARCH QUESTION ................................................................................. 6. 1.4. RESEARCH PURPOSE .................................................................................. 6. 1.5. RESEARCH OBJECTIVES ............................................................................. 6. 1.6. PARADIGMATIC PERSPECTIVES................................................................. 6. 1.6.1. Constructivism.......................................................................................... 8. 1.6.2. Meta-theoretical assumptions .................................................................. 9. 1.6.3. Theoretical assumptions ........................................................................ 10. 1.6.4. Methodological assumptions .................................................................. 11. 1.7. DEFINITION OF KEY CONCEPTS ............................................................... 12. 1.7.1. Preparedness ......................................................................................... 12. 1.7.2. Newly qualified professional nurse ......................................................... 12. 1.7.3. Experiences ........................................................................................... 12. 1.7.4. Practice .................................................................................................. 13. 1.7.5. Private hospital setting ........................................................................... 13. 1.8. RESEARCH DESIGN AND METHOD........................................................... 13. 1.8.1. Research design .................................................................................... 13. 1.8.2. Research method ................................................................................... 14. 1.8.3. PHASE 1: Exploration and description of newly qualified professional nurses’ experiences of preparedness for practice in a private hospital setting .................................................................................................... 15. viii.
(9) 1.9. POPULATION AND SAMPLING ................................................................... 15. 1.9.1. Population .............................................................................................. 15. 1.9.2. Sampling ................................................................................................ 15. 1.10. DATA COLLECTION ..................................................................................... 16. 1.11. DATA ANALYSIS .......................................................................................... 18. 1.11.1. Literature control .................................................................................... 19. 1.11.2. PHASE 2: Recommendations to support newly qualified professional nurses in a successful transition to the new role as professional nurses, improving their confidence and preparedness for practice in a private hospital setting ........................................................................... 19. 1.12. MEASURES OF TRUSTWORTHINESS ....................................................... 19. 1.12.1. Credibility ............................................................................................... 20. 1.12.2. Transferability......................................................................................... 20. 1.12.3. Dependability ......................................................................................... 20. 1.12.4. Confirmability ......................................................................................... 21. 1.13. ETHICAL CONSIDERATIONS ...................................................................... 21. 1.13.1. Autonomy ............................................................................................... 22. 1.13.2. Principle of beneficence and non-maleficence ....................................... 23. 1.13.3. Principle of justice .................................................................................. 24. 1.14. DIVISION OF CHAPTERS ............................................................................ 25. 1.15. SUMMARY .................................................................................................... 25 CHAPTER 2 RESEARCH DESIGN AND METHOD. 2.1. INTRODUCTION ........................................................................................... 27. 2.2. RESEARCH DESIGN .................................................................................... 27. 2.2.1. Qualitative research design.................................................................... 28. 2.2.2. Exploratory research design................................................................... 29. 2.2.3. Descriptive research design ................................................................... 30. 2.2.4. Contextual research design ................................................................... 30. 2.3. RESEARCH METHOD .................................................................................. 31. ix.
(10) 2.3.1. PHASE 1: Exploration and description of newly qualified professional nurses’ experiences of preparedness for practice in a private hospital setting .................................................................................................... 32. 2.3.1.1. Phenomenology research method ...................................................... 32. 2.3.1.2. Population........................................................................................... 34. 2.3.1.3. Sample and sampling ......................................................................... 35. 2.3.1.4. Data collection .................................................................................... 36. 2.3.1.5. Data analysis ...................................................................................... 41. 2.3.1.6. Literature Control ................................................................................ 44. 2.3.2. PHASE 2: Recommendations to support newly qualified professional nurses in a successful transition to the new role as professional nurses, improving their confidence and preparedness for practice in a private hospital setting ........................................................................... 45. 2.3.3 2.4. MEASURES OF TRUSTWORTHINESS ....................................................... 46. 2.4.1. Credibility ............................................................................................... 46. 2.4.1.1. Prolonged engagement by the researcher ......................................... 46. 2.4.1.2. Data Triangulation .............................................................................. 47. 2.4.1.3. Persistent observation ........................................................................ 47. 2.4.1.4. Member checking ............................................................................... 48. 2.4.1.5. Peer evaluation................................................................................... 48. 2.4.1.6. Authenticity of the research ................................................................ 48. 2.4.2. Transferability......................................................................................... 48. 2.4.2.1. Purposive Sampling............................................................................ 49. 2.4.2.2. Rich, dense description of results ....................................................... 49. 2.4.3. Dependability ......................................................................................... 49. 2.4.3.1. In-depth descriptions of research methodology .................................. 50. 2.4.3.2. Stepwise replication............................................................................ 50. 2.4.3.3. Code-recode procedure...................................................................... 50. 2.4.3.4. Dependability audit ............................................................................. 50. 2.4.4. 2.5. Ethical considerations ............................................................................ 45. Confirmability ......................................................................................... 51. 2.4.4.1. Auditing .............................................................................................. 51. 2.4.4.2. Trail of evidence of research process ................................................. 51. SUMMARY .................................................................................................... 51 x.
