COMPARISON OF THE EFFECT OF CONTINUOUS/INTERVAL
AEROBIC EXERCISE ON THE URINARY AMOUNT OF SODIUM
AND POTASSIUM OF THE BOYS AGED 15-18 YEARS
Mahmoud Reza Mottaghi1, Mojtaba Kianmehr2, Mostafa Amiri3, Zahra Rouhani4, Seyed-Hosein Abtahi-Eivary*5
1
PhD of Physical Education and Sport Sciences, Department of Basic Sciences, Faculty of
Medicine, Gonabad University of Medical Sciences, Gonabad, Iran.
2
Associate Professor, Department of Medical Physics, Faculty of Medicine, Gonabad
University of Medical Sciences, Gonabad, Iran.
3
Assistant Professor in TEFL, Department of Basic Sciences, Faculty of Medicine, Gonabad
University of Medical Sciences, Gonabad, Iran.
4
MA of Physical Education and Sport Sciences, Department of Basic Sciences, Faculty of
Medicine, Gonabad University of Medical Sciences, Gonabad, Iran.
5
*Assistant Professor, Department of Biochemistry, Faculty of Medicine, Gonabad
University of Medical Sciences, Gonabad, Iran.
ABSTRACT
Sport exercises cause many changes in the kidney hemodynamics and
water balance and electrolyte. The aim of this study was to compare
the effect of a continuous/interval aerobic training session on the
amount of sodium and potassium in the urine of boys. This study was a
quasi-experimental study and the population of the study consisted
male students aged 15-18 at the boarding high schools of Gonabad in
the school year of 2012. Of those students who met the inclusion
criteria, 40 students (20 subjects in each group) were randomly
selected. Before exercise, 24-hour urine samples were collected.
Subjects did continuous aerobic exercises in a day and catabolic wash
out was performed for a week and then subjects did interval aerobic
exercises and the priorities in training procedures were determined by
draw. To analyze the data statistically, paired t-test was used to
compare means of quantitative factors before and after the intervention in dependent groups
Volume 5, Issue 7, 1853-1863. Research Article ISSN 2277– 7105
*Corresponding Author
Seyed-Hosein
Abtahi-Eivary
Assistant Professor,
Department of
Biochemistry, Faculty of
Medicine, Gonabad
University of Medical
Sciences, Gonabad, Iran. Article Received on 23 May 2016,
Revised on 13 June 2016, Accepted on 03 July 2016
and independent t-test was used to compare means of quantitative factors between two
training groups. Significance level was considered smaller than. 05. The results showed that
there was no significant difference (p<.05) between the effects of continuous/interval aerobic
exercises on the 24-hour urinary sodium and potassium levels. Moreover, there was no
significant difference between the values of these variables with the exception of 24-hour
urinary potassium (p<.05) before and after both types of these exercises. Therefore, these
exercises not only improve the students' athletic performance but also prevent excessive
pressure on those who lack glycogen, lipid and protein supplies as fuel.
KEYWORDS: Aerobic exercise, sodium, potassium, urine.