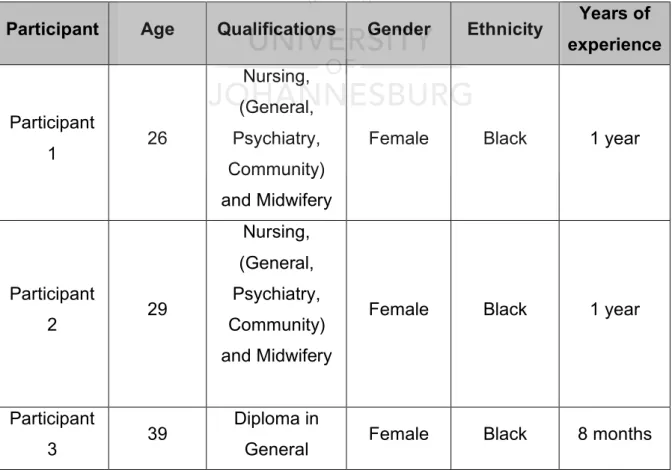
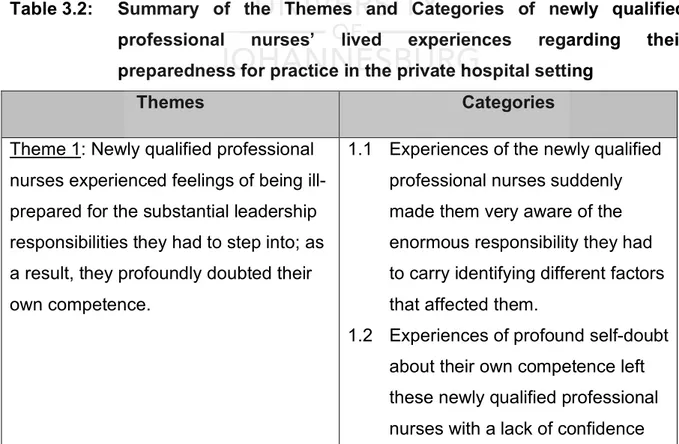
(11) CHAPTER 3 RESEARCH RESULTS AND FINDINGS 3.1. INTRODUCTION ........................................................................................... 53. 3.2. DESCRIPTION OF THE RESEARCH ENVIRONMENT ............................... 53. 3.3. OVERVIEW OF DATA ANALYSIS ................................................................ 54. 3.4. DESCRIPTION OF SAMPLE ........................................................................ 55. 3.5. ANALYSIS OF FIELD NOTES ...................................................................... 56. 3.5.1. Theoretical notes.................................................................................... 57. 3.5.2. Methodological notes ............................................................................. 57. 3.5.3. Observational Notes............................................................................... 58. 3.5.4. Personal notes ....................................................................................... 58. 3.6. DESCRIPTION OF CENTRAL STORYLINE ................................................. 59. 3.7. DESCRIPTION OF FINDINGS: THEMES AND CATEGORIES .................... 59. 3.7.1. Theme 1:Newly qualified professional nurses experienced feelings of being ill-prepared for the substantial leadership responsibilities they had to step into; as a result, they profoundly doubted their own competence............................................................................................ 62. 3.7.1.1. Category 1.1: Experiences of the newly qualified professional nurses suddenly made them very aware of the enormous responsibility they had to carry identifying different factors that affected them ...................................................................................... 62. 3.7.1.2. Category 1.2: Experiences of profound self-doubt about their own competence left these newly qualified professional nurses having a lack of confidence and feeling lost ...................................................... 67. 3.7.1.3. Category 1.3: Experiences of newly qualified professional nurses who carried the weight of an expectation to know everything ............. 69. 3.7.2. Theme 2: At an interpersonal level, they realised that they have to acquire a range of skills in order to deal with various role players and to ensure a high standard of nursing care .............................................. 71. 3.7.2.1. Category 2.1: The newly qualified professional nurses had to perform the duties associated with their roles and thus reached out to different staff members for assistance ............................................ 71. xi.
(12) 3.7.2.2. Category 2.2: As newly qualified professional nurses they experienced challenges in delegation and staff undermining behaviours .......................................................................................... 73. 3.7.2.3. Category 2.3: The experiences of newly qualified professional nurses identified dynamics with various role players, familiarising themselves with procedures, equipment and culture while also having to provide high- quality nursing care ....................................... 76. 3.7.3. Theme 3: Newly qualified professional nurses experienced that they needed time to develop into skilled proficient professional nurses......... 79. 3.7.3.1. Category 3.1 The participants experienced that they had certain needs as newly qualified professional nurses setting out in the clinical practice ................................................................................... 79. 3.7.3.2. Category 3.2 The newly qualified professional nurses experienced personal development of identity, professional maturity and confidence in the process ................................................................... 82. 3.7.3.3. Category 3.3 The newly qualified professional nurses became aware of how much was still to be learned ......................................... 84. 3.8. SUMMARY .................................................................................................... 86 CHAPTER 4 EVALUATION, RECOMMENDATIONS, LIMITATIONS AND CONCLUSION. 4.1. INTRODUCTION ........................................................................................... 87. 4.2. PURPOSE AND OBJECTIVES ..................................................................... 87. 4.3. EVALUATION OF THE STUDY .................................................................... 88. 4.4. STRENGTHS OF THE STUDY ..................................................................... 89. 4.5. LIMITATIONS ................................................................................................ 90. 4.6. RECOMMENDATIONS ................................................................................. 90. 4.6.1. Recommendations for nursing education ............................................... 98. 4.6.2. Recommendations for nursing management ......................................... 99. 4.6.3. Recommendations for nursing practice ................................................ 100. 4.6.4. Recommendations for nursing research .............................................. 100. 4.6.5. Policy development .............................................................................. 101. 4.7. PERSONAL REFLECTIONS ....................................................................... 101 xii.
(13) 4.8. SUMMARY .................................................................................................. 102. REFERENCE LIST ................................................................................................ 104 TABLES Table 3.1: Summary of participants’ biographical details ......................................... 55 Table 3.2: Summary of the Themes and Categories of newly qualified professional nurses’ lived experiences regarding their preparedness for practice in the private hospital setting ............................................... 60 Table 4.1: Summary of themes and recommendations to support new professional nurses in a successful transition to their new role, improving confidence and preparedness for practice ............................. 91 ANNEXURES ANNEXURE A: INFORMATION LETTER TO THE PARTICIPANT ....................... 117 ANNEXURE B: INFORMED CONSENT FOR THE PARTICIPANT ....................... 120 ANNEXURE C: CONSENT FOR THE USE OF AN AUDIO-TAPE RECORDER ... 121 ANNEXURE D: REQUEST FOR PERMISSION TO CONDUCT RESEARCH AT PRIVATE HOSPITAL SETTINGS ................................................. 122 ANNEXURE E: LETTER OF APPROVAL TO CONDUCT RESEARCH AT PRIVATE HOSPITALS ................................................................. 124 ANNEXURE F: LETTERS OF ACKNOWLEDGEMENT FROM PRIVATE HOSPITALS TO CONDUCT RESEARCH .................................... 126 ANNEXURE G: UJ FACULTY OF HEALTH SCIENCES ETHICAL CLEARANCE 128 ANNEXURE H: SAMPLE OF TRANSCRIPT ......................................................... 130 ANNEXURE I: LETTER FROM THE INDEPENDENT CODER ............................ 140 ANNEXURE J: LETTER FROM THE LANGUAGE EDITOR.................................. 141. xiii.
(14) CHAPTER 1 OVERVIEW OF RESEARCH STUDY 1.1. BACKGROUND AND RATIONALE. The preparedness of newly qualified professional nurses for clinical practice has been debated since the 70’s (Murray, Sundin & Cope, 2018:44). The claim of a lack of work preparedness, while not new, continues to haunt nursing practices today (Missen, McKenna & Beauchamp, 2017:230-231). The growing intricacy of the healthcare setting as entered into by newly qualified professional nurses has grown to be very challenging. Newly qualified professional nurses are expected to be even more prepared for practice (Hudson, 2017:1). However, employers believe that the education and clinical experiences provided to student nurses prior to entering the workplace are inadequate, leading to a lack of preparedness for the reality of clinical practice. Newly qualified professional nurses are expected to “hit the floor running” from the first day they enter the clinical setting, which is also a clear indication of the urgency for qualified professionals in hospital settings (Usher, Mills, West, Park & Woods, 2015:3246; El Hadad, Moxham & Broadbent, 2017:392). Effectively transitioning new professional nurses into the clinical setting is fundamental. The demands on new professional nurses are increasing as the patient population presents with more complex health problems and nurses are faced with new healthcare technologies that continue to evolve (Silvestre, Ulrich, Johnson, Spector & Blegen, 2017:110). Population ageing and increased occurrence of complex chronic diseases with multiple co-morbidities have placed pressure on general healthcare services. Nurses provide cost-effective, high-quality patient care services to these patients with complex and chronic conditions. Hence, newly qualified professional nurses play a central role in the effective integration of care and they are an essential part of patient care in healthcare services globally (Aggar, Bloomfield, Thomas & Gordon, 2017:1-2). Promoting public safety is one of the goals of every healthcare service, both nationally and internationally (Silvestre, et al. 2017:110). Quality patient care. 1.