INTRODUCTION
One of the most important ways to prevent problems and diseases in the human body is
having a healthy diet which should contain the consumables necessary for the body such as
proteins, vitamins and minerals.[1]
Sodium, potassium and chloride are minerals that are known as electrolytes and are present in
the body as solutions in the form of electrically charged elements called ions. Potassium is
the major cation (positively charged ion) found inside the cells. Setting the body fluid level is
the major function of potassium. Enhancing the control of the muscular performance,
potassium helps the growth and health of nerve cells. This mineral also helps the kidneys to
excrete their waste and plays an important role in mental functions and physical processes.[2]
Sodium and potassium levels play an important role in the diagnosis of various diseases. The
normal range potassium in serum 1.5-3.5 mmol, 4-9.7 in male perspiration and 7.6-15.6
mmol in female perspiration and 25-125 mmol/day in urine.[3]
Failure to provide the required amount of potassium in the body can cause health problems
such as cramps and muscle strain, weak reactions, muscle weakness, fatigue, osteoporosis,
irregular heartbeat, kidney and pulmonary failure and heart attack and mental health
problems such as nerve disorders, anorexia, insomnia, and depression.[4]
Sodium is a major extracellular cation that plays an important role in the distribution of body
fluids. The normal range of sodium in serum is 136-145 mmol, 10-40 mml in male
muscle contraction and nerve reactions. Sodium is also important for the maintenance of
body fluids and the electric potential of animal tissue.[5]
During cell activity, the normal balance of the electrolytes inside and outside cells is changed
and sodium ions enter into the cell and potassium ions exit. To return to the initial state of
such imbalance, intake energy and sodium ions are sent out of the cell and potassium ions
return into the cell. Ions entering and leaving cells in the presence of fluids provide the
cellular energy and excrete waste from them.[2]
The 24-hour urinary excretion of potassium shows the potassium intake in the diet.[6] The
24-hour sodium excretion in the urine is an important parameter showing the daily salt intake.[7]
The best way to estimate the amount of sodium and potassium in the body is analyzing the
24-hour urine.[8, 9] High sodium intake is known as a risk factor for patients with hypertension
and cardiovascular diseases.[10]
Hugh Butler et al. (2007) investigated the relationship between body weight, plasma level,
and serum sodium concentration in 181 men competing in three disciplines through
observations during prolonged exercises. Body weight, plasma level and plasma sodium
changes were measured and the body weight significantly decreased. Although the plasma
sodium level increased after exercise, blood and red blood cells reduced and there was a
strong relationship between blood changes rate and plasma volume and the percentage of the
body fluids change.[11]
High-intensity sport training has an anti-diuretic effect and the changes in urine depend on
the level of antidiuretic hormone and it increases as the exercise intensity increases.[12]
Furthermore, high-intensity exercise causes an increase in urinary electrolyte excretion.[13]
Ahmadi et al. (2009) in a study entitled "On the comparison of the effects of one aerobic
training session and sauna on as sodium and potassium concentration of serum and urine
among athletes" concluded that a session of physical activity significantly increased sodium
and potassium concentrations of serum and one session in the sauna significantly increased
the potassium concentration of the serum; however, there was no significant change in
sodium concentration of the serum. One session of aerobic activity without significant change
of urinary potassium, significantly increased the urinary sodium concentration and finally the
returned to their initial states.[14] Cohen et al. investigating the electrolyte level changes
during the marathon concluded that serum potassium and sodium levels increase.[15] Dave
Johns et al. (2007) studying the electrolyte homeostasis in healthy subjects with/without
exercise after a one-year period of tactile motion decrease observed imbalance in electrolyte
homeostasis of both groups; however, the extent of this imbalance was greater in the group of
participants doing exercises.[16] Lijnen et al. investigating the effect of prolonged sport
exercise (marathon) on the concentration of intracellular erythrocytes and plasma potassium
concluded that the exercise duration is conversely related with changes in potassium
concentration of plasma and it has a direct correlation with urinary potassium excretion.[17]
Since research on changes of urinary sodium and potassium resulting from various aerobic
activities (interval and continuous) has been limited and no research has been conducted
comparing 24-hour urine electrolytes in both continuous and interval aerobic activity
conditions, the present study compares the changes in urinary sodium and potassium during
interval/continuous aerobic activities.
METHODOLOGY
This study was a quasi-experimental study and the population of the study consisted male
students aged 15-18 (n=615) at 4 boarding high schools of Gonabad in the school year of
2012. Mola Mozafar High School with 165 students was selected by draw. Of those students
who met the inclusion criteria, 40 students were randomly selected. Inclusion criteria were
being healthy with regard to medical examinations, doing regular specialized exercises,
having the normal body mass index and only eating the school's dining hall food.