(15) requires newly qualified professional nurses to meet patients well-prepared with sufficient knowledge and practical skills in the hospital setting (Solvik & Struksnes, 2018:1). However, this can only be achieved through effectively supporting the newly qualified professional nurses during their critical transition period, which is the first time they enter the clinical setting; known as the transition period (Silvestre, et al. 2017:110). A known fact in the clinical setting, which was first discovered in the landmark study by Marlene Kramer in 1974 who described this crisis as a “reality shock”, has most recently been recognised as transition shock. This concept illuminates that there were significant concerns in the transition process of newly qualified professional nurses which remains true in the current transition of new professional nurses in the clinical setting (Odland, Snetveldt & Sörlie, 2014:538; Ankers, Barters & Parry, 2017:319). A reality shock is first encountered in the clinical setting when there is an abrupt entrance from practising in a simulated environment into the clinical setting. A disparity exists between nursing as taught and nursing as practised, resulting in a gap between theory and practice (Freeling & Parker, 2014:48; Kaihlanen, Salminen, Flinkman & Haaivisto, 2018:2). This is a sad reality whereby one lacks the ability to connect nursing education to that of the realities of the clinical setting, resulting in difficulties for nurses to adapt to their. new. roles,. resolve. conflicts. and. make. decisions. (Gaunden. &. Mohammadnezhad, 2018:1-2). The longstanding deliberation forces one to inquire as to whether newly qualified professional nurses are, in fact, prepared for practice (El Hadad, et al. 2017:392). The real world of working in a clinical setting for newly qualified professional nurses is overwhelming, and these feelings can result in a lack of confidence in their ability to perform quality patient care (Woods, West, Mills, Park, Southern & Usher, 2014:360; Gardiner & Sheen, 2016:7). Morgan and Edmonds (2017:2) have stated that newly qualified professional nurses go through a range of emotions from joy and excitement for a new career, to stress and anxiety of assuming their new role. Due to the extreme pressures, stress and emotional tension experienced, the newly qualified professional nurse’s ability to meet patients’ emotional needs may result in a negative outcome of compromised 2.
(16) patient care and a discouraged professional nurse (Zamanzadeh, Jasemi, Valizadeh, Keogh & Taleghani, 2015:366; Gaunden & Mohammadnezhad, 2018:1). The study highlights the difficulties that new professional nurses have in preparing for their role, an inevitable stage in one’s adaptation to the nursing profession. The realisation that one is becoming a fully accountable professional nurse can thus lead to the questioning of one’s own competence (Morrell & Ridgway, 2014:519; Twine, 2017:56). According to Green (2015:42) and Walker, Foster and De Bruin (2017:505), the role transition from student to professional nurse is a vital area in need of support. The effective roles that are required by newly qualified professional nurses need to be examined, as this is vital to support the consolidation of nursing knowledge, developing competence and confidence for safer practice with successful assimilation into the clinical setting. Newly qualified professional nurses find it difficult to transition from nursing student to a professional nurse (Kaihlanen, et al. 2018:2). These new professional nurses must receive effective clinical experiences in order to ease the transition process, which is usually described as the first year of qualification. The first year of being newly qualified in the clinical setting is crucial and the most challenging experience. The new professional nurses encounter numerous trials at the onset of their careers as they struggle to build confidence in their professional practice (Gaunden & Mohammadnezhad, 2018:1, 4). Over decades there has also been transition-topractice programmes that have been established, but in spite of some successes there remains discussions that arise around the transitional challenges that newly qualified professional nurses face. This identifies a need for new solutions that are still required for a smooth transition process in the clinical setting (Kaihlanen, et al. 2018:2). Newly qualified professional nurses are valuable components of a healthcare system that largely depends on the knowledge and skills of professional nurses who are responsible for delivering quality health care (Mampunge & Seekoe, 2014:59; Morgan & Edmonds, 2017:1). The transition journey of newly qualified professional nurses in preparedness for practice from educational institutions to the clinical. 3.
(17) settings, and their development and adjustments as professional nurses, remains a challenging period (Ankers, et al. 2017:320). Enhancing positive transitional experiences after entering their new role would increase safer and higher quality patient care in the clinical settings (Kaihlanen, et al. 2018:6). Newly qualified professional nurses are the future of the nursing profession, therefore the difficulties they face through the transition process must immediately be addressed so that it will support the nursing profession, enhance quality patient care and improve the clinical setting outcomes within the organisation. This will result in effectively transforming new professional nurses into confident healthcare providers in the nursing profession who provide quality patient care (Henderson, Ossenberg & Tyler, 2015:225; Gaunden & Mohammadnezhad, 2018:5). 1.2. RESEARCH PROBLEM STATEMENT. The transition from student to professional nurse has been identified as a period of turbulence characterised by stress and anxiety (Walker, Storey, Costa & Leung, 2015:2; Morgan & Edmonds, 2017:1). The newly qualified professional nurse is often tense due to experiences of uncertainty and fear in a clinical setting. Lack of clinical experience is found to undermine the newly qualified professional nurses’ confidence in their knowledge and skills, resulting in an uncomfortable workplace transition. As student nurses, the facilitated practical experiences should play a significant part in nurses’ training because as they adapt to new roles, they will relate to previous nursing experiences. These prior experiences in the clinical setting can affect one’s feelings regarding preparedness for practice (Joolaee, Amiri, Farahani & Varaei, 2015:14; Kaihlanen, et al. 2018:2). Hence, effective quality education and training for preparedness of practice is fundamental to a successful role transition and improved quality patient care outcomes (Twine, 2017:58). Generally, the nursing education curriculum provides nursing students with theoretical knowledge and skills competencies, although there may still be a lack in confidence and clinical exposure (Wu, Enskär, Lee & Wang, 2014:357; Gaunden & Mohammadnezhad, 2018:1). Furthermore, Hansen-Salie and Martin (2014:550) and Morgan and Edmonds (2017:2) state that new professional nurses have sufficient 4.
(18) knowledge, yet they lack the ability to solve problems by assessing and reasoning out their actions before making informed decisions and applying these to practice. Similarly, Ballem and MacIntosh (2014:383) and Ankers, et al. (2017:319) agree that the level of work preparedness of new professional nurses is essential, and the differences between nursing education and the realities of the clinical setting contribute to poorly prepared newly qualified professional nurses. Dr Benner (in Peate & Wild, 2018:9) states that nursing education can do a better job of closing the gap between education and clinical practice in assisting newly qualified professional nurses in understanding their profession through education and hands-on experiences. According to Woods, et al. (2014:360) and Walker, et al. (2017:510), tertiary nurse education programmes aim to produce a new professional nurse with the knowledge and skills for registration. Further, employers expect new professional nurses to be “work ready”, meeting competency standards, functioning independently and providing safe, quality patient care. However, newly qualified professional nurses do not feel confident to utilise these clinical abilities independently. Assuming that work preparedness is impossible to learn from books, it is a skill that requires getting familiar with practical skills in a clinical setting where one learns, over time, how to deal with situations. The clinical settings of healthcare organisations must realise that independent practice and critical thinking skills grow over time, provided that newly qualified professional nurses are adequately supported (Gaunden & Mohammadnezhad, 2018:5). Newly qualified professional nurses who are in transition from tertiary to their clinical settings commonly encounter various difficulties. Adjusting to workplace expectations and taking responsibility in the clinical setting is extremely stressful in the first few months of employment for these new nurses (Walker, et al. 2017:511). The researcher, a clinical facilitator, identified challenges faced by newly qualified professional nurses in the private hospital setting. Newly qualified professional nurses often have the knowledge but lack confidence and support in the hospital setting, which makes them feel like they have been thrown into the deep end (Hussein, Everett, Ramjan, Hu & Salamonson, 2017:5). Driven by this important motivation, the researcher set out to explore and understand the experiences of 5.
(19) preparedness for practice of newly qualified professional nurses’, and to make recommendations to support a meaningful start to a professional nursing career delivering quality patient care with confidence in a private hospital setting. 1.3. RESEARCH QUESTION. The following research question emerged from the research problem: • What are newly qualified professional nurses’ experiences of preparedness for practice? 1.4. RESEARCH PURPOSE. The purpose of this study was to gain an understanding of newly qualified professional nurses’ experiences of preparedness for practice in the private hospital setting, and to develop recommendations to support newly qualified professional nurses for the transition into their clinical role, delivering quality patient care with confidence in a private hospital setting. 1.5. RESEARCH OBJECTIVES. The research objectives were: • To explore and describe newly qualified professional nurses’ experiences of preparedness in a private hospital setting. • To provide recommendations to support newly qualified professional nurses in a successful transition to their new role as a professional nurse, improving their confidence and preparedness for practice in a private hospital setting. 1.6. PARADIGMATIC PERSPECTIVES. A paradigm refers to a worldview perspective of beliefs and understanding. This is a framework through which research is perceived and implemented, thus, it is vital for these beliefs to be recognised as they guide the researcher’s thoughts and actions (Leavy, 2017:12). Paradigms are categorised as assumptions that influence the. 6.
(20) research process and are joined by the following belief systems: reality (ontology), an understanding that can be gained from research (epistemology), and appropriate methods to conduct research (methodology) (Ling & Ling, 2017:4). • Ontology Creswell and Poth (2018:20) describe ontology as the nature of reality, which embraces the idea of multiple realities as well as individuals beings studied. It also supports the realities in a qualitative study. The researcher’s intent during this study was to report these multiple realities in forms of units of meanings. The actual words of the different newly qualified professional nurses presenting their varied experiences of preparedness for practice as they experienced it, were used. • Epistemology Epistemology is the theory of knowing reality (Creswell & Poth, 2018:18) leading to how we know what we know (Holloway & Galvin, 2017:21). Evidence is based on individual views by which knowledge is then known through the participants’ subjective experiences. Creswell and Poth (2018:21) state that in a qualitative study the researcher gets as close to the participants of the study as possible. Through these perspectives, the research stances were within the constructed realities which provided direction for the study. It allowed the researcher to gain knowledge and insight about newly qualified professional nurses regarding preparedness for practice. • Methodology The methodology refers to the process used in qualitative research. During data analysis the researcher follows a path in analysing data; this enhances knowledge of the topic under study. As a constructivist, the researcher engaged in the social setting and daily life experiences of the research participants. Unstructured individual interviews allowed the researcher access to the participants. She became familiar with how the newly qualified professional nurses experienced preparedness for practice and their support needs to facilitate the transition process (Creswell & Poth, 2018:21).. 7.
(21) The assumptions of the study are based on the Theory for Health Promotion in Nursing (University of Johannesburg, 2010), Benner’s Theory of Novice to Expert (1982), and the Constructivist worldview. A constructivist approach was utilised in the research study based on the researcher’s worldview. The constructivist worldview is further elaborated on next. 1.6.1. Constructivism. Denicolo, Long and Bradley-Cole (2016:4-5) refer to constructivism as a specific way of discovering how people understand their worlds. A multiple of realities provided a general approach which stimulated rich and deep insights into the participants’ inner experiences. The supporting philosophy effectively produced data that represent a person’s outlook in making sense of reality. In this study, the worldview of the researcher is linked to the constructivist approach which seeks to understand how people make sense of their personal world. The central focus for the researcher was the research participants, who constructed personal meanings from their own realities in their environments. Emphasis was placed on understanding the newly qualified professional nurses’ interpretation of their lived experiences in the private hospital setting. It remained imperative that the researcher made every effort to understand the viewpoint of the participants involved in the study and not her own (Kivunja & Kuyini, 2017:33). Creswell (2014:8) and Flick (2018:35) state that constructivism is an approach to qualitative research whereby individuals seek understanding of the world in which they live and work. Constructivists place prominence on understanding the context of the participants through visiting the field, gathering information, and generating meaning from the data collected in the field. The research design was qualitative and related to the participants being newly qualified professional nurses who experienced the phenomenon (preparedness for practice) under study. Hence, a constructivist approach was utilised to gather data from the participants’ realities and meanings from their own experiences in their environments, from a phenomenological perspective. This phenomenological qualitative approach was used to explore these personal experiences of newly qualified professional nurses in the private hospital setting. These human experiences were reviewed through descriptions presented by 8.