Before exercise, 24-hour urine samples were collected. To this end, 24-hour urine samples
were collected 24 hours before and immediately after the exercise and sent to Jihad
Daneshgahi Laboratory to be examined and the amounts of their urinary sodium and
potassium to be determined. Using sodium - potassium kit (Biochemistry Company, Tehran,
Iran) and flame photometer (Hospitx Flame Photometer, the screen Leith Model, Firenz,
Italy), 24-hour urine sodium and potassium levels were measured.
The participants did continuous aerobic exercise in one day and then to eliminate the effects
of the transition effect of this exercise, catabolic wash out was performed for one week. Next,
the participants performed interval aerobic exercise and the priorities in training procedures
room temperature was controlled and was constant and equal to 22°C at all stages of the
exercise. Using the available sensors in treadmill machines (T960, Rhine Company,
Mashhad, Iran), the participants' heart rate, exercise pressure, as well as the distance were
controlled.
The study procedure was as follows. First, the participants did warm-up exercises (jogging)
for 10 minutes. Then, they did the specific exercise with the intensity of 65-75 percent and
the maximum heart rate (135-175 heartbeats per minute). The test used to do interval aerobic
running was of six 500-meter repetitions (about 4.5 minutes per repetition) and half to one
active rest was used within repetitions. Continuous test with a 3,000-meter distance was
performed steadily. One-week period intervals were considered after each exercise to wash
out. To analyze the data statistically, paired t-test was used to compare means of quantitative
factors before and after the intervention in dependent groups and independent t-test was used
to compare means of quantitative factors between two training groups. Significance level was
considered smaller than. 05.
[image:5.595.110.484.452.609.2]Findings
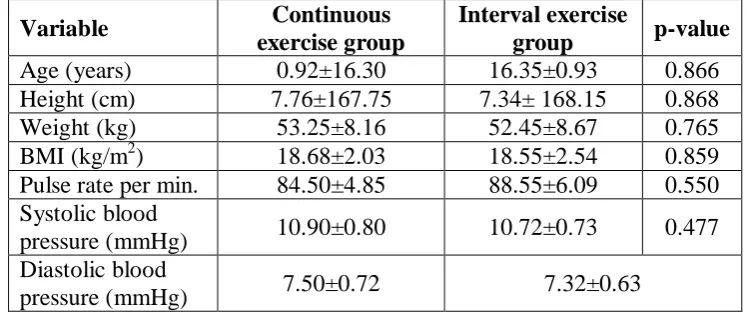
Table 1. Demographic information of the study participants (number of subjects in each group: 20)
Variable Continuous
exercise group
Interval exercise
group p-value
Age (years) 0.92±16.30 16.35±0.93 0.866
Height (cm) 7.76±167.75 7.34± 168.15 0.868
Weight (kg) 53.25±8.16 52.45±8.67 0.765
BMI (kg/m2) 18.68±2.03 18.55±2.54 0.859
Pulse rate per min. 84.50±4.85 88.55±6.09 0.550
Systolic blood
pressure (mmHg) 10.90±0.80 10.72±0.73 0.477
Diastolic blood
pressure (mmHg) 7.50±0.72 7.32±0.63
Individuals' demographic information and information on the untrained 15-18 year male students'
physical health is shown in Table 1 for both types of continuous and interval training. The means of
the demographic information and health variables were not significantly different in continuous and
Table 2. Comparison of the means of 24-hour urinary sodium and potassium of subjects before and after the continuous and interval exercise periods (number of subjects in each group: 20)
Variable Types of aerobic
exercises Before exercise After exercise Significant level Sodium
(mmol/24-hour urine)
Continuous 202.50±82.73 175.95±63.53 0.241
Interval 192.30±88.70 175.55±63.27 0.502
Significant level 0.709 0.984
Potassium (mmol/24-hour urine )
Continuous 219.96±116.68 328.40±152.16 0.002*
Interval 195.07±67.60 288.75±145.22 0.010*
Significant level 0.414 0.404
Table 2 shows the mean and standard deviation of the participants' 24-hour urinary sodium
and potassium before and after exercise. According to Table 2, there was no significant
difference between the effects of one continuous/interval aerobic exercise session on the
24-hour urinary sodium and potassium levels. Moreover, there was no significant difference
between the values of these variables with the exception of 24-hour urinary potassium
(p<.05) before and after both types of these exercises.