(22) the individual participants involved in the research study (Creswell, 2014:187; Flick, 2018:35-36). The meta-theoretical, theoretical and methodological assumptions are discussed next. 1.6.2. Meta-theoretical assumptions. Meta-theoretical assumptions deal with the researcher’s view of man and society, providing a framework within which theoretical statements are made (University of Johannesburg, 2010:12). The researcher’s assumptions concerning newly qualified professional nurses are based on the Theory for Health Promotion in Nursing (University of Johannesburg, 2010). The newly qualified professional nurse is viewed as a sensitive, therapeutic professional who demonstrates knowledge, skills and values to facilitate the promotion of health (University of Johannesburg, 2010:4). The researcher’s assumptions of the person (newly qualified professional nurse), the environment (internal and external) and nursing, are described next. • Person The whole person symbolises the body, mind and spirit which functions in an integrated, interactive manner in the environment (University of Johannesburg, 2010:4). This research refers to newly qualified professional nurses who have experiences with the phenomenon under study, and who are integrated and interactively fulfilling their roles in delivering patient care in the private hospital setting. • Environment The environment includes an internal and external environment. The internal environment comprises the body, mind and spirit. The external environment consists of the physical, social, spiritual dimensions where the phenomenon under study occurs (University of Johannesburg, 2010:5).. 9.
(23) • Nursing Nursing refers to an interactive process where the nurse is referred to as a sensitive, therapeutic professional who enables the promotion of health through the use of resources (University of Johannesburg, 2010:4). The newly qualified professional nurse is seen in this study as a delicate professional who should demonstrate knowledge, skills, attitudes and values that promote health and quality care for the patient. 1.6.3. Theoretical assumptions. Theoretical assumptions are statements that provide the scope of knowledge about the research domain that forms part of the existing theory of discipline or related disciplines. They offer a framework for the epistemic statements in the research (University of Johannesburg, 2010:12). The researcher’s assumptions about preparedness for practice are based on Benner’s Novice to Expert Model (1984:402407 in Peate & Wild, 2018:9). Patricia Benner, a contemporary theorist, introduced the theory that nurses develop skills. and. understanding. through. experience. and. continuous. professional. development of caring. The phrase from “Novice to Expert” signified the perception that the expert nurse learned quality patient care through a process that involved theory integrated with practice and various experiences in the clinical settings. New professional nurses developed skills and understanding of patient care over time. This includes a combination of a strong foundational education and individual personal experiences. The theory compartmentalises nursing into five levels of capabilities. The well-known theorist believed that experience in the clinical setting was vital to nursing because it allowed nurses to continuously expand their knowledge in providing holistic and quality care to patients. Benner found that in nursing, improved practice depended on experience, and when it came to developing skills, this was a lengthy and progressive process. This also indicated that when nurses engaged in various circumstances, they learned from them as they developed skills by being involved with the patients. When applied to the understanding of newly qualified nurses’ preparedness for practice, it is understood that the newly qualified professional nurse is seen as an advanced beginner, who 10.
(24) still requires support in the field and reminds us that expertise is a process learned over time. The assumptions related to the study are the following: • The complexity and responsibility of nursing practice require ongoing career development for newly qualified professional nurses. • Experience in the clinical setting is key to preparedness for practice as it allows for expanding the nurse’s knowledge base, and providing holistic, competent care to the patient. • Development of mentorship programmes increase the competency, confidence and satisfaction of newly qualified professional nurses. • Maintaining a healthy working environment supports newly qualified professional nurses who are the future employee pool. • A positive experience will encourage the newly qualified professional nurse to mentor novice nurses and give the same positive experience he/she had during the transition period. 1.6.4. Methodological assumptions. The methodological assumptions reveal the researcher’s views of the nature and structure of science in the discipline, providing an outline to the research objective and research context which guides the decisions about the research design. The researcher viewed this study as a framework of the lived experiences of the newly qualified professional nurse in preparedness for practice. The research problem and objectives direct the research design and methods in formulating the type of research approach (University of Johannesburg, 2010:10-12). The researcher intended to make sense of the meanings of newly qualified professional nurses’ individual experiences of preparedness for practice. In the context of the constructivist view, a qualitative research design was employed. The researcher attempted to understand by engaging with the setting in order to construct meaning through open-ended, in-depth interviews (Creswell 2014:38;. 11.
(25) Creswell & Poth, 2018:21). The research aimed to rely on the participants’ views of the situation being studied. The researcher utilised the measures of reliability and trustworthiness in supporting the usefulness of the research findings (University of Johannesburg, 2010:10). 1.7. DEFINITION OF KEY CONCEPTS. The following concepts have been identified as key concepts and are defined as follows: 1.7.1. Preparedness. Preparedness is defined as being ready to confidently deliver safe patient care (Usher, et al. 2015:3246; Walker, et al. 2017:509). In this research study, preparedness is identified as being competent in skills, knowledge and attitude with the ability to render quality and effective, safe patient care. 1.7.2. Newly qualified professional nurse. A newly qualified professional nurse is defined as a competent and independent practitioner in nursing who gives comprehensive nursing care, assuming responsibility and accountability for the holistic care provided to a patient (Nursing Act, No.33 of 2005). In this study, the newly qualified professional nurse is referred to as being newly registered with the South African Nursing Council, employed in the private hospital setting for six months to a year. 1.7.3. Experiences. Experiences relate to personal knowledge that individuals have gained from being personally involved in daily events and situations (Ndawo, 2016:2; Gray, Grove & Sutherland, 2017:10). In this study, experiences are personal encounters and livedthrough events of newly qualified professional nurses in a private hospital setting.. 12.
(26) 1.7.4. Practice. Practice is defined as a profession where knowledge is put into practice by which actions are integrated and collaborated within the healthcare team by assessing, planning and implementing health care, entirely for the enhancement of the health and wellbeing of an individual (Searle, Human & Mogotlane, 2009:60; Finkelman, 2019:43). In this study, practice is defined as the theoretical and practical understanding of implementing the role and responsibilities of a professional nurse, as guided by the Nursing Act no.33 of 2005 as in the Regulation 2598 regarding the scope of practice of a professional nurse. 1.7.5. Private hospital setting. A private hospital setting is a private health establishment not owned by the state (National Health Act, No 61 of 2003). In this study, a hospital setting is a private, forprofit health establishment that provides quality health care in various disciplines, and which offers clinical placements for student nurses’ facilitation and training to become professional nurses. 1.8. RESEARCH DESIGN AND METHOD. The research design and method utilised in this study was qualitative, exploratory, descriptive and contextual. The design was chosen in order to explore and describe the newly qualified professional nurses’ experiences of preparedness for practice in a private hospital setting. 1.8.1. Research design. A research design refers to a complete plan selected to conduct the research study. The design chosen was one that was well-suited for the research study and it addressed the research purpose in detail (Bruce & Klopper, 2017:460). A qualitative, exploratory, descriptive and contextual design was employed in this study which was contextual in nature. A qualitative research study involves a holistic 13.