DISCUSSION
Since only 20-25% of the metabolism energy is converted into mechanical energy and the
rest (75-80 percent) is converted into heat energy, sweating is the most effective way to
reduce and remove heat generated in the body. Therefore, the lower the rate of perspiration,
the more incomplete the heat removal is and hence the more the cellular damage including
muscular damages will be.[18]
Sweating, on the one hand, leads to dehydration and, on the other hand, to removing the heat
generated. Therefore, its usefulness or harmfulness depends on the condition. In addition,
reduced sweating capacity in boys does not necessarily mean low heat dissipation during
exercise. Perhaps, since large sweat droplets coming together in adults lose their sweating
cooling feature, the efficiency of heat dissipation through sweating is greater for these
athletes as they have smaller and more scattered sweat droplets.[19]
The aim of this study was to examine the effect of one continuous/interval aerobic exercise
session on the 24-hour urinary sodium and potassium levels in males aged 18-15 years in
Gonabad. The results showed that there was no significant difference (p<.05) between the
continuous/interval aerobic exercises for both experimental groups. Moreover, the sodium
level of their urine decreased; however, it was not statistically significant. The potassium
concentration before and after both types of exercises was significantly different.
Ninety percent of the body potassium is intercellular and 70-75 percent of this amount exists
in the skeletal muscle cells and the sodium potassium pump keeps the concentration gradient.
During the workout, potassium quickly exits from the muscle cells and it can even lead to
hyperkalemia depending on the intensity of exercise, which can cause increased urinary
potassium after doing continuous/interval exercise.[18] Such findings have also been obtained
in this study. As it is shown in Table 2, continuous exercise compared with the interval one
has increased the outflow of potassium from the cells, which represents greater damage of
muscle cells caused by continuous exercise so that the amount of potassium excretion out of
the cell during interval training has increased about 20%. An increase in extracellular
potassium of muscle tissues causes the dilation of blood vessels in these tissues and this
would, in turn, lead to improved blood supply. On the other hand, it also leads to
hyperpolarized heart cells and consequently reduces the sensitivity to stimulation and
ultimately reduces the heart rate. Obviously, the greater the extent of the potassium excretion
from the cells is, the more it would lead to reduced heart rate, increased dilation of vessels,
reduced blood pressure, lack of blood supply to tissues, and increased tissue hypoxia.[19]
The lower extracellular potassium in the second phase of exercises, compared to the first
phase, after the wash out indicates the likely depletion of intracellular potassium which the
wash out period has failed to replace it. Of course, another possibility is that angiogenesis in
the muscles has occurred due to exercises of the first phase and this metabolism reduced
anaerobic, resulting in reduced production of lactic acid. These show less muscle damage and
less potassium excretion. Sodium excretion during the first phase of these two types of
exercise leads to increased secretion of aldosterone and this aldosterone causes sodium
retention in the body (which is shown by reduced sodium excretion in the second phase of the
exercises) and the excretion of potassium. Reduced sodium excretion in the urine causes
decreased sweating, increased body temperature, increased muscle damage, and increased
potassium excretion.
Sodium plays an important role in effective hydration so that when sufficient amounts of
sodium and water are taken, some sodium remains in intravascular fluid and prevents the
drinking. Thus, vasopressin and aldosterone levels have also been maintained and
inappropriate diuresis (it is inappropriate because the body water balance is negative) does
not occur. Furthermore, the tendency to drink water while keeping plasma osmolality and to
reach balanced sustainable water is triggered.[20] Although the amounts of sodium excretion
in individuals' sweating are different, sodium excretion through sweating decreases among
athletes due to getting accustomed to certain weather conditions.[21] This can be in line with
sodium excretion from the kidneys as well. Sports activities and their intensity reduce blood
supply to the kidneys and depending on the intensity, it can reach 25% of the rest state[22] and
this could lead to a decreased urine volume.[23]
The major part of sweat is composed of electrolyte sodium chloride with the concentration of
10-70 mm, while potassium, calcium and magnesium are also present in smaller amounts.
The concentration of these components depends on factors such as diet, sweating intensity,
body hydration, and environment temperature. Sweat glands absorb sodium via active
transport mechanism. The absorption will not be increased by sweating speed and, as a result,
the higher the sweating intensity is, the more the sodium excretion would be.[24] However, the
amount of sodium in a person accustomed to a certain weather condition could be reduced to
50%.[25] The concentration of sweat potassium with an average of 5 mm varies from 3 to 15
mm. Gender, maturity, and age have no significant effect on the concentration of sweat
electrolytes.[26]
The limitations of this study include inability to increase the amount of exercise according to
the subjects' ability and age as well as failure to measure participants' sweat urea.
CONCLUSION
Cardiovascular system, on the one hand, supplies the required oxygen and fuel via redirecting
blood flow to the muscles during exercise and on the other hand removes the heat from the
tissue. Obviously, when excessive sweating occurs due to dehydration, the heartbeat and the
amount of the blood sent out of the heart simultaneously reduce as the internal temperature of
the body enhances and this ultimately would lead to a reduction in athletic performance.[27-29]
Although the cardiovascular response to exercise training is weaker in children than that of
adults, it will not be regarded as a defect any longer and will they not have any difference
Interval and continuous aerobic exercise had no significant effect on the amount of urine
sodium of the subjects; however, the amount of urine potassium showed significant
differences before and after both types of exercise and none of other variables were
significantly different in both continuous and interval aerobic exercise groups. Therefore,
despite the fact that the training pressure was in the range of 65-75 percent of maximum heart
rate, the body was not in the deficiency of energy resources, sugar and fat. Hence, these
exercises not only improve the students' athletic performance but also prevent excessive
pressure on those who lack glycogen, lipid, and protein supplies as fuel.
ACKNOWLEDGEMENT
We, researchers, would like to express our gratitude to the research deputy of the Gonabad
University of Medical Sciences for the financial support provided and the dear principal of
Mola Mozafar boarding High School in Gonabad for his cooperation in this project. We also
appreciate the students who participated in this study.
RESOURCES
1. Ganio MS, Armstrong LE, Casa DJ, McDermott BP, Lee EC, Yamamoto LM , et al.
Mild dehydration impairs cognitive performance and mood of men. Br J Nutr, 2011; 106:
1535-1543.
2. Everts M. Potassium Homeostasis during Exercise in Domestic Species: The role of the
sodium potassium pump in skeletal muscle. Veterinary Sciences Tomorrow, 2000; 1-10.
3. A Kaplan and L. VL Szabo. Clinical Chemistry: Interpretations and techniques. In:
Electrolytes, pH and Blood gases. edition 1st, lea and Febiger. Philadelphia. 1979; 131.
4. Importance of Potassium in Human Body by Samuel Murray Retrieved July 19, 2010,
from http://articles.directorym.com/Importance Of Potassium In Human Body a
980047.html.
5. Determination of sodium and potassium by flame photometry. Medical chemistry
LOKT.00.009 Retrieved July 19, 2010, from http://tera .chem .ut. ee/ ~
koit/arstpr/nak_en.
6. Ljutić D, Dodig J, Kovacić V. Arterial hypertension and diet. Lijec Vjesn 2007; 129:
364-6.
7. Erdem Y, Arici M, Altun B, et al. The relationship between hypertension and salt intake
8. Bingham SA: The dietary assessment of individuals; methods, accuracy, new techniques
and recommendations. Nutrition abstract review, 1987; 57(10): 705–741.
9. J.G. Mill, A.B.T. da Silva, M.P. Baldo, M.C.B. Molina and S.L. Rodrigues Correlation
between sodium and potassium excretion in 24- and 12-h urine samples. Brazilian Journal
of Medical and Biological Research, 2012; 45: 799-805.