(27) approach that describes life experiences with uniqueness in understanding and giving meaning to them. This approach enhanced understanding of the nature of the participants within the context of the research (Grove, Burns & Gray, 2013:87; Gray, et al. 2017:10, 25). The researcher played an active role in entering the field to acquire an understanding of newly qualified professional nurses’ experiences of preparedness for practice. The study was conducted as an exploratory-descriptive study aiming to gain an understanding by obtaining insight of the phenomenon in need of a solution (Grove, et al. 2013:87; Gray, et al. 2017:6). The contextual study considered the broader framework of the phenomenon under study, including the locality and conditions under which data were gathered as events occurred in real life settings. Participants are linked to their environment, thus, when the context is understood, the experiences and actions of the participants lead to an enriched meaning of the clinical setting (Holloway & Wheeler, 2010:5; Holloway & Galvin, 2017:6). 1.8.2. Research method. A research method is the data collection and data analysis methods of the research study. The method chosen for the study must be appropriate to the research purpose, including the sample of the study. This enhances the transparency of the study as it presents accurate details of the method the researcher utilised in accomplishing the purpose of the study (Rees, 2016:113). A phenomenological approach was applied in this study as it was an effective method for discovering meaning and capturing the essence of experiences as lived by participants (Grove, et al. 2013:27, 60; Gray, et al. 2017:29). This research method was valuable in recognising individual participants’ unique personal experiences of preparedness for practice (Glasper & Rees, 2017:154). The research method was conducted in two phases. In Phase 1, the newly qualified professional nurses’ experiences of preparedness for practice in the private hospital setting were explored and described. In Phase 2, recommendations to support new professional nurses in a successful transition to their new role as professional nurses, improving. 14.
(28) confidence and preparedness for practice in a private hospital setting, were presented. 1.8.3. PHASE 1: Exploration and description of newly qualified professional nurses’ experiences of preparedness for practice in a private hospital setting. In this phase, the researcher utilised the phenomenological research method to uncover the meanings of the shared individual experiences of newly qualified professional nurses’ preparedness for practice as they encountered it in their everyday clinical settings (Glasper & Rees, 2017:153). This method enabled the researcher to explore and describe what meanings these experiences held for each individual, thereby illuminating the essence of the phenomenon (Gray, et al. 2017:87). 1.9 1.9.1. POPULATION AND SAMPLING Population. A population is indicated as an entire group of people that represent the research study’s focus. In this study, the population signified all newly qualified professional nurses employed for six months to one year at a private hospital setting in Gauteng. The participants whom the researcher had access to are termed the accessible population (Gray, et al. 2017:53). The target population consisted of newly qualified professional nurses employed at the two private hospitals in Gauteng.. The. accessible population comprised of newly qualified professional nurses who qualified with the South African Nursing Council and employed for the last six months to a year at the two selected private hospitals that belonged to one private healthcare group in Gauteng. 1.9.2. Sampling. The use of purposive sampling in this study enabled the researcher to obtain information from participants of particular interest, who represented the full range of 15.
(29) the study with relevant experiences, thus increasing the depth of information obtained (Grove, et al. 2013:353; Pajo, 2017:144). A purposive sampling method assisted the researcher to gain dense in-depth data about newly qualified professional nurses’ preparedness for practice. The participants of the study were unknown to the researcher and were employed at a private hospital setting also unknown to researcher. This ensured credibility, objectivity and eradicated bias. The estimated sample size was eight participants, and the final number was concluded when data saturation was reached. This occurs when no new information is added and additional samples or collecting new data becomes repetitive (Bazeley, 2013:50; Silverman, 2017:269). The inclusion criteria for this study was professional nurses who were newly qualified for six months to a year, practising at private hospital settings in Gauteng. 1.10. DATA COLLECTION. According to Holloway and Wheeler (2010:19) and Glasper and Rees (2017:79), data collection in qualitative research in health care provides the foundation for both exploring and understanding the participants’ experiences to create meaning. In this study, the researcher used experiences by engaging with participants through unstructured individual in-depth phenomenological interviews. To collect data, these unstructured in-depth interviews are commonly designed for guidance on specific aspects to understand the phenomenon being studied. It allows the researcher to be open to the responses and perspectives of the participants (Grove, et al. 2013:271; Holloway & Galvin, 2017:87). The researcher conducted unstructured in-depth interviews so that participants were encouraged to reveal details of their experiences regarding their preparedness for practice as newly qualified professional nurses. The research question for the interview was broad and open-ended, stated as: “What are your experiences of preparedness for practice as a newly qualified professional nurse in the private hospital setting?” The one-on-one interviews lasted between 3045 minutes. The interviews were audio-taped with permission from the participants, which increased credibility as the data could be accurately captured in this way. The individual unstructured in-depth interviews were conducted at a venue, date and time 16.
(30) as agreed upon by the interviewer and participants. The unstructured in-depth interviews included follow-up questions that allowed for a deeper understanding and more clarity on certain aspects that were unclear. The participants were encouraged to elaborate on their experiences by means of probing and follow-up questions that were non-threatening yet thought-provoking. Interview responses were positive in order to support the participant, but not leading (Grove, et al. 2013:272; Glasper & Rees, 2017:79). Through utilising qualitative research methods, data were also collected through observations and field notes that identified the participants’ actions, interactions, and behaviours in the natural setting. This enabled the researcher to capture all data into the study (Marshall & Rossman, 2016:143). • Field notes Field notes are a type of record keeping that represent participant information and setting observations, personal experiences and development in the field (Polit & Beck, 2018:202). The field notes served several purposes and will be described in detail in Chapter 3. Following is an outline of the field notes that the researcher utilised for the study. • Observational Notes Through observational note taking the researcher was able to explore and tried to understand the participants of the study (Holloway & Galvin, 2017:112). Observational notes provide the researcher with rich information of participants’ behaviours, reactions and interactions during the process of the unstructured interview. This type of data collection strategy is prevalent as the central focus is observing behaviours, verbal and non-verbal communication, including the environment setting. These assisted the researcher to explore and describe the phenomenon of interest (Waltz, Strickland & Lenz, 2017:178). • Theoretical Notes Theoretical notes were compiled from observations during the face-to-face unstructured in-depth interviews. This was achieved through listening carefully to participants’ experiences and during transcribing of interviews from the audio-tapes (Yin, 2016:9). 17.