10.Dickinson HO, Mason JM, Nicolson DJ, et al. Lifestyle interventions to reduce raised
blood pressure: a systematic review of randomized controlled trials. J Hypertens, 2006;
24: 215-33.
11.Hew, Butler T., Collins, M., Bosch, A., Sharwood, K., Wilson, G., Armstrong, M.,
Jennings, C., Swart, J., Noakes, T., Maintenance of plasma volume and serum sodium
concentration despite body weight loss in ironman triathletes. Clin J Sport Med., 2007
Mar; 17(2): 116-22.
12.Maughan RJ. Fluid and Electrolyte loss and Replacement in Exercise. J Sports Sci., 1991;
9: 117-42.
13.Poortmans JR. Exercise and renal function. Sports Med, 1984; 1: 125-53.
14.Ahmadi N, Aghili AK, Azimzadeh E, Hedayati M. Comparison of the effects one session
aerobic activity and sauna on serum and urinary sodium and potassium athletes. Pajohesh
Pezeshki, 2009; 2(33): 70-76.
15.Cohen I, Zimmerman AL. Changes in serum electrolyte levels during marathon running.
S Afr Med J., 1978; 53: 449- 53.
16.Deogenes KG, Kakuris KK, Deogenov VA, Yerullis KB. Electrolyte homeostasis in
trained and untrained healthy subjects during prolonged Hypokinesia. Gomel, Belarus:
Higher Institute of Biochemistry, 2007; 40(8): 536-544.
17.Lijnen P, Hespel P, Fagard R, Goris M, Lysens R, Vanden Eynde E, et al. Effect of
prolonged physical exercise on intra-erythrocyte and plasma potassium. Eur J Appl
Physiol Occup Physiol., 1989; 59: 296-302.
18.Maughan RJ, Shirreffs SM. Development of individual hydration strategies for athletes,
Int J Sport Nutr Exerc Metab, 2008; 18(5): 457-72.
19.Rowland T. Thermoregulation during exercise in heat in children: old concepts revisited.
J Appl physical, 2008; 105: 718- 724.
20.Andrew Carlton, Robin Marc Orr. The effects of fluid loss on physical performance: A
critical review. Journal of Sport and Health Science, 2015; 4(4) 357-363.
21.Edward f. Coyle. Fluid and fuel intake during exercise. Journal of Sports Sciences, 2004;
22.Poortmans JR. Exercise and renal function. Sports Med, 1984; 1: 125-53.
23.Maughan RJ. Fluid and electrolyte loss and replacement in exercise. J Sports Sci., 1991;
9: 117-42.
24.Sawka MN, Wenger CB, Pandolf KB. Thermoregulatory responses to acute exercise-heat
stress and heat acclimation. In: Fregly MJ, Blatteis CM, eds. Handbook of physiology.
Section 4, environmental physiology. New York: Oxford University Press, 1996; 157–85.
25.Allan JR, Wilson CG. Influence of acclimatization on sweat sodium concentration. J Appl
Physiol, 1971; 30: 708–12.
26.Brouns F. Heat-sweat-dehydration-rehydration: A praxis oriented approach J Sports Sci.,
1991; 9: 143–52.
27.Gonza´les-Alonso G, Mora-Rodriguez JR, Below PR, Coyle EF. Dehydration markedly
impairs cardiovascular function in hyperthermic endurance athletes during exercise. J
Appl Physiol, 1997; 82: 1229–1236.
28.Abedi, Gh, Mohammadi, A., Mohammadi, F, Alizadeh, A, Hosseini, H, Rostami, F.
University students' personality profile based on casta & MaCrea five factor theory.
International Journal of Collaborative Research on Internal Medicine and Public Health.,
2012; 4(6): 1330-1336.
29.Abedi Gh, Azimehr L, Rostami F. Mohammadi, S. Applying a model of patient's right in
the state hospital, Sari, Iran. International Journal of Collaborative Research on Internal