(31) • Methodological notes The study acquired rich information from the different methods of data collection which were employed for the phenomenological study. The researcher used unstructured, in-depth interviews, observations, field notes and audio-taping as data collection methods which assisted the study’s purpose and objectives (Holloway & Galvin, 2017:89). • Personal notes Personal notes were recorded of the researcher’s personal outlook and thoughts in the process of data collection. 1.11. DATA ANALYSIS. In this study, Giorgi’s phenomenological method was used for data analysis. The data from the transcribed, unstructured in-depth interviews are read (Whiting, 2013:63; Christensen, 2017:84) to gain a sense of the whole meaning. In this qualitative phenomenological study, the researcher dwelled on the data by reading the transcripts of the in-depth experiences of the newly qualified professional nurses (Whiting, 2013:65; Christensen, 2017:84). Once the units of meaning had been identified, the data were then consolidated into essential units of meanings associated with the data. The question “What are your experiences of preparedness for practice as a newly qualified professional nurse in the private hospital setting?” was repeated if necessary during the interview; this revealed clear facts about the phenomenon and lead to the creation of units of meanings (Whiting, 2013:67; Christensen, 2017:85). When the units of meanings had been categorised, descriptive statements were transformed from the participants’ experiences adding structure and essence. Each significant unit of meaning identified had relevant literature references in support of the participants’ quotes, providing an overview of the meaning of preparedness for practice as experienced by the participants of this study (Whiting, 2013:69; Christensen, 2017:85).. 18.
(32) 1.11.1 Literature control Literature control is the theoretical framework that assists in guiding the research study. Literature was integrated into the data obtained from the findings of the research for a solution of the problem identified and an interpretation of the findings of the study. On completion of data analysis, relevant national and international literature of similar studies were integrated which formulated the contribution to this study’s thick descriptions, enhancing knowledge on the phenomenon under study (Bruce & Klopper, 2017:459-460). The researcher searched literature in order to explore and describe the experiences of newly qualified professional nurses’ preparedness for practice. Various resources were utilised such as the institution library and various databases to search for literature: CINAHL, MEDLINE, Science Direct, Ebscohost, Sage, Journals online, and Google Scholar for any related literature focused on newly qualified professional nurses, the transition of newly qualified professional nurses, their experiences and quality patient care thereof. 1.11.2 PHASE 2: Recommendations to support newly qualified professional nurses in a successful transition to the new role as professional nurses, improving their confidence and preparedness for practice in a private hospital setting The recommendations will assist in supporting newly qualified professional nurses in a successful transition into private hospital settings. This will enhance their preparedness for practice and improve their confidence to deliver quality patient care. The research study findings and results assisted the researcher in formulating recommendations for a smoother transition process for the newly qualified professional nurse. 1.12. MEASURES OF TRUSTWORTHINESS. In this study, trustworthiness was ensured by applying the model of Lincoln and Guba (1985:289-331 in Krefting, 1991:214-222; Korstjens & Moser, 2017:120-124). The model is based on the following four criteria for trustworthiness:. 19.
(33) 1.12.1 Credibility Credibility is referred to as reliable, truthful evidence that is obtained from the discovery of human experience and insights as they are lived. It ensures that, that which the study is set out to measure is followed through with correct interpretations of the participants’ perspectives (Krefting, 1991:216; Korstjens & Moser, 2017:121). Credibility in this study was established with the participants through in-depth, individual interviews. The researcher immersed herself into the world of the participants, thereby gaining insight from their viewpoint. Peer examinations involving methodological experts took place to review the research design, methods and purpose, thereby increasing the credibility in the study. 1.12.2 Transferability This refers to the aspect of applicability. Transferability is concerned with whether the research findings can be applied to a similar setting or situation (Krefting, 1991:216; Korstjens & Moser, 2017:122). A dense description of the research design and methods, including a rich description of results with supporting direct quotations of the participants, ensured transferability and enables the reader to assess transferability to their own setting. 1.12.3 Dependability Dependability reflects the consistency of the data. In other words, if the study had to be repeated with the same subjects and in the same context, the findings should remain consistent with the original findings. Coding and re-coding procedures for data checks during the data analysis were carried out by an independent coder. Dependability was ensured by providing detailed descriptions of the research design and methodology; this included the population and sampling method, data collection method, data analysis method and measures of trustworthiness (Krefting, 1991:216; Korstjens & Moser, 2017:121-122).. 20.
(34) 1.12.4 Confirmability Confirmability applies to the strategies used in the study to enhance the neutrality of the researcher and the study. The primary researcher remained free from bias in this research study by ensuring that the findings were only based on the experiences of the participants of the study. Confirmability was furthermore ensured by providing copies of the verbatim transcripts and field notes captured during the interviews to an independent coder familiar with qualitative studies. The application of triangulation and reflexivity methods enhanced the neutrality of the study by utilising a confirmability audit (Krefting, 1991:216; Korstjens & Moser, 2017:121-122). 1.13. ETHICAL CONSIDERATIONS. Ethics in research refers to a set of standards, measures and systems that regulate research activities. Ethics also considers the responsibilities individuals have towards each other with careful attention to right and wrong conduct, including good and bad qualities of character. The manner of treatment of research participants is crucial in ethics; hence, ethics in research provides a strengthened framework regarding the quality of research output. In research it is imperative that ethical approval is granted before the commencement of a research study (Sibinga, 2018:23). This research study was supported by the effective, sound measures of an ethical framework. Ethical considerations for this research study included the obtained permission and clearance from the Research Ethics Committee (Annexure G, REC-01-08-2017) and the Higher Degrees Committee (Annexure G, HDC-01-08-2017) of the University of Johannesburg which was requested before the commencement of the study. Once the clearance letters were received from the University of Johannesburg, the researcher then proceeded to seek approval from the research committee of the private healthcare group. During this time a request was also made to the selected private hospital settings to set up a meeting to introduce the nursing management to the research study. The private hospital group’s Research Operational Committee (Annexure E, UNIV-2017-0025) granted permission to conduct the study and a permission letter was sent to the researcher for the commencement of the research 21.
(35) study; the same was also sent through to the selected hospitals’ nursing management. The following ethical principles of Dhai and McQuoid-Mason (2011), Morison and Furlong (2019), Polit and Beck (2018) and Sibinga (2018) were applied to guide the research: autonomy, beneficence, non-maleficence and justice. 1.13.1 Autonomy The principle of autonomy, according to Dhai and McQuoid-Mason (2011:14) and Morison and Furlong (2019:10), emphasises respect for participants. It involves the self-determination of the participants to make decisions without being influenced by external controls. The researcher respectfully adhered to this principle by not withholding any information from the participants, and by remaining professional during conduct at all times so that the study remained absolute. Respect for the participants’ human dignity encompassed that the participant had the right to make an informed decision about participation in this research study. Thus, in this study a research information letter (Annexure A) was handed to the participants which indicated the full disclosure of the purpose and procedures of the study (Polit & Beck, 2018:81). Informed consent is an important procedure in the research study as it protects the participant. The informed consent ensures that the participant has sufficient information about the study and understands the information about the study. In this research study, the participants had the right to self-determination by making their own decisions of their own free will (Polit & Beck, 2018:83). Information letters handed to the participants were discussed in detail, and the researcher offered to answer any relevant questions related to the research. All consent forms were requested from the participants prior to the start of the interview. The participants signed an informed consent only after they were fully cognisant about the research study. This warranted sufficient time of approximately one to two weeks for the participants’ to think through their contributing to this study. The consent forms were signed in the presence of the researcher, who conducted the interviews. Participants were also made aware that the informed consent included their right to withdraw. 22.
(36) from the study at any time. There was no coercion regarding any decision or statement that the participants delivered to this study. It remained vital that the privacy and confidentiality of the participants were maintained so that the participants did not feel intruded upon at any time (Polit & Beck, 2018:82). The researcher ensured that a private meeting room was arranged so that participants were comfortable and felt safe during the duration of the interview. Participants were also made aware that all data would be treated with confidentiality with no real names being revealed. It was also made known that no information would be used against them at any time, but the data shared would only be utilised to improve support of new professional nurses in their successful transition to the new role as a professional nurse, enhancing confidence and preparedness for practice. Participants were made aware that information would be recorded for accuracy purposes, and participants signed consent for audio-taping (Annexure C). The researcher ensured that the hard copy data of the participants provided to the research were kept under lock and key in a cabinet in the researcher’s office which has secured access to only the researcher and no unauthorised persons. The soft copy data was saved on a hard drive with protected access, only known to the researcher and supervisors of the study. The data provided by the participants will be destroyed two years after publication of the research study (Polit & Beck, 2018:82). 1.13.2 Principle of beneficence and non-maleficence Beneficence is viewed as doing good to participants and permitting no harm, whether social, physical or economical to befall them (Dhai & McQuoid-Mason, 2011:175; Morison & Furlong, 2019:10). The active role of beneficence in this study was that participants’ interests were of utmost value. The participants were viewed as vulnerable individuals who were sensitive to the phenomenon under study. Therefore, the researcher applied great care to permit only good to these sensitive participants. There were no direct benefits for the participants in this study, but the. 23.
(37) vital contribution of their valuable information will improve knowledge and assist in paving the way for future newly qualified professional nurses in their new role. Non-maleficence imposes a duty on the researcher to ensure that no harm is inflicted on any participant during the research study (Polit & Beck, 2018:79). The researcher made sure, as an essential duty that all participants were made to feel comfortable and at ease at all times. It was imperative that participants remained a priority since their participation contributed significantly to the research study. Participants were provided with a private meeting room, with comfortable seating and good ventilation, arranged so that participants were comfortable throughout the interview. Water was available as a beverage if the participants required any. Schedule dates and times for the interviews were made at the participants’ convenience, which participants chose time off from duty. Interviews were arranged for times after the shift and ward meeting days. This permitted that no participant was under any duress for time or concerned about being on duty. Debriefing sessions were available and were made known to the participants if any unpredicted emotional situations arose. The debriefing sessions were part of the employee wellness programme named Care Call with professional counsellors available to assist; this service was free of charge should any participants have required the assistance. Throughout all the interviews, participants felt comfortable, relieved to have spoken out and that someone was listening to their experiences. None of the participants of the research study required any external assistance with regard to debriefing. 1.13.3 Principle of justice Dhai and McQuoid (2011:175) and Morison and Furlong (2019:121) define the principle of justice as an obligation to treat all participants with what is right and proper, and treating all individuals fairly. The researcher thus ensured that the participants were selected and treated fairly with equality and on a nondiscriminatory basis. Participants selected for the study were unknown to the researcher and employed in private hospital settings that were also unknown to the 24.
(38) researcher. Participant selections were based on the inclusion criteria for the research. The research study was open to both genders, and any ethnicity. All participants were treated with great respect and dignity regarding their diverse backgrounds and beliefs. The researcher ensured that no participants were treated in a prejudiced manner (Polit & Beck, 2018:81-82). The researcher acknowledged the principles of anonymity and confidentiality by applying code names for all participants of the study. No personal identifying information was captured for the study, therefore data cannot be linked to any of the participants. Only the researcher and supervisors of the study had access to the collected data (Sibinga, 2018:115). 1.14. DIVISION OF CHAPTERS. Chapter 1: Overview of research study Chapter 1 presents the overview of the research study, the background to the research problem, and the research paradigms outlining the study’s perspectives. Chapter 2: Research design and method Chapter 2 explains the research design and method applied in the study following details of the population and sampling, data collection, data analysis and measures to ensure trustworthiness. Chapter 3: Research results and findings Chapter 3 is an exploration and description of the lived experiences of newly qualified professional nurses’ preparedness for practice. Chapter 4: Evaluation, Recommendations, Limitations and Conclusion Recommendations to assist newly qualified professional nurses in a successful transition to their new role as a professional nurse, as well as limitations and evaluation of the research study, are discussed in Chapter 4. 1.15. SUMMARY. This chapter has briefly outlined the overview of the research study with a focus on the background and rationale, research problem, research purpose and objectives. 25.
(39) Paradigmatic perspectives, as viewed by the researcher, were also described. The definition of key concepts, in addition to the research design, research method, population and sampling method, data collection, and data analysis were further presented. Trustworthiness and ethical considerations utilised in this study were highlighted and the proposed division of chapters for the research was described. Chapter 2 entails a detailed description of the research design and methodology applied in this study.. 26.
Figure
Outline
RESEARCH DESIGN
ANALYSIS OF FIELD NOTES
Category 1.1: Experiences of the newly qualified professional
Category 2.2: As newly qualified professional nurses they
Category 2.3: The experiences of newly qualified professional
Category 3.1 The participants experienced that they had certain
RECOMMENDATIONS
PERSONAL REFLECTIONS
Related documents
3) If it is determined that an underground operation could be resumed in the environment of the Kenricia peninsula, carefully map the outcrop of #3 vein to
While it is difficult to determine the fraction of gene ex- pression changes in drm1 drm2 cmt3 that can be attrib- uted to secondary effects, in many cases, the loss of DNA
(2) In case of any hurdles in implementation of this guideline, the Ministry of Urban Development shall remove hurdles for the municipality or village
contribute significantly to the delivery of School and Departmental strategies by developing and delivering undergraduate and postgraduate curricula; developing their own research and
A preliminary study by Malm, Bryngfors, and Mörner (2010) at the School of Engineering at Lund University (based on a different and more limited student group than the present
While platinum and taxane chemotherapy kills most ovarian tumor cells, we unexpectedly find that FAK activation is elevated in the residual tumor cells of patients
PARADISEC is a collaborative digital research resource set up by the University of Sydney, the University of Melbourne and the Australian National University in
Based on the empirical research of the quality of business environment in Czech Republic and Slovakia, we quantify the Index of perception of fi nancial and credit risk and
